
Abstract
Background:
Female patients undergoing surgery for femoroacetabular impingement syndrome (FAIS) often experience inferior clinical outcomes and higher failure rates when compared with male patients. The influence of athletic status on hip arthroscopic outcomes in female patients, however, is unclear.
Purpose:
To compare patient-reported outcomes (PROs) of athletic and nonathletic female patients undergoing hip arthroscopic surgery for FAIS, and to determine the return-to-sports rate in the athlete group.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Two-year PROs were assessed in female patients who had undergone hip arthroscopic surgery for FAIS by a single surgeon. Patients who self-identified as athletes were compared with nonathletes. Preoperative and postoperative PRO scores including the Hip Outcome Score–Activities of Daily Living (HOS-ADL), Hip Outcome Score–Sport-Specific (HOS-SS), modified Harris Hip Score (mHHS), and visual analog scale (VAS) for pain and satisfaction were analyzed and compared between athletes and nonathletes. Subanalysis was performed based on patient age and body mass index (BMI).
Results:
A total of 330 female patients undergoing hip arthroscopic surgery for FAIS were identified. Of these, 221 patients identified as athletes (mean age, 29.1 ± 11.1 years; mean BMI, 23.0 ± 3.5 kg/m2) and 109 as nonathletes (mean age, 39.3 ± 11.4 years; mean BMI, 27.8 ± 5.8 kg/m2). Both groups demonstrated improvements in HOS-ADL, HOS-SS, mHHS, VAS for pain, and VAS for satisfaction scores (P < .001 for all). Athletes had significantly higher postoperative PRO scores compared with nonathletes (P < .001 for all). A 1:1 matched-pair subanalysis of 97 athletes and 97 nonathletes controlling for age and BMI indicated that these relationships held independently of potential demographic confounders (P < .001 for all). The number of patients meeting the minimal clinically important difference (MCID) and patient acceptable symptomatic state (PASS) for the HOS-ADL, HOS-SS, and mHHS was significantly higher in athletes aged ≤25 years versus those aged >25 years and for athletes versus nonathletes (P < .05 for all). Further, 189 of 194 athletes returned to sports at a mean of 6.0 ± 3.9 months postoperatively, with 93.7% reporting returning to the same or higher level of competition.
Conclusion:
Among female patients undergoing hip arthroscopic surgery for FAIS, patients considered athletes achieved superior clinical outcomes compared with patients considered nonathletes. In addition, younger female athletes had higher rates of achieving the MCID and PASS for all PRO measures.
Keywords
Hip arthroscopic surgery has become an increasingly utilized treatment modality for hip preservation in patients with femoroacetabular impingement syndrome (FAIS). 2,3,10,29,35 Much of the success of this surgical approach has been attributed to its ability to reproducibly reduce pain, 23,34 restore functional capabilities, 8,11,25 improve quality of life, and maintain a low rate of complications. 16,47 Nevertheless, as the field of hip arthroscopic surgery advances, it remains somewhat unclear as to which patients have the propensity to benefit the most from this treatment option. Of note, female sex has been reported to be a risk factor for inferior outcomes after hip arthroscopic surgery for FAIS when compared with male sex. 28,41,49 Inconsistent results could be attributed to differences in laxity, pelvic tilt, and bony coverage in this group of patients in whom capsular management then becomes of utmost importance (a variable that has significantly evolved during the past decade of arthroscopic hip surgery).
Additionally, athletic status has been previously reported to be an important factor for improved patient-reported outcomes (PROs) and satisfaction. In this regard, the minimally invasive nature of hip arthroscopic surgery has allowed for a successful return to a variety of sports. § Notably, it has been suggested that athletes experience improved postoperative outcomes compared with nonathletes. 36 However, as the previous literature has mainly focused on the male population, the primary aim of the present study was to (1) compare the PROs and satisfaction of athletic versus nonathletic female patients undergoing hip arthroscopic surgery for FAIS and (2) determine the return-to-sports rate and time to return to sports in female athletes. We hypothesized that female athletes would experience better outcomes than their nonathlete counterparts and that female athletes would have a high rate of return to sports.
