
Abstract
Background:
Studies have shown that meniscal and chondral lesions are more common at the time of revision anterior cruciate ligament reconstruction (ACLR) compared with primary surgery; however, few have evaluated the same patients through both primary and revision surgery.
Purpose:
To describe the prevalence of meniscal and chondral lesions at the time of primary and subsequent revision ACLR and to determine the effect of age and femoral tunnel drilling technique on the development of intra-articular pathology over time.
Study Design:
Case series; Level of evidence, 4.
Methods:
All patients who had primary and subsequent revision ACLR in the same knee between 1997 and 2022 were identified from a prospectively collated database. The grading of chondral surfaces in each compartment, the presence of any meniscal tears, and treatment performed were recorded. Patients were grouped according to age and femoral tunnel drilling technique to allow subgroup analysis.
Results:
Overall, 262 patients were included. Median age at primary surgery was 20.2 years. Lateral meniscal tears were more prevalent than medial tears at both primary (34.7% vs 28.2%; P = .11) and revision surgery (44.3% vs 40.8%; P = .43). Chondral lesions were most frequently found on the patella (8.8%) and the medial femoral condyle (MFC; 8.0%) at primary surgery. Between surgeries, new lesions developed most commonly on the MFC (13.0%) and the lateral femoral condyle (LFC; 11.1%). It was significantly more common for lateral meniscal tears treated with repair or left in situ at primary surgery to be healed at the time of revision surgery than medial tears (P = .01). Significantly more patients who had transtibial drilling of the femoral tunnel had a new meniscal tear at revision surgery (P = .001). Age did not have a significant influence on the prevalence of meniscal pathology.
Conclusion:
The prevalence of intra-articular pathology increased between primary and revision ACLR. Lateral meniscal tears were more prevalent than medial tears at both surgeries. At revision surgery, new chondral lesions were more commonly found on the MFC than the LFC. The higher incidence of new meniscal tears observed in the transtibial group may reflect the more vertical graft orientation with this technique and its inferior ability to control rotation.
Keywords
Injuries to the anterior cruciate ligament (ACL) are commonly associated with concomitant injuries to the menisci and chondral surfaces. The incidence of meniscal tears associated with injury to the ACL has been reported at between 44% and 85%.3,6,10,11,13-16,20 Chondral injuries have been reported to occur in between 7% and 39% of these patients.11,16,27 Meniscal and chondral lesions are generally more prevalent in patients undergoing revision anterior cruciate ligament reconstruction (ACLR) compared with those undergoing primary ACLR.16,22 Chronic instability of the knee has been shown to result in higher rates of intra-articular pathology which may, in part, explain this difference. 13
Surgical factors may influence the degree of knee stability postoperatively. Historically, femoral tunnels were frequently drilled using a transtibial (TT) technique, but most surgeons changed to an anteromedial (AM) portal technique after the more vertical graft position produced by the TT technique was shown to be nonanatomic and offer poorer rotational stability postoperatively.1,4,12,21
A number of studies have documented the prevalence of meniscal and chondral lesions at the time of ACLR.3,5,6,7,10,11,14-16,20 Fewer studies have followed the same patients through both primary and revision ACLR.16,22,27 This study reports the prevalence of meniscal and chondral lesions in a group of patients who underwent primary ACLR and then subsequent revision ACLR.
The aim of the study was to investigate the effect of age on the prevalence of meniscal and chondral lesions and also to compare how the evolution of intra-articular pathology differed between patients who had their femoral tunnel drilled using a TT technique and those in whom an AM portal technique was utilized. We hypothesized that both meniscal and chondral lesions would be more prevalent with increasing age and also with a TT technique given the inferior ability of a more vertical graft to provide rotational stability to the knee.
