
Abstract
Background:
Medial meniscus posterior root tear (MMPRT) repair is indicated in patients with preserved articular cartilage to prevent rapidly progressive osteoarthritis. However, there is limited published data on midterm outcomes after MMPRT repair.
Purpose:
To report the patient-reported outcome measures (PROMs), complication, and failure rate for patients undergoing MMPRT repair at a minimum of 5-year follow-up.
Study Design:
Case series; Level of evidence, 4.
Methods:
A single-institution prospectively collected database was retrospectively queried for patients who underwent isolated MMPRT repair from January 2016 to March 2019. Exclusion criteria included Kellgren-Lawrence grade ≥3 osteoarthritis, concurrent ligamentous or realignment procedures, all-inside suture anchor repair, and concomitant lateral meniscal tears. The clinical outcome measures included conversion to knee arthroplasty, the shortened Knee injury and Osteoarthritis Outcome (KOOS) Jr, International Knee Documentation (IKDC), and Veterans RAND 12-Item Health Survey (VR-12) scores. Clinical failure was defined as failing to achieve the minimal clinically important difference (MCID) for ≥1 PROM. The MCID and Patient Acceptable Symptom State (PASS) thresholds were derived from a peer-reviewed study and were as follows: IKDC (MCID, 10.2; PASS, 67.8), KOOS Jr (MCID, 10.4; PASS, 71.9) and VR-12 Physical (MCID, 6.1; PASS, 47.8).
Results:
A total of 38 patients who met inclusion criteria and underwent transtibial root repair before March 2019 were retrospectively identified, of which 36 (94.7%) were available for follow-up at mean 65.8 ± 6.7 months (range, 60-81). Of this total, 5 patients (13.9%) converted to arthroplasty (mean ± SD, 41.8 ± 28.0 months). Transtibial pullout repair had an overall survivorship of 97.2%, 94.4%, and 91.6% at the 1-year, 2-year, and 5-year time points, while 2 patients failed after 60 months postoperatively, for an 86.1% arthroplasty-free survivorship at mean 65.8 months. MCID and PASS achievement rates at final follow-up for KOOS Jr were 74.2% and 51.6%, respectively. Three patients (8.3%) failed to achieve MCID for any 1 of the 3 PROMs while 28 patients (77.8%) achieved the MCID for ≥1 PROM.
Conclusion:
Clinically significant outcomes for KOOS Jr were achieved in 74.2% and 51.6% of patients undergoing transtibial pullout repair for isolated MMPRT at 5-year follow-up. There was an 86.1% survivorship free of arthroplasty at midterm follow-up.
The menisci play a critical role in knee stability, proprioception, lubrication, and distribution of axial force in hooplike stresses. 19 Medial meniscus posterior root tears (MMPRT) are a distinct category of meniscal tears defined as a radial tear within 10 mm of the posterior horn attachment or either a bony or soft tissue avulsion of the posterior root. 30 These injuries have become an increasingly recognized pathology5,12 due to biomechanical evidence indicating that disruption of the meniscal attachment alters joint mechanics, resulting in tibiofemoral contact pressures comparable with those of a total meniscectomy.1,18 As such, meniscus root tears have been implicated in degenerative cartilage changes and rapidly progressive knee osteoarthritis (OA).4,26,28,32,33 Notably, previous literature has indicated that 92.8% of adults who underwent a total knee replacement under the age of 60 had an associated meniscus root tear, further emphasizing the deleterious effects of this pathology previously referred to as a “silent epidemic.”6,12
Traditionally, the management of MMPRT has involved nonoperative approaches or partial meniscectomy.4,34 However, nonoperative management has yielded unsatisfactory outcomes, with 31% of adults undergoing total knee arthroplasty (TKA) within a mean follow-up period of 30 months. 28 Similarly, meniscectomy has shown poor results, with a previous meta-analysis indicating that OA rates reached 99% after meniscectomy at minimum follow-up of 5 years for meniscus root tears. 35 Emerging evidence underscores transtibial pullout repair as an effective surgical treatment for these injuries. 7 Although it may not entirely prevent cartilage degradation, transtibial pullout repair significantly decelerates OA progression compared with meniscectomy and nonoperative management at midterm follow-up. 23 Moreover, it has been demonstrated to be a cost-effective alternative to meniscectomy and nonoperative approaches for managing MMPRT. 17
To date, there are limited reports of clinical outcomes of transtibial pullout repair and conversion to arthroplasty rates at mid- to long-term follow-up.3,10,23 Furthermore, recent evidence suggests that modifications to transtibial pullout repair techniques, such as alterations in suture configuration and the treatment of the medial collateral ligament (MCL), may affect outcomes.20,21 Previous studies examining the outcomes of root repair at midterm follow-up have not commented on root repair techniques or addressed the achievement of the minimal clinically important difference (MCID) and Patient Acceptable Symptom State (PASS) in patients who do not experience treatment failure.3,10,23 The purpose of this study was to report on patient-reported outcome measures (PROMs), reoperation rate, and failure rate for patients undergoing transtibial pullout repair for isolated MMPRT at a minimum of 5-year follow-up. We hypothesized that at midterm follow-up, patients undergoing root repair will exhibit an arthroplasty-free survival rate of ≥80% and that ≥70% of patients would achieve MCID thresholds.
