
Abstract
Background:
After anterior cruciate ligament (ACL) reconstruction (ACLR), the function and strength of the quadriceps muscle are essential for a successful recovery. Low-load blood flow restriction training (LL-BFRT) is believed to reduce muscle atrophy and restore muscle function.
Purpose:
To systematically analyze the evidence on the effectiveness of LL-BFRT in early rehabilitation after ACLR.
Study Design:
Systematic review; Level of evidence, 1.
Methods:
A systematic review and meta-analysis were conducted consistent with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Comprehensive literature searches were performed in several electronic databases—including Cochrane Library (trials), PubMed, Embase, Web of Science, China National Knowledge Infrastructure, WanFang, China Science and Technology Journal Database, and Sinomed—from inception to October 1, 2023. Included were randomized controlled trials in Chinese and English comparing LL-BFRT within 6 weeks after ACLR with conventional rehabilitation training. Bias risk was assessed using the Cochrane Risk-of-Bias 2 tool. The outcomes measured were quadriceps muscle size, knee joint functional scores, balance function, and complications. The effects of LL-BFRT versus conventional rehabilitation were analyzed using standardized mean differences (SMDs) or weighted mean differences (WMDs).
Results:
A total of 362 studies were initially identified, and 8 were included for analysis. LL-BFRT was significantly more effective in improving quadriceps muscle volume (SMD, 0.37 [95% CI, 0.08 to 0.66]; P = .01) and Lysholm scores (SMD, 0.74 [95% CI, 0.43 to 1.05]; P < .0001) compared with conventional rehabilitation training. However, no significant improvements were observed in the 3 directions of the Y-balance test: anterior (WMD, 0.55 [95% CI, –6.37 to 7.46]; P = .88), posteromedial (WMD, –2.24 [95% CI, –8.76 to 4.29]; P = .50), and posterolateral (WMD, 0.02 [95% CI, –13 to 13.03]; P = 1.0). No complications were reported in any of the included studies.
Conclusion:
The results of this meta-analysis suggested that LL-BFRT within 6 weeks after ACLR has a more pronounced effect on increasing quadriceps muscle volume and improving Lysholm scores compared with conventional rehabilitation training, with no apparent complications.
Anterior cruciate ligament (ACL) rupture is a prevalent sports injury, with an incidence rate of 35 cases per 100,000 individuals. 12 Most surgeons recommend that patients with a high demand for knee joint function should undergo ligament reconstruction surgery. 28 After ACL reconstruction (ACLR), the function and strength of the quadriceps muscle are essential for a successful recovery. Restoration of optimal function and strength plays a crucial role in maintaining the stability of the knee joint and enhancing athletic performance. The synergistic action of the quadriceps and hamstrings can effectively restrict anterior tibial translation during movement, protecting excessive tension on the anterior cruciate ligament graft.11,20
The quadriceps muscle is the most severely atrophied muscle in the early postoperative period. 1 The interruption of proprioceptive information after ACL surgery leads to reduced recruitment and reflex function of α-motor neurons, preventing autonomous muscular contraction of the quadriceps. 35 Muscle recruitment dysfunction can lead to atrophy, weakness, and neuromuscular control impairments of the quadriceps femoris. 32 Dysfunction of the quadriceps may result in abnormal movement patterns, affecting daily activities and increasing the risk of reinjury, and may even be associated with the development of traumatic osteoarthritis.4,25 The function of the quadriceps muscle is closely related to its size. 23 Therefore, selecting effective rehabilitative strategies for addressing quadriceps atrophy is of high importance.
