
Abstract
Background:
Femoroacetabular impingement syndrome (FAIS) is frequently treated arthroscopically with osteoplasty and labral repair. Surgical preferences vary in terms of equipment, technique, and postoperative protocol. Patient-reported outcome measures (PROMs) are valuable tools to assess outcomes across different institutions.
Purpose:
To compare PROMs after FAIS arthroscopy and evaluate the impact on postoperative outcomes with independent surgeons utilizing different surgical techniques and postoperative protocols.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
Prospective data were collected from patients with a 2-year follow-up after arthroscopic FAIS treatment by 2 orthopaedic surgeons from different states, each attending different sports medicine fellowships. Patients were matched according to age, sex, and body mass index. Data included patient characteristics, surgical findings, and the Hip disability and Osteoarthritis Outcome Score (HOOS) preoperatively and 2 years postoperatively. Patients with revision surgery, concomitant procedures, or incomplete pre- and postoperative data were excluded. Surgeon A utilized interportal capsulotomy, capsular repair, all-suture anchors, and a postoperative hip brace. Surgeon B employed periportal capsulotomy without repair, polyether ether ketone suture anchors, and no brace. The 2 high-volume arthroscopists (>100 hips/year) performed osteoplasty and labral repair and used a large perineal post. Cohorts were analyzed with appropriate t tests, with significance set at P < .05. The percentage of patients achieving minimal clinically important difference (MCID) was calculated using Pearson chi-square tests.
Results:
A total of 176 hips (100 women, 76 men) were included, with 88 matched patients from each institution. The mean age was 33.7 years and the body mass index was 26.3 kg/m2. Both cohorts significantly improved in all 5 HOOS subscales 2 years after surgery. When comparing the mean change in PROMs and the percentage of patients achieving the MCID, differences were only observed in the HOOS-Sports subscale (cohort A: 25.3 ± 29.7 vs cohort B: 34.3 ± 29.7; P = .048; MCID achieved in 57% of patients vs 76%; P = .01).
Conclusion:
This prospective cohort study on arthroscopic FAIS treatment indicates that matched patient cohorts from different institutions show similarly improved PROMs at 2 years. This study suggests consistent patient outcomes across sites despite geography, surgeon, training, surgical technique, implants, and postoperative protocol.
Keywords
Femoroacetabular impingement syndrome (FAIS) is a major cause of hip pain and functional impairment, characterized by atypical articulation between the femoral head-neck junction and the acetabular rim.2,15 A modern definition of FAIS was provided by the Warwick Agreement in 2016 and described a triad of symptoms, clinical signs, and radiographic imaging. 18 FAIS incidence and research publications have exponentially increased over the last 2 decades as surgeon education and diagnostic methods have improved.19,20,47 Arthroscopic treatment of FAIS via labral repair and osteoplasty has emerged as the gold standard treatment for adults and adolescents, has led to better patient outcomes when compared with conservative management, and has proven to be cost-effective.1,16,17,21,26,31,33,39,40 The Hip disability and Osteoarthritis Outcome Score (HOOS) is a patient-reported outcome measure (PROM) tool shown to have good psychometric properties and is appropriate for the general population and young adults.13,20,24,38 It is commonly accepted that combining PROM tools, including but not limited to HOOS, with minimal clinically important difference (MCID), helps interpret results and unveil when patients truly improve.14,20,37,43,44
Despite increased utilization of hip arthroscopy for FAIS, there remains a paucity of comparative research investigating the impact of different surgeon training, surgical techniques, postoperative protocols, and geographic locations on postoperative PROMs and MCIDs. These factors could influence the effectiveness of hip arthroscopy and impact outcomes. It has been noted in trauma literature that a lack of homogeneity between different orthopaedic centers’ processes and primary outcome measures, including PROMs, leads to different outcomes and limits interpretation. 32 This sentiment has been echoed in some hip arthroscopy literature, including different surgeons and institutions, which creates heterogeneity and therefore is considered a limitation.3-5,37
The objective of this prospective cohort study is to determine whether postoperative PROMs, as measured by the HOOS score, are associated with surgeon training, surgical technique, postoperative protocol, and geographic location. We hypothesized that there would be no significant difference in HOOS scores despite the above variations. Furthermore, we anticipated that comparable levels of hip-related symptoms, pain, activities of daily living, function in sports, and quality of life would be observed.