Methods
This retrospective cohort study utilized data from a prospectively collected database at a single institution to examine outcomes of transtibial pullout repair for MMPRT over a period from January 2016 to March 2019. Diagnosis of MMPRT was established through patient history, physical examination suggestive of meniscal injury corroborated by magnetic resonance imaging (MRI) findings, and subsequent confirmation via arthroscopy before repair. Exclusion criteria encompassed Kellgren-Lawrence (KL) grade ≥3 osteoarthritis, simultaneous ligamentous or realignment procedures, all-inside suture anchor root repair, and concurrent tears of the lateral meniscus. Patients lacking complete baseline or postoperative PROMs with a minimum follow-up duration of 5 years were also excluded. The study received institutional review board approval, including permission for database access and patient contact for follow-up.
Preoperatively collected data included age, sex, body mass index (BMI), cardiac disease, diabetes, hypertension, thyroid disease, psychiatric disease, tobacco use, and mean follow-up. Preoperative radiograph and MRI were also evaluated for KL grade and preoperative joint space remaining on Rosenberg flexion weightbearing view in addition to mechanical axis alignment, and meniscal extrusion. Meniscal extrusion was assessed in millimeters of the medial meniscus from the edge of the medial tibial plateau on the coronal slice at the halfway point of the medial femoral condyle, following the methodology proposed by Costa et al. 13 Intraoperative data included the number of tunnels, sutures, suture configuration, MCL trephination, and method of fixation. PROMs were recorded preoperatively and at minimum 5-year follow-up.
A secure electronic platform (Patient IQ) was used for both the storage and the distribution of PROMs via phone and email. The PROMs investigated in this study included International Knee Documentation Committee (IKDC), Knee injury and Osteoarthritis Outcome Score (KOOS) Jr (a shortened version of the original KOOS score), Veterans RAND 12-Item Health Survey (VR-12) Mental and Physical component scores. Thresholds for MCID and PASS achievement were applied to assess clinically significant improvement after root repair. These thresholds were established in a separate study that is forthcoming in Orthopaedic Journal of Sports Medicine. That study utilized a distribution-based approach to determine MCID and an anchor-based approach for PASS. The cohort used in that study consisted of patients undergoing isolated MMPRT repair using a transtibial pullout technique at ≥2-year follow-up. The thresholds for clinically significant outcome achievement were as follows: IKDC (MCID, 10.2; PASS, 67.8), KOOS Jr (MCID, 10.4; PASS, 71.9), and VR-12 Physical (MCID, 6.1; PASS, 47.8). MCID and PASS thresholds for VR-12 Mental were not established in the prior study due to low reliability (AUC < 0.70). Clinical failure was defined as patients who did not achieve MCID for ≥1 of 3 PROMs. The primary outcome measures of this study included the rates of conversion to knee arthroplasty, either total knee arthroplasty (TKA) or unicompartmental knee arthroplasty (UKA), and clinical failure. Secondary clinical outcome measures included MCID and PASS achievement for KOOS Jr, IKDC, and VR-12 in addition to complication and reoperation rates.
Surgical Technique
Three fellowship-trained orthopaedic surgeons (B.J.C., A.B.Y. and N.N.V.) performed a medial meniscus posterior root transtibial pullout repair procedure using arthroscopic techniques using either 1 or 2 transtibial tunnels, based on surgeon preference. Diagnostic arthroscopy was initially performed through standard portals, confirming the presence of an MMPRT. The MCL was trephinated to open the medial joint space at surgeon preference. Nonabsorbable sutures were passed through the posterior medial meniscus and brought through either 1 or 2 transtibial tunnels located at the anatomic footprint of the posterior medial meniscus root. The footprint was prepared using a combination of curette and shaver. The sutures were then secured either through a suture anchor or a cortical button and appropriately tensioned on the anterior tibia to complete the repair (Figure 1). A detailed description of all surgical techniques utilized are outlined in Table 1.

(A) Full-thickness tear of the posterior root of the medial meniscus visualized during arthroscopy. (B) Suture-passing device passed through the far posterior portion of the detached meniscus root. (C) Passage of the second suture positioned through the midportion of the meniscus root and anterior to the first suture.
