
Abstract
Background:
A subchondral stress fracture of the femoral head (SSFFH) is managed with nonoperative treatment. There is a lack of knowledge regarding whether hip arthroscopic management is effective for active patients with SSFFHs.
Purpose:
To elucidate whether arthroscopic management of SSFFHs enables active patients to return to sports activity.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 22 patients undergoing hip arthroscopic management (labral repair/reconstruction and fragment fixation with hydroxyapatite and poly-L-lactic acid [HA/PLLA]–threaded pins) were enrolled and divided into 2 groups. The active group was defined as patients who participated in any kind of sports, regardless of the level of competition. The inactive group was defined as patients who did not participate in sports or any activity. Patient-reported outcome measure (PROM) scores, including the modified Harris Hip Score (mHHS) and Non-Arthritic Hip Score (NAHS), were collected preoperatively and at 6 months, 12 months, and the final follow-up (mean, 70.0 ± 36.6 months [range, 24-144 months]) after surgery. The authors performed chi-square and Mann-Whitney U tests to compare the PROM scores between the 2 groups.
Results:
There were 10 patients in the active group and 12 patients in the inactive group in the final analysis. Overall, 14 SSFFHs underwent internal fixation with HA/PLLA–threaded pins. The PROM scores significantly improved from preoperatively to the final follow-up. The active group had significantly better PROM scores than the inactive group at 6 months (mHHS: 96.6 ± 5.0 vs 85.3 ± 13.6, respectively [P = .033]; NAHS: 74.3 ± 6.4 vs 57.0 ± 15.6, respectively [P = .008]) and 1 year (mHHS: 98.8 ± 1.8 vs 92.7 ± 8.6, respectively [P = .040]; NAHS: 78.0 ± 2.1 vs 65.9 ± 11.7, respectively [P = .007]). Additionally, 9 of 10 patients in the active group returned to their sports activity.
Conclusion:
The study showed that arthroscopic management (femoroacetabular impingement correction, labral preservation, and stabilization with HA/PLLA–threaded pins) provided favorable clinical outcomes and a high rate of return to sports activity in active patients with SSFFHs. Active patients with SSFFHs had better postoperative results than inactive patients.
Keywords
A subchondral stress fracture of the femoral head (SSFFH) is an uncommon cause of acute hip pain and is different from osteonecrosis of the femoral head.1,20 It is crucial for practitioners to distinguish an SSFFH from avascular necrosis of the femoral head. Magnetic resonance imaging (MRI) findings are useful for the differentiation between osteonecrosis of the femoral head and an SSFFH. Both conditions may initially present with a bone marrow edema pattern on MRI. SSFFHs typically present as low-intensity signal lines serpiginous and parallel to the articular surface with a high-intensity signal proximal to the fracture line on fat-suppressed MRI. 28 On the other hand, avascular necrosis is revealed as well-defined focal lesions with a low-intensity band concave (crescent sign) to the articular surface with the absence of a high-intensity signal proximal to the band on fat-suppressed MRI. 28 A recent study reported that SSFFHs can occur in military recruits and patients with osteoporosis. 26 An SSFFH consists of a subchondral insufficiency fracture of the femoral head and subchondral fatigue fracture of the femoral head. A subchondral insufficiency fracture of the femoral head occurs in patients whose bone quality is abnormal because of osteoporosis or other causes, and a subchondral fatigue fracture of the femoral head occurs in healthy adults with normal bone quality who experience greater than average stress. 20 Patients usually have acute onset of pain after a minor injury, and prolonged untreated SSFFHs can result in the rapid progression of osteoarthritis of the hip joint.3,26
The early phase of an SSFFH is typically managed with nonoperative treatment, including nonweightbearing with crutches to minimize adverse mechanical stress against the injured femoral head and nonsteroidal anti-inflammatory agents. 26 Although some patients improve with nonoperative treatment, many cases progress to femoral head collapse, despite a prolonged period of nonweightbearing. 13 Although transtrochanteric rotational osteotomy has been reported to have favorable results for patients with SSFFHs, 26 it takes approximately 6 months before full weightbearing is permitted. Additionally, a disadvantage of this procedure is that total hip arthroplasty is more complicated when collapse occurs after osteotomy.