Methods
This was a retrospective review of prospectively collected data. Protocols for the study were reviewed and approved by local institutional review boards. Patients undergoing hip arthroscopic surgery for FAIS between December 2014 and June 2021 were included in the study. All patients had positive symptoms, physical examination findings, and imaging consistent with FAIS and had completed appropriate conservative measures (such as activity modification, physical therapy, nonsteroidal anti-inflammatory drugs, and corticosteroid injection) before surgical intervention. To better match cohorts and limit confounding, patients who underwent revision surgery, labral reconstruction, or concomitant abductor repair or did not have complete preoperative and 2-year postoperative data were excluded. We also excluded patients with the following diagnoses: hip dysplasia, synovial chondromatosis, pigmented villonodular synovitis, or inflammatory arthritis. Hip dysplasia was defined as a lateral center-edge angle (LCEA) of <20°. 28
Baseline data included patient characteristics—including age, sex, and body mass index (BMI); preoperative radiographic measurements of the Tönnis grade, the alpha angle, and the LCEA; and preoperative HOOS scores. Routine preoperative imaging included radiographs and magnetic resonance imaging. Computer tomography was performed in select cases when clinically indicated. Intraoperative procedures were recorded, which included labral treatment, femoroplasty, acetabuloplasty/subspine decompression, chondroplasty, microfracture, iliopsoas release, and capsular closure. Traction time was recorded. Patients completed a HOOS score 2 years after surgery.
The patients were divided into 2 cohorts based on surgeon (surgeon A [n = 250], surgeon B [n = 180]). Both were board-certified orthopaedic surgeons but attended different residencies, attended different sports medicine fellowships, and practiced in 2 different states. Both surgeons currently perform over 100 hip arthroscopic procedures per year and started outcome collections directly after fellowship training when they began practice. The patient data collection in this study covered the first 3 years of each surgeon’s practice: surgeon A spanned 2018-2021 and surgeon B 2014-2016, with surgeon A starting practice in 2018 and surgeon B starting in 2014. Both surgeons follow best practices in the management of FAIS as reported by Lynch et al. 30
Both surgeons operated at ambulatory surgery centers for tertiary referral academic institutions. Both surgeons used a large perineal post and 2-portal technique with anterolateral and midanterior arthroscopic portals. Surgeon A performed an interportal capsulotomy and used all-suture anchors and a simple suture configuration for labral repair along with capsule closure when possible. Reasons capsular closure was forgone included inadequate tissue, scarring, inability to hold suture, or earlier cases before capsule closure was routine for surgeon A. Surgeon B performed a periportal capsulotomy and used polyether ether ketone suture anchors with a simple suture configuration for labral repair without capsule closure. Both surgeons performed osteoplasty when they felt indicated based on preoperative imaging and dynamic arthroscopic examination. Indications for chondroplasty included unstable chondral defects (Outerbridge grade ≥2). After surgery, both surgeons limited patients to 20 pounds (9.07 kg) of flat-foot weightbearing with crutch use for 2 weeks (up to 6 weeks for microfracture). Surgeon A placed patients in a hip orthosis for 2 weeks postoperatively set to 90° of flexion, 0° of extension, neutral rotation, and 10° of abduction, while surgeon B did not use a brace. Formal physical therapy was allowed within a few days after surgery, with impact allowed after 3 months and release to full sports after 6 months from surgery.