High-load strength training effectively stimulates muscles, resulting in strength and volume gains. 10 High-load strength training in knee extension exercises may result in excessive anterior tibial translation, increasing the stress on the graft and rendering the joint unable to withstand the mechanical stress applied during training, leading to graft tear.15,33 The first 6 weeks after ACLR are a critical period for protecting the graft. 3 Consequently, implementing high-load strength training in the early stages after ACL surgery, where muscle strength restoration is crucial, becomes challenging.22,40 Recent studies have demonstrated that blood flow restriction training (BFRT) with low-load resistance (LL-BFRT) can ameliorate postoperative knee joint pain and improve function, which is equally effective as high-load strength training in enhancing the thickness and strength of the quadriceps muscle.6,30,39
During LL-BFRT, pneumatic cuffs are positioned proximally on the limb, intermittently or continuously inflating them to generate pressure, thereby fully or partially restricting arterial and venous blood flow.31,42 LL-BFRT can create a hypoxic environment by restricting blood flow circulation during resistance training, which in turn enhances the recruitment of type 2 muscle fibers, increases levels of anabolic hormones related to synthetic metabolism, and promotes protein synthesis, while reducing myostatin expression.24,29,34 This approach aims to improve muscle strength and increase muscle volume. A 2020 systematic review reported that BFRT may be an effective method for increasing the cross-sectional area of the quadriceps femoris muscle. 2 However, their study included different knee joint conditions, which may influence the assessment of efficacy in patients who had ACLR. Another systematic review performed in 2022 highlighted the potential benefits of LL-BFRT on muscle size and strength after ACLR; however, because of the limited quantity of included studies, only a qualitative synthesis was performed. 21 Despite the recognized efficacy of LL-BFRT in attenuating quadriceps atrophy, 8 a 2023 systematic review found no significant difference between BFRT and conventional rehabilitation therapy on maintaining or improving knee muscle size in patients after ACLR. 5
In this study, we aimed to assess the impact of early intervention (≤6 weeks) after ACLR with LL-BFRT. We compared the effectiveness of LL-BFRT with conventional rehabilitation training on quadriceps muscle size, knee joint function, and balance function. The hypothesis was that early LL-BFRT after ACLR would enhance quadriceps muscle size, knee joint function, and balance compared with conventional rehabilitation.
Methods
Search Strategy
This systematic review was registered on PROSPERO (registration No. CRD42024539458). A systematic meta-analysis was conducted consistent with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Comprehensive literature searches were performed in several electronic databases—including Cochrane Library, PubMed, Embase, Web of Science, China National Knowledge Infrastructure, WanFang, China Science and Technology Journal Database, and Sinomed—from the inception of each database to October 1, 2023. This search strategy involved the use of MeSH terms and text words. The MeSH terms included “Anterior Cruciate Ligament Reconstruction” and “Blood Flow Restriction Therapy.” Details of the final search algorithm for PubMed are shown in Appendix Table A1.
Study Selection
Two reviewers (Q.L. and Y.Z.) independently evaluated the titles, abstracts, and full texts of the retrieved articles using Zotero 6 (Corporation for Digital Scholarship). The following inclusion and exclusion criteria were applied:
Inclusion Criteria
(1) Patients who underwent primary ACLR; (2) randomized controlled trials with language restrictions of English and Chinese; (3) intervention group received LL-BFRT (20%-35% of 1 repetition maximum [1-RM; ie, the maximum weight that can be lifted once]); the control group received routine, non-BFRT rehabilitation training; (4) LL-BFRT was initiated ≤6 weeks postoperatively; and (5) outcomes included at least 1 of the following: muscle size, knee joint functional scores, and balance function.
Exclusion Criteria
(1) nonrandomized controlled trial; (2) control group received high-intensity resistance training; (3) presence of additional injuries such as extra ligament tears, severe meniscus damage, or fracture; (4) inability to access the full text or extract useful information from the article despite attempts to request it from the authors; and (5) unclear training program.
After the screening process, cross-validation was performed, and any discrepancies in opinions were resolved through discussions or by seeking the opinion of a third reviewer (J.Q.).
Risk-of-Bias Assessment
We employed the Cochrane Risk of Bias Version 2 (RoB 2) tool, to assess the risk of bias in the included studies. 37 This tool assesses bias risk across 5 domains—including the randomization process, deviations from intended interventions, missing outcome data, outcome measurement, and selection of reported results. Each domain is graded as having a low, moderate, or high risk of bias, after which an overall risk-of-bias score is calculated. According to the algorithm of this tool, if all domains are rated as low risk, the overall bias risk for each trial is classified as low; if any domain is at high risk, the overall risk is classified as high. If no domain is classified as high risk but ≥1 domains are deemed to have some concerns, the overall bias risk is categorized as “some concerns.” 37
The risk-of-bias assessment was conducted independently by 2 assessors (Q.L. and Y.Z.), with any discrepancies resolved by a third assessor (J.Q.).