On the other hand, recent studies have shown that a precollapse SSFFH is associated with labral abnormalities and can be managed by arthroscopic labral preservation, fragment fixation with hydroxyapatite and poly-L-lactic acid (HA/PLLA)–threaded pins, and capsular repair.3,22 A pilot study by Ishihara et al 11 demonstrated that an SSFFH is associated with femoroacetabular impingement (FAI). More recently, a case report has shown that SSFFHs occurred in patients with overcoverage of the acetabular rim, which can be implicated in the pincer type of impingement. 14 A study showed that 8 of 9 patients with rapidly progressive hip osteoarthritis associated with SSFFHs had inverted labral tears. 4 Because an SSFFH is more prevalent in active patients (who participate in any kind of sports) than in inactive patients, a better understanding of the clinical outcomes and a comparative investigation of arthroscopic treatment options are important. However, there is limited knowledge regarding whether hip arthroscopic management is effective for active patients with SSFFHs.
The purpose of this study was to elucidate whether arthroscopic management, including FAI 27 correction, labral preservation, and internal fixation with bioabsorbable pins, for SSFFHs enables active patients to return to sports activity. It was hypothesized that arthroscopic internal fixation of SSFFHs, labral repair, and FAI correction would provide favorable clinical outcomes and a high rate of return to sports.
Methods
This study was approved by our institutional review board (No. B21-026). Between 2011 and 2018, a total of 30 patients who underwent arthroscopic management for SSFFHs were retrospectively reviewed. Surgical management was indicated for patients who requested surgery because of groin pain that did not improve, despite nonoperative treatment for >3 months. No patients had a history of hip surgery. Patients who were available for follow-up for at least 2 years after surgery were included. There were 8 patients excluded (mental disorder, spinal disorder, knee surgery, <2 years of follow-up, loss to follow-up within 1 year). Thus, 22 hips from 22 patients (12 men and 10 women; mean age, 46.9 ± 12.4 years [range, 16-68 years]) were enrolled in this study. The 22 patients were divided into 2 groups according to their participation in sports. There were 10 active patients (1 professional level, 2 competitive level, and 7 recreational level) and 12 inactive patients (Figure 1). The active patients participated in marathons, soccer, surfing, bicycle races, golf, tennis, mountain climbing, or rhythmic gymnastics. The inactive patients did not participate in any sports or activity, and their activities were limited to daily life.

Flowchart of the recruitment of patients with subchondral stress fractures of the femoral head (SSFFHs). MPFL, medial patellofemoral ligament.
The diagnosis of an SSFFH was based on a comprehensive history of hip pain without any instance of major trauma; normal radiographs regarding the femoral head (Figure 2A); a fracture line parallel to the articular surface on computed tomography (Figure 2D); a subchondral low-intensity signal band that was irregular, serpiginous, and parallel to the articular surface on proton density– or T1-weighted MRI (Figure 2E); and a diffuse bone marrow edema pattern on oblique sagittal or coronal views on MRI (Figure 2F). 26 Patients with osteonecrosis and osteochondritis dissecans of the femoral head were excluded.

A 34-year-old male surfer presented with a 4-month history of increasing right groin pain. He had limited range of motion of 90° of flexion and 30° of abduction. (A) Anterior-posterior pelvic radiographic view shows a lateral center-edge angle of 43°. There was no visible fracture line or loss of sphericity of the femoral head. (B) Modified Dunn radiographic view and (C) cross-table lateral radiographic view show an alpha angle of 70° and 49°, respectively (circles). (D) Coronal view on computed tomography shows a curved hairline (arrows) fracture parallel to the articular surface of the femoral head. (E) Coronal proton-density-weighted magnetic resonance imaging (MRI) shows a hypointense band parallel to the subchondral region along the femoral head (arrow). (F) Coronal view on proton density–weighted fat-suppressed MRI shows a diffuse high-intensity area, suggesting a bone marrow edema pattern.
Clinical inclusion criteria suggestive of SSFFH-related bony abnormalities, including FAI and borderline developmental dysplasia of the hip (BDDH), were groin pain for >3 months, restricted hip range of motion (flexion <105° and/or restricted internal rotation in flexion <20°), a positive flexion–abduction–external rotation test finding, and a positive flexion–adduction–internal rotation test finding.