The HOOS questionnaire was used for all patients. It is a validated PROM with 5 subscales—Symptoms, Pain, Activities of Daily Living, Sports and Recreation (Sport/Rec), and hip-related Quality of Life. 40 Standardized answer options are given in 5 Likert boxes, with scores from 0 (worst) to 4 (best), and the total score is calculated by adding the subscale scores as follows: 100 – [(patient’s score of the subscale × 100)/(total score of the subscale)]. A maximum score of 100 indicates that a patient has no hip symptoms. It has been shown to have high internal consistency with excellent test-retest reliability for FAIS.24,38,42
Statistical Analysis
The primary outcome of the study was the 2-year postoperative HOOS score. Patients from surgeon A’s cohort were matched 1 to 1 with patients from surgeon B’s cohort according to age, sex, and BMI to limit confounding bias. Matching ranges for age and BMI were set to 14 to 64 years and 18 to 45 kg/m2, respectively. To compare the demographic, radiographic, and intraoperative characteristics between the 2 cohorts, unpaired sample t tests were performed and standard deviations were calculated for continuous variables (age, BMI, LCEA, alpha angle, and traction time), while the chi-square test (sex and Tönnis grade) and the Fisher exact test (femoroplasty, acetabuloplasty, labral treatment, chondroplasty, microfracture, iliopsoas release, and capsular closure) were performed for categorical variables. Paired t tests were employed to examine the differences in HOOS scores within each cohort (preoperative vs 2-year postoperative). Unpaired sample t tests were utilized to compare the change in HOOS scores between the 2 cohorts. The MCID cutoff for each cohort was determined using a distribution-based method described by Norman et al 36 and calculated as one-half of the standard deviation for each HOOS subscale. 36 Pearson chi-square tests were performed to compare the proportion of patients achieving MCIDs between the 2 cohorts. The MCID values and percentages of patients achieving MCIDs were calculated for each HOOS subscale, and the mean and standard deviation were calculated for each continuous variable. Statistical significance was set at P < .05. Statistical analyses were conducted using R Statistical programming Version 2022.02.3 (R Core Team). An a priori power analysis performed with preoperative and 2-year postoperative HOOS scores from a previous study determined that to achieve a statistical power of 80%, 17 hips were needed in each group for HOOS symptoms 14 (effect size, 1.03).
Results
A total of 176 hips (100 women, 76 men) met the 2-year follow-up and the inclusion criteria, with 88 matched patients from each institution (Figure 1). The mean age of the study population was 33.7 ± 11.2 years, ranging from 14 to 64 years, and the BMI was 26.3 ± 6.2 kg/m2, ranging from 18 to 45 kg/m2. Baseline patient characteristics, radiographic findings, and most intraoperative procedures were comparable between the 2 cohorts and are listed in Table 1. There were statistically significant intraoperative differences as surgeon A performed fewer femoroplasties, more acetabuloplasties, more chondroplasties, and more capsular closures (Table 1). There were no patients with Tönnis grade ≥2 in either cohort.

A flowchart demonstrating patient selection. Both surgeons had just begun practice at the start of data collection. BMI, body mass index.
Demographic, Radiographic, Intraoperative, and Complication Findings a

Values are presented as mean ± SD, n, or n (%). The bold P values indicate significance (P < .05). The chi-square test and the Fisher exact tests were used for categorical values and Student unpaired sample t test for mean values. BMI, body mass index; LCEA, lateral center-edge angle; THA, total hip arthroplasty.
Perioperative complications, revision arthroscopy, and revision to total hip arthroplasty (THA) were documented throughout the study duration for each cohort. Surgeon A saw a 1% and surgeon B saw a 0% complication rate within their respective cohorts. Neither surgeon performed revision arthroscopy on their respective cohort throughout the follow-up. A total of 2% of surgeon A’s cohort and 0% of surgeon B’s cohort required conversion to THA within the 2-year follow-up period.
No significant differences were observed in preoperative HOOS scores between cohorts (all P > .05). All mean subscale scores increased significantly (P < .001) from preoperative to 2 years postoperative in both cohorts, with a clinically significant change in each subscale (Tables 2 and 3, Figure 2). The mean change in pre- to postoperative HOOS scores was the same between surgeon cohorts except for the Sport/Rec subscale, where surgeon B had a statistically (P = .048) but not clinically greater change (Table 3). Most patients in all 5 HOOS subscales for both cohorts achieved the calculated MCID threshold. No difference (P > .05) was seen when comparing the number of patients who achieved MCID between cohort subscales, except for the Sport/Rec subscale where surgeon B saw a greater percentage than surgeon A (P = .01) (Table 3).