Methods
Patient Selection
This study was approved by an institutional review board. A retrospective review of prospectively collected data on consecutive female patients undergoing hip arthroscopic surgery for FAIS by a single fellowship-trained surgeon (S.J.N.) was performed. Inclusion criteria were all female patients undergoing hip arthroscopic surgery between January 2012 and January 2015 with history, physical examination, and radiographic findings consistent with FAIS who failed nonoperative management, with a minimum of 2-year follow-up. Exclusion criteria were retired athletes, patients unwilling to participate in the study, symptomatic FAIS in the contralateral hip requiring surgery, patients undergoing revision surgery, patients with ipsilateral knee and ankle injury/surgery within the postoperative period, length of follow-up less than 2 years, history of pediatric deformities (developmental dysplasia of the hip [lateral center-edge angle <20°, slipped capital femoral epiphysis, and Perthes disease]), and/or osteoarthritis or joint space narrowing (Tönnis grade >1).
Surgical Technique
Our preferred surgical techniques for labral repair or labral debridement, femoral osteochondroplasty, acetabular rim trimming, and capsular closure have been previously described. 13,17,46 All surgeries were performed with the patient in the supine position on a standard traction table under general anesthesia. Anterolateral and midanterior portals were created to establish visualization into the central compartment, and T-capsulotomy was performed for visualization of the peripheral compartment. Closure of the capsulotomy site via repair of the interportal and T-capsulotomy incisions was performed in all cases. 12,42 Hip traction was released immediately after work was concluded in the central compartment, and a dynamic examination was then performed to confirm the resolution of impingement. Labral refixation was performed when gross detachment of the labrum from the acetabular rim was observed; otherwise, partial debridement was used for patients with sufficient labral tissue and little or no detachment.
Postoperative Rehabilitation
Rehabilitation started on postoperative day 1 for all patients regardless of their athletic status and has been described previously in the literature. 42 Patients went through a 4-phase rehabilitation protocol that lasted a mean of 16 to 18 weeks. Phase 1 prioritized joint protection and soft tissue mobilization techniques. The surgical limb was initially restricted to 20-lb foot-flat weightbearing during this phase. Patients were weaned off crutches if they demonstrated ambulatory capabilities without significant pain or compensatory movements 3 weeks postoperatively. Patients advanced to phase 2 if they demonstrated full weightbearing capabilities. Phase 2 concentrated on normal gait maintenance, full range of motion restoration, improvement of neuromuscular control, and maintenance of pelvic and core stability. Patients progressed to phase 3 if gait was determined to be normal and pain free with adequate neuromuscular control. Phase 3 included single-legged squats and strengthening, soft tissue and joint mobilization, and cardiovascular fitness. Phase 4 emphasized returning to the preinjury level of sports participation. Patients were cleared to return to sports if they were able to participate in sports without pain, had full dynamic functional control, and passed all return-to-sports tests.
Functional Outcome Evaluation
All patients completed hip-specific outcome instruments, including the Hip Outcome Score–Activities of Daily Living (HOS-ADL), 30 Hip Outcome Score–Sport-Specific (HOS-SS), 31 and modified Harris Hip Score (mHHS) 3 as well as patient-determined pain and satisfaction as measured on a 1-to-10 visual analog scale (VAS) at a minimum of 2 years postoperatively. Patients also provided information on sports participation and level of competition on intake forms and, based on these data, were either classified as “athlete” or “nonathlete.” Athletes were defined as patients who participated in 1 of the included sports for ≥1 year, and nonathletes were defined as patients who had no history of sports participation. Patients classified as athletes completed a postoperative return-to-sports survey (Appendix). Questions from this survey included return-to-sports capability, length of time to return to sports, subjective current competition level relative to the preinjury competition level, and sports played. Differences in preoperative and postoperative outcome scores were compared with the minimal clinically important difference (MCID) for each PRO measure previously established in the literature. 32 The 2-year MCID was set at 9, 6, and 8 for the HOS-ADL, HOS-SS, and mHHS, respectively. Similarly, the 2-year patient acceptable symptomatic state (PASS) was set at 87, 75, and 74 for the HOS-ADL, HOS-SS, and mHHS, respectively. 6
Radiographic Measurements
Radiographs were taken preoperatively and at the time of the latest follow-up. All patients underwent anteroposterior 7 pelvis, false profile, and Dunn lateral views in the supine position. The lateral center-edge angle of Wiberg was assessed on anteroposterior pelvis radiographs, and the alpha angle was assessed on Dunn lateral radiographs. 7
Statistical Analysis
Statistical analysis was performed using SPSS statistical software (IBM). Patient demographic information was presented as means ± SDs. Continuous and categorical data were compared using parametric and nonparametric tests when appropriate. The normality of data distribution was confirmed using the Shapiro-Wilk test. Female athletes were further segregated into groups based on level of participation: recreational, high school, collegiate, and professional athletes. Study patients were segregated into groups based on age (≤25 vs >25 years) both for the athletes and nonathletes. A post hoc power analysis (alpha value of 0.05 and beta value of 0.8) confirmed that the study was adequately powered to detect differences between preoperative and postoperative outcome scores. A Tukey-Kramer honest significant difference test was used to compare outcome differences between participation levels for athletes and nonathletes. Statistical significance was set at P < .05.