Radiological evidence of a cam deformity consisted of an alpha angle >55° or head-neck offset <8 mm on at least 1 radiographic view, computed tomography, or MRI, 2 and radiological evidence of a pincer deformity consisted of a lateral center-edge angle (LCEA) >25° on the anterior-posterior pelvic radiographic view plus a crossover sign, coxa profunda, or posterior wall sign, with an ischial spine sign or an LCEA >40° or Tönnis angle <0° indicating global pincer-type FAI.4,29 Patients with an LCEA ranging between 20° and 24° were diagnosed with BDDH. 6 Avulsions of the anterior inferior iliac spine (AIIS) were classified into 3 variants based on the classification proposed by Hetsroni et al 7 : type I when there was a smooth ilium wall between the AIIS and the acetabular rim, type II when the AIIS extended to the level of the rim, and type III when the AIIS extended distally to the acetabular rim.
Surgical Techniques
Hip arthroscopic surgery was performed with the patient in the supine position on a traction table with a well-padded peroneal post. An anterolateral portal and proximal midanterior portal (PMAP) were established. After intraportal capsular release, intra-articular abnormalities, including SSFFHs, labral tears, and any associated injuries, were assessed. If an acetabular labral tear and/or associated cartilage delamination was observed (Figure 3A), labral refixation was performed with bioabsorbable suture anchors (Figure 3B).
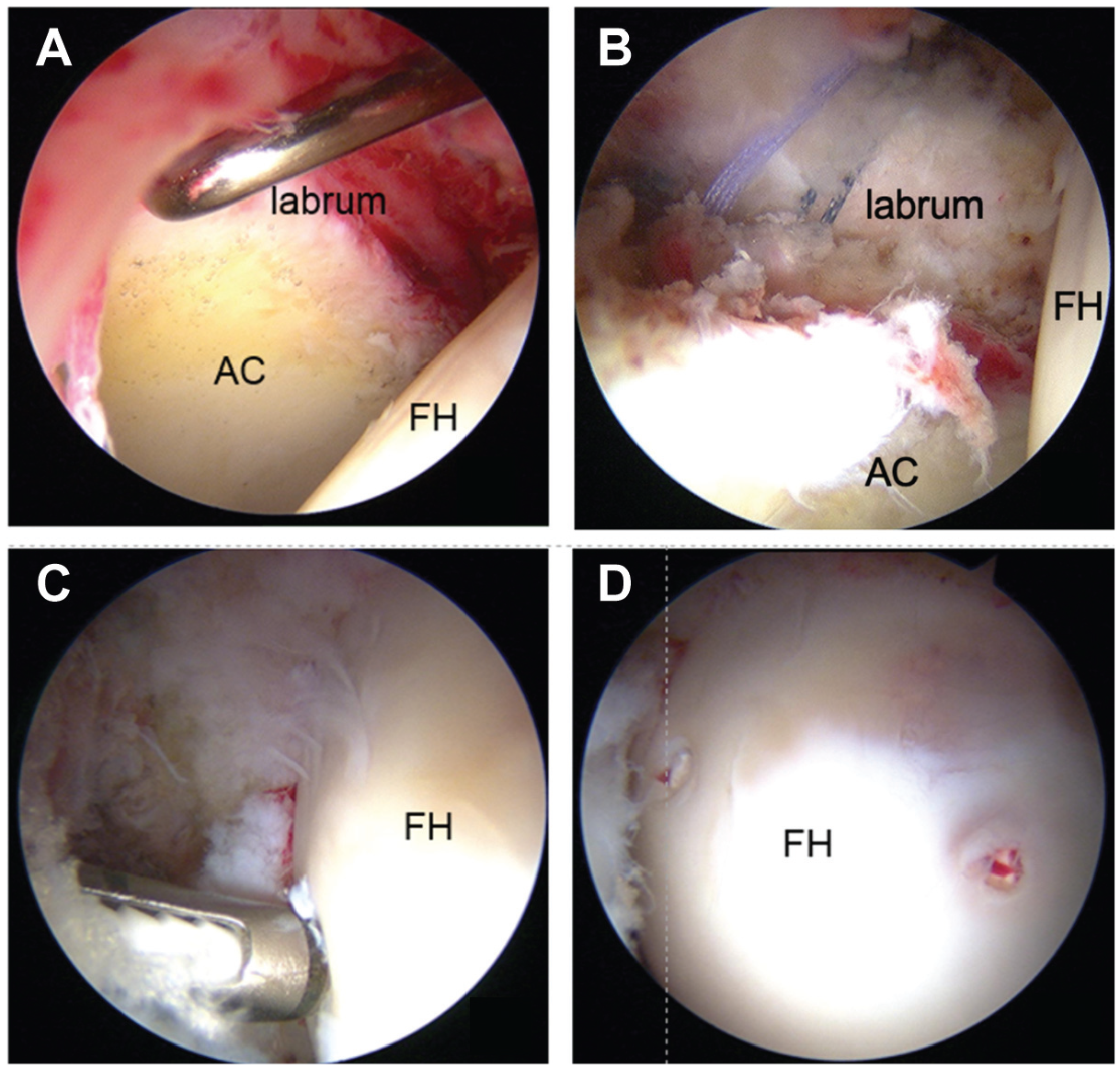
Arthroscopic findings. (A) Supine arthroscopic view from the anterolateral portal (ALP) shows anterosuperior labral tearing. (B) Supine arthroscopic view from the ALP shows labral repair via 4 sutures with 2 anchors. (C) Supine arthroscopic view from the ALP shows internal fixation of a subchondral stress fracture of the femoral head (SSFFH) with SuperFixsorb-threaded pins introduced via the drill guide through the proximal midanterior portal (PMAP). (D) Supine arthroscopic view from the PMAP shows a stable SSFFH after fixation with 2 hydroxyapatite and poly-L-lactic acid–threaded pins. AC, acetabulum; FH, femoral head.
