
Abstract
Background:
The exponential rise in arthroscopy for femoroacetabular impingement (FAI) has led to increased revision surgery rates, although this is often an exclusion criterion from arthroscopy literature.
Purpose:
To examine the midterm (minimum 5-year follow-up) outcomes after revision arthroscopic correction of FAI compared with a matched control group of primary surgical cases.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Prospective outcome data, collected in a consecutive series of patients undergoing revision arthroscopic FAI correction, was retrospectively reviewed. Revision procedures were compared with a matched group of primary surgical cases. Survivorship was defined as the avoidance of total hip replacement (THR) and assessed using a Kaplan-Meier curve with the log-rank test. Regression analysis was conducted to identify predictors of THR conversion. Patient-reported outcomes (PROs) including modified Harris Hip Score (mHHS), University of California, Los Angeles (UCLA), 36-Item Short Form Health Survey (SF36), and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) preoperatively and at 5 years postoperatively were compared between the groups. The proportion of patients across groups achieving the minimal clinically important difference (MCID) was compared for each PRO. Finally, a subgroup analysis was performed to compare the outcomes of those who had their index surgery at our clinic and those who had an index procedure elsewhere.
Results:
A total of 124 revision cases were compared with 268 primary cases. The most common indication for revision surgery was residual bony deformity. Both groups had high survivorship rates at 5 years (>90%) although revision cases did have a statistically higher conversion to THR than did primary cases (6.5% vs 1.5%; P = .008). Increasing age and revision surgery were identified in regression analysis as predictors for THR conversion. Where THR was avoided, improvements in PROs were observed in both groups (P < .05 for all). Before surgery, revision cases reported lower scores for all PROs. At 5 years, the only statistical difference between the groups was in the distribution of mHHS scores. There were no differences in the rate of MCID achievement between groups.
Conclusion:
Residual bony deformity is the most common indication for revision arthroscopy. Revision procedures may have a lower survival than primary cases, although overall survivorship at midterm follow-up is high. Of the revision cases, 17% required further arthroscopy. Where THR is avoided, improvements in pain and function can be expected that are similar to primary surgical cases.
Keywords
Femoroacetabular impingement (FAI) is a debilitating hip condition arising from pathological bone growth on the femoral head-neck junction (cam impingement) and/or the acetabular rim (pincer impingement). 11 These deformities disrupt fluid movement of the femoral head into the acetabulum during motion. Over time, this leads to progressive damage to the labral tissue and articular cartilage, culminating in pain and stiffness during activities of daily living and more vigorous physical activity. 6 The condition is common in young adults and diagnosed with a triad of clinical signs, patient history, and radiological indications of bony deformity. 12 Although the natural history of FAI is still being examined, consensus is that prolonged injury to the intra-articular tissues results in development of early osteoarthritis of the joint.2,15 Improvements in imaging and surgical techniques, particularly arthroscopy, have led to an exponential rise in surgical treatments for hip disorders including FAI. 3 Hip preservation surgeries, which involve removal of bony deformities and repair of the natural intra-articular tissue, is a successful treatment for patients in the short, medium and longer term. 4 As the number of surgeries rise, there is a corresponding increase in revision procedures. 30 Revision surgery is often cited as an exclusion criterion in arthroscopy literature and, as such, the outcomes for this cohort are less well reported on. Some studies have been conducted, however, and studies included in a systmatic review with meta-anlaysis indicate improvements in this cohort following revision surgery, although they may still report higher levels of pain and dysfunction compared with primary cases. 29 As time progresses, the mid- to long-term outcomes of revision cases need to be quantified.
The aim of the study was to determine the 5-year outcomes, including total hip replacement (THR) conversion rates and changes in patient-reported outcomes (PROs) of revision procedures, compared with primary hip arthroscopy cases. The hypothesis was that those undergoing revision surgery would have a lower survivorship and poorer PROs compared with primary arthroscopy patients.
Methods
Patient Selection
Ethical approval was granted by the Medical Advisory Committee (MAC) to review data collected as part of the institutional hip arthroscopy registry within clinic. The MAC is responsible for clinical and medical governance related to issues on behalf of the hospital. All hip arthroscopies conducted by the senior author (P.C.) between January 2009 and December 2017 with minimum 5-year follow up were considered (Figure 1). Patients were divided into 2 categories: revision cases (study group) and matched primary cases with no repeat hip arthroscopy during the study period (control group). Cases were matched by sex, Tönnis grade, and capsular repair. Cases were excluded if they presented with Tönnis grade >1, lateral center-edge angle <25o, avascular necrosis, or Protrusio. Protrusio was diagnosed by the senior author on anteroposterior radiographs if the femoral head was considered to encroach on the ilioischial line. Revision cases were removed from the primary group to avoid being matched with themselves. Bilateral cases in which the patient belonged to both groups were also removed.