Preoperative and 2-Year Postoperative HOOS Scores a
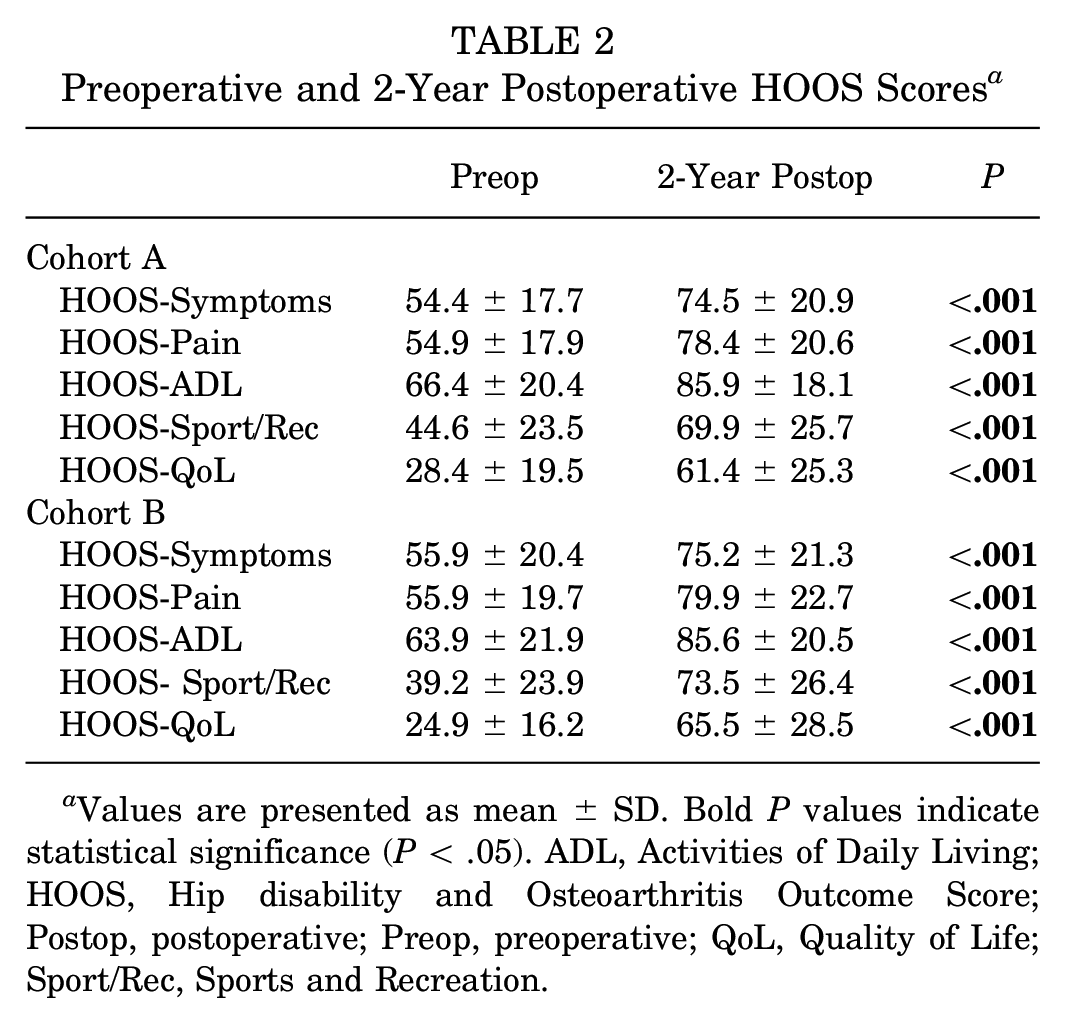
Values are presented as mean ± SD. Bold P values indicate statistical significance (P < .05). ADL, Activities of Daily Living; HOOS, Hip disability and Osteoarthritis Outcome Score; Postop, postoperative; Preop, preoperative; QoL, Quality of Life; Sport/Rec, Sports and Recreation.