During central compartment procedures, the SSFFH was assessed by viewing from the anterolateral portal. The location of the SSFFH was assessed using the geographic zone method, and the SSFFH was categorized according to the Uchida classification system (Table 1).10,22
Uchida Classification System for Subchondral Stress Fractures of the Femoral Head 22

The PMAP was established to access the SSFFH. If the SSFFH was located in the weightbearing area, the hip was hyperextended 10°. If the SSFFH was determined to be grade 1C or 2A, arthroscopic fixation of the SSFFH was then performed using HA/PLLA–threaded pins (SuperFixsorb; Takiron). A tamp (DePuy Synthes) was utilized to insert the HA/PLLA–threaded pins. A 2-mm drill guide was introduced through the PMAP under arthroscopic guidance (Figure 3C). The guide hole was initiated with a custom-made dilator bit. Drilling was advanced to the desired depth using a 2.0-mm Kirschner wire. The dilator was inserted into the drill guide and tapped to the desired depth. The HA/PLLA–threaded pins were then advanced through the drill guide with a delivery tamp to fix the SSFFH (Figure 3, C and D). Typically, 2 or 3 HA/PLLA–threaded pins were needed, especially for unstable (grade 1C) SSFFHs. After the release of traction, cam osteochondroplasty was performed using a motorized round bur when indicated. Finally, arthroscopic capsular repair (double shoelace technique 23 ) was performed using Ultratape (Smith & Nephew). 24
Postoperative Rehabilitation Protocol
Patients remained nonweightbearing for 4 weeks. After 4 weeks, weightbearing was gradually increased, with full weightbearing by 8 weeks after surgery. Endurance strengthening began at 16 weeks postoperatively after range of motion and control of the lower extremities were achieved.