RESULTS
A total of 330 female patients who underwent hip arthroscopic surgery for FAIS were included in the final analysis. Of these patients, 221 (67.0%; mean age, 29.1 ± 11.1 years) identified as athletes and 109 (33.0%; mean age, 39.3 ± 11.4 years) identified as nonathletes. There were significant improvements in the HOS-ADL (64.1 ± 19.9 vs 92.7 ± 9.9, respectively), HOS-SS (41.0 ± 22.3 vs 83.1 ± 19.2, respectively), mHHS (58.2 ± 13.1 vs 88.2 ± 12.1, respectively), and VAS for pain (7.1 ± 1.7 vs 1.3 ± 2.0, respectively) scores at a mean follow-up of 2.6 ± 1.0 years postoperatively compared with preoperatively (Table 1).
Preoperative and Postoperative Patient-Reported Outcome Scores a
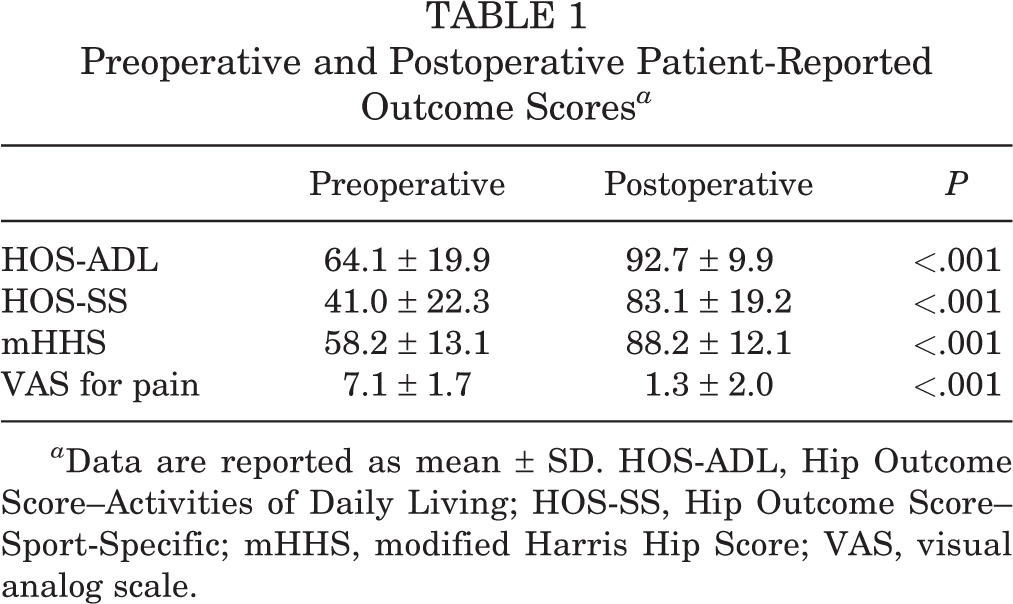
a Data are reported as mean ± SD. HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sport-Specific; mHHS, modified Harris Hip Score; VAS, visual analog scale.
Athlete Versus Nonathlete Analysis
To confirm that differences in postoperative outcomes were not solely attributed to potential confounding variables, a subset of 97 athletes and 97 nonathletes from the total cohort of 330 consecutive female patients were matched 1:1 by age (±1 year) and BMI (±5 kg/m2) (Table 2). Age and BMI have been identified as confounders of PROs in previous studies. 21 ,43 Athlete versus nonathlete analysis demonstrated that athletes achieved superior clinical outcome scores for all PRO measures at a mean of 2.6 ± 1.0 years postoperatively (P < .001 for all) (Figure 1). Overall, while patients in both groups reported excellent satisfaction, athletes reported higher mean VAS satisfaction scores versus nonathletes (87.8 ± 18.5 vs 66.4 ± 35.7, respectively; P < .001). Within the 2-year follow-up period, 1 patient converted to total hip arthroplasty and 2 patients underwent revision hip arthroscopic surgery in the nonathlete group. In the athlete group, 1 patient underwent revision hip arthroscopic surgery and no conversions to arthroplasty were documented. Although BMI could not completely be controlled for in this subset, a nonparametric correlation analysis indicated that BMI only had weak negative correlations with postoperative functional outcome scores, a weak positive correlation with the VAS for pain score, and no correlation with the VAS for satisfaction score at 2 years postoperatively (Table 3).