Methods
Patients who had undergone both primary and subsequent revision ACLR in the same knee were identified from a prospectively collated database. All procedures were performed by a single surgeon (J.A.F.). This study was a retrospective analysis of the prospectively collected data and for this study, patients were excluded if they had sustained a multiligamentous knee injury or if they had undergone surgery to the ipsilateral knee before primary ACLR. This study received ethics committee approval from the ethics board of our university and all patients provided informed consent to participate in clinical research.
All procedures were performed between 1997 and 2022. For all patients, data were recorded for each surgery including patient age, time from injury to surgery, time from surgery to reinjury, time from reinjury to revision surgery, sex, graft type, and femoral drilling technique. Chondral surface integrity was graded in each area of the knee (patella, trochlea, medial femoral condyle [MFC], medial tibial plateau, lateral femoral condyle [LFC], and lateral tibial plateau) according to the International Cartilage Repair Society (ICRS) classification system. When a lesion was noted at revision surgery, this was compared with the grading at primary surgery so that progression could be quantified and new lesions could be counted accurately. The presence or absence of a meniscal tear was recorded and note was made of any treatment performed to any area of pathology.
Subgroup analysis was conducted to determine any association of meniscal pathology with age and femoral tunnel drilling technique. Patients were grouped according to age at the time of primary surgery: <20 versus ≥20 years. Age 20 years was used as a cutoff as it has been shown in previous studies that patients aged <20 years have a higher chance of graft rupture than those aged >20 years. 25 Patients were also grouped according to femoral tunnel drilling technique: TT versus AM portal.
Statistical Analysis
Statistical analysis was performed using SPSS (IBM Version 28). The Kolmogorov-Smirnoff test confirmed that the demographic data did not follow a normal distribution and therefore these data were presented using median and range. The Mann-Whitney test was used to check for significant differences in age between the femoral tunnel drilling technique groups. It was also used to compare time from injury to surgery, time from surgery to reinjury and reinjury to revision between both age groups and femoral tunnel drilling technique groups.
The prevalence of medial and lateral meniscal tears was compared using the chi-square test. Comparisons were made using the chi-square test where the sample sizes were sufficient, and the Fisher exact test was used where sample sizes were too small to reliably use the chi-square test. The prevalence of chondral lesions in the patient group as a whole was compared descriptively without formal statistical analysis in order to make an observation of the patterns of injury. The prevalence of chondral lesions was compared between age groups and femoral tunnel groups using chi-square test. Results were considered statistically significant with a P value < .05.
Results
A total of 262 patients were included who had both primary and revision ACLR performed. Of the 262 patients having primary surgery, all had an ipsilateral autograft. Hamstring tendons were used in 227 patients, patellar tendon in 21 patients and quadriceps tendon in 14. Basic demographic data for all groups are listed in Table 1.
Demographic Data of the Study Cohort a

Data are presented as median (range) unless otherwise indicated. Five patients were excluded from analysis of time from surgery to injury and from injury to surgery because they had instability with an intact graft. AM, anteromedial; TT, transtibial.
For the analysis by age, there was no significant difference between the 2 groups in terms of time from injury to surgery (P = .46) or time from reinjury to revision surgery (P = .2). There was a difference between age groups in terms of time from primary surgery to reinjury (P = .01) with the older patients having a longer period with intact grafts. When comparing the demographic data for the femoral tunnel groups, there was no significant difference in age between groups (P = .46) or time from injury to primary surgery (P = .46). There was, however, a difference in terms of time from primary surgery to reinjury with the TT patients having a longer time with an intact primary graft (P < .001) and a longer period of time between graft rupture and revision surgery (P < .001).
