
Abstract
Background:
Changes in limb length and coronal pelvic tilt, which occur along with changes in limb alignment, may affect the functional lateral acetabular coverage of the hip joint under weightbearing conditions.
Purpose:
To analyze the functional lateral acetabular coverage after unilateral closed-wedge and open-wedge high tibial osteotomies with a large wedge correction of ≥10 mm.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective analysis was conducted for 107 unilateral closed-wedge high tibial osteotomies (CWHTOs) and 100 unilateral open-wedge high tibial osteotomies (OWHTOs) with a wedge correction of ≥10 mm and without correction loss during a 2-year follow-up. Limb length and coronal pelvic tilt were measured. Functional lateral acetabular coverage was evaluated using the lateral center-edge angle (LCEA), acetabular index, sharp angle, and femoral head extrusion index (FHEI) with reference to the ground horizontal line. Appropriate ranges of the LCEA (22° to 40°), acetabular index (−8° to 14°), sharp angle (34° to 43°), and FHEI (11% to 27%) were investigated.
Results:
Limb length significantly decreased after CWHTO (−7.2 mm) and increased after OWHTO (11.5 mm). The pelvis of the operative limb tilted downward after CWHTO (−1.0°) and upward after OWHTO (2.1°). The mean parameters for functional lateral acetabular coverage significantly changed toward more coverage after CWHTO and less coverage after OWHTO (change in LCEA, acetabular index, sharp angle, and FHEI = 1.2°, −1.1°, −1.0°, and −0.7%, respectively, in CWHTO and −1.3°, 1.8°, 1.6°, and 2.7%, respectively, in OWHTO). When evaluating the appropriateness of each parameter for coverage, cases of conversions from undercoverage to appropriate coverage (1.9% to 4.7%) and appropriate to overcoverage (0.9% to 5.6%) after CWHTO and from overcoverage to appropriate coverage (0% to 8%) and appropriate to undercoverage (2% to 7%) after OWHTO were observed.
Conclusion:
The functional lateral acetabular coverage increased after CWHTO and decreased after OWHTO. Surgeons may want to consider the acetabular coverage of the ipsilateral hip joint when performing a unilateral high tibial osteotomy with a large correction.
Keywords
High tibial osteotomy (HTO) is a surgical procedure used to treat medial compartmental osteoarthritis in the knee joint by adjusting limb alignment. Because of the interconnected functionality of the hip and knee joints, lower extremity interventions involving knee procedures inevitably affect the hip joint.13,15 Understanding the effect of HTO on the hip joint is important for surgeons to improve patient satisfaction through establishing appropriate indications and ensuring enhanced limb alignment correction.
Lateral acetabular under- or overcoverage may be associated with labral tears and progression of hip joint osteoarthritis.7,22 Changes in limb length and coronal pelvic tilt, which occur along with changes in limb alignment, may affect the functional lateral acetabular coverage of the hip joint under weightbearing conditions.3,13,15 Although the biomechanical changes of the hip joint after HTO have been addressed,10,13,15 the changes of the functional lateral acetabular coverage remain unexplored.
The present study analyzed functional lateral acetabular coverage after unilateral closed-wedge and open-wedge HTOs with a large wedge correction of ≥10 mm. We hypothesized that changes in the limb length and coronal pelvic tilt caused by HTO would affect the lateral acetabular coverage and that these changes would present in different ways depending on the type of HTO performed.
Methods
Patients
We retrospectively searched our hospital's database for patients who underwent unilateral closed-wedge high tibial osteotomy (CWHTO) or open-wedge high tibial osteotomy (OWHTO) between 2012 and 2020. During this period, 261 CWHTOs and 333 OWHTOs were performed. The inclusion criteria were as follows: (1) a minimum follow-up period of 2 years after unilateral HTO (the period when sufficient weightbearing was possible because bone union occurred at osteotomy sites 6 ); (2) availability of pre- and postoperative radiographs; and (3) a large wedge correction of ≥10 mm, which has been reported to sufficiently affect limb length and coronal pelvic tilt in previous literature.3,17 The exclusion criteria were as follows: (1) bilateral HTO in both knees; (2) loss of correction at the osteotomy site, which was defined as absolute change of ≥3° in the medial proximal tibial angle (MPTA) during follow-up 20 ; (3) history of trauma, infection, or previous surgery on the affected limb; (4) instability of the affected knee due to any ligament problems; and (5) any clinical symptoms or degenerative arthritis of the ipsilateral hip joint.
