
Abstract
Background:
Blood flow restriction training (BFRT) is a safe and potentially effective adjunctive therapeutic modality for postoperative rehabilitation related to various knee pathologies. However, there is a paucity of literature surrounding BFRT in high-performance athletes after anterior cruciate ligament reconstruction (ACLR).
Purpose:
To (1) compare the overall time to return to sports (RTS) in a cohort of National Collegiate Athletic Association (NCAA) Division I athletes who underwent a standardized rehabilitation program either with or without BFRT after ACLR and (2) identify a postoperative time interval for which BFRT has the maximum therapeutic benefit.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 55 student-athletes who underwent ACLR between 2000 and 2023 while participating in NCAA Division I sports at a single institution were included in this study. Athletes were allocated to 1 of 2 groups based on whether they participated in a standardized postoperative rehabilitation program augmented with BFRT (BFRT group; n = 22) or completed the standardized protocol alone (non-BFRT group [control]; n = 33). Our primary outcome measure was time to RTS. The secondary outcome measure was handheld dynamometry quadriceps strength testing at various postoperative time points, converted to a limb symmetry index (LSI). Quadriceps strength was not tested between the BFRT and non-BFRT groups because of the limited amount of data on the control group.
Results:
The mean age at the date of surgery was 18.59 ± 1.10 years for the BFRT group and 19.45 ± 1.30 years for the non-BFRT group (P = .011), and the mean RTS time was 409 ± 134 days from surgery for the BFRT group and 332 ± 100 days for the non-BFRT cohort (P = .047). For the BFRT group, the mean quadriceps strength LSI increased by 0.67% (95% CI, 0.53%-0.81%) for every week of rehabilitation, and there was a significantly positive rate of change in quadriceps strength in weeks 13-16 compared with weeks 9-12 (ΔLSI, 8.22%; P < .001).
Conclusion:
In elite NCAA Division I athletes, a statistically significant delay was observed in RTS with BFRT compared with standardized physical therapy alone after undergoing ACLR. There also appeared to be an early window during the rehabilitation period where BFRT had a beneficial impact on quadriceps strength.
Keywords
The anterior cruciate ligament (ACL) is one of the most frequently injured ligaments of the knee with an estimated incidence of 1 in 3000 in the United States; injuries occur predominantly in athletes.5,7 After ACL reconstruction (ACLR), the rehabilitation process specifically related to weakness and atrophy of the quadriceps and hamstring muscles can strongly influence an athlete's return to sports (RTS) chances.11,13,27,28,30
Blood flow restriction training (BFRT) has become increasingly popular as a promising therapy to promote physiologic changes that increase muscle burden at lower levels of resistance training and joint loading. 34 BFRT involves the application of an extremity tourniquet, which allows arterial inflow while simultaneously preventing venous outflow, resulting in an anaerobic environment that is thought to promote muscle hypertrophy through cell signaling and hormonal changes comparable to those seen at higher-intensity training loads.8,24 Surrounding BFRT, it has been suggested that resistance training at 20% to 50% of 1-repetition maximum (1-RM) could result in hypertrophy seen at the traditional strength protocols that utilize 70% of 1-RM per the American College of Sports Medicine recommendation.2,14,36,38 Although the data are limited, BFRT has been shown to be safe and potentially effective in improving quadriceps muscle strength in patients with weakness or atrophy related to knee pathology and after surgery.3,4,6,26,35 A recent systematic review of the effects of BFRT on patients undergoing knee surgery (ACLR and knee arthroscopy) demonstrated that BFRT use in the postoperative period could lead to a significant improvement in the cross-sectional area when quantifying muscle atrophy; however, no significant differences were found for patient-reported outcome measures. 18
While the muscle hypertrophy benefits of BFRT have been studied, it remains unknown at what time points in the postoperative rehabilitation period BFRT is most effective. In addition, there are limited data, specifically in high-level athletes, on the effect of BFRT on RTS timing. Our primary aim for this study was to compare RTS times in National Collegiate Athletic Association (NCAA) Division I athletes using either BFRT or traditional physical therapy rehabilitation after ACLR. Our secondary aim was to use strength metrics to search for specific time points in the postoperative period where BFRT is most effective. We hypothesized that the BFRT cohort would have faster RTS and that the benefit of this novel therapy would be maximized in the early postoperative period in this population.