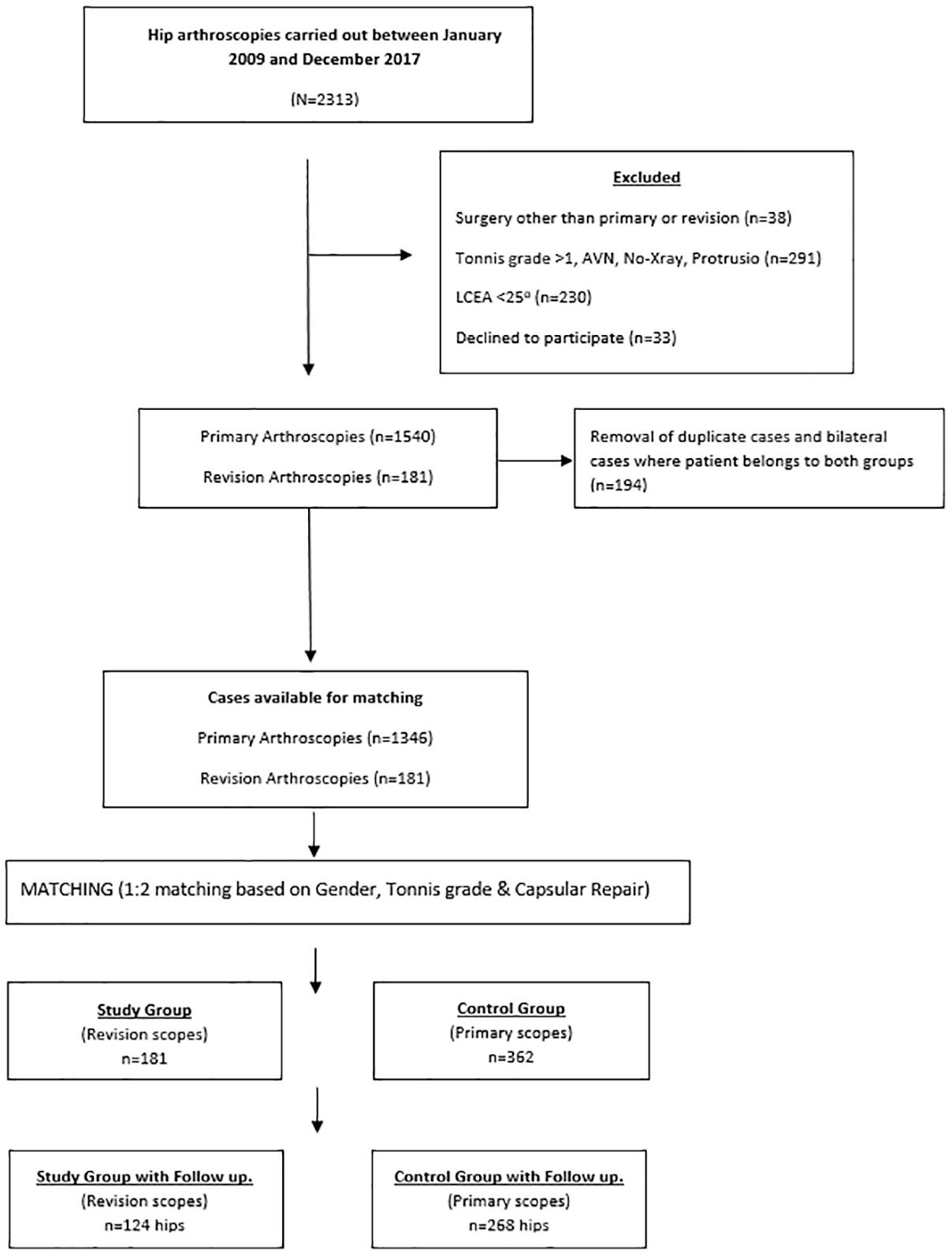
Flowchart of patient selection. AVN, avascular necrosis; LCEA, lateral center-edge angle.
