
Abstract
Background:
Patellar dislocation is a common knee injury and up to 35% of those who dislocate the patella can develop recurrent patellar instability. In the setting of recurrent instability, medial patellofemoral ligament (MPFL) reconstruction is often performed to restore knee stability. There has been recent interest in patient and surgical factors that influence outcomes of MPFL reconstruction. Much of the previous work has focused on influences of anatomic measures; however, patients and injury characteristics may also impact surgical outcomes.
Hypothesis:
Patients who experience >2 patellar dislocations before MPFL reconstruction would demonstrate poorer patient-reported outcomes (PROs) compared with those with ≤2 previous dislocations.
Study design:
Cohort study; Level of evidence, 3.
Methods:
Records were reviewed to identify patients who underwent MPFL reconstruction at a single institution between 2008 and 2016. Patients who underwent concomitant tibial tubercle osteotomy or fixation of an osteochondral fracture were excluded. Patient demographics (age, sex, body mass index [BMI]), number of previous patellar dislocations, and patient anatomic measures (Caton-Deschamps index (CDI), tibial tubercle-trochlear groove (TT-TG) distance, and trochlear sulcus angle) were collected. PROs were assessed with Norwich Patellar Instability score, Knee injury and Osteoarthritis Outcome Score (KOOS), and Marx activity score. Outcomes of patients with >2 patellar dislocations were compared with those with ≤2 dislocations using multiple linear regression analysis.
Results:
Medical record review revealed 160 patients who underwent isolated MPFL reconstruction (71 with ≥2 dislocations and 89 with >2 dislocations); 95 patients (59%) completed PROs at a median follow-up of 4.6 years postoperation (range, 1.0-12.6 years). Patients with ≥2 dislocations were younger (≥2 dislocations: 20.7 ± 7.3 years, >2 dislocations: 28.5 ± 10.0 years; P < .001), although there were no other differences in demographics or radiographic anatomic measures between groups. Adjusting for age, sex, BMI, CDI, TT-TG distance, and trochlear sulcus angle, patients with >2 dislocations had 13.7 points lower KOOS-Pain (P = .003), 8.3 points lower KOOS-Activities of Daily Living (P = .025), 18.2 points lower KOOS-Sports and Recreation (P = .009), and 19.8 points lower KOOS-Knee-Related Quality of Life (P = .008) subscale scores than patients with ≤2 dislocations. No significant differences in KOOS symptoms subscale, Norwich Patellar Instability, or Marx score were noted between groups.
Conclusion:
Patients with >2 patellar dislocations before MPFL reconstruction exhibited poorer PROs at a median of 4.8 years postoperation compared with those who had ≤2 dislocations before surgery, when adjusting for age, sex, BMI, CDI, TT-TG distance, and trochlear sulcus angle.
Patellar dislocation is a relatively common injury, affecting primarily young active patients. The incidence is higher in certain contact sports and in female patients. 17 Whereas first-time patellar dislocations are generally treated nonoperatively, recurrent patellar instability can develop. Recent risk stratification models have identified younger age and certain anatomic factors as predictors of recurrence, with recurrent instability risk as high as 75% to 80% in some populations.7,14,29 After the development of recurrent instability, surgical treatment is frequently recommended. 31
While multiple surgical procedures have been described for the treatment of recurrent patellar instability, reconstruction of the medial patellofemoral ligament (MPFL) has become the gold standard treatment in the majority of patients. 31 The MPFL is the primary soft tissue restraint to lateral patellar translation and is frequently injured in the setting of a patellar dislocation. 5 Clinical studies have described excellent outcomes of isolated MPFL reconstruction in appropriately selected patients, with recurrent instability risk between 2% and 5% described.16,25
Although isolated MPFL reconstruction does yield excellent outcomes in most patients, it is not a silver bullet for the treatment of all patients with recurrent patellar instability. Multiple recent studies evaluating the outcomes of MPFL reconstruction have strived to identify factors that lead to poor outcomes.2,13,20,21,24,25 The majority of these studies have focused on the anatomic abnormalities alluded to above, including trochlear dysplasia, patella alta, and lower extremity torsional and coronal plane malalignments. While findings vary, it is generally accepted that anatomic abnormalities sufficient enough to create substantial patellar maltracking (obligatory dislocation or very large J-sign) are contraindications to isolated MPFL reconstruction and require additional procedures. 24 Evaluation of the impact of other patient and history factors on outcomes of isolated MPFL reconstruction has been limited.
