
Abstract
Background:
Delayed anterior cruciate ligament (ACL) reconstruction has been associated with an increased risk of meniscal tears. However, studies comparing early versus delayed ACL reconstruction have not clearly demonstrated that meniscal tears diagnosed arthroscopically are new injuries as opposed to concomitant injuries sustained during ACL rupture.
Purpose:
To determine whether and how delay of ACL reconstruction is associated with risk of “new” meniscal tears (defined as those visualized arthroscopically that had not been detected on magnetic resonance imaging [MRI]) in adult and pediatric patients.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We retrospectively identified patients who underwent primary ACL reconstruction between 2013 and 2022 at our institution. To ensure that MRI reflected initial intra-articular pathology, we included only patients who had an MRI scan within 3 weeks after injury (173 pediatric and 369 adult patients). Multivariate Poisson regression was performed to calculate the adjusted relative risk (ARR) of new meniscal tears after delayed (≥8 weeks from injury) operative treatment.
Results:
The mean (± SD) time from injury to MRI was 1.0 ± 0.8 weeks for pediatric patients and 1.1 ± 0.7 weeks for adults. Less than half of the meniscal tears observed arthroscopically had been absent on initial MRI. New medial meniscal tears occurred in 15% of pediatric patients and 16% of adults. New lateral meniscal tears occurred in 48% of pediatric patients and 34% of adults. Among pediatric patients, delayed ACL reconstruction was associated with higher risk of new medial tears (ARR, 3.9; 95% CI, 1.5-10) but not lateral tears (ARR, 0.8; 95% CI, 0.4-1.5). In contrast, adults had no significant increase in risk of meniscal tears associated with operative delay.
Conclusion:
Delayed ACL reconstruction may be acceptable in adults, who may be less active and less injury-prone than children and adolescents.
Keywords
Anterior cruciate ligament (ACL) tear is one of the most common sports injuries, with an estimated incidence of 69 tears per 100,000 person-years. 36 Historically, operative management of ACL injuries in pediatric patients has been delayed to allow physeal maturation, with the understanding that early operative intervention may cause angular deformity or leg-length discrepancy secondary to physeal disruption in skeletally immature patients.1,5,25,35,38 However, delayed reconstruction of the ACL-deficient knee has been associated with a higher risk of meniscal pathology in patients of all ages.2,6,13,19,23,26,41,42 Specifically, translational stress exceeding physiologic ranges may be placed on the medial meniscus due to loss of structural support from the ACL, resulting in tears of the medial meniscus. 2 Several studies have documented poor long-term outcomes in patients who develop such meniscal injuries after ACL tears, including a greater risk of knee osteoarthritis.10,11,28,31,37 Although recent advancements in physeal-sparing techniques have reduced the need for purposeful delay of ACL reconstruction, the issue of expediting surgical treatment remains pertinent for patients of all ages.
Studies comparing early versus delayed reconstruction of the ACL-deficient knee have not clearly demonstrated that meniscal tears discovered arthroscopically are, in fact, “new” injuries, as opposed to concomitant injuries sustained at the time of ACL rupture. Many of these studies have relied on intraoperative findings, without magnetic resonance imaging (MRI) data, and analyzed the overall incidence of meniscal pathology in relation to time to surgery. § Several studies have attempted to differentiate patients according to the presence of meniscal injuries on initial MRI, although methodologic shortcomings (eg, extensive or unspecified time between injury and MRI, focus on variables other than operative delay, inclusion of patients who never underwent surgery, and small sample size) limit the generalizability of their findings.7,14,20,22,40 Moreover, Anstey et al 4 found that 80% of meniscal tears discovered arthroscopically occur within the first 2 months after ACL injury, demonstrating that such tears may occur during a much shorter time frame than previously recognized.
In the current study, we compared the incidence of “new” meniscal tears associated with delayed ACL reconstruction in adult versus pediatric patients, using early, initial MRI findings to isolate these new meniscal tears—that is, those not sustained with the initial injury. We hypothesized that delayed surgery would be associated with a significant risk of secondary meniscal injury in both adult and pediatric patients and that the risk would be greater in pediatric patients.