Surgical Procedure
Patients were placed in the supine position and following distraction, anterolateral and modified anterior portals were created. These were used to access the joint by creating a limited interportal capsulotomy. Correction of pincer deformities was carried out initially. This was achieved by surgically reflecting the acetabular labrum from the rim and resecting the abnormal underlying bone using a 4.5-mm mechanical burr under radiographic guidance. The labrum was refixed to the rim, using 2 suture anchors. 5 Cam deformities were resected using a 5.5-mm mechanical burr. Capsular repair was not undertaken at the beginning of this hip registry and only became routine in 2013, and so not all cases underwent capsular repair. In no case was microfracture undertaken. In the clinic, postoperative radiographic images were collected on day 1 postsurgery before patient discharge. Patients were then provided with a standard rehabilitation protocol that lasted 12 weeks, to be carried out at home. Postoperatively, patients were mobilized 4 hours following the procedure and ambulation was allowed as comfortable on day 5. Hydrotherapy was permitted after stitches were removed on day 10. Running was permitted at week 6, with sprinting as comfortable on week 8.
Surgical Outcomes
Patients were contacted via telephone ≥5 years postsurgery (post–revision surgery in revision cases) and invited for review. In the telephone follow-up, it was determined whether avoidance of THR was acheived (survival) or if further arthroscopic procedures were necessary. If phone contact was not possible, hospital records were consulted for this determination. Where patients declined a review in clinic, they were provided with a copy of the outcomes via the postal service. Secondary outcomes (PROs) were collected using the modified Harris Hip Score (mHHS), University of California, Los Angeles, activity scale (UCLA), the 36-Item Short Form Health Survey (SF-36), and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). The mHHS is the most expansively used outcome measure in FAI research and heavily influenced by daily pain. The UCLA activity scale quantifies sporting engagement ranging from total inactivity to full involvement in competitive sports. The WOMAC has also formed the basis of more recent FAI specific outcome measures (including the international Hip Outcome Tool, the Copenhagen Hip and Groin Outcome Score [HAGOS], and the Nonarthritic Hip Score) and quantifies both pain and stiffness. Finally, the SF-36 is one of the most versatile and widely used international health and well-being questionnaires, fulfilling roles in outcome measurement across an enormous number of medical and surgical specialties, and has been used to assess the construct validity of the HAGOS, Hip Outcome Score, and Hip disability and Osteoarthritis Outcome Score.18,22,31 Combining these tools gives a comprehensive evaluation of patient status with high reliability over time. As not all revision cases had their index surgery at our clinic, their preoperative PROs were those collected before their revision surgery at our hospital.
Statistical Analysis
The primary outcome of the study was survivorship, as defined by the avoidance of THR. A priori power analysis was conducted using independent-sample proportions and based on previously reported THR rates for revision cases. 21 For 80% power at a significance level of .05 with a 1:2 matching ratio, it was determined that a minimum of 117 cases in the revision group and 234 cases in the control group would be required. Case-control matching using SPSS software was applied with exact matching for sex, Tönnis grade, and capsular repair.
Survival between the 2 groups was assessed using a Kaplan Meier curve and log-rank (Mantel-Cox) test. A regression analysis was undertaken to establish if any characteristics were predictive of failure in the revision group. All potential variables likely to predict success or failure were included in a bivariate regression analysis, and any statistically significant variables were then included in a multivariate forward stepwise regression analysis. The variables included in the analysis were group, age, lateral center-edge angle, alpha angle, sex, capsular repair, surgical approach to the labrum, and Tönnis grade.
Secondary outcomes consisted of the PROs. Patients who underwent bilateral operative procedures were instructed to complete the PRO relative to each hip, and as such each hip was treated as an independent case. Normality was assessed using the Shapiro-Wilk test, which indicated that the PRO scores were not normally distributed. The Wilcoxon signed-rank test was therefore used to analyze the difference between baseline and postoperative PRO scores for both groups. Group comparisons between PRO scores at baseline and 5-year follow-up were conducted using the nonparametric Mann-Whitney U test. The minimal clinically important difference (MCID) was determined for each PRO using a distribution method (0.5*change in PRO score from baseline to follow up) to identify the threshold for improvement and determining the percentage of cases in each group that exceeded the threshold at follow-up. 27 The percentages of cases between the groups who achieved MCID were assessed using a chi-square analysis.