Results for All Patients
Lateral meniscal tears were more common than medial meniscal tears at primary surgery (34.7% vs 28.2% P = .11) and at revision surgery (44.3% vs 40.8% P = .43), but these differences were not statistically significant. Some patients had a meniscal tear either left in situ or repaired at primary surgery which was noted to have healed at revision (12 medial tears and 30 lateral tears). When this was taken into account, the medial meniscus was more likely to remain intact through both primary and revision surgery when compared with the lateral meniscus (P = .02). The lateral meniscus was more likely than the medial meniscus to be intact at primary and torn at revision surgery, but the difference was not significant. Lateral meniscal tears that were not addressed surgically were less likely to require further treatment at revision than medial meniscal tears that were not addressed surgically (P = .03). Lateral meniscal tears that were either left in situ or repaired at primary ACLR were more likely to have healed at revision than medial tears that were either left in situ or repaired at primary ACLR (P = .01). A summary of meniscal pathology observed in all patients is provided in Table 2.
Summary of Meniscal Pathology in All Patients a

Data are presented as n/N (%). Those categorized as tear at primary which had healed at revision include patients who had a tear treated nonoperatively and those who underwent repair.
Chondral lesion data are summarized in Figure 1, and the severity of chondral lesions is illustrated using the ICRS classification in Figure 2. The patella was the most common site for a chondral lesion at primary surgery (8.8% of patients) closely followed by the MFC (8.0% of patients). The MFC was the most common site for a lesion at revision surgery (21% of patients). A new lesion at revision surgery was most frequently observed on the medial femur (13% of patients). At revision surgery, a new lesion was found on the lateral femur in 11.1% of cases. Medial femoral lesions were also most likely to progress (1.5% of cases), but overall, progression of chondral lesions was rarely observed. In terms of severity of the chondral lesions observed, 93% of all lesions were ICRS grade 1 or 2 and 7% were grade 3 or 4 at primary surgery. At revision surgery, 78% of all lesions were ICRS grade 1 or 2 and 22% were grade 3 or 4 (Figure 2).

Percentage of patients with a chondral lesion in each area. Also shown are the percentages of patients with a new lesion at revision and those in whom a chondral lesion demonstrated progression.

Chondral lesion classification according to the International Cartilage Repair Society (ICRS) grading system.
Results Based on Age Group