Methods
Patient Selection and Data Extraction
Institutional review board approval was waived for this retrospective cohort study. We searched electronic medical records from our academic tertiary care center to identify all patients who underwent primary ACL reconstruction (Current Procedural Terminology code 29888) between October 1, 2013, and January 31, 2022. We excluded patients with a history of ipsilateral knee injury, degenerative meniscal tears, unknown date of injury, unknown MRI date or findings, and/or concomitant knee injuries (intra-articular fracture, patellar dislocation). Because MRI findings were used as a surrogate for intra-articular pathology at the time of initial injury, it was important to include only MRI scans that were performed soon (ie, ≤3 weeks) after the injury date. We also controlled for time from injury to MRI in a subsequent multivariate analysis. To limit the evaluation to ACL tears without extensive chronicity, we excluded patients whose time from MRI to surgery was ≥52 weeks, as done previously by Kolin et al 24 and Church and Keating. 8
Of 1332 eligible patients, 790 patients were excluded, leaving 542 patients in the final sample. These patients were classified according to age at the time of surgery as pediatric (<18 years; n = 173) or adult (≥18 years; n = 369) (Figure 1).

Flowchart of patient enrollment. ACL, anterior cruciate ligament; MRI, magnetic resonance imaging.
Data Collection and Primary Outcome
For all patients, we extracted demographic and injury characteristics including age, sex, body mass index (BMI), and ACL injury laterality. Date of injury, date of MRI, and date of index ACL surgery were also collected for each patient. Radiologists’ interpretations of MRI scans were reviewed to determine presence or absence of meniscal tears at the time of injury. Surgeons’ operative reports were reviewed to determine presence or absence of meniscal tears visualized arthroscopically, as well as to determine whether meniscal repair or meniscectomy was performed. We included all meniscal tears observed arthroscopically, regardless of type or severity.
The primary outcome was new meniscal tears, which we defined as tears visualized arthroscopically that had not been previously detected on MRI. Operative delay was defined as ACL reconstruction performed ≥8 weeks after injury. Patients in the pediatric and the adult groups were separately assigned to an “early ACLR” subgroup if they underwent ACL reconstruction <8 weeks after injury and a “delayed ACLR” subgroup if they underwent ACL reconstruction ≥8 weeks after injury.
Statistical Analysis
Patient and injury characteristics were reported as means and standard deviations for continuous data and as frequencies and percentages for categorical data. The incidence of medial and/or lateral meniscal tears was compared between the early and delayed subgroups for each study group at the time of initial MRI and at the time of surgery. Comparison of intraoperative findings was repeated after isolating only new meniscal tears. Normality analysis of continuous variables was conducted using the Shapiro-Wilk test. Student t tests and Mann-Whitney U tests were used for univariate analysis of normally and nonparametrically distributed continuous variables, respectively. The Pearson chi-square test was performed for univariate analysis of categorical variables. Multivariate Poisson regression was performed to calculate the adjusted relative risk (ARR) of new meniscal tears after delayed operative treatment while controlling for age, sex, BMI value, and time to MRI. Significance was determined at P < .05. Data analysis was performed using Stata statistical software, release 17 (StataCorp LLC).
Results
Patient and Injury Characteristics
The mean age at surgery was 15 ± 1.8 years in the pediatric group and 31 ± 10 years in the adult group. The mean time from injury to surgery overall was 9.2 ± 7.2 weeks. Patient characteristics according to group are shown in Table 1. The mean time from injury to MRI was 1.0 ± 0.8 weeks for pediatric patients and 1.1 ± 0.7 weeks for adults, with adults significantly more likely to undergo delayed ACL reconstruction (P < .0001). Most patients (n = 359; 66%) had a meniscal tear that was observed arthroscopically, although less than one-third of these (n = 116; 32%) were new meniscal injuries. There were 36 new medial meniscal tears and 97 new lateral meniscal tears, including 17 patients who had developed both medial and lateral tears by the time of surgery. Among patients who did not have meniscal tears visible on initial MRI, the incidence of new medial meniscal tears was 15% for pediatric patients and 16% for adults, and the incidence of new lateral meniscal tears was 48% for pediatric patients and 34% for adults.
Patient and Injury Characteristics by Study Group a

Data are reported as mean ± SD or n (%). Boldface P values indicate statistically significant difference between groups (P < .05). ACL, anterior cruciate ligament; BMI, body mass index; MRI, magnetic resonance imaging.
Secondary Meniscal Tears
Among pediatric patients, we found no difference in the incidence of medial meniscal tears diagnosed on MRI (P = .12) and diagnosed at surgery (P = .22) between those undergoing early versus delayed ACL surgery (Table 2). However, when isolating new meniscal tears, patients who underwent delayed surgery had a higher incidence of medial meniscal tears diagnosed intraoperatively (P = .004) (Figure 2).