A subanalysis was conducted to determine the outcomes of revision cases where the index surgery was carried out at another institution in comparison with those where index surgeries were undertaken at our institution. A subanalysis was also conducted to examine the rate of THR or further arthroscopy between revision cases whereby the labral tissue was excised or reconstructed compared with those who had a labral repair or debridement.
Results
A total of 124 revision cases were included in the analysis (115 patients). Of these, 48 cases had their index procedure at another institution. The mean follow-up for the revision group was 62 ± 2 months, while the mean follow-up for the primary group was 69 ± 6 months. For comparison, 268 primary scope cases were included (230 patients). Comparisons between baseline demographics of those who responded to follow-up and those who did not are shown in Appendix Table A1. Those who did not respond to the review and were younger than those who did had a higher proportion of male participants and a higher proportion of capsular repair. The demographics for the revision and primary cases are reported in Table 1. The decision to undertake revision surgery was based on continued symptoms, clinical examination, patient consultation, and radiographic imaging. The indications for revision surgery are detailed in Table 2. The revision group had a higher preoperative alpha angle and a higher incidence of labral debridement and excision compared with the primary group, the majority of which had a labral repair. Four of the revision cases that had no viable labral tissue had a labral reconstruction using a hamstring graft. Changes in radiographic parameters following surgery are reported in Table 3.
Patient Demographics a

NS, not significant.
Indications for a) Revision Surgery and b) Further Arthroscopy in Revision Cases

Radiographic Parameters a

Data are shown as mean ± SD. Bold values indicate a statsitcally significant finding. ES, effect size. NS, not significant.
Survivorship and Regression Analysis
A total of 21 cases in the revision group required a third arthroscopy (17%), the reasons for which are detailed in Table 2. The mean time to further surgery was 22 ± 12 months. Eight cases (6.5%) had converted to THR by 5 years at a mean of 15 ± 8 months following revision surgery. In contrast, 4 (1.5%) cases in the primary group converted to THR at a mean of 30 ± 22 months, which was a statistically lower conversion rate (P = .008) compared with the revision group. The differences in survival between the groups are illustrated in Figure 2. Revision surgery and age at the time of surgery were identified as predictive of THR conversion. For every unit increase in age at the time of surgery, the likelihood of THR increased by 1.13 (95% CI, 1.060-1.204; P < .001). Seven times increased likelihood of THR conversion for those undergoing revision surgery compared with primary scopes was observed (95% CI, 1.931-26.566; P = .03).

Differences in survival between revision and primary cases.
PROs and MCID
Before revision surgery, revision patients reported statistically lower scores mHHS, UCLA, SF-36, and WOMAC than primary surgical cases, all of which were small in magnitude. At 5 years, the only difference between the groups was the distribution of mHHS scores, which was lower in the revision group, although this difference was also small in magnitude (Table 4). The full complement of PRO scoring before and at 5 years is reported in Table 4. The threshold for MCID for the mHHS was 9 points, UCLA 2 points, SF-36 9 points, and WOMAC 8 points. There was no difference in the rate of MCID achieved between revision and primary cases for any PRO (Table 5). MCID achievement ranged from 53% to 73% of cases.