Methods
Study Patients
The study protocol received institutional review board approval, and all participants provided written informed consent. Using training room data from 2000 to the present, 2377 NCAA Division I athletes at our institution who were diagnosed with any knee injury were initially identified. We included patients with student-athlete status who underwent primary ACLR while participating in Division I athletics at our institution and either received BFRT as part of their rehabilitation protocol after its implementation at our facility in 2017 (BFRT group) or underwent traditional physical therapy alone before that date (non-BFRT group). Patients who underwent revision ACLR had concomitant multiligamentous knee injuries, those who underwent treatment/rehabilitation at outside facilities, and those who had unrelated reasons for not returning to the sport were excluded. Patients with concomitant meniscal repair during ACLR or those with previous injuries were not excluded from study participation.
Of 105 student-athletes who underwent ACLR, 50 were excluded, and 55 were included in the final analysis. The 55 athletes included 22 patients in the BFRT group and 33 patients in the non-BFRT group. Figure 1 provides a summary of patient inclusion in the study.

A CONSORT flow diagram depicting the grouping and flow of patients in the study. ACLR, anterior cruciate ligament reconstruction; BRFT, blood flow restriction training; CONSORT, Consolidated Standards of Reporting Trials; HHD, handheld dynamometry; Quad HHD, quadriceps strength on a handheld dynamometer; RTS, return to sports.
A chart review of the training room’s electronic medical records was performed to obtain patient data. Age at the time of surgery, sex, sport, RTS, injured side, type of graft, and surgeon were recorded. Moreover, for the BFRT group, quadriceps strength testing using handheld dynamometry (HHD) at various postoperative time points was obtained. HHD testing was performed with 3 trials of each limb, always beginning with the unaffected extremity. The tested knee was flexed to 90°, with the thigh strapped down proximally, and the dynamometer placed 5 cm proximal to the tip of the lateral malleolus. Each HHD trial lasted roughly 6 seconds, with 30 seconds of recovery between trials. The HHD values were then expressed as a percentage of the strength of the operative limb compared with the unaffected limb (ie, a limb symmetry index [LSI]).
BFRT Protocol
BFRT was conducted using a Personalized Tourniquet System (Delfi Medical Innovations). Each BFRT session was performed with the tourniquet system inflated to 80% of occlusion pressure in the target limb, which was simultaneously measured with the device.
Each therapy session consisted of an initial set of 30 repetitions of a particular exercise, followed by 30 to 45 seconds of rest. Subsequently, each participant performed 3 to 5 sets of 15 repetitions, with 30 to 45 seconds of rest after each set. Occlusion was approximately 5 minutes for each particular exercise, with a 1-minute reperfusion period before the subsequent exercise. Generally, 2 to 3 exercises were performed per session throughout the rehabilitation period, with 3 to 4 sessions per week. The external load was progressively increased throughout the therapy session, within 20% to 50% of the participant's 1-RM. Each specific exercise, the initial load, and load progression were variable and dependent on the physical therapist's discretion and the participant's tolerance. Moreover, there were differences between participants in the exact time point at which BFRT was implemented postoperatively and the frequency of BFRT repetition. BFRT was used in some select cases preoperatively but not for all participants. Postoperative BFRT was initiated at the time of suture removal and continued until the athlete reached 90% strength of operative limb compared with unaffected limb (ie, 90% LSI).
Non-BFRT Protocol
Participants who did not participate in BFRT followed a traditional ACLR postoperative rehabilitation guideline. Athletes who underwent ACLR and rehabilitation before 2015 followed a surgeon-specific protocol, and the protocol for ACLR performed after 2015 was based on the guidance of the Multicenter Orthopaedic Outcome Network (MOON) panel. 37 However, each participant followed a regimen specific to the preferences of the surgeon who performed the ACLR, with updated adaptations determined by the participant's certified athletic trainer. Of note, progression from one phase to the next was based on the patient meeting the functional criteria of each phase and not on the time elapsed since surgery.
Data Analysis
All statistical analyses were performed using R software Version 4.0.3 (The R Project for Statistical Computing). The significance threshold was set at P < .05 for all statistical tests. Values are expressed as means ± standard deviations and relative frequency unless otherwise stated.