The meniscal pathology observed in each age group is detailed in Table 3. The prevalence of medial meniscal tears was higher in the older group (30.7%; n = 42) compared with the under age 20 years group (25.6%; n = 32). A similar trend was observed at revision surgery where 35.2% of patients had a medial meniscal tear at revision in the under age 20 years group versus 46% of patients in the 20 years and older group. Neither of these trends reached statistical significance. The prevalence of lateral meniscal tears at primary surgery also increased with age, but the trend was not significant. There was no significant difference between the rate of lateral meniscal tears found at revision.
Meniscal Pathology Data Based on Age Group a
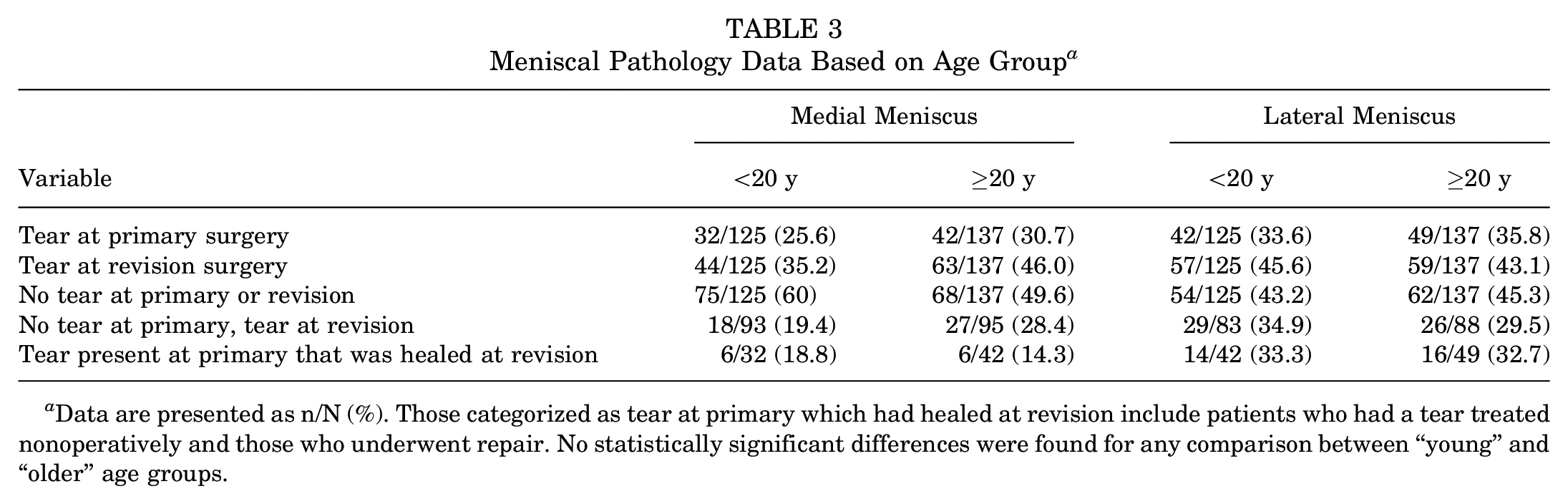
Data are presented as n/N (%). Those categorized as tear at primary which had healed at revision include patients who had a tear treated nonoperatively and those who underwent repair. No statistically significant differences were found for any comparison between “young” and “older” age groups.
Detailed results for chondral pathology by age group are listed in Table 4. To summarize these findings, lesions on the patella were more prevalent in the older age group at primary surgery (P < .001). New patellar lesions at revision surgery were also more frequently observed in the older group, but this difference was not statistically significant. Trochlear lesions were uncommon in both age groups at primary surgery. New trochlear lesions were more frequently noted in the older age group at revision surgery (P = .01) Medial femoral lesions were the most prevalent chondral injury found in the under age 20 years group (5.6% of patients). They occurred more commonly in the older group (10.2%), but this difference was not statistically significant. New lesions on the medial femur at revision surgery were also more frequently seen in the older patient group although the difference was not significant and the medial femur was the most common site for a new lesion to occur in both age groups. LFC lesions were relatively rare in both groups, but new lesions in this area occurred at similar rates to the medial femur in both age groups. There was no evidence of progression of chondral lesions in any of the patients in the under age 20 years group. Only 7 chondral lesions progressed between surgeries in the 20 years and older group.
Chondral Lesion Data Based on Age Group a

Data are presented as n (%).
Significantly higher prevalence of patellar lesions at primary surgery in the older age group (P < .001).
Significantly more trochlear lesions observed in older age group at revision surgery (P = .01).
Results Based on Femoral Tunnel Technique
The meniscal pathology observed in the femoral tunnel groups is presented in Table 5. There was no significant difference in the prevalence of medial meniscal tears or lateral meniscal tears at primary surgery when comparing the TT and AM portal groups. New medial meniscal tears were observed more frequently in the TT group at revision surgery (P = .049). New lateral meniscal tears were also observed more frequently in the TT group at revision surgery (P = .009). More patients had a meniscal tear in general at revision surgery in the TT group (P = .001). None of the other differences in meniscal pathology between groups reached statistical significance.