PRO Scores for Revision and Primary Cases a
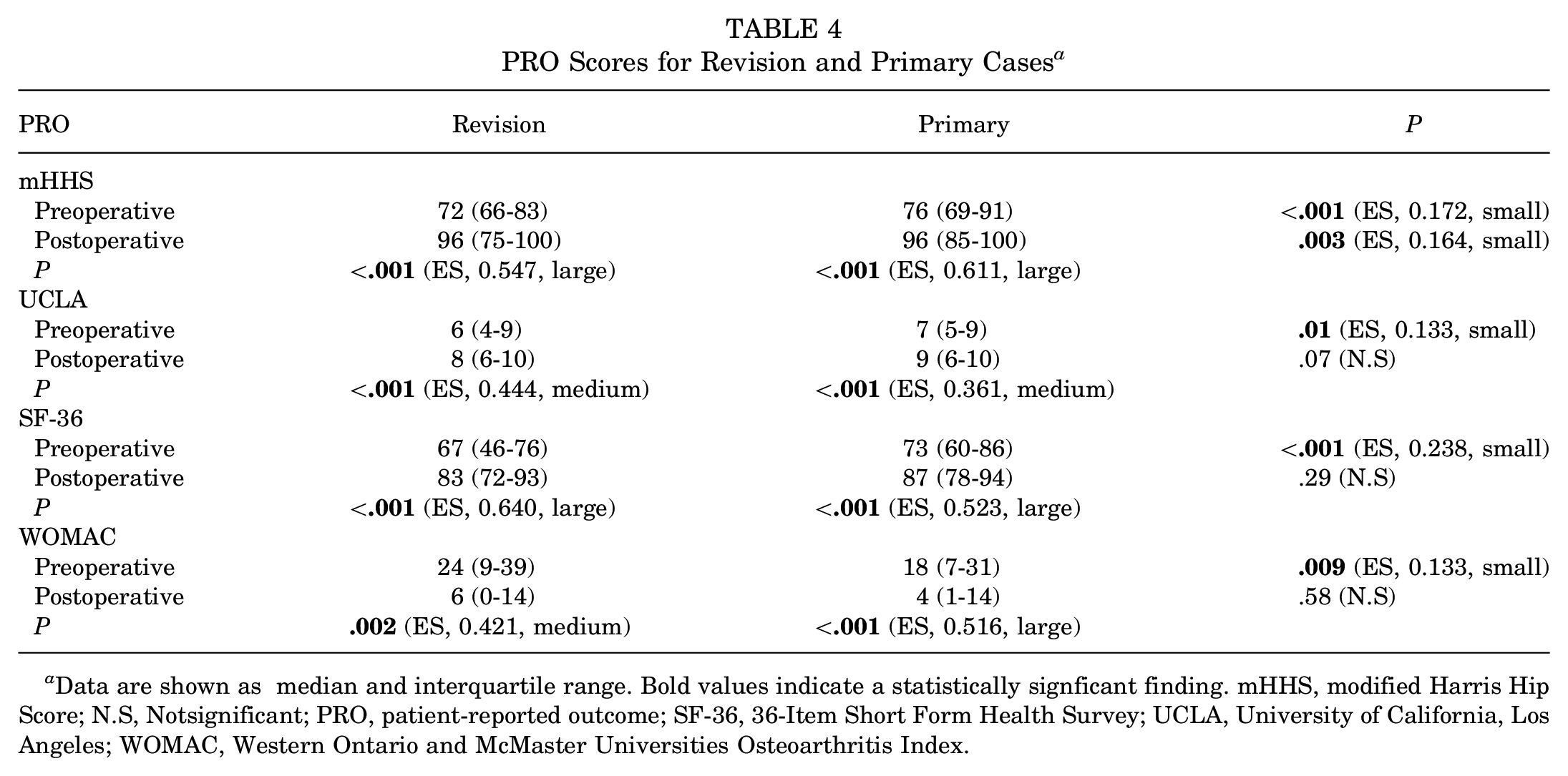
Data are shown as median and interquartile range. Bold values indicate a statistically signficant finding. mHHS, modified Harris Hip Score; N.S, Notsignificant; PRO, patient-reported outcome; SF-36, 36-Item Short Form Health Survey; UCLA, University of California, Los Angeles; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
MCID Achievement a

MCID, minimal clinically important difference; Data is presented as percentage of those achieving or not acheiving MCID; mHHS, modified Harris Hip score; N.S, Not significant; PRO, patient-reported outcome; SF-36, 36-Item Short Form Health Survey; UCLA, University of California, Los Angeles; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Revision Case Subanalysis
A subanalysis of revision cases between those who had their index surgery at our clinic (n = 76) and those who had the initial procedure elsewhere (n = 48) was undertaken. Before revision, cases in which the index procedure was carried out at another institution had significantly larger preoperative alpha angles (72 ± 18 vs 61 ± 19; P = .002; ES, 0.274, small). This between-group difference was maintained following revision surgery (60 ± 18 vs 51 ± 15; P = .007; ES, 0.247, small). There was no difference between the groups for the lateral center-edge angle either before (34 ± 5 vs 35 ± 8; P = .46) or following (32 ± 7 vs 31 ± 7; P = .26) revision surgery. Preoperatively, those coming from other institutions had significantly poorer WOMAC scores (33 vs 19; P = .02; ES = 0.207, small). At 5 years, there was no difference between subgroups for any PRO. There was no difference in the survival rate between subgroups at 5 years (P = .92), although those coming from other institutions had a higher rate of further arthroscopy than revision cases that had their index surgery at our clinic (35% vs 12%; P = .007; ES, 0.284, small). A chi-square analysis was also conducted to determine the differences between cases with labral repair/debridement compared with excision/labral reconstruction with respect to THR conversion and further arthroscopy. There was no difference in the proportion of cases who converted to THR or further arthroscopy between labral excision/graft and repair/debridement (P = .86). There were also no differences between these groups for any PRO (P > .05 for all).