Data Extraction
Relevant data were extracted to a predesigned table. Extracted data characteristics from the included studies encompassed (1) basic information, comprising lead author, year of publication, language of publication, sample size, intervention and control measures, intervention duration, training regimen, and frequency; (2) basic characteristics of the study population, including age and sex; (3) study outcomes; and (4) relevant information pertaining to risk of bias assessment. The original author was contacted when any relevant information was not reported.
Meta-analysis of Outcomes
The outcomes measured focused on the following parameters: (1) quadriceps muscle size (eg, muscle cross-sectional area, thickness, and muscle quantity); (2) knee joint functional scores (eg, Lysholm score); (3) balance function (eg, Y-balance test, proprioception, and motor coordination); and (4) complications (eg, thrombosis, skin issues, limb numbness, delayed-onset muscle soreness, and rhabdomyolysis). If a study reported results at different time points, the results evaluated at the end of the intervention period were used for analysis. Any data that could not be directly used were either converted into usable data using the Cochrane Handbook’s data transformation formula or excluded.
Statistical Analysis
A meta-analysis using Stata 17 was conducted. The included studies had continuous variable data, and effect sizes were represented as weighted mean difference (WMD) with 95% CI or standardized mean difference (SMD) with 95% CI, depending on whether the units were the same or different, respectively. Heterogeneity among the included study results was analyzed using the chi-square test (α = .1) and was quantified using the I2 statistic. Low heterogeneity was considered if P > .10 and I2 < 50% and a fixed-effects model was used for the meta-analysis. High heterogeneity was indicated if P < .10 and I2 > 50% and a random-effects model was employed for the meta-analysis. In addition, subgroup analysis, sensitivity analysis, and publication bias tests were conducted to identify and determine the sources of high heterogeneity. Sensitivity analysis was performed by sequentially removing individual literature from the analysis using Stata 17 software (Stata Corp) to assess whether any single study significantly influenced the overall effect. Publication bias was evaluated using the Egger test.
Results
Study Selection
A total of 362 relevant studies were initially retrieved from various databases using MeSH terms and text words. Among them, 126 duplicate articles were eliminated, resulting in 236 unique articles. After reviewing the titles and abstracts, 206 articles were removed based on the exclusion criteria, leaving 30 articles for full-text review. After reading the full texts, 22 studies were excluded, resulting in the final inclusion of 8 studies.17,18,19,26,27,36,38,43 In total, the experimental group included 138 patients, while the control group included 136 patients. The flowchart of the study selection process is shown in Figure 1.

A PRISMA flowchart showing the selection process of studies. CNKI, China National Knowledge Infrastructure; Preferred Reporting Items for Systematic Reviews and Meta-Analyses; WOS, Web of Science.
Characteristics of the Studies
All studies in this review were randomized controlled trials with level 2 evidence; there were 2 master’s theses27,38 with randomized controlled trial methodology. Five studies26,27,36,38,43 were in Chinese and the remaining 3 studies17,18,19 were in English. The studies featured varied training methodologies, with 1 employing fascia compression band training 27 and the remaining 7 utilizing LL-BFRT.17,18,19,26,36,38,43 The control groups uniformly underwent conventional rehabilitation training without blood flow restriction. The mean age of the participants in the intervention group ranged from 24.9 to 37.16 years, while that of the control group ranged from 24.1 to 38.67 years. Within the intervention group, there were 100 male and 38 female participants, whereas the control group consisted of 97 men and 39 women. Five studies17,18,26,27,38 assessed quadriceps muscle size, 6 studies19,26,27,36,38,43 evaluated knee joint function, and 3 studies18,19,36 examined balance function. Notably, none of the 8 studies reported any complications. Individual study information and patient characteristics of these studies are presented in Table 1.
Characteristics of the Included Studies a

No complications were reported in any of the studies. CG, control group; EG, experimental group; IKDC, International Knee Documentation Committee; LL-BFRT, low-load blood flow restriction training; LOP, limb occlusion pressure; 1-RM, 1 repetition maximum; QF, quadriceps femoris; ROM, range of motion; VAS, visual analog scale for pain.