Intraoperative Techniques Utilized a
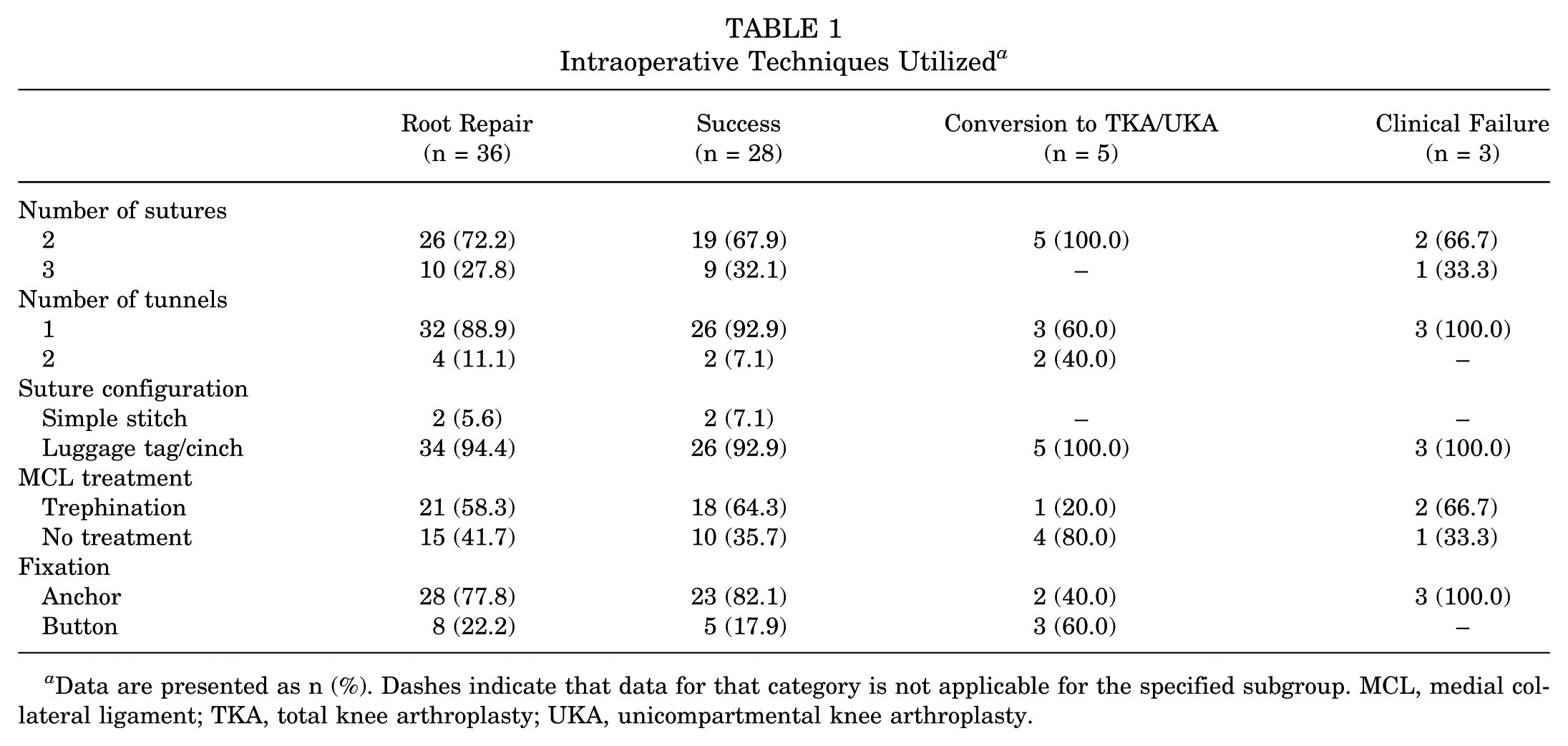
Data are presented as n (%). Dashes indicate that data for that category is not applicable for the specified subgroup. MCL, medial collateral ligament; TKA, total knee arthroplasty; UKA, unicompartmental knee arthroplasty.
After surgery, a standardized postoperative rehabilitation regimen was implemented. Patients were instructed to remain nonweightbearing while wearing a hinged knee brace for 6 weeks, with knee range of motion limited to 0° to 90° for the first 4 weeks. At the 6-week mark, patients were permitted to begin weightbearing activities as tolerated, discontinue the hinged knee brace, and resume full range of motion. Closed chain exercises were initiated at 8 weeks, and jogging was allowed to commence at 3 months postoperatively.
Statistical Analysis
Descriptive statistics were generated with RStudio Team (2022) (RStudio: Integrated Development Environment for R). A Kaplan-Meier curve was generated within the RStudio platform to depict conversion to arthroplasty across the 1-year, 2-year, and 5-year time points. Paired Student t tests were applied to evaluate the significance of improvement in PROMs from baseline to final follow-up. Significance was set at P < .05.