Demographics and Patient-Reported Outcome Scores for Case-Control Subset a

a Data are reported as mean ± SD. Bolded P values indicate statistically significant between-group differences (P < .05). BMI, body mass index; HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sport-Specific; mHHS, modified Harris Hip Score; VAS, visual analog scale.
b Age was matched ±1 year, and BMI was matched ±5 kg/m2.

Outcome scores between groups at the time of the latest follow-up. The error bars indicate the standard error of the mean. Athletes showed significantly greater scores in all hip outcome instruments at 2 years postoperatively. **Statistically significant difference (P < .001).
Correlation Analysis of BMI and Patient-Reported Outcome Scores for Case-Control Subset a

a Bolded P values indicate a statistically significant correlation between BMI and patient-reported outcome scores (P < .05). BMI, body mass index; HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sport-Specific; mHHS, modified Harris Hip Score; VAS, visual analog scale.
MCID and PASS rates were calculated for the HOS-ADL, HOS-SS, and mHHS for both athletes and nonathletes (Table 4). Overall, athletic patients were associated with significantly higher rates of achieving the MCID for the HOS-ADL (P < .001), HOS-SS (P = .0001), and mHHS (P = .015) when compared with nonathletic patients. The MCID for athletes was 99% for the HOS-ADL and HOS-SS and 100% for the mHHS. Furthermore, being athletic was associated with significantly higher rates of achieving the PASS for the HOS-ADL (99%), HOS-SS (97%), and mHHS (100%) (P < .001 for all).
MCID and PASS for Athletes and Nonathletes a
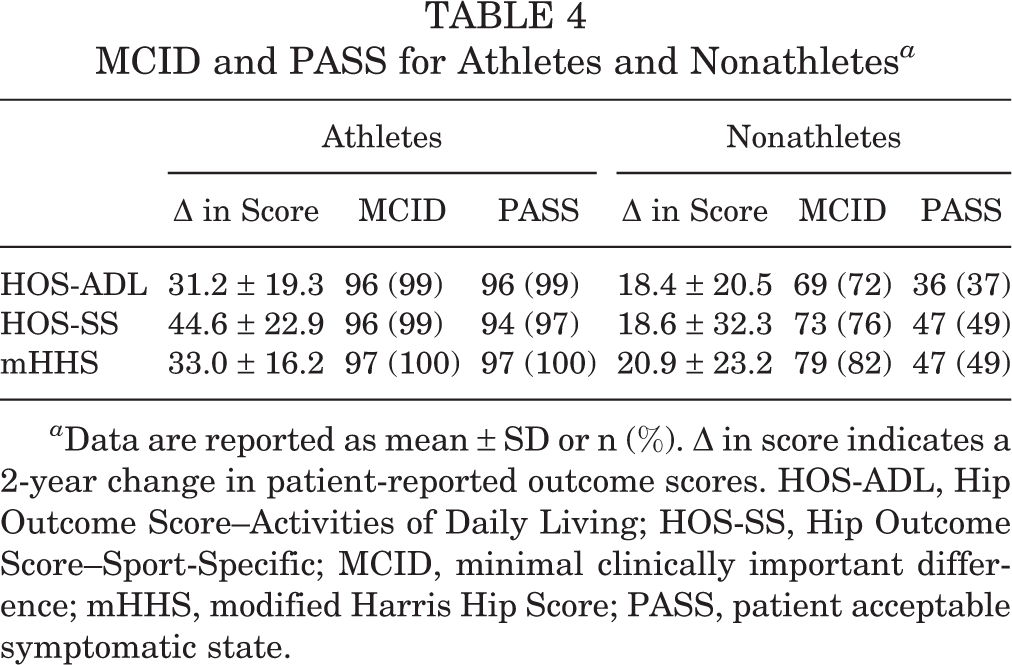
a Data are reported as mean ± SD or n (%). Δ in score indicates a 2-year change in patient-reported outcome scores. HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sport-Specific; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; PASS, patient acceptable symptomatic state.
Radiographic Outcomes
A summary of all preoperative and postoperative radiographic outcomes is provided in Table 5. Notably, both the preoperative and the postoperative alpha angles were greater in the nonathlete group compared with the athlete group (P < .05 for both).