Following these criteria, 107 CWHTOs and 100 OWHTOs were included in the study. The surgical indications for CWHTO and OWHTO were similar. These included (1) symptomatic medial compartment osteoarthritis (Kellgren-Lawrence grades 2-3); (2) varus deformity of 5° to 15°; (3) flexion contracture of <15° and flexion angle of >90°; and (4) absence of symptomatic lateral compartmental and patellofemoral arthritis, active infection, inflammatory arthritis, or lateral tibial subluxation of >1 cm.
There were no significant differences in patient demographics, wedge correction size, or preoperative limb alignment between the CWHTO and OWHTO groups (Tables 1 and 2). Informed consent was obtained from all patients before the review. This study was approved by the institutional review board of our affiliated hospital.
Patient Demographics a
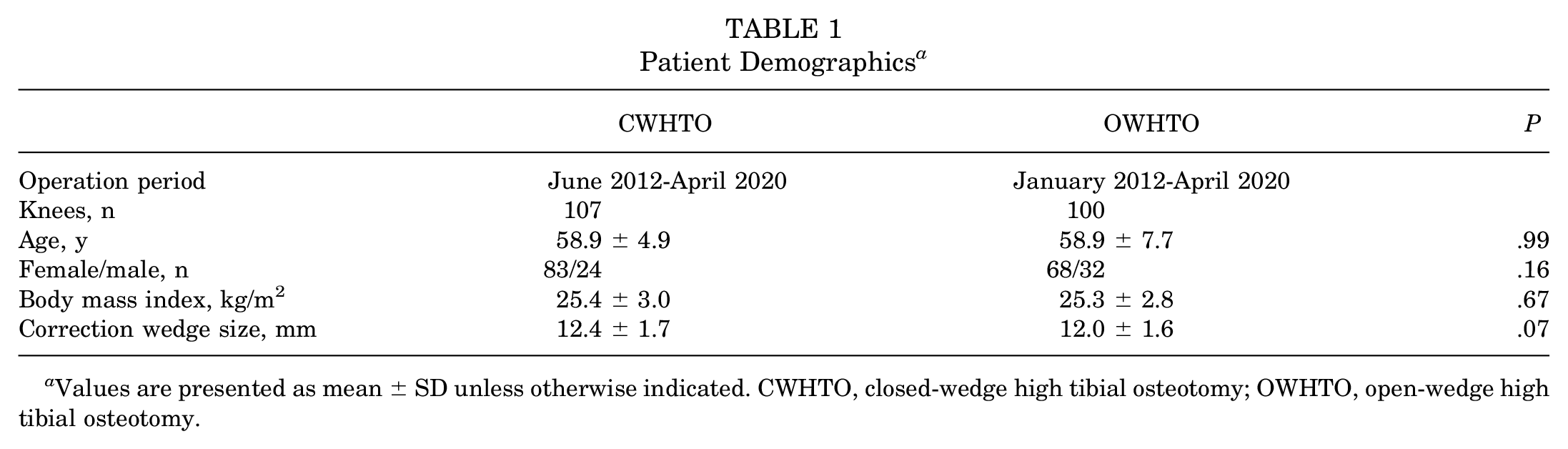
Values are presented as mean ± SD unless otherwise indicated. CWHTO, closed-wedge high tibial osteotomy; OWHTO, open-wedge high tibial osteotomy.
Radiographic Results a

Values are presented as mean ± SD. CWHTO, closed-wedge high tibial osteotomy; OWHTO, open-wedge high tibial osteotomy; Postop, postoperative; Preop, preoperative.
Surgical Techniques
Two senior surgeons (S.J.S. and K.H.Y.) performed each CWHTO or OWHTO procedure according to their preferences; one surgeon performed only CWHTOs, while the other performed only OWHTOs. Both surgeons had similar experience and had performed >100 procedures for each type before the study period. Anteroposterior (AP) long-leg weightbearing radiographs were used for preoperative planning with the Dugdale method. 18 The postoperative hip-knee-ankle angle (HKA) was targeted as valgus 2° to 3° in both types of HTO; this target angle has been reported to improve osteotomy longevity and patient satisfaction.9,11 Arthroscopic procedures including cartilage debridement, microfracture, partial meniscectomy, and meniscal repair were performed during the operation but before the osteotomy procedure.