Results
A total of 38 patients were eligible for study inclusion, and 36 (94.7%) were available for minimum 5-year follow-up (Figure 2). Mean follow-up was 65.8 ± 6.7 (range, 60-81) months. Preoperative weightbearing radiographs demonstrated a mean K-L grade of 1.7 ± 0.5 (range, 1-2) while mean medial joint space remaining was 4.8 ± 1.4 mm (range, 2.5-9.8 mm). Long limb radiographs were obtained in 18 patients with a mean 4.8°± 3.3° of varus (range, 0.5°-10.7°). Preoperative MRI was obtained for all patients, and the mean preoperative extrusion was 4.1 ± 1.1 mm (range, 1.6-6.2 mm) (Table 2). The most prevalent comorbidities included a history of hypertension (44.4%) and tobacco use (27.8%) (Table 3).

Flowchart of patient selection. ACL, anterior cruciate ligament; PROM, patient-reported outcome measure.
Patient Demographics a

Data are presented as mean ± SD or n, unless otherwise indicated. Dashes indicate that data for that category is not applicable for the specified subgroup. BMI, body mass index; KL, Kellgren-Lawrence; TKA, total knee arthroplasty; UKA, unicompartmental knee arthroplasty.
Patient Comorbidities a
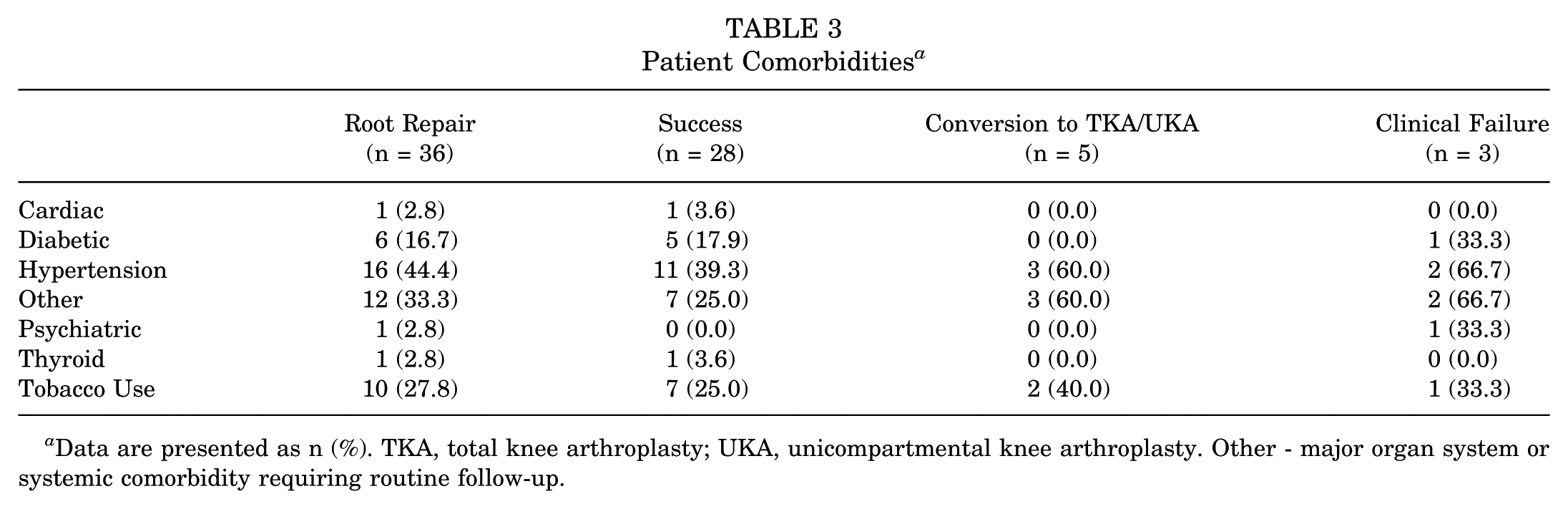
Data are presented as n (%). TKA, total knee arthroplasty; UKA, unicompartmental knee arthroplasty. Other - major organ system or systemic comorbidity requiring routine follow-up.
