
Abstract
Background:
Posterior medial meniscus root (PMMR) tears (PMMRTs) can be repaired using various techniques to promote healing. However, the biomechanical properties of suture-relay all-suture anchor (ASA) versus conventional suture anchor (CSA) and loop-locking transtibial pullout (TTP) have not been well established.
Purpose:
To compare the biomechanical properties of PMMR repairs using suture-relay ASA, CSA, and loop-locking TTP.
Study Design:
Controlled laboratory study.
Methods:
A total of 33 fresh-frozen porcine knee joints with intact medial menisci were randomly divided into 3 groups, with 11 specimens in each group: ASA, CSA, and TTP. The study involved cyclic loading, with displacement measurements taken after 100, 500, and 1000 cycles. Subsequently, the specimens were loaded until clinical failure (defined as 3-mm displacement) and then to ultimate failure of the construct, with data recorded for displacement after cyclic loading, load to 3-mm displacement, and ultimate load to failure.
Results:
After 1000 cyclic loadings, the suture-relay ASA group showed considerably less displacement than the loop-locking TTP group (1.8 ± 0.7 mm vs 2.9 ± 0.3 mm; P < .001), but the displacements did not differ considerably between the suture-relay ASA and CSA groups (2.2 ± 0.9 mm; P > .05). The mean loads to clinical failure were significantly greater in the suture-relay ASA and CSA groups (61.3 ± 6.5 and 57.5 ± 9.7 N, respectively) than in the loop-locking TTP group (38.3 ± 9.4 N; P < .05). The ultimate load to failure was significantly greater in the suture-relay ASA group than in the loop-locking TTP group (153 ± 55.1 N vs 102 ± 12.9 N; P < .05). All specimens in the loop-locking TTP group failed by suture elongation mode, whereas only 2 specimens (18%) in the suture-relay ASA group and 5 specimens (45%) in the CSA group failed by suture elongation. Nine specimens (82%) in the suture-relay ASA group and 6 specimens (55%) in the CSA group failed due to suture cutout through the meniscal tissue.
Conclusion:
The biomechanical properties after PMMR repair did not statistically differ between the suture-relay ASA and CSA groups. The suture-relay ASA technique had a higher load to failure than the loop-locking TTP technique.
Clinical Relevance:
The suture-relay ASA technique is a promising option for the repair of PMMRTs; its repairing strength is also comparable to that of the CSA technique. Notably, the suture-relay ASA technique can be utilized without establishing a posteromedial portal, resulting in decreased procedure time and mitigating challenges associated with working from the posterior aspect of the knee.
Keywords
Posterior medial meniscus root (PMMR) tears (PMMRTs) are bony or soft tissue avulsions or radial tears within 1 cm from the posterior attachment. Meniscus root tears account for 10% to 21% of all meniscal tears, and approximately 8% are concomitant with anterior cruciate ligament injury.5,29 The meniscus root and its attachment are important in preventing meniscal extrusion under an axial load. A PMMRT increases the joint contact pressure and leads to loss of hoop strain resistance. Previous studies1,6 have shown that the knee biomechanics after a PMMRT are similar to total medial meniscectomy. Both situations produce the same effects on knee-joint contact pressure and kinematics, accelerating degenerative changes and the development of an osteoarthritic knee. 7 As medial meniscus root repair can restore the hoop strain function and reduce the joint contact pressure, 11 the repair could slow the osteoarthritis progression compared with the meniscectomy.12,17,28
Various techniques for PMMRT repair have been developed. Two common types of fixations are indirect fixation with transtibial pullout (TTP) and direct fixation using suture anchor techniques. The meniscus root is repaired through the standard anteromedial and anterolateral portals in the TTP technique. 15 An ultrahigh molecular weight polyethylene suture is shuttled into the tibial tunnel and fixed on the anteromedial cortex of the tibia. In direct fixation, a suture anchor is placed at the footprint of the meniscus root.4,14 This technique increases the stiffness because the meniscus is directly fixed to the anchor near the cortex. Meniscus root repair can also employ an all-suture anchor (ASA). Although the ASA repair can be performed via the posteromedial portal, it could also be performed via the anteromedial portal using the suture-relay of the anchor, which does not require a posteromedial portal. 3 The ASA is shuttled from the anteromedial portal into the tibial tunnel hole at the footprint of the meniscus by a loop suture. In a previous study, the ASA repair after PMMRT restored the tibiofemoral contact surface area and reduced contact pressure from the medial compartment of the knee. 24
The biomechanical properties after various PMMR repair techniques can influence the appropriateness of postoperative rehabilitation care. This study aimed to compare the biomechanical properties of PMMR repairs using suture-relay ASA, a conventional suture anchor (CSA), and loop-locking TTP. It was hypothesized that the biomechanical properties of the suture-relay ASA technique would be comparable to the CSA technique.