In the CWHTO, partial resection of the fibular head was performed to avoid the fibular tethering effect on wedge closing. One pin was inserted in the proximal plane of the tibial osteotomy 1.5 cm below the joint line, and the other pin was placed in the distal plane under fluoroscopic guidance to determine the alignment correction. The wedge size was based on the preoperative radiographic planning. Finally, the wedge was removed and the osteotomy site was carefully closed. A miniplate staple (U&I) was used for fixation. In the OWHTO, 2 guide pins were inserted obliquely toward the tibiofibular joint. The main osteotomy was performed according to the guide pins using an oscillating saw and chisels. A biplanar cut for a separate ascending or descending osteotomy was performed posterior to the tibial tuberosity. An opener was used to open the osteotomy site until the planned open-wedge size was reached. A medial locking anatomic plate (Nowmedipia) was used for fixation. Minimal alteration of the posterior tibial slope (PTS) was achieved by ensuring equivalent anterior and posterior heights of the wedge in CWHTO and an appropriate lateral hinge position with proper posterior cortical osteotomy in OWHTO.12,16,19,21
A similar rehabilitation protocol was used for all patients: isometric exercises were recommended on the operative day, straight-leg raising exercises were initiated 3 days postoperatively, tolerable weightbearing with crutches began 3 to 4 days postoperatively, and full weightbearing without crutches was started at 6 to 12 weeks after surgery, based on the patient's condition.
Clinical Evaluation
Any clinical symptoms of the ipsilateral hip joint of the operated knee, including inguinal pain, snapping or popping, and loss of range of motion, were investigated preoperatively and at 3 months, 6 months, 1 year, and 2 years postoperatively.
Radiographic Evaluation
Radiographic parameters were measured preoperatively and at 2 years postoperatively. Pre- and postoperative AP leg and lateral radiographs were obtained under weightbearing conditions. HKA, MPTA, limb length, and coronal pelvic tilt were measured using long-leg radiographs,4,21 and PTS was measured using lateral knee radiographs. 21 The limb length was defined as the distance between the hip and ankle centers (Figure 1). 3 The coronal pelvic tilt was defined as the angle between the ground horizontal line and pelvic horizontal line, represented by the interteardrop line (Figure 1). 13 If the pelvis on the operative side tilted upward, the coronal pelvic tilt was presented as a positive value; however, if it tilted downward, the tilt was presented as a negative value. The PTS was measured using the angle formed by a line perpendicular to the reference line and the medial tibial plateau; the reference line was defined as a line connecting the center of the medullary canal 10 cm and 20 cm distal to the tibial plateau. 21

Pre- and postoperative limb length and coronal pelvic tilt after open- and closed-wedge high tibial osteotomies. Limb length was defined as the distance between the hip and ankle centers, and coronal pelvic tilt was defined as the angle between the ground horizontal line (dotted line) and the pelvic horizontal line represented by the interteardrop line (solid line connecting the teardrops in the pelvis); HKA, hip-knee-ankle angle; MPTA, medial proximal tibial angle; PTS, posterior tibial slope.
Functional lateral acetabular coverage and degenerative changes in the hip joint were evaluated using long-leg radiographs (Figure 2). Radiographic parameters for functional lateral acetabular coverage, including lateral center-edge angle (LCEA), acetabular index, sharp angle, and femoral head extrusion index (FHEI), were measured according to the ground horizontal line rather than the pelvic horizontal line. The ground horizontal line represented the actual and functional acetabular lateral coverage under weightbearing conditions and may be more clinically relevant to hip joint deterioration. 14 The LCEA was measured as the angle between the line perpendicular to the ground horizontal line and the line connecting the hip center and lateral edge of the sclerotic sourcil on the acetabulum.8,14 The acetabular index was defined as the angle between the ground horizontal line and the tangential line extending from the medial edge to the lateral upturn edge of the acetabular sourcil.14,22 The sharp angle was defined as the angle between the ground horizontal line and tangential line extending from the inferior aspect of the pelvic teardrop to the lateral upturn edge of the acetabular sourcil.14,22 The FHEI was defined as the percentage of the uncovered femoral head in comparison with the total horizontal femoral head diameter.14,22 Appropriate ranges of the LCEA, acetabular index, sharp angle, and FHEI were defined as the LCEA of 22° to 40°, acetabular index of −8° to 14°, sharp angle of 34° to 43°, and FHEI of 11% to 27%, based on previous literature. 22 Undercoverage was defined by an LCEA of <22°, acetabular index of >14°, sharp angle of >43°, or FHEI of <11%. Conversely, overcoverage was defined by an LCEA of >40°, acetabular index of <−8°, sharp angle of <34°, or FHEI of >27%. Any degenerative change of the hip joint identified as ≥1 of the Kellgren-Lawrence progression was investigated.