Preoperative and Postoperative Radiographic Variables for Athletes and Nonathletes a
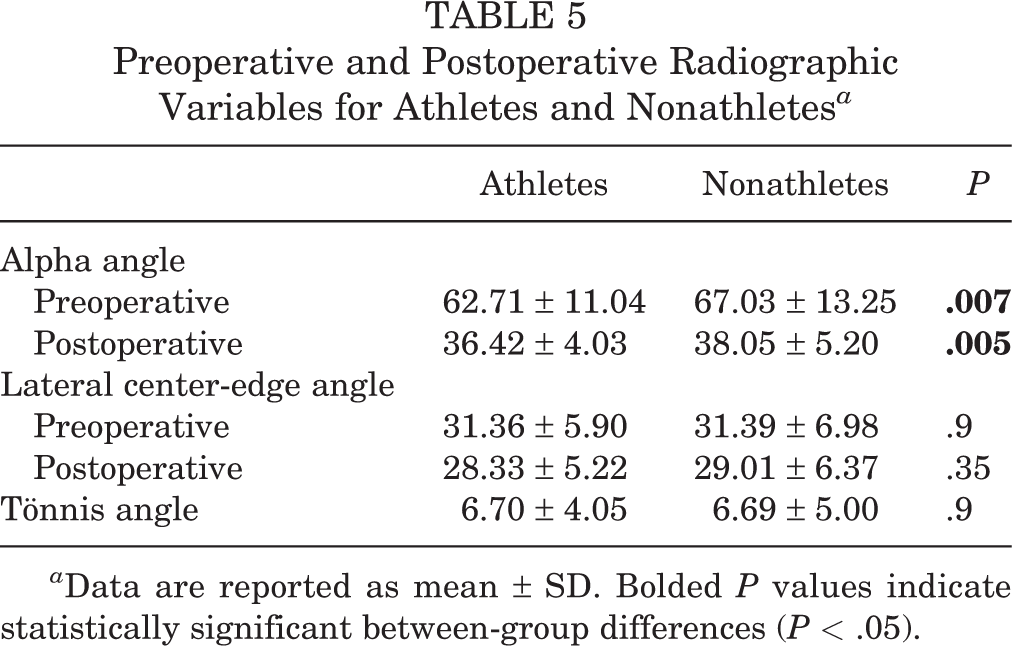
a Data are reported as mean ± SD. Bolded P values indicate statistically significant between-group differences (P < .05).
Intraoperative Findings and Procedures
A summary of all intraoperative procedures and findings is provided in Table 6. Labral tears were found intraoperatively in 100% of athletes versus 90% of nonathletes (P = .93), and labral repair was performed in all cases of labral tears for both athletes and nonathletes. Likewise, the percentages of cam, pincer, and combined FAIS morphology were relatively the same in both groups. With regard to procedures, there were no statistically significant associations between the frequency of acetabular rim trimming, femoral osteochondroplasty, and capsular plication and athlete status.
Intraoperative Findings and Procedures for Athletes and Nonathletes a
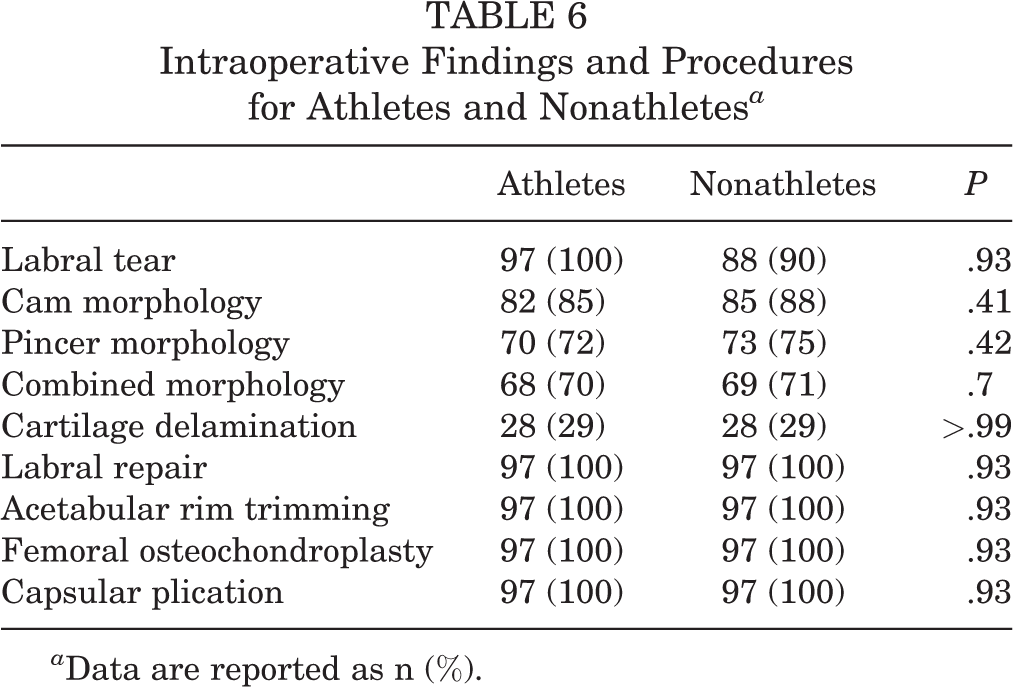
a Data are reported as n (%).