Methods
Biomechanical tests were performed on 33 fresh-frozen porcine knee joints with intact medial menisci. The specimens, aged between 24 and 30 weeks, were randomly assigned to the suture-relay ASA, CSA, or loop-locking TTP group (11 specimens in each group). This study was approved by the institutional review board (COA. MURA2020/868).
Specimen Preparation
The specimens were frozen at −20°C and thawed for 12 hours overnight before testing. The specimens were dissected, and all muscle and soft tissue were removed, leaving only the intact medial meniscus. The tibia was cut 20 cm from the joint line to facilitate specimen mounting. To create the PMMRT, a cut was made in the meniscal substance 5 mm from the tibial insertion of the PMMR 10 (Figure 1).

(A) Dissection of the porcine hind knee. All muscles and soft tissue were detached and disarticulated, leaving only the intact medial meniscus. A 20 cm-long cut was made in the tibia. (B) The posterior horn medial meniscus root was cut 5 mm from the tibial insertion. The arrow shows the aiming guide at the menisuc root cut site.
ASA Repair
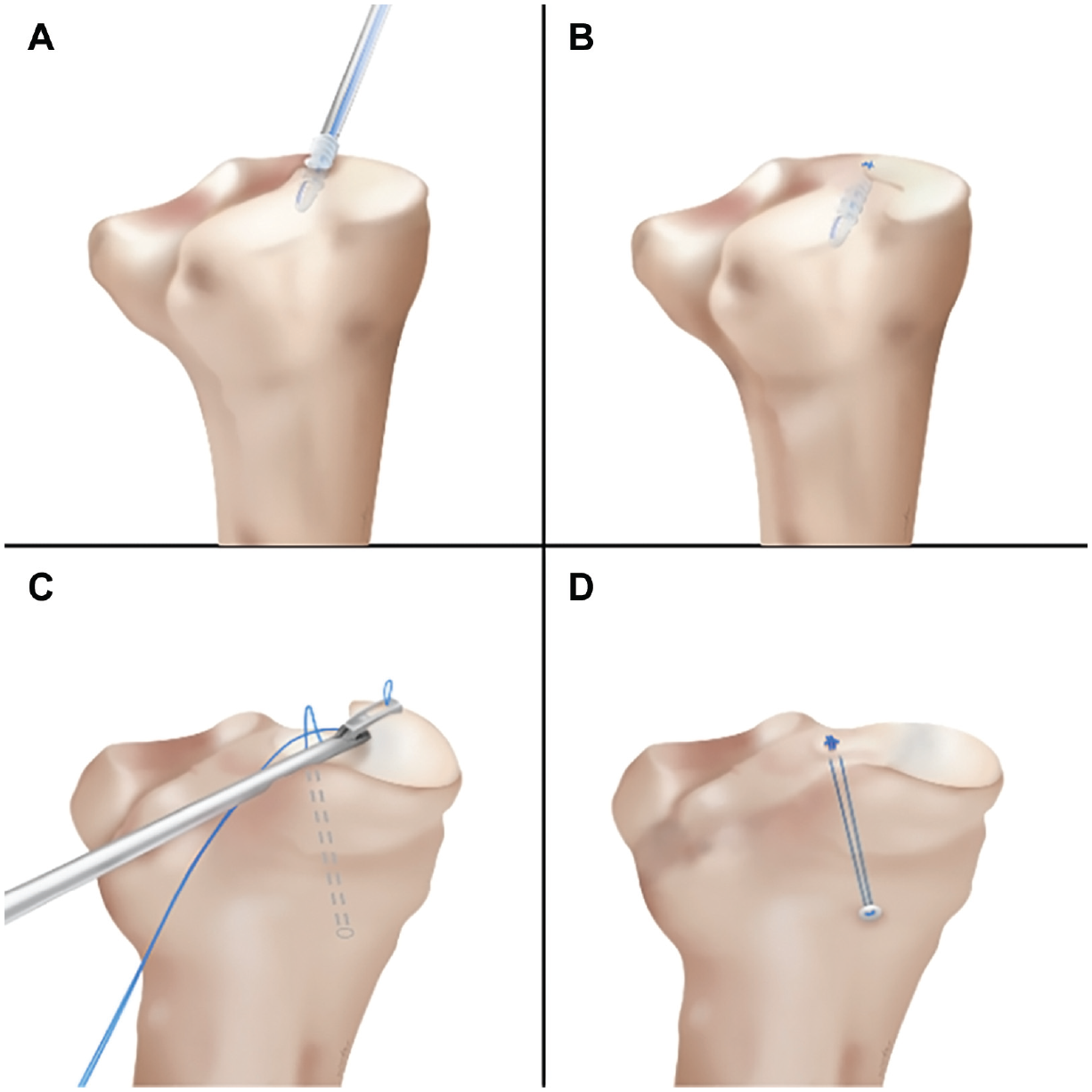
The tibial tunnel (diameter, 2.4 mm) was created using a tibial guide and a drill sheath (Smith & Nephew). The tibia was drilled from approximately 3 cm below the anteromedial tibial plateau to the footprint of the meniscus root. The ASA (2.8-mm Y-Knot RC; ConMed Linvatec) was unloaded from the inserter and held with a looped suture. The suture limb of the unloaded ASA was marked at 20 mm from the anchor using a marking pen. A spinal needle loaded with a nonabsorbable braided suture (No. 2 Ethibond; Ethicon) was inserted into the tibial tunnel as a loop suture. The ASA was pulled into the tibial tunnel using the loop suture until it reached the marked level. The ASA was deployed at the meniscus root footprint by pulling both suture limbs of the anchors back into