Radiographic parameters for functional lateral acetabular coverage. The radiographic parameters were measured with reference to the ground horizontal line.
The quality of the radiographic evaluations was improved following the protocol of standardizing the knee position and creating an identical distance between the x-ray beam and the cassette. The images were digitally transferred to a picture archiving and communication system (PACS; Infinitt) and assessed using PACS software. The minimal differences detected by the software were 0.1° and 0.1 mm. Two independent investigators (S.J.L. and C.H.P.) measured all radiographic parameters to reduce observation bias. The interobserver reliabilities of the radiographic variables were assessed using intraclass correlation coefficients (ICCs). In this study, the ICCs were 0.91, 0.88, 0.83, 0.92, 0.84, 0.84, 0.83, 0.82, and 0.85 for the HKA, MPTA, PTS, limb length, pelvic tilt, LCEA, acetabular index, sharp angle, and FHEI, respectively. Therefore, the mean values of the ICCs developed by the 2 investigators were used in the analysis.
Statistical Analysis
The HKA, MPTA, and PTS between the CWHTO and OWHTO groups were compared using an independent t test. The pre- and postoperative limb lengths, coronal pelvic tilt, and relevant parameters for functional lateral acetabular coverage were compared using a paired t test for CWHTO and OWHTO. The pre- and postoperative proportions of appropriate parameters for functional lateral acetabular coverage were compared using the McNemar test in both CWHTO and OWHTO. The proportions of hip joint degeneration between the CWHTO and OWHTO groups were compared using the chi-square test or Fisher exact test. Statistical analyses were performed using SPSS Version 25.0 (IBM Corp.), and a P value of <.05 was considered statistically significant.
Post hoc power analysis with significance levels set to an alpha of .05 was performed to determine whether the sample had sufficient power to detect significant differences. A power level of >80% was considered sufficient, and all variables that were significantly different met this criterion. Thus, we conclude that our study was adequately powered.
Results
No clinical symptoms were detected around the hip joint both preoperatively and during 2 years of postoperative follow-up.
No significant differences were observed in the pre- and postoperative HKA, MPTA, PTS, and value changes between the CWHTO and OWHTO groups (Table 2). The limb length significantly decreased after CWHTO and increased after OWHTO (Tables 3 and 4). The pelvis of the operative limb tilted downward after CWHTO and upward after OWHTO (Tables 3 and 4).
Relevant Radiographic Results for Functional Lateral Acetabular Coverage a

Values are presented as mean ± SD. CWHTO, closed-wedge high tibial osteotomy; OWHTO, open-wedge high tibial osteotomy; Postop, postoperative; Preop, preoperative.
Comparison of the Changes in Relevant Results in Functional Lateral Acetabular Coverage a

Values are presented as mean ± SD. CWHTO, closed-wedge high tibial osteotomy; OWHTO, open-wedge high tibial osteotomy.
The mean parameters for functional lateral acetabular coverage significantly changed toward more coverage after CWHTO and less coverage after OWHTO (Tables 3 and 4, Figure 3), and the changes in these parameters differed between CWHTO and OWHTO (Table 4, Figure 3). The proportion of appropriate lateral acetabular coverage did not significantly change after CWHTO or OWHTO (Figure 4). However, upon evaluating the appropriateness of each parameter for coverage, cases of conversions were observed from undercoverage to appropriate coverage (1.9% to 4.7%) and appropriate to overcoverage (0.9% to 5.6%) after CWHTO and from overcoverage to appropriate coverage (0% to 8%) and appropriate to undercoverage (2% to 7%) after OWHTO (Figure 5).