Intervention Measures Used
The training durations in the included studies ranged from 2 to 12 weeks. Training frequency was unreported in 1 study, 18 while 1 study 17 conducted daily sessions, and the remaining 6 studies19,26,27,36,38,43 varied between 2 to 5 sessions per week. All exercise regimens across the 8 studies commenced immediately postoperatively. Two studies27,36 in the experimental group initiated LL-BFRT interventions 2 weeks postoperatively, while the remaining 6 LL-BFRT interventions commenced immediately postoperatively.17,18,19,26,38,43 Control group training regimens consisted of standard rehabilitation training (non-BFRT) encompassing muscle strength training, range of motion exercises, proprioception training, resistance training, and gait training. Experimental group training protocols integrated BFRT with the control group’s muscle strength training regimen, with resistance set <30% of 1-RM. The rehabilitation plans for each group from each study are detailed in Appendix Table A2.
Risk-of-Bias Assessment
Based on the criteria established by the Cochrane RoB 2 tool, 5 studies17,18,19,26,43 had a high risk of bias, 2 studies36,38 had some concerns, and only 1 study 27 had a low risk of bias. The predominant reason for many studies exhibiting a high risk of bias was the lack of blinding in their design. Detailed information can be found in Figure 2.

Results of bias assessment using the Cochrane Risk of Bias Version 2 tool. 37
Results of the Meta-analysis
Quadriceps Muscle Volume
Five studies17,18,26,27,38 (n = 180 patients) investigated the impact of LL-BFRT on muscle volume. Two of the studies17,26 measured the cross-sectional area of the quadriceps muscles (cm2) using magnetic resonance imaging, while 2 studies27,38 measured the maximum thickness of the medial vastus muscles (cm) using ultrasound imaging, and 1 study 18 used dual-energy x-ray absorptiometry to measure muscle mass (cm3). Because of the different measurement units and low heterogeneity among the 5 articles (P = .86; I2 = 0%), a fixed-effects model and SMD were used. The pooled results indicated that LL-BFRT significantly improved quadriceps atrophy compared with routine rehabilitation training (SMD, 0.37 [95% CI, 0.08-0.66]; P = .01) (Figure 3). Sensitivity analysis excluding individual studies showed no significant change, suggesting the stability of the results. The publication bias in these 5 articles as assessed using the Egger test indicated no significant publication bias (P = .6995).

Forest plot of standardized mean differences in quadriceps muscle size.
Lysholm Score
Included were 6 studies19,26,27,36,38,43 (n = 166 patients) that employed the Lysholm score as an outcome measure; 1 study 19 utilized the difference in Lysholm scores before and after treatment, while another study 38 had difficulty obtaining Lysholm score data and was therefore excluded. Of these studies, 5 studies19,26,27,36,43 exhibited low heterogeneity (P = .9; I2 = 0%), and a fixed-effects model was used. The pooled results demonstrated that LL-BFRT significantly improved knee joint function compared with routine rehabilitation training (SMD, 0.74 [95% CI, 0.43-1.05]; P < .0001) (Figure 4). Sensitivity analysis by excluding individual studies showed no significant change, indicating the stability of the results. The publication bias in the 5 evaluated studies as assessed using the Egger test indicated no significant publication bias (P = .4002).