Meniscal Pathology Data Based on Femoral Drilling Technique a
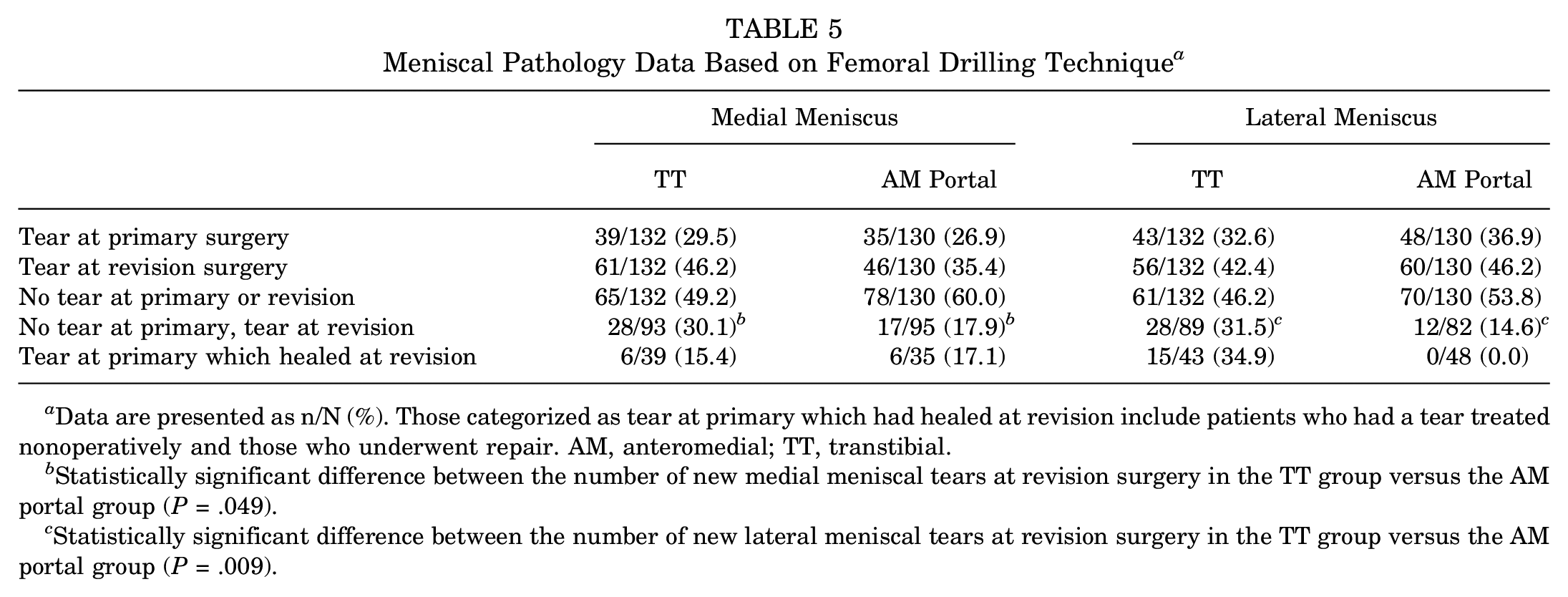
Data are presented as n/N (%). Those categorized as tear at primary which had healed at revision include patients who had a tear treated nonoperatively and those who underwent repair. AM, anteromedial; TT, transtibial.
Statistically significant difference between the number of new medial meniscal tears at revision surgery in the TT group versus the AM portal group (P = .049).
Statistically significant difference between the number of new lateral meniscal tears at revision surgery in the TT group versus the AM portal group (P = .009).
The prevalence of chondral lesions, subdivided by femoral tunnel drilling technique, is presented in Table 6. New chondral lesions were observed more frequently at revision surgery when a TT technique had been used in all anatomic areas, with the exception of the lateral tibial plateau. None of the differences observed between groups in terms of chondral lesions were statistically significant.
Chondral Lesion Data Based on Femoral Drilling Technique a

Data are presented as n (%). No statistically significant differences were found between the groups. AM, anteromedial.
Discussion
There are several key findings in this study. Lateral meniscal tears were more prevalent than medial meniscal tears at both primary and revision surgery. New lateral meniscal tears were also more prevalent than new medial meniscal tears at revision surgery, although these trends did not reach statistical significance. Patients who had a TT femoral tunnel were found to have a significantly higher prevalence of new lateral and medial meniscal tears at revision surgery compared with those who had an AM portal technique. Age did not appear to have a significant influence on the prevalence of meniscal tears at either surgery. Chondral lesions were observed most commonly on the patella and MFC. New lesions were observed most commonly on the MFC and LFC at revision surgery and in general, it was uncommon to see progression of chondral lesions according to ICRS grade.