the joint. The ASA collapsed and compressed under the bone, forming a ball-like shape providing a broad contact and fixation area. The suture was pretensioned to avoid displacement in the anchor hole (Figure 2). The torn meniscus was repaired with 4 suture limbs using a modified Mason-Allen technique with a suture passer. The suture was tied with nonsliding knots (Figure 3).

(A) The bone tunnel was created using a 2.4 mm–diameter pin and an anterior cruciate ligament aiming guide. (B) Unloading the 2.8-mm all-suture anchor from the inserter and holding it with a suture loop. (C) Insertion of a spinal needle loaded with a No. 2 nonabsorbable suture loop into the tunnel. (D) Shuttling the all-suture anchor by the looped suture into the tibial tunnel and then pulling it back to deploy. The arrows show the direction of needle insertion and the pulling back of the suture, respectively.

(A and B) The meniscus was repaired with a suture passer using a modified Mason-Allen stitch. (C and D) The sutures were tied with 5 nonsliding knots assisted by a knot pusher.
CSA Repair
A double-loaded suture anchor—5.5-mm CrossFT (CONMED Linvatec)—was placed at the footprint of the medial meniscus root. The anchor was screwed in along the superomedial to inferolateral and posterior to anterior directions, simulating anchor insertion from the posteromedial portal. The meniscus root was sutured using the modified Mason-Allen technique with a suture passer and tied with nonsliding knots, as performed in vivo (Figure 4, A and B).
(A) Conventional suture anchor repair: the suture anchor is inserted first, (B) followed by meniscus root repair using the modified Mason-Allen technique. (C) Transtibial pullout repair: a tibial tunnel is created, and the meniscus root is repaired with a suture passer. (D) The loop-locking technique secures the meniscus root, and the suture is shuttled through the tibial tunnel.