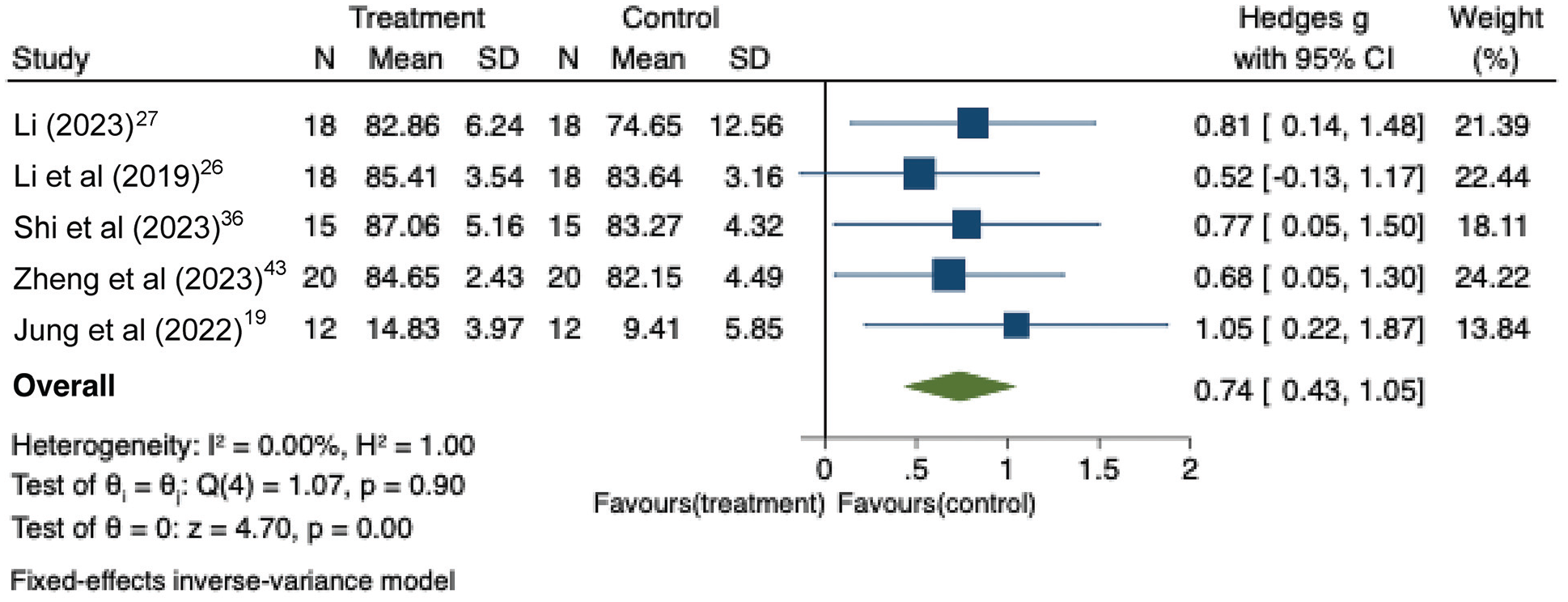
Forest plot of standardized mean differences in Lysholm score.
Balance Function
The evaluation of balance function comprised 3 studies, with 2 studies18,19 (n = 56 patients) using the Y-balance test and 1 study 36 focusing on proprioception and motor coordination. The 2 studies that used the Y-balance test reported the scores as the difference between pretreatment and posttreatment, ensuring the consistency of measurement units, and high heterogeneity was observed for the 3 directions of postural control: anterior (P = .04; I2 = 76%), posteromedial (P = .07; I2 = 70%), and posterolateral (P = .01; I2 = 86.7%). Therefore, a random-effects model with WMD was employed. The pooled results indicated no significant improvement in dynamic postural control between LL-BFRT and routine rehabilitation training on any of the 3 postural control directions: anterior (WMD, 0.55 [95% CI, –6.37 to 7.46]; P = .88) (Figure 5A); posteromedial (WMD, –2.24 [95% CI, –8.76 to 4.29]; P = .50) (Figure 5B); or posterolateral (WMD, 0.02 [95% CI, –13 to 13.03]; P = >.999) (Figure 5C).

Forest plots of WMD for the (A) anterior, (B) posteromedial, and (C) posterolateral directions of the Y-balance test. REML, restricted maximum likelihood; WMD, weighted mean differences.
Complications
No complications were reported in any of the included studies.