In relation to our findings on meniscal pathology, the increased prevalence of lateral tears at both surgeries and new lateral tears at revision surgery is a finding that is not reflected in much of the previous literature on this topic. Pioger et al 16 reported on a series of 213 patients who underwent both primary and revision ACLR and found that medial meniscal tears were more prevalent at both surgeries. Similarly, when studying patients at primary ACLR only, both Tandogan et al 20 and Paletta et al 15 reported that medial meniscal tears were more prevalent than lateral meniscal tears. Conversely, Wyatt et al 27 studied a series of 261 patients at both primary and revision ACLR and found that lateral meniscal tears were more common at primary surgery, whereas medial meniscal tears were more common at revision. To explain these mixed findings, some authors have suggested that lateral meniscal tears are seen more frequently when ACLR is performed acutely, whereas medial meniscal tears are associated with chronic instability or a delay to surgical stabilization.11,13
Our patients had a median time from initial injury to primary surgery of 59 days. This was shorter than the 107 days in the study by Wyatt et al. 27 Our time from graft rupture to revision surgery was a median of 56 days which is shorter than the 5.8 months reported by Pioger et al. 16 Therefore, the patients in our study did have a shorter duration with an unstable knee than those in previous studies, which could account in part for our finding of a lower prevalence of medial meniscal tears at revision surgery. It is important to note that the observed differences between medial and lateral meniscal tears at primary surgery, at revision surgery and in the prevalence of new tears are statistically not significant and therefore caution should be exercised when interpreting these findings.
Nonoperative treatment of selected lateral meniscal tears appeared to be more successful than nonoperative treatment of selected medial tears. We found that lateral meniscal tears treated nonoperatively at primary surgery less frequently required any treatment at revision surgery when compared with nonoperatively treated medial tears. Furthermore, lateral meniscal tears were more frequently found to have healed at revision surgery after either being repaired or treated nonoperatively at primary surgery. These findings may reflect a better innate healing capacity of the lateral meniscus when compared with the medial side. It has previously been postulated that this may be due to improved vascularity on the lateral side. 2
The patient group was composed predominantly of young patients, which is an expected finding given that these patients are most likely to sustain an ACL injury and are also most likely to have a graft rupture. 25 There was no significant difference between age groups in terms of time from primary injury to surgery. There was, however, a difference between groups in terms of time from primary surgery to graft rupture. The older patient group had a longer period with an intact graft, which may be due to lower activity levels in older patients which make them less susceptible to graft rupture. Although we did observe that there was a trend for an increased prevalence of meniscal tears (particularly medial) at both primary and revision surgery in the older patient group, this did not reach statistical significance. To the best of the authors’ knowledge, the effect of age on the prevalence of meniscal tears at the time of ACLR has not been studied previously and, thus, there are limited data with which to compare the current findings.
Those patients who had a TT femoral tunnel had a significantly higher frequency of new medial meniscal tears and new lateral meniscal tears at revision when compared with the AM portal group. Before making comparison between the TT and AM portal groups, we should consider that there was a difference between the groups in terms of time from reinjury to revision surgery with the TT patients having a median delay of 69 days and the AM portal group having a median delay of 44 days. However, it seems unlikely that a difference of just over 3 weeks could result in a significant difference in the prevalence of intra-articular pathology between groups. ACLR performed using an AM portal technique has been shown to provide a more anatomically positioned graft, provide better rotational control of the knee and result in more normal biomechanics in gait when compared with the traditional TT approach.1,4,12,19,23 This may explain the higher prevalence of intra-articular pathology observed at revision surgery in the TT group. However, some authors have suggested that by placing the ACL graft in a more “anatomic” position using an AM portal technique, the graft is under more tension throughout the range of motion and that this may result in more graft ruptures. 17 This may be part of the explanation for the observation that the time from primary surgery to graft rupture was significantly longer in the TT group. Although the AM portal technique has been shown to provide better rotational control, to the best of the authors’ knowledge, ours is the first study that shows the direct impact that this has on the prevalence of meniscal tears at revision surgery.