Complications, Reoperations, and Conversion to Arthroplasty
After root repair, 1 patient underwent manipulation under anesthesia with lysis of adhesions for arthrofibrosis at 12.6 months postoperatively. Two patients underwent subsequent procedures of the ipsilateral knee. One patient underwent knee arthroscopy for an undersurface tear of the medial meniscus, which was meniscectomized. A second patient was found to have a tear of the midbody and underwent a partial medial meniscectomy, leaving 75% of the peripheral rim with an additional lateral partial meniscectomy. During arthroscopy, the posterior meniscus root was found to be intact in both cases. A total of 17 (47.2%) patients received ≥1 postoperative intra-articular corticosteroid injection of which 16 out of 17 (94.1%) had a history of intra-articular corticosteroid injections before arthroscopy. The mean time from arthroscopy to the first postoperative injection was 17.0 ± 16.6 months. Out of the 8 patients who converted to arthroplasty or were found to be clinical failures, a total of 6 (75.0%) patients underwent ≥1 postoperative intra-articular injection.
Five patients converted to arthroplasty (TKA, n = 3; UKA, n = 2) at 10.7, 15.1, 45.9, 66.4, and 70.7 months postoperatively (mean ± SD, 41.8 ± 28.0 months) (Table 4). Overall, transtibial pullout repair survivorship rates at the 1-year, 2-year, and 5-year time points were 97.2%, 94.4% and 91.6%, respectively, with 2 patients (5.6%) converting to TKA beyond the 5-year postoperative time point. The overall survivorship free of knee arthroplasty at mean 65.8 months follow-up was 86.1% (Figure 3). Five patients were found to be ≥5° of varus on preoperative long leg radiographs. Of these 5 patients, 2 patients converted to arthroplasty before final follow-up.
Reoperation and Failure Rates a

Data are presented as n or n (%) unless otherwise indicated. Dashes indicate that data for that category is not applicable for the specified subgroup. TKA, total knee arthroplasty; UKA, unicompartmental knee arthroplasty.

Kaplan-Meier survival curve for transtibial pullout repair.
Patient-Reported Outcome Measures
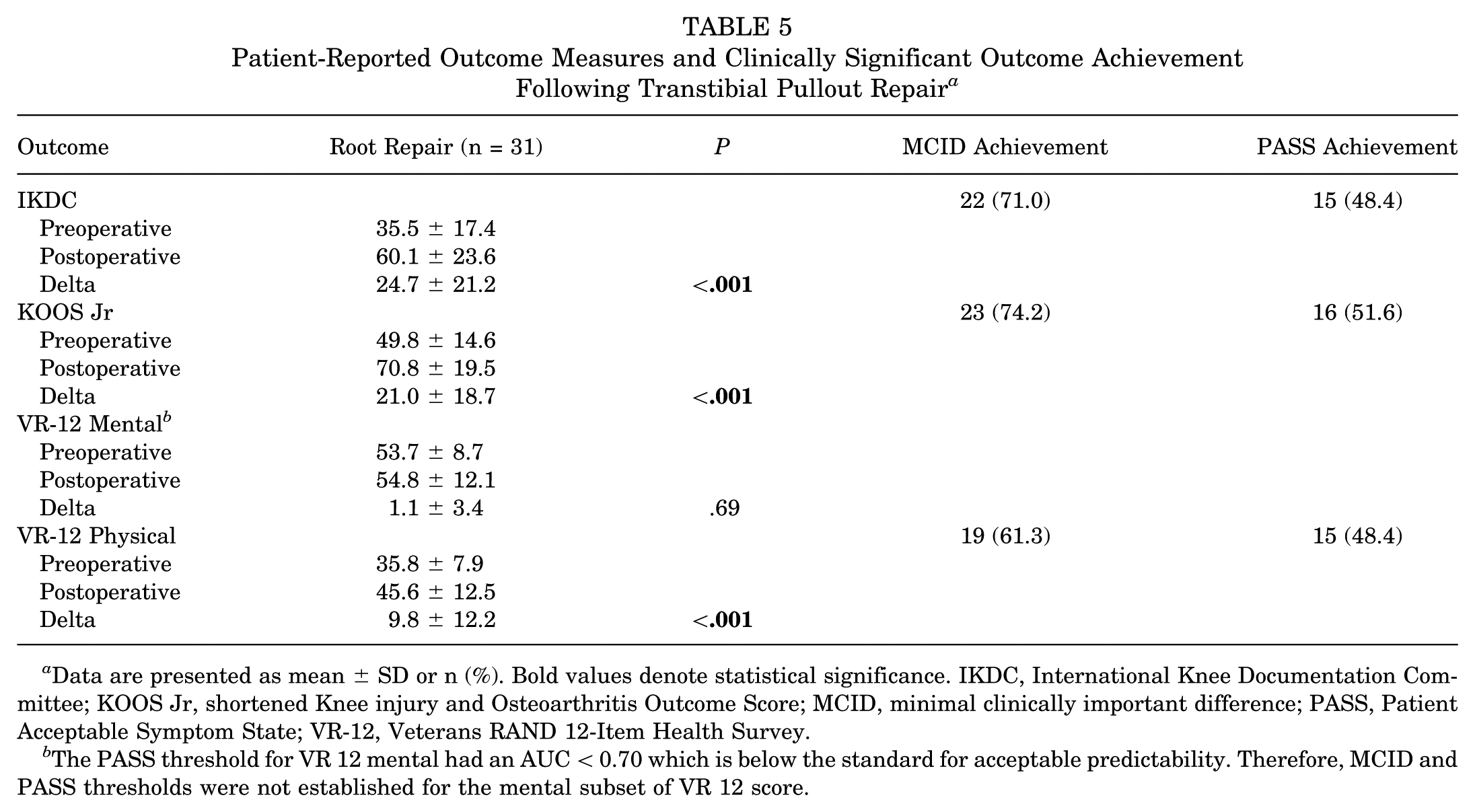
The mean preoperative IKDC, KOOS Jr, VR-12 Mental, and VR-12 Physical scores were 35.5 ± 17.4, 49.8 ± 14.6, 53.7 ± 8.7, and 35.8 ± 7.9, respectively. At a final mean follow-up of 65.8 months, the IKDC (60.1 ± 23.6; P < .001), KOOS Jr (70.8 ± 19.5; P < .001), and VR-12 Physical (45.6 ± 12.5; P < .001) scores significantly improved postoperatively from baseline values. MCID achievement for IKDC, KOOS Jr, and VR-12 Physical ranged from 61.3% to 74.2%, while PASS achievement ranged from 48.4% to 51.6% (Table 5). Three patients (8.3%) did not achieve MCID for ≥1 of the 3 PROMs evaluated and were noted as clinical failures. A total of 28 patients (77.8%) achieved MCID for ≥1 PROM at a minimum of 5-year follow-up.
Patient-Reported Outcome Measures and Clinically Significant Outcome Achievement Following Transtibial Pullout Repair a