Radiographic Parameters
We assessed the preoperative radiographs of the 22 patients (22 hips). All radiographic measurements were manually performed by 2 authors (S.U. and Y.O.) using a picture archiving and communication system. We determined the LCEA, the Tönnis angle, the femoral neck shaft angle, and the vertical-center-anterior angle on the false profile view and the alpha angle on the cross-table lateral view or modified Dunn view (Figure 2, A-C).15,16,25 We also evaluated all preoperative and annual postoperative radiographs for osteoarthritic changes using the Tönnis classification system (Tönnis grade). 21
The interobserver and intraobserver reproducibility of these radiographic parameters were investigated. For interobserver reliability, 2 hip surgeons (Y.M and H.N.) blinded to the clinical data and details of the radiology reports independently assessed each radiograph. For intraobserver reliability, 1 hip surgeon (Y.M.) independently assessed the radiographs 3 separate times, with at least 1 week between measurements. Interclass correlation coefficients (ICCs) and corresponding 95% confidence intervals were calculated to quantify interobserver and intraobserver reliability for continuous variables. The strength of agreement was interpreted as follows: ICCs >0.80 indicated almost perfect agreement, ICCs of 0.61-0.80 indicated substantial agreement, ICCs of 0.41-0.60 indicated moderate agreement, and ICCs of 0.21-0.40 indicated fair agreement. We assessed the interobserver and intraobserver reliability of the radiographic measurements. The interobserver and intraobserver ICCs for the LCEA were 0.991 and 0.916, respectively; for the Tönnis angle were 0.956 and 0.974, respectively; for the femoral neck shaft angle were 0.874 and 0.702, respectively; for the vertical-center-anterior angle were 0.985 and 0.951, respectively; and for the alpha angle were 0.939 and 0.874, respectively.
Clinical Outcomes
Patient-reported outcome measure (PROM) scores, including the modified Harris Hip Score (mHHS), the Non-Arthritic Hip Score (NAHS), and the 12-item International Hip Outcome Tool (iHOT-12), were collected preoperatively and at 6 months, 12 months, and the final follow-up (mean, 70.0 ± 36.6 months [range, 24-144 months]) after surgery. The minimal clinically important difference (MCID) for the mHHS, NAHS, and iHOT-12 was also calculated by the distraction method. 19 We typically allowed athletes to return to full competitive activity between 16 and 24 weeks after surgery. Return to competitive sports depended on whether there was pain-free recovery of muscle function and strength, which we determined by a retrospective chart review and personal follow-up communication with the active patients.
Statistical Analysis
A power analysis was performed using G*Power (Version 3.1; Universität Dusseldorf). Power analysis using data from an initial 5 patients demonstrated that a minimum sample size of 4 patients produced significantly different results between the preoperative and postoperative mHHS scores (Wilcoxon rank-sum test; alpha = .05; effect size = 3.04; actual power = 0.95). We used chi-square and Mann-Whitney U tests to compare clinical scores between the 2 groups. We compared radiographic measurements, including the LCEA, the Tönnis angle, and the alpha angle, using the Mann-Whitney U test. We presented these values as the mean and standard deviation. The Student t test, paired t test, or Fisher exact test and the Bonferroni correction were utilized for statistical analysis. We performed statistical analyses using the SPSS software package (Version 13; IBM), and a P value of <.05 was considered statistically significant.
Results
A total of 22 patients with 22 hips met the inclusion criteria with a minimum of 2 years of follow-up (10 in the active group and 12 in the inactive group). No patients had a history of hip surgery. The mean age was 46.9 years (range, 16-68 years) at the time of surgery. The mean body mass index was 23.7 kg/m2.
Relevant preoperative hip examination findings are summarized in Table 2. The active group had a significantly higher proportion of male patients compared with the inactive group (90% vs 25%, respectively; P = .004). No significant differences between the active group and inactive group were observed regarding imaging findings (Table 2).
Patient Characteristics a

Data are presented as mean ± SD unless otherwise indicated. AIIS, anterior inferior iliac spine; LCEA, lateral center-edge angle.
P values were calculated for comparisons between the active and inactive groups using the Student t test, Fisher exact test, and Mann-Whitney U test.
Intra-articular findings, including SSFFHs and status of acetabular articular cartilage and the labrum, are shown in Table 3. Labral tears were found in all patients, and labral repair was performed in all 22 hips using suture anchors. An SSFFH was observed in all cases. Overall, 8 SSFFHs (grade 1A or 1B) of 8 hips were left in situ, and 14 SSFFHs were internally fixed using HA/PLLA–threaded pins (2.8 ± 1.1 pins per case). The rate of requiring internal fixation of SSFFHs was higher in the inactive group than in the active group but did not reach statistical significance (83% vs 40%, respectively; P = .074) (Table 3).