The mean values for the age at time of surgery and RTS between the BFRT and non-BFRT cohorts were compared using the Welch t test. Differences in sex, injured side, sport played, and autograft type between the cohorts were evaluated with the Fisher exact test. Given that HHD testing was very limited for the non-BFRT group, an analysis of quadriceps strength was only performed on the BFRT group. A mixed-effects linear regression model was used to assess changes in quadriceps strength over the study time course. Time effects were modeled linearly and expressed as rates of change compared with the previous 4-week time interval. The time to achieving thresholds of 50% LSI, 70% LSI, and 90% LSI in quadriceps strength for the BFRT group were calculated and depicted using Kaplan-Meier failure curves.
Results
In the BFRT cohort (n = 22), 17 patients had RTS data available, 18 patients had quadriceps HHD data available, and 15 patients had both data available. In the non-BFRT cohort (n = 33), all participants had RTS data, and only 3 patients had quadriceps HHD data available.
The patient characteristics according to the group are summarized in Table 1. All patients in the BFRT group and all but 1 patient in the non-BFRT group underwent bone-patellar tendon-bone (BTB) autograft ACLR. Women's soccer and football were the 2 largest cohorts of individual sport participants in both groups. The BFRT group consisted of 55% men versus 39% in the non-BFRT group. The age at surgery was significantly lower in the BFRT cohort versus the non-BFRT cohort (18.6 vs 19.5 years; P = .011). The mean RTS time was significantly longer for the BFRT compared with the non-BFRT group (409 vs 332 days; P = .047).
Comparison of Patient Characteristics in the BFRT and Non-BFRT Groups a
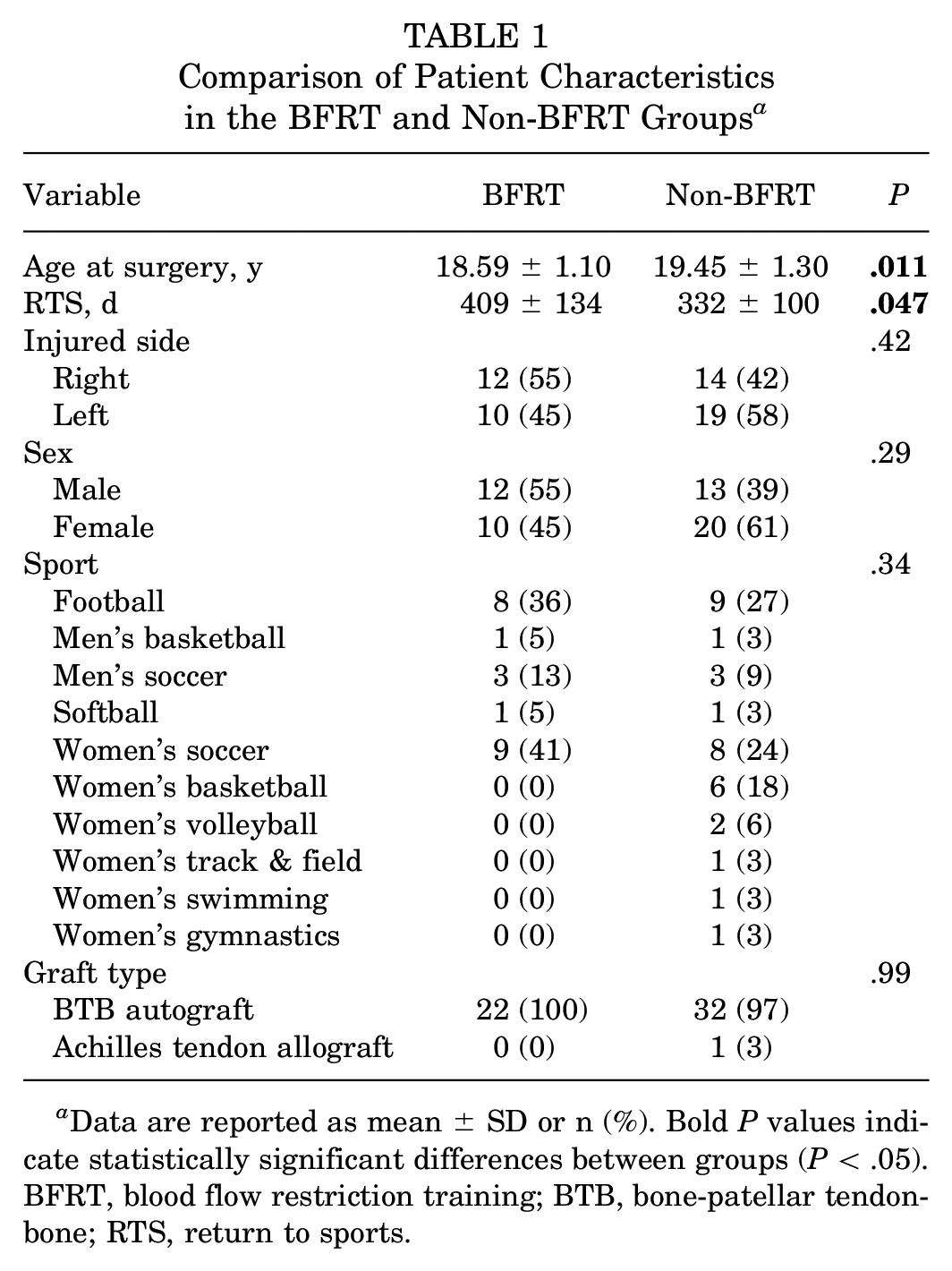
Data are reported as mean ± SD or n (%). Bold P values indicate statistically significant differences between groups (P < .05). BFRT, blood flow restriction training; BTB, bone-patellar tendon-bone; RTS, return to sports.