Athlete-Only Analysis
Return-to-Sports Time
Athletes recorded their level of sports participation on intake forms and were self-designated as recreational, high school, collegiate, or professional athletes. Of 194 single-sport athletes, 170 patients (87.6%) identified as recreational athletes, 17 (7.7%) as high school athletes, 6 (2.7%) as collegiate athletes, and 1 (0.5%) as a professional athlete (Table 7). Sports included yoga, dance, golf, CrossFit, Pilates, swimming, running, cycling, and soccer. Twenty-seven (12.2%) patients participated in multiple sports.
Return-to-Sports Rate and Time a

a Data are reported as n (%) or mean ± SD.
After controlling for athletes who played multiple sports, 189 of 194 single-sport athletes (97.4%) returned to sports at a mean of 6.0 ± 3.9 months after hip arthroscopic surgery. Overall, 94 patients returned to sports at a subjectively higher competition level (49.7%), 83 patients returned to the same level before the onset of symptoms (42.8%), and 12 patients returned to a lower level of competition level (6.2%). The mean return-to-sports time was lowest in swimmers (3.9 ± 3.1 months) and highest in CrossFit athletes (10.8 ± 5.9 months).
Clinical Outcomes and PROs
Analysis of variance with the Bonferroni correction was used to compare postoperative outcomes among the various sports groups. No statistically significant differences were found between sports groups for the postoperative HOS-ADL, mHHS, VAS for pain, and VAS for satisfaction scores. Notably, patients participating in Pilates had a lower mean postoperative HOS-SS score (68.1 ± 26.3) when compared with those participating in dance (85.5 ± 18.4; P = .044) and cycling (86.9 ± 15.8; P = .038).
Multivariate Regression Analysis
A multivariate linear regression analysis was performed in an effort to determine the association between age, BMI, and being an athlete with 2-year PROs (Table 8). This analysis demonstrated a mild inverse relationship between age, BMI, and 2-year PROs that was not statistically significant, with the exception of BMI and 2-year HOS-ADL scores. Furthermore, being an athlete had a strong positive relationship with all 2-year hip-specific outcomes and patient satisfaction as well as a strong negative relationship with self-reported pain.
Multivariate Linear Regression Model for 2-Year Patient-Reported Outcome Scores and Age, BMI, and Being an Athlete a
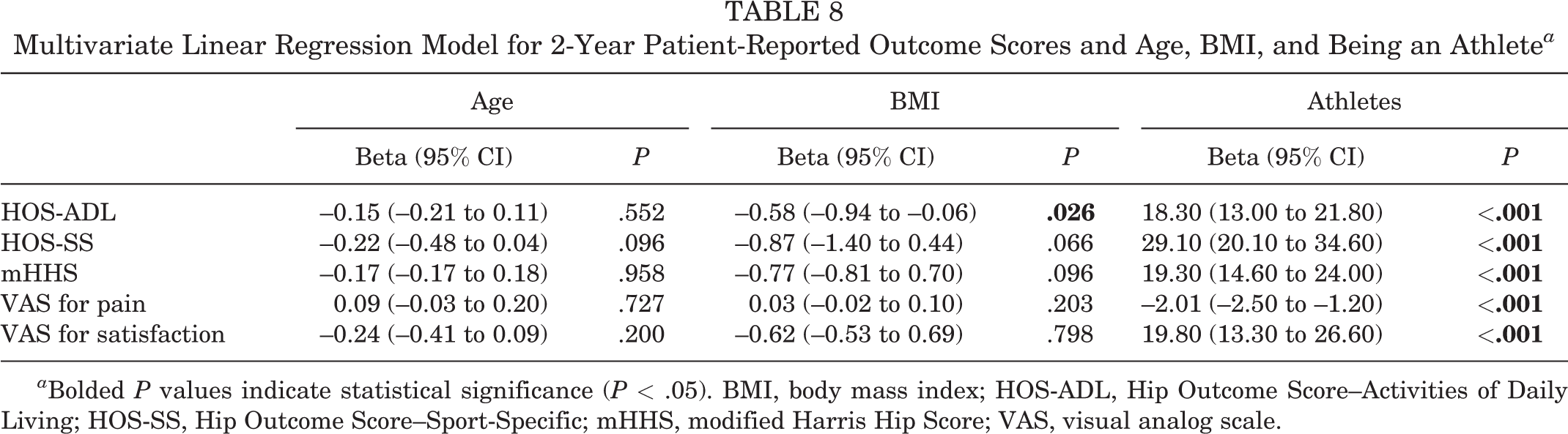
a Bolded P values indicate statistical significance (P < .05). BMI, body mass index; HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sport-Specific; mHHS, modified Harris Hip Score; VAS, visual analog scale.