Arthroscopic Findings and Treatment a

Data are presented as n (%) or mean ± SD unless otherwise indicated. HA/PLLA, hydroxyapatite and poly-L-lactic acid; ICRS, International Cartilage Repair Society; MAHORN, Multicenter Arthroscopy of the Hip Outcomes Research Network; SSFFH, subchondral stress fracture of the femoral head.
P values were calculated for comparisons between the active and inactive groups using the Student t test, chi-square test, Fisher exact test, and Mann-Whitney U test.
At a mean of 28.8 ± 14.7 months after surgery, the PROM scores of both the active group (mHHS: from 68.6 ± 15.2 to 99.0 ± 1.6 [P < .001]; NAHS: from 49.8 ± 13.7 to 73.7 ± 12.1 [P < .001]; iHOT-12: from 36.7 ± 19.4 to 90.4 ± 16.2 [P < .001]) and inactive group (mHHS: from 53.9 ± 21.1 to 95.1 ± 7.8 [P < .001]; NAHS: from 35.2 ± 16.2 to 71.6 ± 11.7 [P < .001]; iHOT-12: from 23.3 ± 14.1 to 87.1 ± 16.1 [P < .001]) were significantly improved from preoperatively to postoperatively (Figure 4).

Changes in patient-reported outcome measure scores. (A) Comparison of the active group and the inactive group in terms of preoperative and postoperative modified Harris Hip Score (mHHS) scores. In both groups, there was a significant improvement at 6 months, 1 year, and 2 years after surgery compared to preoperatively (Prop). (B) Comparison of the preoperative and postoperative Non-Arthritic Hip Score (NAHS) scores of the active group and the inactive group. In both groups, there was a significant improvement at 6 months, 1 year, and 2 years after surgery compared to preoperatively. (C) Comparison of the active group and the inactive group in terms of preoperative and postoperative 12-item International Hip Outcome Tool (iHOT-12) scores. In both groups, there was an improvement at 6 months, 1 year, and 2 years after surgery compared to preoperatively.
The active group had significantly better PROM scores than the inactive group at 6 months (mHHS: 96.6 ± 5.0 vs 85.3 ± 13.6, respectively [P = .033]; NAHS: 74.3 ± 6.4 vs 57.0 ± 15.6, respectively [P = .008]) and 1 year (mHHS: 98.8 ± 1.8 vs 92.7 ± 8.6, respectively [P = .040]; NAHS: 78.0 ± 2.1 vs 65.9 ± 11.7, respectively [P = .007]); however, the PROM scores at the final follow-up were not significantly different (P > .1).
Of 10 patients in the active group, 9 were able to return to sports activity at the same level or higher level at a mean of 6.6 ± 2.6 months after surgery; 8 patients returned to the same sports activity, and 1 patient changed sports from rhythmic gymnast to lacrosse. Characteristics of the active group are presented in Table 4. No total hip replacement conversion was required at 1 year or 2 years. No radiographic osteoarthritic progression was observed using the Tönnis grade. MRI at 1 year after surgery showed that bone marrow edema completely resolved, and SSFFHs successfully healed in all patients (Figure 5).
Patient Characteristics of Active Group a

SSFFH, subchondral stress fracture of the femoral head.