TTP Repair
A tibial tunnel (diameter, 2.4 mm) was created using a tibial-aiming drill guide. The tibia was retrograde drilled from approximately 3 cm below the anteromedial tibial plateau to the footprint of the meniscus root. The PMMRT was repaired with a nonabsorbable braided suture (No. 2 Hi-Fi; CONMED Linvatec) and sutured using the loop-locking technique with a suture passer (FIRSTPASS mini; Smith & Nephew). The free-end suture was shuttled through the tibial tunnel. The sutures were tensioned and tied with 5 square knots over a surgical button (Endobutton; Smith & Nephew) on the anteromedial tibia (Figure 4, C and D).
Biomechanical Testing
Mechanical testing was conducted at room temperature. The testing protocol was adopted from a previous study on meniscus root repair. 10 Cyclic displacement and load to failure were tested on a tensile testing machine (LRK-20KN; NTS). The remainder of the meniscus was detached from the joint capsular attachment. The meniscus was marked and held by a customized meniscal clamp 1 cm from the repair site. The load was applied parallel to the circumferential fiber of the PMMR, simulating the axial load over a repaired meniscus root during knee motion (Figure 5).

(A) The actuator stabilized the porcine tibia in the tensile testing machine. Note that the meniscus was detached from the joint capsular attachment. (B) The meniscal clamp was placed 1 cm from the repair site and loaded parallel to the meniscal circumferential fibers, representing the axial load during knee motions.
Each specimen was initially preloaded with 2 N then subjected to 1000 cycles under loads ranging from 5 to 20 N at a rate of 0.5 Hz. Displacements were recorded after 100, 500, and 1000 loading cycles. Next, the specimens were loaded to failure at 30 mm/min. This testing procedure was adopted in previous studies to simulate the tensile forces in a postoperative rehabilitation protocol.5,13,23 The load to clinical failure was defined as the load giving a displacement of 3 mm. 26 Finally, the ultimate load to failure was determined by increasing the load until the construct failed (as evidenced by suture elongation and consequent loss of fixation strength or by cutting of the suture through the meniscal tissue). The failure modes were also recorded.
Statistical Analysis
Eleven specimens per group are required to detect the differences between groups in terms of load to failure when a power of 0.80 and an alpha of .05 are used. 8 The sample size was calculated using G*Power 3.1.3 software (Franz Paul). The group-variable differences in load to clinical failure, ultimate load to failure, and stiffness were evaluated using a 1-way analysis of variance. The cyclic displacements after 100, 500, and 1000 cycles and the displacements at failure were analyzed by median regression analysis. The significance level was corrected using the Bonferroni adjustment. All statistics were analyzed using STATA software Version 16.1 (StataCorp LLC).
Results