In relation to chondral pathology, we found that the patella and the MFC were the most common sites for chondral lesions at primary surgery. At revision surgery, new lesions occurred most frequently in the MFC and then the LFC. Our older patient group had a significantly higher prevalence of patellar lesions and a higher prevalence of new trochlear lesions at revision surgery. It may be that patellofemoral lesions are more related to patient age than to ACL injury and reconstruction, but our study was not powered or designed to investigate this specifically. The prevalence of new chondral lesions was higher at revision surgery in the TT group in all anatomic areas with the exception of the lateral tibial plateau. While this finding may be in keeping with chronic instability from a more “vertical” graft, none of the differences observed were statistically significant.
Relatively few chondral lesions demonstrated progression in severity between primary and revision surgeries in our study. Previous studies have not documented chondral lesion severity or progression and therefore comparison is not possible.16,27 Although we do know that osteoarthritis of the knee is common in the longer term after ACLR, it is likely that the time interval between primary and revision surgery is insufficient to see significant macroscopic progression of chondral lesions. 26 It also is possible that modern ACLR techniques do offer some protection to the knee against osteoarthritis although this was beyond the scope of this study and this topic remains a source of significant controversy in the literature.18,24 Our study demonstrated a higher prevalence of patellar lesions than those reported previously with 8.6% of patients in our study having a patellar lesion at primary surgery versus 0.4% and 2.3% in the Pioger et al 16 and Wyatt et al 27 studies, respectively. This difference is difficult to explain, but there is some evidence to suggest that the prevalence of patellofemoral lesions is influenced by specific patient activities. An increased prevalence is seen in those participating in jumping activities and there is an increased prevalence in the athletic population in general.8,9 Our findings could therefore be potentially explained by subtly different patient activity profiles.
Limitations
There are some important limitations of this study that must be recognized. This was a retrospective series which includes patients who had surgery across a large time period. There may have been changes to rehabilitation and other more subtle changes to surgical technique and rehabilitation over this time which may also have influenced patient outcomes and intra-articular pathology and made direct comparison of some variables such as femoral drilling technique less reliable. One specific example of this is the recent repopularization of the lateral extra-articular tenodesis (LEAT) as it has been shown to decrease the rate of graft rupture. In our study, 10 patients had a LEAT at the time of primary surgery which could in theory give more stability to their knee and potentially reduce the prevalence of intra-articular pathology at the time of revision surgery. All 10 of these patients were in the AM portal group and this could be a factor in the lower prevalence of intra-articular pathology observed in the AM portal group at revision. However, the overall number of patients who had a LEAT at primary surgery was small and therefore unlikely to have had a significant impact on our results as a whole. Subtle equipment changes such as the introduction of 4K arthroscopic cameras during the study period could theoretically have improved diagnostic accuracy as time progressed. Drawing conclusions about the causation of certain lesions observed in the knee is not possible given the retrospective nature of this study. Statistical analysis of differences observed, particularly in reference to chondral lesions, is less reliable due to the overall small numbers of lesions observed. It would have been interesting to look more closely at the development of chondral lesions as a result of meniscectomy at revision surgery, but we were unable to do so given the surprisingly small numbers of new chondral lesions observed at revision surgery.
Conclusion
We have found that the prevalence of intra-articular pathology increases between primary and revision ACLR. Lateral meniscal tears were more prevalent at both time points although this difference was not statistically significant. The patella and MFC were the most common sites for chondral lesions. The higher incidence of new meniscal tears observed in the TT group could potentially be due to the relatively more vertical graft orientation yielded by this technique and poorer rotational control.
Footnotes
Final revision submitted June 27, 2023; accepted July 31, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.A.F. is a paid associate editor for the Orthopaedic Journal of Sports Medicine. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from La Trobe University (Ref. No. HEC22221).