For the BFRT group, the mean quadriceps strength increased by 0.67% (95% CI, 0.53%-0.81%) every 1 week of rehabilitation. Rates of change in quadriceps strength LSI values per 4-week interval were then calculated with respect to the previous 4-week interval, with the first data points being measurements taken during postoperative weeks 5-8 (Table 2). A significant positive rate of change was seen in weeks 13-16 compared with the previous segment of weeks 9-12 (ΔLSI, 8.22%; P < .001). A significant increase was seen in the week 41-44 segment compared with the week 37-40 interval (ΔLSI, 9%; P = .008). Most intervals included in the study period had positive gains in quadriceps strength relative to the previous segment, but no others achieved statistically significant increases in quadriceps strength values (Figure 2.)
Rates of Change in the Mean Quadriceps Strength LSI for Sequential 4-Week Segments a

There were no values for postoperative weeks 0 to 4. Bold P values indicate statistical significance (P < .05). LSI, limb symmetry index.
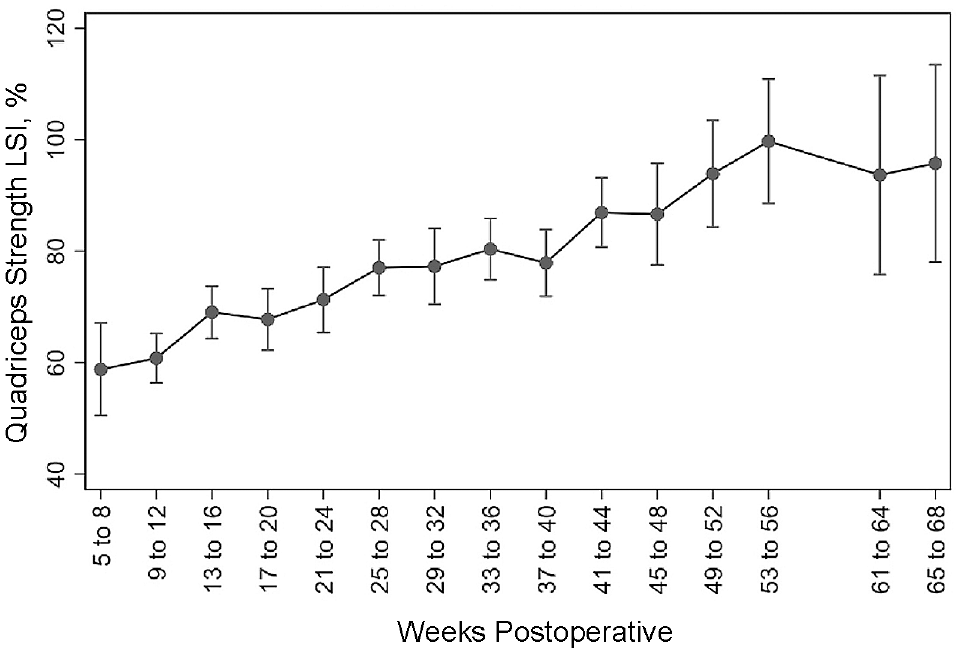
The mean quadriceps strength as measured on a handheld dynamometer, represented as a percentage compared with unaffected extremity (LSI) for each given 4-week postoperative time interval. Error bars represent 95% CIs. LSI, limb symmetry index.