Discussion
The main findings of the current study were that (1) all patients, regardless of age or athlete status, had significant improvements in all outcomes after hip arthroscopic surgery for FAIS; (2) athletes had superior postoperative outcomes when compared with nonathletes; (3) athletes had a 97.4% rate of return to sports at a mean of 6.0 months after hip arthroscopic surgery, with 94% reporting returning to sports at the same or higher level of competition; and (4) athlete status in female patients undergoing hip arthroscopic surgery for FAIS was the most influential independent predictor of postoperative PROs of all the variables examined in the current study.
The female FAIS population is unique in that studies examining sex differences in hip function after hip arthroscopic surgery have demonstrated inferior outcomes in female patients when compared with their male counterparts. Joseph and colleagues 22 reported on a cohort of 229 patients (68.4% women) with the purpose of determining postoperative functional differences between sexes. Using the International Hip Outcome Tool (iHOT-33) and HOS-ADL, they demonstrated that women had inferior preoperative HOS-ADL and iHOT-33 scores. At 6, 12, and 24 months postoperatively, although women consistently had lower mean HOS-ADL and iHOT-33 scores, there were no significant differences between the groups. 22 Another study of postoperative hip function in 60 adolescents undergoing hip arthroscopic surgery for FAIS reported that female patients had significantly inferior hip function compared with male patients at 2 and 5 years postoperatively. 40 Female sex is also a known predictor of longer recovery times, 11,25 and sex-specific differences in the bone morphology of patients with FAIS have been identified preoperatively, 19,37,50 suggesting a sex influence on postoperative outcomes. In the present study, it was also shown that female athletes had smaller preoperative and postoperative alpha angles measured on Dunn lateral views when compared with female nonathletes, suggesting that there may be some association between athletic activity and the severity of the abnormality. Despite these disparities, the current study indicates that female patients possess a significant postoperative recovery potential, especially if they are athletes. Importantly, the aforementioned studies demonstrating that female patients experience inferior outcomes were published when capsular management (repair and plication) was not performed in the majority of cases. The female patients in this study are unique given that all underwent capsular repair or plication, which may have contributed to the observed improvement in outcomes.
There is a paucity of literature on female athletes’ postoperative outcomes compared with their nonathletic female counterparts. Murata and colleagues 36 compared a cohort of athletes (47 patients) with a cohort of nonathletes (27 patients), which included both women and men in both groups, and reported that the mean Non-Arthritic Hip Score was superior in the athlete group at all postoperative time points and that the mHHS was superior in the athlete group only at 2 years postoperatively. These results are in agreement with those of the current study suggesting that female athletes have superior postoperative outcome scores at a minimum of 2 years postoperatively when compared with their nonathlete counterparts. Murata et al 36 also reported a 95.7% return-to-sports rate, which is comparable with our return-to-sports rate of 97.4%.