Data are presented as mean ± SD or n (%). Bold values denote statistical significance. IKDC, International Knee Documentation Committee; KOOS Jr, shortened Knee injury and Osteoarthritis Outcome Score; MCID, minimal clinically important difference; PASS, Patient Acceptable Symptom State; VR-12, Veterans RAND 12-Item Health Survey.
The PASS threshold for VR 12 mental had an AUC < 0.70 which is below the standard for acceptable predictability. Therefore, MCID and PASS thresholds were not established for the mental subset of VR 12 score.
Discussion
The main findings of this study demonstrate 86.1% survivorship free of UKA or TKA at a mean 65.8-month follow-up using contemporary arthroscopic transtibial pullout MMPRT repair techniques with minimum of 2 sutures and either suture anchor or cortical button fixation on the anterior tibia. Despite 77.8% of patients achieving MCID for ≥1 PROM, only 48.4% and 51.6% of patients achieved PASS for the IKDC and KOOS Jr scores, respectively, indicating improvement in pain and function but still some degree of persistent symptoms.
The superiority of meniscus root repair in comparison with nonoperative management or partial meniscectomy in patients without advanced OA has been well-documented.12,28,29 In one of the few natural history studies of MMPRT to date with 5-year follow-up, Krych et al 28 reported that 87% of patients failed to respond to nonoperative treatment and 31% converted to TKA at a mean 30 months after their diagnosis. Similarly, Krych and colleagues 28 conducted a separate study to investigate if partial meniscectomy was superior to nonoperative care in symptom management of degenerative MMPRT and reported no advantage to meniscectomy. In fact, the authors reported that 54% (14 of 26 patients) converted to TKA at a mean 54.3 months after partial meniscectomy. 27 Furthermore, a matched 1:1:1 cohort study based on meniscal laterality, age, sex, and KL grade of patients with MMPRT who underwent nonoperative care, partial meniscectomy, or MMPRT repair at mean 74-month follow-up also found nonoperative care (4/15 patients; 26.7%) and partial meniscectomy (9/15 patients; 60%) to have significantly higher conversion rates to TKA than MMPRT repair (0/15 patients; 0%). 3 In contrast to the high rates of arthroplasty conversion with nonoperative care or partial meniscectomy, a recent systematic review of root tears that included 5 studies reporting on conversion to TKA after MMPRT repair reported an failure rates ranging from of 0% to 22% (11 failures in 205 knees at a mean follow-up 85.8-125.9 months). 29 Others have corroborated these findings of much lower rates of conversion to arthroplasty with MMPRT repair over other treatment options. In a separate systematic review and meta-analysis by Krivicich et al, 24 the authors compared clinical outcomes of partial meniscectomy with MMPRT repair reported 9.8% (8 of 82 patients) conversion rate to TKA at a mean 64.8-month follow-up in the repair cohort. The results of the present study are largely concordant with the findings of these systematic reviews, as our study found 91.6% survivorship free of UKA or TKA at 5 years and 86.1% survivorship extending to a mean 65.8-month follow-up.