Patient and Injury Characteristics of the Pediatric Patients According to Timing of Surgery a
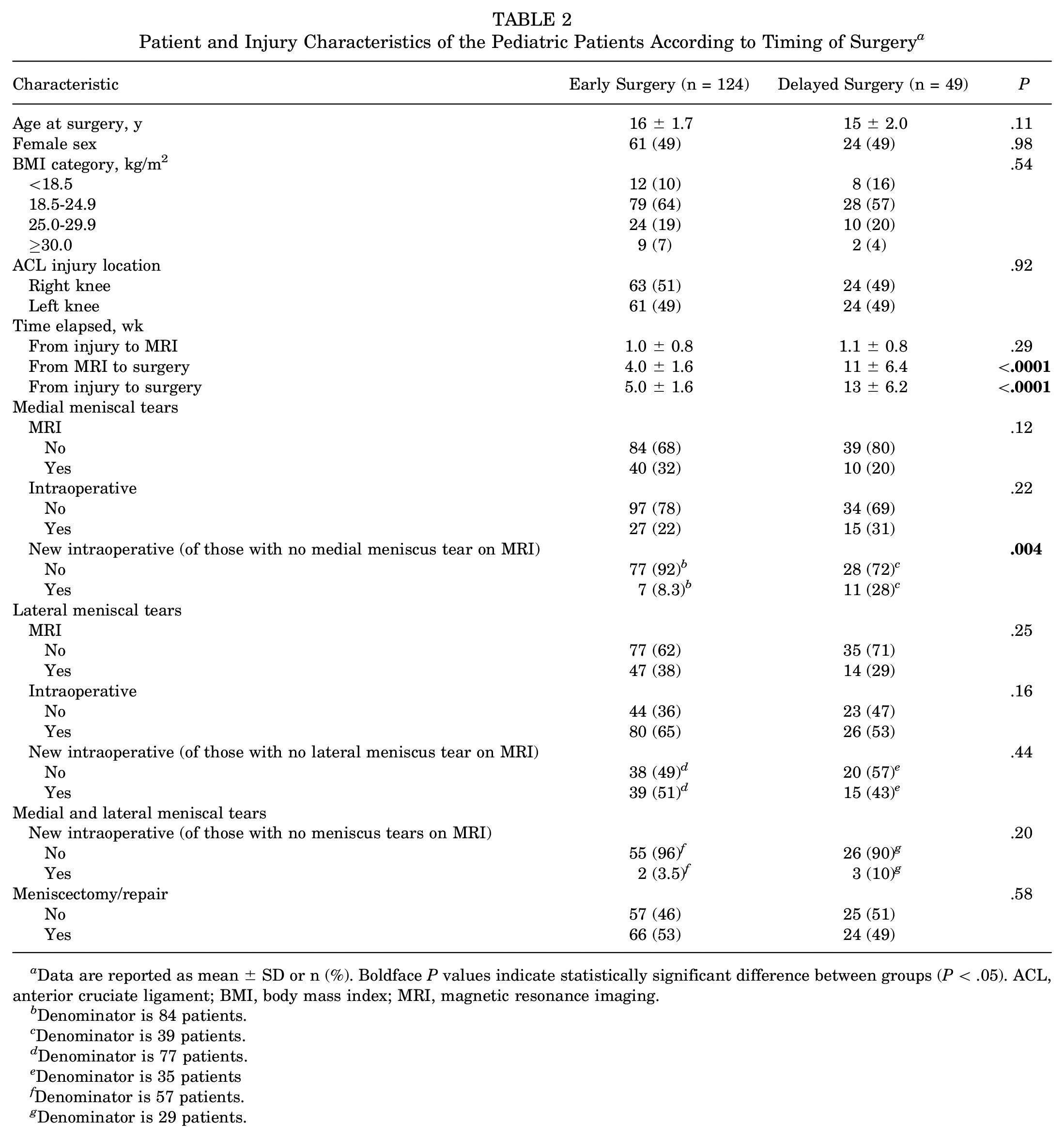
Data are reported as mean ± SD or n (%). Boldface P values indicate statistically significant difference between groups (P < .05). ACL, anterior cruciate ligament; BMI, body mass index; MRI, magnetic resonance imaging.
Denominator is 84 patients.
Denominator is 39 patients.
Denominator is 77 patients.
Denominator is 35 patients
Denominator is 57 patients.
Denominator is 29 patients.

Incidence of new meniscal tears for (A) pediatric patients and (B) adult patients, by operative delay. *Statistically significant difference between groups (P < .05).