The primary outcome of return to sports is frequently used for assessing the success of surgical interventions in populations of athletes. Reports on the ability of athletes with FAIS to return to sports after hip arthroscopic surgery have demonstrated the effectiveness of this procedure in active patient populations. Weber and colleagues 48 compared 49 recreational and 17 high-level amateur athletes and concluded that both groups demonstrated significant improvements in PRO measures, with no differences between the groups, and that both returned to sports at high rates (94% and 88%, respectively). These findings have also been reported in professional and collegiate athletes undergoing hip arthroscopic surgery for FAIS. 4 Despite numerous reports of hip arthroscopic surgery serving as an effective surgical intervention in athletic populations with FAIS, 1,5,38,40 no study to date has conducted a return-to-sports analysis focusing solely on the female athletic population. Furthermore, the types of sports engaged in by the patient population in this study are different than in previous studies, as these examined generally male sports (ie, football, hockey, soccer, etc). This study focused mainly on patients who participate in more recreational sports (eg, running, cycling, swimming, Pilates, CrossFit).
A recent systematic review of the literature conducted by Casartelli and colleagues 5 demonstrated that the average return-to-sports rate after hip arthroscopic surgery for FAIS was 87% and that the return-to-sports rate increased as the competition level increased. The overall return-to-sports rate in the current study, 97.4%, is comparable with but greater than that shown in the most recent systematic review of the literature. One possible explanation for the high return-to-sports rate is the nature of our entirely female patient cohort. Furthermore, it is possible that the routine use of capsular plication in our cohort may account for the superior return-to-sports rate and high postoperative outcome scores. Frank and colleagues 12 demonstrated in a comparative matched-pair analysis that patients with complete capsular closure had greater sports-specific activity scores than those with partial repair, suggesting that complete capsular closure may facilitate increased return to sports and postoperative success after hip arthroscopic surgery. The findings in this study are unique in that they demonstrate that female athletes of all levels of sports competition return to sports at high rates and have increased postoperative success in the midterm (approximately 2 years after surgery) when compared with their female nonathlete counterparts. Another possible explanation for the increased postoperative success in the athlete group is the known association between exercise and benefits in mental health, 18,20,45 as mental disorders have been reported to negatively influence outcomes both preoperatively and postoperatively after hip arthroscopic surgery. 24 Future studies are warranted to investigate whether these differences persist at long-term follow-up and whether there is an association between athlete status and psychological influence on outcomes.
This study is not without limitations. Although prospective data collection was performed, the information regarding ability and time to return to sports was collected retrospectively and was subject to recall bias. Additionally, the return-to-sports questionnaire that we used in the study was not validated and may limit the validity of the presented results. However, we believe that the survey provides an accurate and comprehensive representation of the ability to return to sports. Despite attempts to match female athletes and nonathletes on BMI and age, we were not able to match on BMI while maintaining statistical power. It should also be noted that we did not match by other variables such as workers’ compensation status and the Beighton score, which may have had confounding effects. Finally, our cohort represents the outcomes by a single, large-volume, hip-specialized surgeon, which might not make the abovementioned outcomes generalizable.
Conclusion
Female patients who are athletes can expect a high likelihood of pain relief, functional improvements, and return to competition at a mean of 6.0 months after hip arthroscopic surgery for FAIS. Among female patients undergoing hip arthroscopic surgery for FAIS, patients considered athletes achieved superior clinical outcomes compared with patients considered nonathletes.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: C.A.B.-J. has received educational support from Medwest and has stock or stock options in Cresco Labs. S.J.N. has received research support from AlloSource, Arthrex, Athletico, DJ Orthopedics, Linvatec, MioMed, Smith & Nephew, and Stryker; has received educational support from Elite Orthopaedics; is a paid consultant for Ossur, Pivot Medical, and Stryker; and receives royalties from Springer and Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Rush University Medical Center Institutional Review Board (#12022108-IRB01-CR05).
Notes
APPENDIX
Return-to-Sports Survey for Female Athletes

| Question | Possible Responses |
|---|---|
| 1. Have you had surgery since your first hip surgery? 1A. If yes, was it on the same hip? |
Yes/no Yes/no |
| 2. Which type of sports/recreational activities did you partake in before surgery? | Contact sports Football Lacrosse Hockey Overhead sports Volleyball Tennis Baseball Endurance sports Running Soccer Fitness-based Swimming CrossFit Yoga Dance-based Dance Ice skating Gymnastics |
| 3. Did your hip injury cause you to alter your participation in these activities? | I had to completely stop my participation I had to decrease my participation I did not have to change my participation |
| 4. If you had to stop or decrease your participation, how long before surgery was it? | Open answer |
| 5. Since surgery, which sports or activities that you participated in before surgery have you resumed? | Open answer |
| 6. For the sports or activities that you have resumed, please rate your current ability/competition level relative to where it was before surgery. | Better (competing at a higher level now) Same (before symptoms) Lower (competing less or not at all) |