MCID Thresholds for HOOS Scores a

Data are presented as mean ± SD or %. The bold P values indicate statistical significance (P < .05). ADL, Activities of Daily Living; HOOS, Hip disability and Osteoarthritis Outcome Score; MCID, minimal clinically important difference; PROM, patient-reported outcome measure; QoL, Quality of Life; Sport/Rec, Sports and Recreation.
P values from unpaired sample t test.
MCID calculated using a distribution-based method. P values are from the chi-square t test.

Preoperative and 2-year postoperative HOOS scores for both cohorts. The error bars indicate standard error. The mean postoperative scores improved significantly from the preoperative scores in both cohorts for all HOOS subscales: Symptoms, Pain, ADL, Sport/Rec (Sports), and QoL. *A statistically significant difference was observed in the Sport/Rec subscale only. ADL, Activities of Daily Living; HOOS, Hip disability and Osteoarthritis Outcome Score; QoL, Quality of Life; Postop, postoperative; Preop, preoperative; Sport/Rec, Sports and Recreation.
Discussion
Our comparison of 2 independent surgeons’ practices demonstrated that meaningful and similar improvement can be seen for patients undergoing FAIS arthroscopy. There is a paucity of research regarding this relationship, and many multicenter studies suggest that including data from different surgeons who vary in technique and rehabilitation protocol contributes to limitations in result interpretation.3-5,37
This study compared patient outcome data from surgeons who practiced in different states, attended different residencies and sports-medicine fellowships, and had variances in intraoperative procedures and rehabilitation protocols. Specific differences included capsular access and management, implant/vendor choice, and postoperative bracing. Both cohorts significantly improved in all 5 HOOS subscales at 2 years after surgery compared with their preoperative HOOS scores. Most patients in each cohort surpassed the MCID threshold set for each subscale, ranging from 57% to 76% of the cohort populations. These results are consistent with previous studies that compared differences in capsulotomy type and use of a postoperative hip brace.22,34 McGovern et al 34 found no difference in patient outcomes when comparing interportal versus periportal capsulotomy. When determining short-term outcomes with and without hip brace use, Johnson et al 22 found no difference in patient results through analysis of postoperative emergency department visits, complications rates, and pain levels. A prior study primarily focused on the biomechanical properties of different suture types in hip arthroscopy without comparison of patient outcomes. 12 Novel to our study is determining outcomes through PROMs and considering several factors—including bracing and suture anchor composition. In our study, all variables were compared in 1 setting and showed no significant differences.
One explanation for the consistency of PROMs between the 2 surgeons’ cohorts is that both surgeons followed best practices regarding patient screening and selection, as well as intraoperative decision-making and execution of labral repair and osteoplasty. 30 Common patient and surgical factors help predict whether patients will improve after arthroscopic treatment for FAIS. 11 Some common and reliable predictors for poor patient outcomes include the presence of hip arthritis, older age, and previous hip arthroscopy.6,11,25,27,29,35,45,46 Other cited predictors of poor outcome include hip dysplasia, elevated BMI, female sex, severe anxiety, depression or other psychological impairment, opioid use, and poor preoperative PROMs.9,23,29,41,45 This study did not include some of these predictors, most notably psychological factors and opioid use. It has been noted in previous literature that there is no difference in outcomes for patients with Tönnis grade 0 or 1; furthermore, none of the patients in this study had radiographic findings of arthritis 10 (Tönnis grade ≥2). Revision cases were also not included, and the effect of age, sex, and BMI were controlled for via matching. Overall, this was a young, healthy patient cohort who had FAIS and had failed nonoperative management and, accordingly, had excellent outcomes after surgery.