The BFRT group had a 50% probability of reaching a quadriceps strength threshold of 50% LSI by 12 weeks and a >90% probability of meeting the same threshold by postoperative week 25 (Figure 3). In addition, the group had a 50% probability of attaining the 70% LSI threshold by roughly 22 weeks. Finally, the BFRT group had a 50% probability of achieving at least 90% LSI quadriceps strength measurements at roughly 52 weeks (1 year) postoperatively.
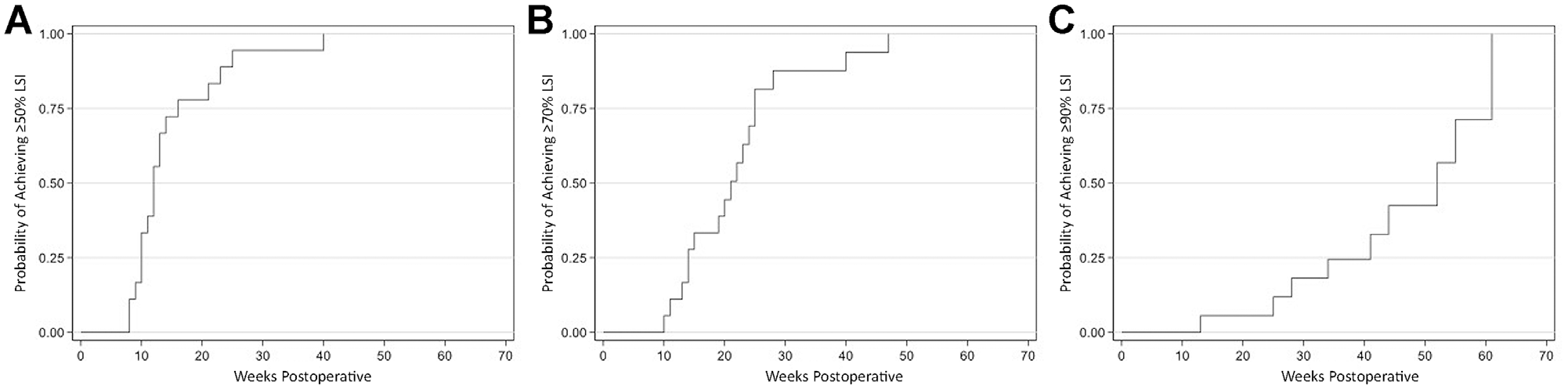
Kaplan-Meier failure curves for achieving quadriceps strength thresholds at various time points in the BFRT group. (A) Time to 50% LSI. (B) Time to 70% LSI. (C) Time to 90% LSI. LSI, limb symmetry index.
Discussion
Significantly longer RTS times with BFRT were found in our patient population than those with traditional physical therapy rehabilitation alone after ACLR (409 vs 332 days; P = .047). This result is similar to previous findings, showing numerous nonsuperior outcomes for BFRT in various knee pathologies.9,21,22 A recent randomized controlled trial investigating BFRT in the acute preoperative period showed no difference in quadriceps circumference, strength, or patient-reported outcome measures between BFRT and control groups. 29
However, the previous literature had generally indicated using BFRT in competitive athlete rehabilitation.1,23,33 For BFRT use after ACLR specifically, data from the 6 available trials have shown either significant improvement or no difference in various biomechanical and functional outcomes after ACLR, with no previous study assessing RTS times.10,12,15,19,25,39 Previous studies of RTS after ACLR in elite athletes have outlined a range of RTS of 6 to 13 months from surgery. 17 Our BFRT cohort had longer RTS times than the non-BFRT group, at 13.45 months after ACLR, which also falls outside the published range. Delayed RTS in the BFRT group may imply that BFRT might only improve strength and muscle bulk but not necessarily functional outcomes required to return to the preinjury level of sport. Furthermore, the extended RTS timeframe of BFRT may be secondary to the fact that the rehabilitation time spent on BFRT takes away from traditional rehabilitation methods that may ultimately be counterproductive in the recovery of an athlete. Beyond the timing and schedule of postoperative rehabilitation, there may also be unforeseen changes at the cellular level that can limit muscle function, proprioception, or tension production that have yet to be identified.