Discussion
In this study, we conducted a meta-analysis on 274 participants from 8 articles to examine the effects of LL-BFRT on quadriceps muscle volume, knee joint function, and balance function in patients after ACLR. Our findings revealed that LL-BFRT significantly improved quadriceps muscle volume (P = .01) and knee joint function (P < .0001) compared with routine rehabilitation training. The results of our study have important implications for improving quadriceps muscle volume and knee joint function impairments in patients after ACLR. Given the numerous instabilities—such as pain and abnormal range of motion associated with accurately measuring quadriceps strength in the early post-ACL surgery period—changes in quadriceps strength were not selected as an outcome measure. The muscle size and Lysholm scores, however, can serve as effective indicators of the efficacy of LL-BFRT in improving quadriceps function. 23
Our findings are consistent with those of previous systematic reviews.2,21 Our meta-analysis showed that LL-BFRT is beneficial for reducing quadriceps muscle atrophy and enhancing knee joint function in the early stages after ACLR. However, we observed variations in the impact of different LL-BFRT programs on quadriceps muscle volume among the included studies. One study 17 had a shorter training duration (only 2 weeks), with the program consisting solely of open-chain exercises. The lack of diversity in the training program and the short training duration may explain the limited improvement in muscle atrophy. Conversely, 4 other studies18,26,27,38 had longer treatment durations (≥6 weeks) and a variety of training modalities—including open-chain exercises, closed-chain exercises, gait training, balance training, and proprioceptive training. The diverse training protocols and longer durations resulted in significant improvements in quadriceps muscle atrophy with LL-BFRT. Previous systematic reviews have also recommended LL-BFRT durations of 6 to 12 weeks. 21 Therefore, the diversity of training programs and duration may be crucial factors influencing the extent of muscle atrophy improvement. Notably, 1 study in our review 27 utilized fascial compression band training, which involves restricting blood flow using a pressure band to enhance muscle strength performance and accelerate recovery. Pressure sensors were employed to monitor the pressure, with commonly used values ranging from 150 to 160 mm Hg. The compression band was applied 10 cm above and below the knee joint, and considering the potential benefits of fascial compression band training, it can be considered a form of BFRT.
Quadriceps muscle atrophy after ACLR can result in functional impairments to the knee joint. 23 In this study, it was found that LL-BFRT significantly improved Lysholm scores compared with routine rehabilitation training. In the 5 studies19,26,27,36,43 included for Lysholm score assessment, the treatment duration ranged from 8 to 12 weeks. Apart from muscle strength training, the training protocols also encompassed activities targeting mobility, resistance training, gait training, and balance function enhancement. Such improvements may be associated with alleviating muscle atrophy, as well as reducing pain, joint effusion, and increasing range of motion. 14
In 2 of the included studies,18,19 balance function was assessed with the Y-balance test, which evaluates dynamic posture control of the lower extremities. 7 Results of the meta-analysis indicated that LL-BFRT did not exhibit superior improvements across any of the 3 directions of postural control (Figure 5). The high heterogeneity of the results might be attributed to differences in assessment timing and training protocols between these 2 studies.18,19 Jack et al 18 conducted initial assessments in the 8th week of training and final assessments in the 12th week, with only a 4-week interval for conducting the Y-balance test. The training program consisted solely of strength training, which may have limited the extent of changes in dynamic postural control values. 18 On the other hand, Jung et al 19 conducted the Y-balance test with a 12-week interval before and after treatment, within a training program that included balance functional training, which may be the reason for the significant improvement in dynamic postural control in their study. Although we did not find significant differences in postural control between LL-BFRT and conventional rehabilitation, Shi et al 36 have reported potential benefits of LL-BFRT in enhancing proprioception, movement coordination, and balance function.
Only 3 studies18,27,38 in this review mentioned dropout rates, all of which were <15%, with the predominant reason for dropout being voluntary withdrawal. None of the studies reported complications such as infection or lower limb deep vein thrombosis. However, other studies have suggested that BFRT use in the early postoperative period may prolong joint swelling and promote thrombus formation.9,16 Therefore, BFRT should be avoided in patients at risk of deep vein thrombosis—including those with a history of deep vein thrombosis or genetic factors that increase their risk. 41
BFRT constitutes an adjunctive modality, and combined with strength training, appears to align more closely with early postoperative rehabilitation protocols. 13 Within our encompassed investigations, sole LL-BFRT seems to exhibit limited efficacy in mitigating muscle atrophy and enhancing postural control, whereas LL-BFRT combined with range of motion exercises, resistance training, gait training, and balance exercises may yield more pronounced therapeutic benefits in attenuating muscle atrophy, fortifying knee joint functionality, and enhancing balance capabilities. Future inquiries may explore amalgamating blood flow restriction with diverse training regimens to assess the effectiveness of combined protocols. Moreover, methodological refinements—such as allocation concealment and blinding—should be implemented to enhance the credibility of outcomes.
Limitations
There are several limitations to this study. First, the number of included studies was relatively small, which may not be sufficient to detect the effects of interventions. Therefore, all results should be interpreted with caution. Second, postoperative rehabilitation training programs varied across studies, which may lead to bias in research results. Third, most of the included studies were at high risk of bias, which could compromise the reliability of the findings. Fourth, information on the blood flow restriction pressure and transplant types was not reported, which may affect the results. 28 Fifth, only studies in Chinese and English were included, which may introduce certain biases. Finally, most of the studies were short-term, and the long-term efficacy needs further verification.