In contrast, we found no difference in the percentage of patients with concomitant lateral meniscal tears at the time of ACL injury as seen on MRI in the early group (38%) versus the delayed group (29%) (P = .25); no difference in the incidence of lateral tears observed intraoperatively in the early group versus the delayed group (P = .16); and no difference in new lateral tears in the early group versus the delayed group (P = .44) (Table 2). On multivariate Poisson analysis, delayed ACL reconstruction was associated with higher risk of new medial (ARR, 3.9; 95% CI, 1.5-10), but not new lateral (ARR, 0.8; 95% CI, 0.4-1.5), meniscal tears (Figure 3). The incidence of new combined medial and lateral meniscal tears did not differ significantly between the group with delayed operative treatment (10%) versus early operative treatment (4%).

Adjusted relative risk of developing new meniscal tears after delayed anterior cruciate ligament reconstruction among pediatric and adult patients. Even when controlling for covariates, operative delay was associated with a significantly greater risk of new medial meniscal tears in pediatric, but not adult, patients. Bars represent 95% CIs.
Among adults, a different pattern was observed. Delayed ACL reconstruction was not associated with a higher incidence of medial, lateral, or combined medial and lateral meniscal tears at the time of initial MRI or at the time of surgery (Table 3). This finding persisted even when analyzing only new meniscal tears (Figure 2). On multivariate regression, operative delay was still not associated with greater risk of new medial (ARR, 1.1; 95% CI, 0.6-2.2), new lateral (ARR, 1.2; 95% CI, 0.8-1.9), or new combined medial and lateral (ARR, 1.5; 95% CI, 0.5-4.8) meniscal tears in adults (Table 4).
Patient and Injury Characteristics of the Adult Patients According to Timing of Surgery a

Data are reported as mean ± SD or n (%). Boldface P values indicate statistically significant difference between groups (P < .05). ACL, anterior cruciate ligament; BMI, body mass index; MRI, magnetic resonance imaging.
Denominator is 125 patients.
Denominator is 106 patients.
Denominator is 127 patients.
Denominator is 108 patients
Denominator is 86 patients.
Denominator is 82 patients.
Multivariate Risk of Developing New Meniscal Tears after Delayed ACL Reconstruction in Pediatric and Adult Patients a

Boldface P value indicates statistical significance (P < .05). ACL, anterior cruciate ligament; ARR, adjusted relative risk.
Discussion
In this study, we analyzed the risk of meniscal tears after delayed ACL reconstruction in pediatric and adult patients by differentiating new meniscal tears (those discovered arthroscopically) from those present on initial MRI. By analyzing only patients who underwent MRI shortly after ACL injury with no apparent meniscal tears, we identified the incidence of new medial meniscal tears as 15% for pediatric patients and 16% for adults, and the incidence of new lateral meniscal tears as 48% for pediatric patients and 34% for adults. We also found that pediatric patients undergoing delayed surgery had a higher risk of new medial but not lateral meniscal tears. This did not hold true for adults, who had no greater risk of new meniscal tears associated with operative delay. Our findings suggest that delayed ACL reconstruction may be acceptable in the less active and less injury-prone adult population, but not in children and adolescents.
The risks we found for new medial versus lateral meniscal tears in pediatric patients agree with what is known about the kinematics of the knee joint. The medial meniscus serves as a secondary stabilizer in the ACL-deficient knee and is susceptible to injury with chronic ACL deficiency.2,9,16 Interestingly, new medial meniscal tears occurred at a much higher rate in the operative delay group (28%) compared with the early operative group (8.3%) among pediatric patients (P = .004). This finding suggests an advantage of early ACL reconstruction in pediatric patients. Many studies that have associated delayed ACL reconstruction with meniscal tears have relied solely on intraoperative findings and analyzed the overall incidence of meniscal tears in relation to time to surgery. ‖ Other studies that did differentiate patients according to the presence of meniscal tears on initial MRI were limited by methodologic shortcomings.7,14,20,22,40 Kolin et al 24 reported that each week of delay from ACL injury to surgical reconstruction was associated with a 3% increase in the risk of intraoperative medial meniscal tears among pediatric and adolescent male patients, although they did not isolate patients with intact menisci on postinjury MRI. Guenther et al 20 did stratify patients according to the presence of meniscal tears on MRI and found that a longer interval between injury and surgery (>1 year) was associated with a greater likelihood of new or worsened medial, but not lateral, meniscal tears in adolescents. However, the mean time from injury to MRI was 77 days (range, 1-377 days), so MRI findings could no longer be considered representative of initial injury pattern. 20 To our knowledge, Anstey et al 4 used the earliest cutoff time for MRI at ≤2 months after injury, yet they still found that 80% of meniscal tears discovered arthroscopically were already detectable on MRI, suggesting that even earlier imaging may be useful.