Displacements After 100, 500, and 1000 Loading Cycles
No specimen failed during the cyclic loading test. The suture-relay ASA group showed significantly less displacement than the loop-locking TTP group after 1000 cycles (1.8 ± 0.7 mm vs 2.9 ± 0.3 mm, P < .001). No significant difference was found between the ASA and CSA groups after 100, 500, and 1000 loading cycles (Table 1).
Comparison of Displacements Among ASA, CSA, and TTP Groups a
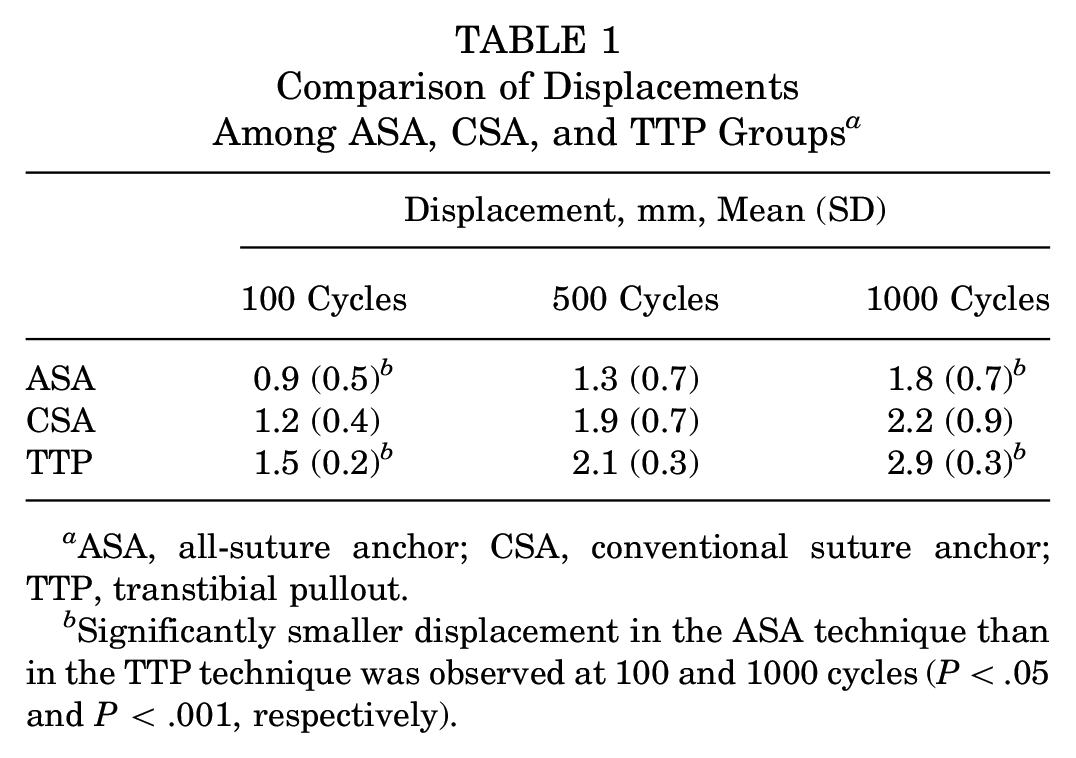
ASA, all-suture anchor; CSA, conventional suture anchor; TTP, transtibial pullout.
Significantly smaller displacement in the ASA technique than in the TTP technique was observed at 100 and 1000 cycles (P < .05 and P < .001, respectively).
Load to Clinical Failure, Ultimate Load to Failure, and Stiffness
The load to clinical failure and ultimate load to failure were significantly higher in the suture-relay ASA group than in the loop-locking TTP group (61.3 ± 6.5 N vs 38.3 ± 9.4 N and 153 ± 55.1 N vs 102 ± 12.9 N; P < .05). Meanwhile, the stiffness was significantly higher in the ASA and CSA groups than in the TTP group (13.3 ± 4.3, 13.7 ± 3.3, and 9.6 ± 1.5 N/mm, respectively; P < .05). No significant differences in load to clinical failure, ultimate load to failure, and stiffness were observed between the ASA and CSA groups (Table 2 and Figure 6).
Comparison of Loads to Clinical Failure, Ultimate Loads to Failure, and Stiffness a

Data are presented as mean (SD). ASA, all-suture anchor; CSA, conventional suture anchor; TTP, transtibial pullout.
The load to clinical failure, ultimate load to failure, and stiffness were significantly higher in the ASA group than in the TTP group (P < .001, P < .05, and P < .05, respectively).
The load to clinical failure and stiffness were significantly higher in the CSA group than in the TTP group (P < .001 and P < .05, respectively).

Box plots demonstrating the loads to clinical failure, ultimate loads to failure, and stiffness values of specimens repaired by the TTP, CSA, and ASA techniques. ASA, all-suture anchor; CSA, conventional suture anchor; TTP, transtibial pullout.
All specimens failed by 1 of 2 failure modes: suture elongation or cutout of the meniscus. All specimens in the loop-locking TTP group failed due to the suture elongation. In the suture-relay ASA group, 9 specimens (82%) failed by suture cutout of the meniscus, and 2 specimens (18%) failed by suture elongation. In the CSA group, 6 specimens (55%) failed by suture cutout of the meniscus, and 5 specimens (45%) failed by suture elongation. The mean displacement at failure was significantly higher in the loop-locking TTP group than in the suture-relay ASA and CSA groups (P < .01) but did not statistically differ between the ASA and CSA groups (P > .05) (Table 3).
Failure Modes and Displacements at Failure a

ASA, all-suture anchor; CSA, conventional suture anchor; TTP, transtibial pullout. A p-value of less than 0.01 indicates statistically significant differences between the groups.