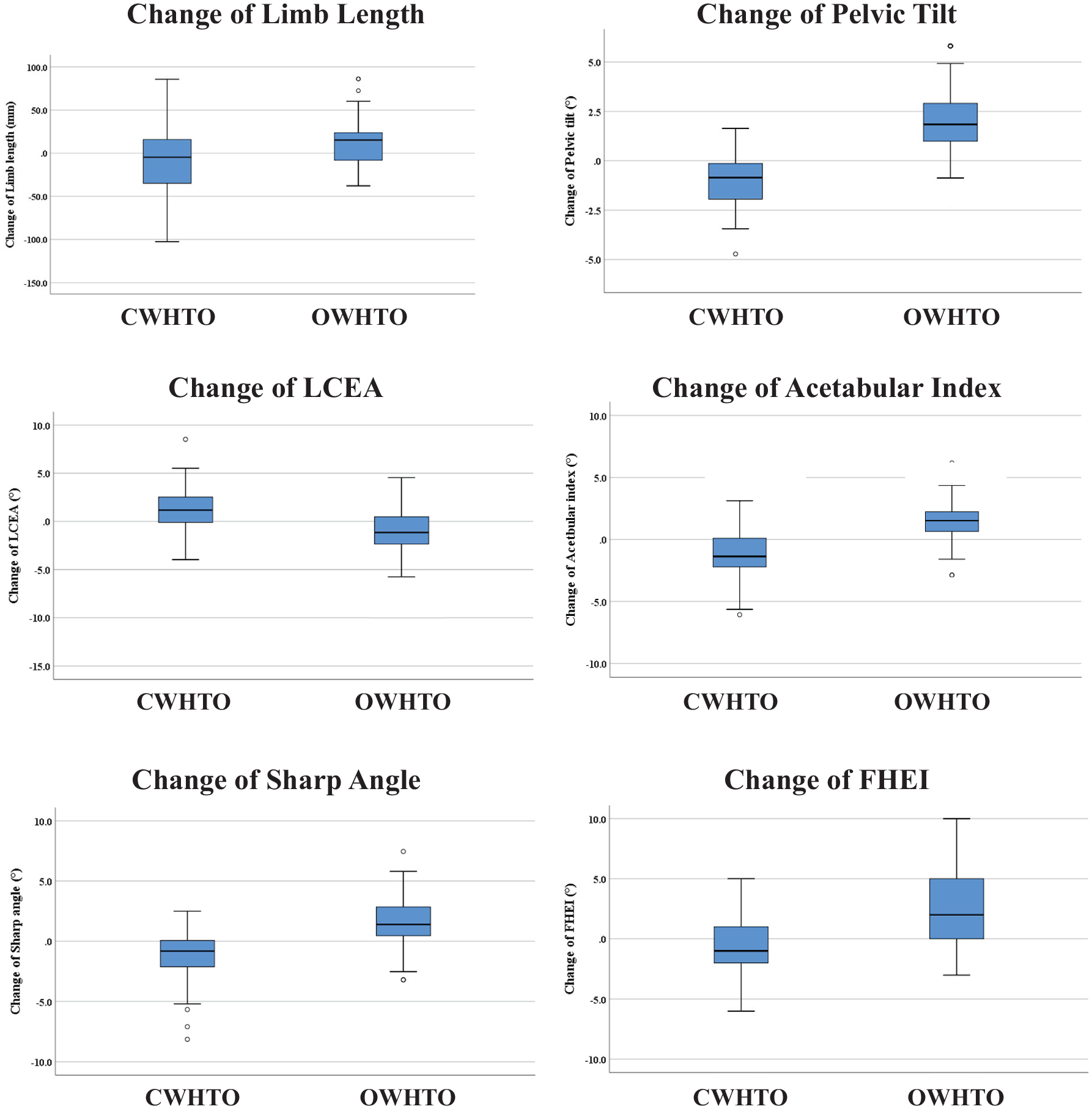
Box plot graphs for the changes in relevant results in functional lateral acetabular coverage. CWHTO, closed-wedge high tibial osteotomy; FHEI, femoral head extrusion index; LCEA, lateral center-edge angle; OWHTO, open-wedge high tibial osteotomy.

The proportion of appropriate parameters of functional lateral acetabular coverage. CWHTO, closed-wedge high tibial osteotomy; OWHTO, open-wedge high tibial osteotomy; Postop, postoperative; Preop, preoperative.

The number of cases of change in appropriateness of parameters of functional lateral acetabular coverage. CWHTO, closed-wedge high tibial osteotomy; OWHTO, open-wedge high tibial osteotomy.
There were 2 cases (1.8%) of radiographic hip joint degeneration after CWHTO (the Kellgren-Lawrence grade increased from 0 to 1 in both cases) and no cases of degeneration after OWHTO during follow-up (P = .382).