We additionally hypothesized that there would be significant improvements in quadriceps strength early in the postoperative rehabilitation course when patients theoretically would benefit most from low-resistance exercises after their reconstructive surgery. Our data showed that the time interval of weeks 13-16 had the first and most significant increase in quadriceps strength while utilizing BFRT (Figure 2). Pottkotter et al 20 investigated strength gains early in non-BFRT rehabilitation and first observed significant increases in quadriceps strength at the 12- to 24-week time point. Historically, BFRT has not been initiated before the end of postoperative week 4 to allow for soft tissue healing and improvements in surgical site inflammation. If initiated during week 5, one could expect these gains in quadriceps strength at postoperative weeks 13 to 16. Given our quadriceps strength data, there may be a benefit in utilizing BFRT therapy early in the postoperative rehabilitation process after ACLR.
In examining the Kaplan-Meier curves, our BFRT group, on average, had a 50% probability of reaching 70% LSI at roughly 22 weeks postoperatively. This compares to many traditional ACL rehabilitation protocols, which estimate progression past a threshold of 70% to 80% LSI by16,31,32 weeks 12-16. In addition, our BFRT group had a 50% probability of reaching 90% LSI by 52 weeks postoperatively and had at least a 90% chance of reaching the same threshold by 65 weeks. It is generally expected that an athlete reaches the 85% to 90% LSI threshold before obtaining full medical clearance to RTS.
Limitations
There are several limitations to consider when interpreting the results of this study. Although there was a standardized inflation pressure used for BFRT at our institution, there was a notable variability in both BFRT and non-BFRT physical therapy rehabilitation. These both depended on many factors, including but not limited to surgeon-specific protocols, clinical judgment of supervising physical therapists, and timing of therapy sessions within the postoperative period. The participants who underwent non-BFRT rehabilitation before 2015 did not necessarily follow the standardized MOON protocol, as those after 2015 did, and this may have led to greater interparticipant variation in rehabilitation. Moreover, our study did not include sufficient HHD data for the non-BFRT group; therefore, we could not evaluate any difference in quadriceps strength between groups. Also, no information was available on hamstring strength progression over the rehabilitation period for our athletes, which contributes to limb function postoperatively.
The study design itself also has its limitations. This is a retrospective study, with a nonrandom selection into BFRT and non-BFRT groupings. The 2 cohorts did not have significantly different composition of sex and sport participation of participants, but patients were not randomized to each group so groups were consequently prone to bias. A causal relationship between BFRT and the primary outcomes of RTS time cannot be obtained through this retrospective study design, and we can only describe a general association or trend. Future prospective, randomized, controlled studies surrounding the implementation of BFRT in collegiate or professional athletes would need to be conducted to best elucidate a cause-effect relationship between the intervention and the outcome.
In addition, the primary outcome measure of RTS has its considerations. Medical clearance for full participation in a sport depends on many factors, including physician availability, scheduling appointments around major summer and winter academic breaks, and timing of the season relative to the injury and targeted return date. There may be less urgency to RTS in the early off-season period than leading up to the beginning of the respective season. An additional limitation of this study surrounds the external validity. Our study population is a very unique patient group of high-performance athletes. Consequently, it may be only applicable to comparable collegiate and/or professional athletes and less generalizable to the average patient undergoing ACLR.
Conclusion
To our knowledge, this is the first study to investigate RTS times with BFRT compared with standardized physical therapy alone in the collegiate athlete patient population. Our data led us to conclude that in elite NCAA Division I athletes, there were significantly longer RTS times with BFRT compared with standardized physical therapy alone after undergoing ACLR. BFRT may have the most therapeutic benefit and showed the largest gains in quadriceps strength between postoperative weeks 13-16 and 41-44. There is an apparent need for additional prospective studies to establish a protocol of progressive load management while utilizing BFRT to better understand and maximize the benefit of this relatively new therapeutic modality. However, given the results of this study, BFRT should be used with caution in this population before conducting future randomized control trials.
Footnotes
Final revision submitted October 24, 2023; accepted November 13, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.K.D. has received hospitality payments from Stryker. C.A.S. has received education payments from Saxum Surgical. K.J.J. has received education payments from Saxum Surgical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from University of California at Los Angeles (ref No. 20-002138).