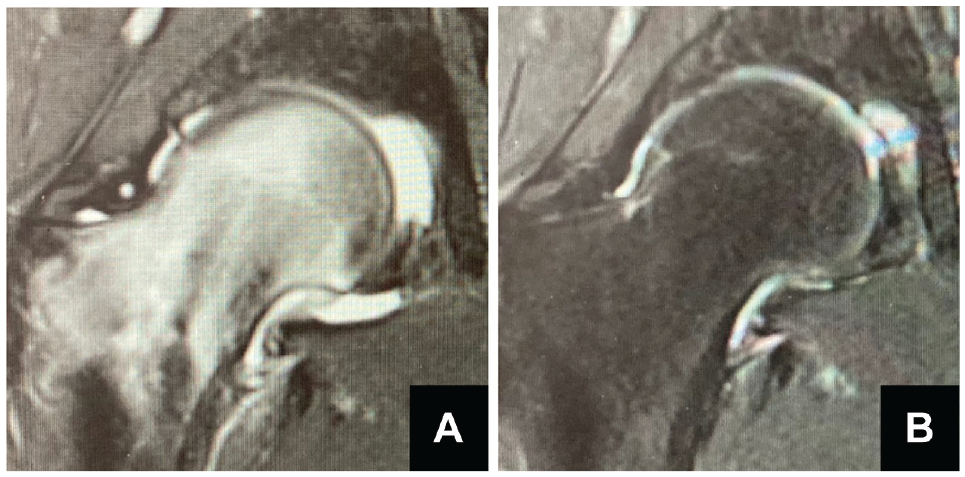
Comparison of preoperative and postoperative magnetic resonance imaging (MRI). (A) Coronal view on preoperative short tau inversion recovery MRI shows a diffuse high-intensity area, suggesting a bone marrow edema pattern. (B) Coronal view on MRI at 1 year after surgery shows that bone marrow edema completely resolved and subchondral stress fractures of the femoral head successfully healed.
The MCID was 9.7 for the mHHS, 8.1 for the NAHS, and 8.7 for the iHOT-12. For the mHHS, 22 patients (100.0%) achieved the MCID. For the NAHS, 19 patients (86.4%) achieved the MCID. For the iHOT-12, 20 patients (90.9%) achieved the MCID. There were no significant differences in achievement rates of the MCID between the active group and the inactive group (Table 5).
Achievement of MCID a

Data are presented as n (%). iHOT-12, 12-item International Hip Outcome Tool; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; NAHS, Non-Arthritic Hip Score.
P values were calculated for comparisons between the active and inactive groups using the chi-square and Fisher exact tests.
Discussion
The main findings of this study are as follows: arthroscopic management, including arthroscopic FAI correction, labral preservation, and internal fixation with HA/PLLA–threaded pins, for SSFFHs provided clinical benefits, even for active patients. Although there were no significant differences between the active and inactive groups in mHHS (99.0 ± 1.6 vs 95.1 ± 7.8, respectively; P > .1) and NAHS (73.7 ± 12.1 vs 71.6 ± 11.7, respectively; P > .1) scores at the final follow-up, the mean mHHS and NAHS scores in the active group at 6 months (mHHS: 96.6 ± 5.0 vs 85.3 ± 13.6, respectively [P = .033]; NAHS: 74.3 ± 6.4 vs 57.0 ± 15.6, respectively [P = .008]) and 12 months (mHHS: 98.8 ± 1.8 vs 92.7 ± 8.6, respectively [P = .040]; NAHS: 78.0 ± 2.1 vs 65.9 ± 11.7, respectively [P = .007]) were significantly higher than those in the inactive group. Additionally, 90% of active patients were able to return to sports activity at 6 months after surgery. A significantly higher proportion of active patients than inactive patients were men, and the active patients tended to have a larger alpha angle.
All patients with SSFFHs who met the inclusion criteria had labral tears associated with bony abnormalities (BDDH and FAI). Uchida et al 22 also noted in a series of 9 cases involving SSFFHs that all patients exhibited labral tears. This observation suggests a potential association between SSFFHs and hip microinstability, possibly stemming from labral tears. It is widely acknowledged that labral tears can contribute to hip microinstability and may eventually lead to the development of hip osteoarthritis. 12 However, it should be noted that the causal relationship between labral tears, hip microinstability, and SSFFHs remains an area for further investigation, as it is still uncertain whether one condition directly precedes or exacerbates the other. 12 Based on the aforementioned evidence, we consider that basic management of SSFFHs should involve the treatment of concurrent labral tears. Indeed, Uchida et al 22 reported that hip arthroscopic surgery enabled them to treat SSFFHs and concurrent intra-articular abnormalities. Our findings indicate that internal fixation combined with FAI correction and labral preservation can be effective for treating unstable SSFFHs, such as grade 1C or 2A, whereas FAI correction and labral preservation without pin fixation can be effective for treating stable SSFFHs, such as grade 1A or 1B.