Discussion
The most important finding of the present study was that the functional lateral acetabular coverage changed toward more coverage after CWHTO and less coverage after OWHTO. When evaluating the appropriateness of each parameter for coverage, cases of conversion from undercoverage to appropriate coverage and appropriate to overcoverage after CWHTO and from overcoverage to appropriate coverage and appropriate to undercoverage after OWHTO were observed.
Several studies have analyzed the effects of HTO on the hip joint. Moghtadaei et al 13 reported that OWHTO could cause downward movement of the greater trochanter due to femoral adduction, consequent shortening of the abductor moment arm, and finally increased stress on the hip joint. Kim et al 10 also showed that hip adduction after OWHTO was associated with unfavorable functional results, as represented by the timed up and go test. Patel et al 15 reported that the increased correction following OWHTO led to an increased change in the coronal alignment of the hip, altering the weightbearing portion of the femoral head and disrupting the function of the adductor. Thus, they recommended hip joint assessment during preoperative planning before performing OWHTO.
Although there is some debate, 1 the extent of acetabular coverage is associated with degenerative changes in the hip joint. Undercoverage may cause increased joint contact pressure and subsequent degeneration of the articular cartilage owing to static overload; overcoverage may result in early pathological contact between the overcovered acetabulum and femoral neck junction, leading to chondral damage due to dynamic conflict at the acetabular rim. 22 Previous clinical studies reported that acetabular under- and overcoverage were associated with degenerative hip osteoarthritis.1,7
Unilateral HTO with a large correction can alter leg length and pelvic obliquity. In general, limb length decreases, and the pelvis of the operative side tilts downward after CWHTO, whereas the opposite is observed after OWHTO.3,13 Theoretically, these changes can affect functional lateral acetabular coverage of the hip joint based on the horizontal ground plane; functional coverage would increase after CWHTO and decrease after OWHTO. The present study is valuable in that it is the first to clinically analyze and demonstrate these changes.
Ideally, knee surgeons should consider the limb a functional unit and weigh all the effects of HTO on the adjacent joints. An appropriate type of HTO should be selected considering the effect of the procedure on the functional lateral acetabular coverage of the ipsilateral hip joint when performing unilateral HTO with a large correction. CWHTO can be considered for patients with acetabular undercoverage and OWHTO can be considered for those with acetabular overcoverage. Additionally, a shoe lift may be used to correct limb length discrepancy, which is the primary reason for changes in functional coverage (and for spinal disorders such as functional scoliosis) in HTOs with a large correction. 2
Limitations
The present study had several limitations. First, it was a retrospective study with a short follow-up period. A sophisticated clinical evaluation of the hip joint using patient-reported clinical scoring could not be performed retrospectively because the patients were followed up at the knee surgeons’ outpatient clinics after HTO. Additionally, despite changes in the acetabular coverage after HTO, no clinical symptoms were observed around the hip joint, and only a small proportion (1.8% of CWHTOs) of cases of radiographic degenerative changes in the hip joint were detected. This could be attributed to the follow-up period of 2 years, which was too short to allow for the development of clinical symptoms and degenerative changes. Second, the sample size was relatively small. This is because only HTOs with large corrections performed at a single center were included. Third, the use of long-leg AP radiographs to evaluate lateral acetabular coverage may have underestimated the prevalence of acetabular under- or overcoverage, which could have been improved by false-profile radiography or computed tomography evaluation. 23 Fourth, only hip joint degeneration was evaluated using radiographs to determine the clinical impact of changes in the lateral acetabular coverage. The use of magnetic resonance imaging to evaluate damage to the hip labrum and cartilage based on acetabular coverage changes would have provided more precise conclusions. Last, only a static evaluation was performed without considering muscle action. As patients place their weight on the affected limb, the hip abductors may affect the acetabular under- or overcoverage. 5 Motion analysis to detect the dynamic changes in the hip joint may provide a more robust conclusion.
Conclusion
The functional lateral acetabular coverage increased after CWHTO and decreased after OWHTO. Surgeons may want to consider the acetabular coverage of the ipsilateral hip joint when performing a unilateral HTO with a large correction.
Footnotes
Final revision submitted April 6, 2024; accepted April 17, 2024.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Kyung Hee University Hospital (KHUH 2021-08-024-001).