Conclusion
The findings of this meta-analysis suggested that LL-BFRT has a more pronounced effect on increasing muscle volume and improving Lysholm scores compared with conventional rehabilitation training, with no apparent complications. Regarding dynamic postural control, no difference was observed between the LL-BFRT and conventional rehabilitation.
Footnotes
Appendix
Intervention Measures of the Included Studies a

| Study (Year) | Frequency | Exercise plan of CG b | Exercise plan of EG b |
|---|---|---|---|
| Li 27 (2023) | 3 d/wk for 8 wk | • 0-2 weeks: a. Straight-leg raises: 10 reps/set, 10 sets/day b. Ankle pumping exercise: 30 reps/set, 10 sets/day c. Knee extension training: 30 min/set, 2 sets/day d. Quadriceps femoris isometric contraction training: 10 reps/set, 10 sets/day e. CPM knee flexion training once a day for 20 min f. Patellar mobilization training: 10 reps/set, 2 sets/day. • 2-6 weeks: Add the following exercises to the protocol above: a. Active knee flexion training: 10 times daily b. Contralateral muscle strength training c. Gait training. • 6-10 weeks: Add weightbearing and proprioceptive training to the protocol above, improve joint control and stability, and gradually improve gait. |
Concurrently with conventional rehabilitation training, myofascial compression band training was incorporated after 2 weeks, encompassing the following exercises: a. Isometric contractions of the quadriceps femoris b. Straight-leg raises c. Passive flexion and extension of the knee joint, 10 reps/set, 10 sets/day. |
| Li et al 26 (2019) | 2 d/wk for 3 mo | Within 1 wk: a. Foundational rehabilitation treatment, including managing lower limb pain and swelling, maintaining, restoring, and strengthening joint mobility and muscle strength b. Functional rehabilitation focusing on training proprioception, balance ability, and gait function c. Correlative rehabilitation addressing core balance stability training and psychological evaluation. |
Routine rehabilitation training incorporating BFRT, applying 30% of 1-RM resistance load to knee flexion and extension exercises within 0°-90°. Each session consisted of 4 sets, with repetitions of 30, 15, 15, and 15, respectively, with 60 seconds of rest between sets |
| Shi et al 36 (2023) | • EG: 3 d/wk for 8 wk • CG: 5 d/wk for 8 wk |
• 0-2 weeks: a. Fixed position at 0° extension b. Elevation of the affected limb c. Passive patellar mobilization d. Straight-leg raises e. Hamstring isometric training f. Ankle pump exercises g. Passive knee flexion training (<90°) h. Isometric quadriceps contraction (10 sec each, 30 reps/set, 2 sets/session, 3 sessions/day). • 3-4 weeks: a. Resisted ankle pump exercises b. Terminal extension knee strengthening exercises c. Passive knee flexion training (0°-100°) d. Active knee flexion training (approaching 90°). • 5-8 weeks: a. Increase weightbearing training on affected limb b. Quadriceps resistance training c. Hamstring resistance training d. Static squat training e. Balance board exercises f. Stair climbing g. walking. |
BFRT was incorporated in addition to conventional rehabilitation: • 3-4 weeks: Resisted knee flexion and extension exercises (2 sets of training: 30 reps in set 1, 15 reps in set 2 with the assistance of sandbags). • 5-8 weeks: a. Building on stage 1, added bilateral knee flexion at 30° squatting exercises (2 sets of 5 minutes each) b. Alternating knee flexion and extension exercises (2 sets at 10 reps/set from a standing position to 0°-15° flexion) c. Power cycling training (10 minutes) All training exercises were performed at 30% of the 1-RM. |
| Su 38 (2021) | 5 d/wk for 6 wk | • Straight-leg raise: Keep the knee joint in an extended position, lift the heel 30 cm away from the surface of the bed, hold for 10 sec, rest for 5 sec, 10 reps/set, 4 sets/session • Knee extension against gravity after reaching 90° of joint mobility: Resistive knee extension between 90° and 60° of knee flexion, 10 reps/set, 4 sets/session • Multi-angle resistive isometric contraction training: Perform maximum resistance isometric contraction training of the quadriceps femoris at positions of 85°, 75°, and 65° of knee flexion, holding for 10 sec, resting for 5 sec, 10 reps/set, 1 set at each angle. • Low-load isotonic contraction training within a limited ROM: Perform knee joint extension exercise against 30% of 1-RM resistance load within 90°-60° of knee flexion; a total of 4 sets, with respective repetitions of 30, 15, 15, 15 per set and 1-min rest between sets. |