Discussion
The aim of the study was to determine the 5-year outcomes, including THR conversion rates and changes in PROs of revision procedures compared with primary hip arthroscopy cases. The results indicate a greater conversion to THR in revision cases at 5 years. Of revision cases, 17% required further arthroscopy. Where THR was avoided, improvements in PROs were observed. Despite revision cases’ reporting inferior PRO scores before surgery, there was no difference in PRO scoring at 5 years except for the distribution of the mHHS. Any statistically significant differences between the groups for PROs at either time point were small in magnitude as denoted by small effect sizes. Most cases in both groups achieved MCID for each PRO. Age at the time of surgery and revision were predictive of THR conversion.
The results of the study support the previous research published with short-term follow-up and are encouraging for long-term survival of the hip joint. The THR rate observed here (6.5%) is comparable with that reported by some previous studies that have ranged from 0% to 14.3%.1,7,9,13,14,19,32 The mean time to THR in the current study was 15 months. In a similar cohort with 12-month follow up, Mygind-Klavsen and colleagues 24 reported a 6.4% conversion to THR within 12 months of revision arthroscopy. Revision procedures, therefore, have the potential to deteriorate relatively quickly. In one of the few studies with a similar follow-up time to that reported here, Maldonado et al 21 reported a conversion to THR and/or hip resurfacing rate of 15% (with a relative risk of 2.7 at 5 years), which is significantly higher than reported in our study. Their study had a predominantly female cohort. Female sex has been identified previously as a risk factor for THR conversion. 34 In contrast, most cases in the current study were male, reflecting the footfall through the clinic. In this instance, age and revision surgery were identified as risk factors for THR conversion in regression analysis.
The decision to undertake revision surgery is based on unresolved symptoms, clinical factors, and radiographic findings identifiable during diagnostic workup. Similar to previous studies, residual bony deformity was the main indication for revision procedures, as demonstrated by higher alpha angles in the revision group. In the revision group, 17% underwent a further arthroscopy, which is higher than that previously reported. 29 Capsular plication was the most common indication for further surgery. Advances in surgical technique may account for this. The capsuloligamentous complex that surrounds the hip joint provides stability and limits extension and external rotation, which in turn resists anterior translation and subluxation of the femoral head. Increased proprioception provided by this complex increases overall function of the hip joint. Capsular closure and/or capsular plication following surgery is advised to restore or improve capsular tension and improve stability of the joint. 8 Before 2013, capsular repair following arthroscopic surgery was not routine at the clinic. It should be noted, however, the capsulotomy used by the senior author is a limited interportal capsulotomy, which is much less invasive than a T-capsulotomy. Repairing the capsule will improve overall stability of the joint and may reduce the need for repeated arthroscopies. Our previously published data, however, have indicated that, in the absence of an interportal repair, patients exhibit similar improvements following surgery to those with a repair. 10 Patients in this cohort, however, were matched by capsular repair ensuring an even distribution of those with and without repair across both groups.
The goals of hip preservation are to sustain the natural structure of the joint for as long as possible while alleviating symptoms associated with hip pathology. In the current paper, revision cases had poorer labral tissue quality than primary cases, resulting in higher rates of excision and debridement than primary cases. The lack of labral tissue has previously been associated with increased risk of joint deterioration and inferior outcomes. 16 Labral reconstruction has been developed to address this problem. The outcomes of labral reconstruction show improved symptoms in revision cases, although they are still lower than primary arthroscopies.17,33 Locks et al 20 examined revision following labral reconstruction with 2-year follow-up. There was a 14% THR rate mostly in female patients; where THR was avoided, improvement in PROs was observed, which was similar to the control group at 2 years. In the current series, a total of 19% of revision cases required excision of a poor-quality labrum and 4 of these cases (3.2%) underwent labral reconstruction. When a subanalysis of revision cases was undertaken comparing those with preservation of the natural labrum (repair/debridement) versus excision/reconstruction, there were no differences with respect to THR conversion, further arthroscopy rates, or PROs at 5 years. This may indicate that providing all residual deformity is corrected, adhesions are resected, and the capsule is rebalanced, patients will have a similar, good outcome whether the labrum is of good quality and preserved (repaired/debrided) or poor quality and resected (excised/reconstructed). Although, for those revision cases where a previous labral excision was undertaken, a newly formed “pseudolabrum” can be clearly observed covering the acetabular rim and therefore may retain some of the original labral functions (sealing and stability).