In this study, it was observed that the mean mHHS and NAHS scores at 6 months and 12 months were notably greater in active patients compared to inactive patients. However, it is worth considering that various factors such as differences in muscle strength, age, and sex ratio between the 2 groups of patients might have influenced these outcomes. Importantly, certain studies have indicated a correlation between preoperative and postoperative muscle strength and clinical outcomes after total hip arthroplasty.8,9 Although the muscle strength of participants was not directly assessed in our study, it remains plausible that greater muscle strength among active patients could contribute to improved postoperative patient-reported outcomes. However, it is essential to acknowledge that this assumption warrants further investigation, as it has not been adequately explored within the scope of this research. Therefore, a more comprehensive examination of these potential confounding variables is necessary to better understand their impact on the observed clinical outcomes.
The indication for internal fixation with HA/PLLA–threaded pins in SSFFHs was based on the arthroscopic classification of SSFFHs (grade 1C). The rate of patients requiring internal fixation tended to be higher in the inactive group possibly because of a higher proportion of grade 1C cases in the inactive group compared to the active group. Patient characteristics revealed that active patients tended to have a larger alpha angle and a higher body mass index, while inactive patients comprised more female patients and older patients. These demographic variances suggest potential differences in the mechanism of SSFFHs between the active and inactive groups. In the active group, we considered that hip microinstability resulting from labral tears caused by large cam lesions would contribute to SSFFHs. Conversely, in inactive patients, hip microinstability induced by degenerative labral tears associated with aging and osteoporosis could be implicated in the development of SSFFHs. Considering these distinctions, it becomes evident that an SSFFH may manifest through different pathways based on patient activity levels and underlying hip cartilage and bony conditions. Further study is necessary to focus on microinstability, and its implications in the cause of SSFFHs would offer readers a clearer understanding of these complex relationships.
This study revealed that arthroscopic management of SSFFHs enabled most active patients to return to sports at 6 months after surgery. It is suggested that this surgical treatment is beneficial for early return to sports in active patients. Because long-term nonweightbearing reduces muscle strength 18 and results in a delay in recovery to the competitive level, practitioners should consider immediate arthroscopic management including inspection, labral preservation, cam osteoplasty, and internal fixation (if grade ≥1C). Further studies are needed to investigate the optimal treatment approach and the best timing to perform surgery in active patients.
Although there were no significant differences in achievement rates of the MCID between the active group and the inactive group, a high MCID achievement rate was obtained in both groups. Nwachukwu et al 17 reported that 283 patients who underwent primary hip arthroscopic surgery for the treatment of FAI with >5 years of follow-up achieved high MCID and Patient Acceptable Symptom State rates for the mHHS and iHOT-12. Similarly, a high MCID achievement rate for arthroscopic management of SSFFHs would suggest that this procedure should be effective in these patients.
Limitations
The present study has several limitations. First, because this was a retrospective study from a single institution, a prospective investigation is needed for further analysis. Second, the mHHS has a significant ceiling effect. 5 Third, there was a difference in the level of sports participation among patients in the active group, with 7 of 10 active patients participating at a recreational level. Fourth, the active group had a significantly higher rate of male patients. The higher proportion of male patients in the active group could have affected the differences in clinical outcomes between the groups. Fifth, we believe that labral tears can lead to hip microinstability, but because the diagnostic criteria for hip instability remain controversial, the term “hip instability due to labral lacerations” is not accurate. Further research is needed on hip microinstability. Sixth, the effectiveness of internal fixation of SSFFHs itself is not clear because not all cases underwent internal fixation, and all patients underwent labral repair. It is difficult to determine whether labral repair is the key factor for improvement. Last, the number of included patients was relatively small. Because of the small number of patients, the Patient Acceptable Symptom State was not calculated, as we could not obtain satisfaction data from all patients in this study.
Conclusion
Our study showed that arthroscopic management (FAI correction, labral preservation, and stabilization with HA/PLLA–threaded pins) provided favorable clinical outcomes and a high rate of return to sports activity in active patients with SSFFHs. Active patients with SSFFHs had better postoperative results than inactive patients.
Footnotes
Final revision submitted April 20, 2024; accepted May 2, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.U. has received consulting fees from Smith+Nephew and CONMED. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from University of Occupational and Environmental Health (B21-026).