When comparing the mean change in HOOS subscales and the percentage of patients achieving MCID, a statistically significant difference was observed in only the HOOS-Sport/Rec subscale (cohort A: 25.3 ± 29.7 vs cohort B: 34.3 ± 29.7: P = .048; and MCID achieved in 57% vs 76% of patients; P = .01). Of note, surgeon A completed significantly more chondroplasties than surgeon B (35% vs 3%). Although Tönnis grades were similar between cohorts, more patients in surgeon A’s cohort may have exhibited higher grades of chondral damage, or the performance of chondroplasty could have a negative effect on outcomes. It has been noted in the literature that preoperative PROM scores influence patient outcomes.9,35,37 Nwachukwu et al 37 specifically noted that patients with greater preoperative Hip Outcome Scores for the Sport/Rec subscale were less likely to achieve MCIDs. Specifically, it was noted that patients scoring >58.3 preoperatively on the Sport/Rec subscale are less likely to achieve MCIDs. Surgeon A had a greater percentage (28%) of patients meeting this criterion compared with surgeon B (20%). Another potential explanation for the Sport/Rec subscale difference could be that surgeon A performed significantly fewer femoroplasties than surgeon B (89% vs 100%, respectively). It has been shown in the literature that patients undergoing femoroplasty perform better postoperatively and have fewer revision operations. 1 Although not a direct comparison, these previous findings may provide insight into why the Sport/Rec subscale for surgeon A demonstrated a significantly lower percentage of patients achieving MCID compared with surgeon B, as the preoperative score for the Sport/Rec subscale in cohort A was greater at 44.55 ± 23.53 compared with cohort B at 39.23 ± 23.93, indicating that the patients in cohort A were able to participate in more sports and recreational activities at baseline. Overall, this study’s HOOS change from pre- to postoperative surveys was similar to that in previous studies.8,14,20
Strengths and Limitations
Multiple strengths were seen in this study—including how the multicenter database was prospectively maintained—and included a variety of patient demographic, radiographic, clinical, and intraoperative findings. Another strength was the use of propensity matching for cohorts to limit confounding variables of age, BMI, and sex. Based on a priori analysis, this study’s cohort population size was adequately powered to detect meaningful differences. Selecting HOOS in conjunction with the MCID improves psychometric properties and strengthens results interpretation regarding meaningful improvement.
This study has noteworthy limitations. Given the sample size, the study could theoretically be subject to type 2 error despite having adequate calculated power. The study was performed in the first 3 years of surgeons’ practices, potentially limiting generalizability to surgeons further along in practice. There was a higher rate of chondroplasty in 1 cohort, which may create bias in the results. This study also did not assess some factors associated with outcomes—including psychological factors, opioid use, and worker’s compensation claims. By focusing on a 2-year follow-up, this study overlooks outcomes seen at mid- or longer-term follow-ups. Early PROMs (6 weeks to 12 months) were excluded from this study and could potentially show faster improvements in patients where capsular closure was performed. Previous literature noted greater PROMs in these patients but demonstrated no significant difference in achievement of MCIDs when compared with patients where the capsule was left unrepaired. 27 Both surgeons are current high-volume hip arthroscopists (>100 hip arthroscopy cases per year); thus, these results may not be generalizable to surgeons with lower hip arthroscopy volume. Another possible limitation of the study is that neither surgeon used an intraoperative postless system during the data collection period, which could limit generalizability, as these systems are increasing in popularity. Last, this study only compared 1 PROM (HOOS), while other studies have employed ≥2 PROMs and incorporated surveys that account for psychological impairment and mental illness.7,20,43 Although HOOS has been shown to have excellent reliability, it has been noted in the literature to have a ceiling effect in the Sport/Rec subscale when assessing hip arthroscopy outcomes.20,42 Despite these limitations, this study adds important information on the reproducibility of hip arthroscopy outcomes in different practices.
Conclusion
This prospective cohort study on arthroscopic treatment of FAIS reveals that matched patient cohorts from 2 separate institutions yielded a similar, meaningful improvement of PROMs at 2 years. Our study suggests that when subspecialty-trained surgeons perform arthroscopic labral treatment and osteoplasty for FAIS, outcomes are consistent despite geography, surgeon, training, implants, surgical technique, and postoperative protocol.
Footnotes
Final revision submitted June 3, 2024; accepted June 19, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.L.Z. has received consulting fees from DePuy Synthes Products, Medical Device Business Services, and Stryker. S.E.W. has received education payments from Evolution Surgical and Arthrex; hospitality payments from Stryker, Wright Medical Technology, and Medwest Associates; consulting fees from Encore Medical; and a grant from Acumed and Arthrex. M.S.H. has received consulting fees from Linvatec Corporation; and education payments from Summit Surgical Corp. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Washington (STUDY00015385).