Irrespective of what tool is used, PROs give an important benchmark of hip function and pain levels during activities of daily living and with more vigorous activity. Supporting previous literature that has included primary cases as a comparison, the current study indicates that before surgery, revision cases reported inferior levels of hip function during activities of daily living and physical activity.23,25,26 It is important to note, however, that any differences in PRO scoring between the groups reported here either at baseline or at follow-up were small in magnitude. Furthermore, these differences were within the MCID thresholds, indicating that differences, although statistically significant, may not be clinically relevant. The MCID is a commonly used metric in clinical literature used to determine the smallest change that would be worthwhile to the patient. In 2018, Nwachukwu et al 28 quantified the MCID in a group of revision patients without a control arm. As well as improvements in raw scoring for PROs, the authors reported that 65% of patients achieved MCID for the Hip Outcome Score Sports-Specific subscale score. The authors did not provide the percentage of patients who achieved MCID for the other PROs used. A similar proportion of cases in the current study achieved MCID for the UCLA, a measure of physical activity. Additionally, most cases achieved MCID for all metrics used with no statistical difference between revision and primary cases with respect to MCID achievement.
Limitations
There are some limitations of the study which must be considered. This is a retrospective analysis; however, all outcomes were collected prospectively throughout the study period. Lost follow-up was observed in our study; however, there were no differences between cases lost to follow-up and reviewed cases with respect to radiological parameters or baseline pain and function levels. This indicates that those who were not reviewed are unlikely to have deteriorated to a greater extent than those who were reviewed. There was also no difference in the rate of lost follow-up between revision and control cases. All cases in the study were operated on by a single high-volume hip surgeon (P.C.), and while this may limit the generalizability of the results, it does add consistency to the surgical treatment. There are newer PROs in hip arthroscopy literature that were not included here. All PROs used in this study are well-established, validated measures of hip-specific function, activity level, and general health, with high sensitivity and specificity. Radiological assessment was not undertaken at the 5-year period, which would have given more information on the progression of hip osteoarthritis.
Conclusion
Residual bony deformities were the most common indication for revision procedures. High survival rates are observed in this cohort at 5 years, although they may display a higher conversion to THR than primary cases. If further surgical procedures can be avoided, revision cases show improvements in pain and function and achieve the MCID at a similar rate to primary cases.
Footnotes
Appendix
Demographics of Followed-up Cases and Lost to Follow-Up Cases a

| Variable | Followed-up (n = 392) | Lost to Follow-up (n = 151) | P |
|---|---|---|---|
| Sex, % | |||
| Male Female |
74 26 |
88 12 |
<. |
| Tönnis grade, % | |||
| 0 1 |
78 22 |
82 18 |
.27 (NS) |
| Surgical treatment of the labrum, % | |||
| Excision Debridement Repair |
12 10 78 |
5 9 86 |
.09 (NS) |
| Capsular repair, % | |||
| No repair Repaired |
33 67 |
6 94 |
<. |
| Age at surgery, y | 32 ± 10 | 28 ± 9 | <. |
| Preoperative alpha angle, deg | 61 ± 19 | 61 ± 17 | .53 (NS) |
| Preoperative lateral center-edge angle, deg | 34 ± 6 | 34 ± 7 | .53 (NS) |
| Preoperative mHHS | 76 (68-86) | 76 (70-86) | .34 (NS) |
| Preoperative UCLA | 6 (5-9) | 6 (5-9) | .92 (NS) |
| Preoperative SF-36 | 71 (57-83) | 71 (56-83) | .78 (NS) |
| Preoperative WOMAC | 19 (8-34) | 16 (7-29) | .23 (NS) |
Data are presented as mean ± SD or median (interquartile range). mHHS, modified Harris Hip Score; SF-36, 36-Item Short Form Health Survey; NS; not significant; UCLA, University of California Los Angeles score; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Final revision submitted July 16, 2024; accepted July 18, 2024.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from UPMC Whitfield Hospital.