There has been limited study on outcomes of MMPRT repairs at minimum 5-year follow-up. Much of the work that does exist is from Chung et al who reported 99% survivorship free from TKA at 5 years9 and 92% at 8 years11 in a series of 91 patients following isolated MMPRT repair (mean age, 58.7 years; mean follow-up, 84.8 months). The authors describe a transtibial pullout repair technique using a simple suture configuration (2-3 sutures), similar to the technique most commonly utilized in the present study, tied over a button on the anterior tibia. 11 Their series of patients is similar to the patients in the present study in terms of mean medial joint space width remaining preoperatively (4.7 mm per Chung et al9 compared with 4.8 mm per the current study) as well as all patients having KL grade <3 OA; however, the patient series of Chung and colleagues9 had a mean BMI of 25.6 kg/m2, vastly lower than the mean 33.9 kg/m2 in the present study. Notably, the 3 patients who were found to be clinical failures had a mean BMI of 40.8 (range, 38.1-44.8). While this suggests that higher BMI could potentially contribute to reduced survivorship at midterm follow-up, our sample size of failures is too small to confirm this relationship. Further studies with larger cohorts are needed to investigate whether BMI affects the durability of MMPRT repairs at minimum 5-year follow-up.
A follow-up investigation by Chung and colleagues 10 compared 18 patients who underwent partial meniscectomy with 37 patients with transtibial pullout MMPRT repair at minimum 10-year follow-up. The authors noted that 56% of patients in the meniscectomy group converted to TKA during the study period while only 22% in the repair group converted to TKA. On Kaplan-Meier analysis, the 10-year survival rates for the meniscectomy and repair groups were 44.4% and 79.6%, respectively. 10 As the authors acknowledge, there may be selection bias, as clinical decision making for partial meniscectomy versus MMPRT repair was at the discretion of the surgeon. In their MMPRT repair group, significant sustained improvements in Lysholm and IKDC scores were seen (mean improvement: Lysholm, 24.8; IKDC, 22.7); however, the authors did not report achievement of clinically significant outcomes including MCID or PASS. 10 Our study found the IKDC (60.1 ± 23.6; P < .001), KOOS Jr (70.8 ± 19.5; P < .001), and VR-12 Physical (45.6 ± 12.5; P < .001) scores all significantly improved postoperatively from baseline values. MCID achievement for IKDC, KOOS Jr, and VR-12 Physical were 71.0%, 74.2%, and 61.3%, respectively. Furthermore, PASS achievement for IKDC, KOOS Jr, and VR-12 Physical were 48.4%, 51.6%, and 48.4%, respectively. These findings suggest durable, meaningful improvements in symptoms and function from the preoperative state, yet approximately half of patients are still experiencing some degree of symptoms as indicated by PASS achievement rates. The findings of the present study can help counsel patients that MMPRT transtibial pullout repair will significantly improve patient-reported symptoms and functional status extending to midterm follow-up in the vast majority of patients with low rates of arthroplasty conversion, but some may have lingering symptoms that they deem unacceptable.
Identifying patient-specific variables that may portend achievement of clinically significant outcome measures at mid- and long-term follow-up remains an area in need of further investigation. The results of the present study add to the growing body of literature demonstrating that MMPRT repairs lower the rates of conversion to arthroplasty and improve patient symptoms; however, as the ~50% PASS achievement rate for multiple PROMs in our study indicates, more work is needed to identify variables associated with success or failure, some of which may be able to be addressed at the time of repair. Previously described risk factors for MMPRT and failure of repair include older age, meniscal extrusion, BMI >30 kg/m2, varus malalignment >5°, and Outerbridge grade ≥3 chondral lesions in the medial compartment.8,9,22,36 Many of these investigations include small patient cohorts and <5-year follow-up. More recently, there has been increased focus regarding centralization techniques for correcting meniscal extrusion to improve joint contact mechanics and potentially improve the clinical outcome of an MMPRT repair.2,14,15,25 Similarly, the effects of increased posterior tibial slope on forces seen by the posterior medial meniscus root and risk for tearing have been explored biomechanically 31 and clinically with a greater posterior tibial slope medially being associated with MMPRT. 16 It remains to be seen if there are additional variables that may portend a poor outcome after MMPRT repair and if correction of factors such as increased posterior tibial slope or meniscal extrusion will improve survivorship free of arthroplasty and achievement of clinically significant outcomes compared with current techniques.