Same strength training protocol as the control group under BFRT conditions. |
| Zheng et al 43 (2023) | • EG: 3 d/wk for 8 wk • CG: 5 d/wk for 8 wk |
• 0-1 weeks: Immobilization with the use of orthosis, elevation of the affected limb, ankle pumping exercises, and isometric contractions of the quadriceps femoris • 2-3 weeks: Passive ROM training, knee joint flexion and extension exercises, and resistance exercises for ankle pumping • 4-6 weeks: Weight training, weight-shifting exercises, lower-limb strength training, balance training, and walking training, among others • 7-8 weeks: Knee flexion and extension exercises, stair climbing, and proprioception training, among others. |
BFRT was incorporated into conventional rehabilitation; BFRT was initiated 2 weeks postop and included the following: • Resisted flexion and extension exercises of the joints (2 sets total: 30 reps for set 1, 15 reps for set 2) • Resisted knee extension exercises (2 sets total: 30 reps for set 1, 15 reps for set 2) There was a 2-minute rest between sets. Intensity was set at 30% of 1-RM. |
| Iversen et al (2016) 17 | Daily for 2 wk | Starting day 2, the quadriceps femoris underwent 20 repetitions of low-load exercises within a single training session, repeated 5 times, twice daily. The training exercises included the following: a. isometric contractions of the quadriceps femoris b. knee extension training c. straight-leg raises. |
Starting from day 2, the experimental group underwent 5 minutes of BFRT followed by 3 minutes of restriction removal. During the BFRT period, the quadriceps femoris muscles were subjected to 20 reps of low-load exercises, repeated 5 times within a single training session, twice a day. The training exercises included (a) isometric contractions of the quadriceps femoris; (b) knee extension training; and (c) straight-leg raises |
| Jack et al 18 (2023) | 12 wk c | a. Quadriceps contractions (2-4 weeks) b. Closed-chain knee extensions (3-5 weeks) c. Bilateral leg press (4-5 weeks) d. Single-leg press (6-12 weeks) e. Single-leg hamstring curl (5-12 weeks) f. Ball squats (7-8 weeks) g. Split lunges (9-10 weeks) h. Box step-ups (11-12 weeks) Reps: 1 × 30; 3 × 15 (30% of 1-RM), 30 secs rest between sets. |
Based on BFRT, a training regime was instituted, aligned with the protocols followed by the control group. |
| Jung et al 19 (2022) | 3 d/wk for 12 wk | • 0-2 weeks: ROM exercise, straight-leg raise, stretching, weight shift, cup walking • 3-6 weeks: CKC exercises (squats, heel raise, gait retraining), OKC exercises (leg curl without weight), single-leg balance • 7-8 weeks: CKC exercises (squats, heel raise, gait retraining), OKC exercises (leg curl, leg extension), single-leg balance • 9-12 weeks: CKC exercises (squats, heel raise, gait retraining), OKC exercises (leg curl, leg extension), perturbation exercise All exercises were performed in 3 sets of 15 reps. |
The experimental group underwent the same ROM exercises and resistance training as the control group. After BFRT they engage in the same CKC exercises and OKC exercises. The exercise intensity began at 10% to 30% of the established 1-RM and gradually increased. |
BFRT, blood flow restriction training; CG, control group; EG, experimental group; CKC, closed kinetic chain; CPM, continuous passive motion; OKC, open kinetic chain; Rep, repetitions; RM, repetition maximum; ROM, range of motion; Postop, postoperative.
All reported time frames are postoperative.
Duration not reported.
Final revision submitted May 22, 2024; accepted June 5, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding for this study was received from the Natural Science Foundation of Fujian Province of China (No. 2021J01391). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.