In contrast, despite the high overall incidence of new lateral meniscal tears, we found no difference in risk of lateral tears between pediatric patients who underwent early versus delayed ACL reconstruction. Previous studies have demonstrated that lateral meniscal tears are associated predominantly with acute ACL injury and, unlike medial meniscal tears, are not associated with chronic instability.9,30 However, the exact timing of secondary lateral meniscal tears has not been well described. Our data suggest that lateral meniscal tears occur early during the acute post–ACL injury period. Specifically, most lateral tears in pediatric patients may occur after 1 week (mean time to MRI) but before 7 to 8 weeks (mean time to surgery). Conversely, the medial meniscus deteriorates in the setting of chronic instability, and most tears likely developed after 8 weeks, which would explain why few were seen arthroscopically in patients who underwent surgery before this time point.
Among adults, we did not detect greater risk of new medial or lateral meniscal tears after delayed ACL reconstruction, despite the larger sample size. Stone et al 39 similarly reported that ACL reconstruction between 90 days and 1 year after injury in adults aged ≥40 years was not associated with a higher rate of intraoperative meniscal tears. This finding might reflect a greater degree of awareness, caution, and responsibility in adults, who may be more likely than children and adolescents to protect their deficient knee from further injury. This explanation is consistent with studies showing that protection of the ACL-deficient knee decreases the risk and severity of meniscal injury.3,24 Our findings suggest that, when needed, short-term delay in ACL reconstruction with appropriate protection of the knee may be acceptable in adults without increasing their risk of meniscal tears.
Limitations
This study has several limitations. First, selection bias is likely present, as surgeons may be more likely to operate soon after injury in patients with more severe knee injuries. However, even if present, this bias would make it less likely to observe a higher risk of meniscal tears in the delayed treatment group because the delayed group would be associated with less severe injury. Therefore, this limitation should not undermine our findings of greater risk of medial meniscal tears in the pediatric population with operative delay but may mask a greater risk of meniscal tears with operative delay in adults. As such, the absence of a higher rate of new meniscal tears in adults should be considered in light of possible observational biases. Nonetheless, the association between operative delay and medial meniscal tears among pediatric patients but not adults suggests that, at a minimum, the association, if present, is much weaker in the adult population. Second, because it is difficult to ascertain the use of crutches, braces, and physical therapy from clinical notes, we were unable to evaluate the association of such measures with the risk of new meniscal tears. Thus, it remains unknown whether the use of nonoperative interventions would modify our findings. Similarly, level of continued activity after ACL injury is likely a major contributor to the development of secondary intra-articular pathology, although its contribution is challenging to quantify within a retrospective study.
A third limitation is that MRI has imperfect sensitivity (78%-89%) and specificity (88%-95%) for detection of meniscal tears, 33 and the quality of MRI interpretation was subject to variability between examiners. Because we relied primarily on radiologists’ and/or surgeons’ original interpretations of MRI images, we were unable to control for intra- or interobserver reliability. Meniscal tears that were missed on initial MRI could have led us to overestimate the incidence of new meniscal tears in some cases. Fourth, we assumed that meniscal tears present on MRI corresponded to tears present at initial injury; however, some may have been new tears that developed between the initial injury and the MRI scan. We adapted our selection criteria and analysis to control for this possibility by including only patients who underwent MRI within 3 weeks after ACL injury and by controlling for time to MRI on multivariate analysis. (The mean time from injury to MRI was approximately 1 week for both groups.) Still, meniscal injuries occurring during this short period may have led to underestimation of the incidence of new tears. Finally, different definitions of operative delay are possible. Given that the mean time from injury to surgery in our patients was 9.2 weeks, we chose a threshold of 8 weeks, and our findings may not be generalizable to longer or shorter periods of operative delay.
Conclusion
We evaluated the risk of secondary meniscal tears after delayed ACL reconstruction in pediatric and adult patients by isolating new intraoperative meniscal tears that were absent on early, initial post–ACL injury MRI. Our findings suggest that delaying ACL reconstruction may be acceptable in adults, who may be less active and less injury-prone than children and adolescents. We hope these findings prompt future studies to assess the risk of new meniscal tears with delayed ACL reconstruction by excluding injuries present on postinjury MRI, rather than including all tears present at the time of surgery.
Footnotes
Acknowledgements
The authors thank Denise Di Salvo, MS, and Rachel Walden, MS, in the Editorial Services Group of The Johns Hopkins Department of Orthopaedic Surgery for editorial assistance.
Final revision submitted May 24, 2023; accepted July 31, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: R.J.L. has received education payments from Arthrex and hospitality payments from Vericel. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by Johns Hopkins Medicine (No. IRB00301240).