Limitations
This study is not without limitations. The study design is a retrospective case series of prospectively collected data with limitation inherent to retrospective investigations including possible selection bias. The sample size was insufficiently powered to perform comparative subanalysis between patients who converted to TKA and those that did not at minimum 5-year follow-up to identify risk factors for failure. Preoperative radiographs, including long limb and Rosenberg weightbearing view, were not available in all patients. Similarly, postoperative radiographs and/or MRIs were not available at minimum 5-year follow-up for the vast majority of patients. Therefore, healing rates of root repair outside of clinical examination and progression or lack of progression of joint space narrowing radiographically cannot be commented on. Although conversion to TKA is a clinically relevant endpoint, TKA is an elective procedure that is influenced by patient considerations, surgeon recommendations, and symptom severity. Progressive joint degeneration and meniscal compromise cannot be evaluated in the absence of serial imaging.
Conclusion
Clinically significant outcomes for KOOS Jr were achieved in 74.2% and 51.6% of patients undergoing transtibial pullout repair for isolated MMPRT at 5-year follow-up. There was an 86.1% survivorship free of arthroplasty at midterm follow-up.
Footnotes
Final revision submitted April 11, 2025; accepted May 19, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.C. is a board or committee member of the AOSSM, Arthroscopy Association of North America, and International Society of Arthroscopy, Knee Surgery, and Orthopaedic Sports Medicine; is a paid consultant for Arthrex Inc, CONMED Linvatec, Ossur, RTI Surgical Inc, Smith & Nephew, and Vericel Corporation; has received hospitality payments from Breg Inc, DePuy Synthes Sales Inc, Joint Restoration Foundation Inc, Medical Device Business Services Inc, Pacira Pharmaceuticals Incorporated, SI-Bone Inc, and Vericel Corporation; has received support for education from Midwest Associates; and is a paid presenter or speaker for Smith & Nephew. B.J.C. has received research support from Aesculap/B.Braun, Arthrex Inc, and National Institutes of Health (National Institute of Arthritis and Musculoskeletal and Skin Diseases and National Institute of Child Health and Human Development); is a paid consultant for Acumed LLC, Arthrex Inc, Bioventus LLC, DJO LLC, Endo Pharmaceuticals Inc, Flexion Therapeutics Inc, Geistlich Pharma, North America Inc, Pacira Pharmaceuticals Incorporated, and Vericel Corporation; is an editorial or governing board member of the American Journal of Sports Medicine and Journal of the American Academy of Orthopaedic Surgeons; is a board or committee member of the Arthroscopy Association of North America; has stock or stock options in Bandgrip Inc and Ossio; receives IP royalties from Arthrex, Inc, and Elsevier Publishing; has received hospitality payments from Encore Medical LP, Flexion Therapeutics Inc, GE Healthcare, Geistlich Pharma, North America Inc, Mallinckrodt LLC, Merck Shapre and Dohme Corporation, Organogenesis Inc, Orthofix Medical Inc, PAVmed Inc, Pinnacle Inc, Pylant Medical, Summit Surgical Corp, Trice Medical Inc, and Zimmer Biomet Holdings Inc; has received other financial or material support from JRF Ortho; is a paid presenter for LifeNet Health and Terumo BCT; and has received publishing royalties and financial or material support from Operative Techniques in Sports Medicine and is a paid consultant for Ferring Pharmaceuticals Inc A.B.Y. has received hospitality payments from Aesculap Biologics LLC, Breg, Linvatec, Joint Restoration Foundation Inc, Vericel Corporation, and Zimmer Biomet Holdings Inc; is a paid consultant for AlloSource, JRF Ortho, Olympus America Inc, and Stryker; has received research support from Arthrex Inc and Organogenesis; has stock or stock options in Icarus Medical, Patient IQ, and Sparta Biomedical; has received support for education from Medwest Associates; is an unpaid consultant for Patient IQ and Sparta Biomedical; and is a paid presenter or speaker for Stryker. N.N.V. has received hospitality payments from Abbot Laboratories, Axonics Inc, Boston Scientific Corporation, Foundation Fusion Solutions LLC, IBSA Pharma Inc, Nalu Medical Inc, Nevro Corp, Orthofix Medical Inc, Pacira Pharmaceuticals Incorporated, Relievant Medsystems Inc, Salix Pharmaceuticals, Vericel Corporation, and Vertos Medial Inc; is a board or committee member of the AOSSM, American Shoulder and Elbow Surgeons, and Arthroscopy Association of North America; receives IP royalties from Arthrex Inc, Graymont Professional Products IP LLC, Smith & Nephew, and Stryker; has received research support from Arthrex Inc, Breg, Ossur, Smith & Nephew, and Stryker; is a paid consultant for Medacta USA Inc and Stryker; has received support for education from Medwest Associates; is an editorial or governing board member of SLACK Incorporated; and has received travel and lodging from Spinal Simplicity LLC. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Rush University Medical Center (No. 23083005).