Discussion
The main finding of this study was the significantly higher displacement in the loop-locking TTP group than in the suture-relay ASA and CSA groups. Similarly, a previous biomechanical study reported that the CSA technique reduces the displacement compared with the TTP technique during cyclic loading tests and raises the stiffness of meniscal repair compared with the TTP technique. 10 Meanwhile, the ultimate loads to failure were comparable in the specimens repaired by CSA and TTP. Although the biomechanical differences between the CSA and ASA groups were insignificant,8,9,19 smaller diameters in ASA better preserve the host bone and can be placed at the meniscal footprint from the anteromedial portal using the suture-relay technique. This technique avoids long sutures in the tunnel, which could compromise fixation stiffness.
The loads to clinical failure echoed the displacement results. The load to clinical failure in the suture-relay ASA group was similar to that of the CSA group but significantly higher than that of the loop-locking TTP group. According to Kopf et al, 16 the mean ultimate load to failure of the native meniscus root attachment is 678 N. Under a 500-N femorotibial load applied at 90° of knee flexion (corresponding to the tibiofemoral load during partial weightbearing), the mean tension at the meniscus root attachment is 60.1 N. 18 To our knowledge, the biomechanical properties of PMMRTs repaired by the suture-relay ASA, CSA, and loop-locking TTP techniques have not been previously compared. The present results showed that none of the repair techniques can restore the ultimate load to failure of the native meniscus. However, the fixation strengths of the suture-relay ASA and CSA techniques might be sufficient for restricted weight-bearing during the early postoperative stage.
Based on the failure mode, our study revealed that all loop-locking TTP repairs failed due to suture elongation, and the ultimate load to failure was less in the loop-locking TTP group than in the other groups. Our study results suggested that the load required to elongate the suture might have been reached before the suture could cut the meniscus in the loop-locking TTP group. Conversely, the suture-relay ASA and CSA groups, which have restricted suture movement in the tunnel of the construct, might have increased the load to ultimate failure. This finding likely explains why the suture-relay ASA group exhibited significantly less displacement after 1000 loading cycles than the TTP group. Additionally, both ASA and CSA groups demonstrated lower displacement at failure, mostly in a cutout mode, whereas the loop-locking TTP group failed due to suture elongation. The fixation strength and stiffness in the TTP group could be improved with different high-strength sutures or suture tapes, increasing the number of sutures placed through different meniscus layers with varying configurations. In a previous study, 10 the loop-locking technique provided less cyclic loading and load to failure compared with the modified Mason-Allen suture. Furthermore, movement of the suture within the bone tunnel might abrade the suture and reduce the suture strength before the meniscus is completely healed. Suture motion could also potentially widen the tibial tunnel and decrease the suture tension.21,22,27
Limitations
This study has inherent limitations that require a cautious interpretation of the findings. First, while there are clear structural and functional similarities between porcine and human knee joints, the absolute numbers obtained in our laboratory may not be directly comparable to those found in studies involving human knees. For instance, the meniscal tissue studied using the porcine model is slightly stiffer than the human meniscal tissue. 25 However, the main purpose of this study was to compare the biomechanical properties of PMMRTs repaired using different fixation methods. Second, our study focused on the immediate postrepair period and did not consider the changes in strength that occur as the repaired tissue heals over time in real-world clinical situations. Third, the procedures and knot tying in this study were performed in an open environment, which might not accurately reflect the difficulty in anchor placement and knot tying during arthroscopy. Last, the fixation strengths and failure modes of the specimens could have been influenced by the arrangement, number, and quality of the repaired meniscal tissue and the amount of surrounding cartilage removed during the repair process.2,20 A careful interpretation of the transposition of these current findings in the context of human clinical application is crucial. Further research involving human tissue is essential to facilitate its practical use and explore its potential benefits in clinical settings.
Conclusion
The suture-relay ASA technique of PMMR repair provided biomechanical properties comparable to those of the CSA technique. This technique also provided greater load to clinical failure, ultimate load to failure, and less displacement after cyclic loading than the loop-locking TTP technique. The suture-relay ASA technique, a standard arthroscopic technique that does not require posteromedial portal or tibial tunnel interferences, is a promising alternative technique for PMMR repair. Further investigation and evaluation in human cadaveric knee studies are warranted to validate its effectiveness and safety.
Footnotes
Final revision submitted March 18, 2024; accepted April 4, 2024.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Ramathibodi Hospital, Mahidol University (MURA2021/868).