One potential factor impacting the outcome of isolated MPFL reconstruction is the number of previous patellar dislocations sustained by the patient. While surgical treatment is often considered after the second patellar dislocation, 31 many patients sustain multiple patellar dislocations on the index knee before surgical treatment. Each recurrent patellar dislocation event stretches and further damages the medial soft tissue restraints to lateral patellar translation. 18 More dislocation events before surgery could therefore lead to increased load on the reconstructed ligament given more damage to native tissues and potentially increased failure risk.
We hypothesized that patients who have had >2 patellar dislocations before MPFL reconstruction would demonstrate poorer patient-reported outcomes (PROs) compared with those who have experienced ≤2 dislocations before surgery.
Methods
This study was approved by our institutional review board. Patient enrollment took place between 2008 and 2016. Consent was received from all patients before participation. Medical record review was utilized to identify retrospectively all patients treated for patellar instability with MPFL reconstruction between 2008 and 2016 at a single academic medical center. Retrospective chart review was performed to record patient demographic (age, sex, and body mass index [BMI]) and injury history information, including the number of patellar dislocations that occurred in the index knee before surgery. Preoperative imaging review was undertaken to measure and record anatomic factors that may affect outcomes of patellofemoral surgery. Imaging reviewed included plain films and magnetic resonance imaging and all measures were made by the senior author (R.A.M.). The Caton-Deschamps index (CDI),4,6 trochlear sulcus angle, 1 and tibial tubercle-trochlear groove (TT-TG) 26 distance were measured as described previously. Operative reports and intraoperative photographs from arthroscopy (performed in all cases) were also reviewed to quantify patellofemoral articular cartilage status at the time of surgery (based on the International Cartilage Repair Society [ICRS] guidelines) and identify any procedures perform in conjunction with MPFL reconstruction. 3 Patients were excluded from the study if they underwent a concomitant bony procedure (tibial tubercle osteotomy, femoral osteotomy, or trochleoplasty), fixation of osteochondral fracture, or a cartilage restoration procedure.
Surgical Indications and Technique
During the study period at this academic medical center, patients presenting with recurrent patellar instability were recommended to undergo treatment with MPFL reconstruction with or without associated bony procedures. The decision to include such procedures was a joint surgeon-patient decision. Bony procedures were generally considered in the setting of a large J-sign with severe trochlear dysplasia (Dejour B, C, D), patella alta with a CDI in excess of 1.30, or a TT-TG distance >20 mm. Patients who underwent concurrent bony procedures were excluded from this study. All procedures were performed by 1 of 4 orthopaedic surgeons who had completed sports medicine fellowship training (R.A.M., R.A.D., D.C.F., B.D.M.) .
In each case, diagnostic arthroscopy was performed and intra-articular pathology was treated. MPFL reconstruction was undertaken with the goal of anatomic placement of an MPFL graft with no tension. Patellar-sided suture anchor fixation was performed on the superior half of the medial patella. Femoral tunnel position was identified with radiographic (Schöttle 27 point) and/or anatomic (the saddle between the adductor tubercle and medial epicondyle) landmarks and relative isometry was confirmed. Graft fixation of the femoral side was achieved with an interference screw. The selected graft type varied over time and by surgeon during the study period. Grafts utilized included allografts (hamstring tendons, peroneus longus tendons, and tibialis anterior tendons) and autografts (hamstring tendons).
All patients were referred to physical therapy postoperatively and recommended to begin therapy within 1 week of surgery. The recommended protocol included immediate full range of motion as tolerated without restriction along with core, hip, quadriceps, and hamstring strengthening. Postoperative weightbearing restrictions and brace use varied over the study period due to changes in practice and by surgeon.
Follow-up and Data Collection
Retrospective chart review was undertaken to identify episodes of recurrent patellar dislocation. Patients were subsequently contacted via mail and/or telephone to ask whether they had a subsequent patellar dislocation event and obtain PROs. Patients were contacted between 2016 and 2021 by medical students and/or attending physicians to collect PROs. PROs included the Norwich Patellar Instability score, 28 Knee injury and Osteoarthritis Outcome Score (KOOS),22,23 and Marx activity level. 15 Patients with a minimum of 12 months of follow-up were included in the evaluation of recurrent dislocation risk and those who completed PROs were included in the final analysis of the effect of number of previous dislocations on PROs after MPFL reconstruction.
A total of 200 patients underwent MPFL reconstruction during the study period. After exclusion of those who underwent tibial tubercle osteotomy (n = 36) or fixation of an osteochondral fracture (n = 4), 160 patients were eligible for inclusion in the study. No meniscal repairs or concomitant ligament procedures were performed in this population. A total of 122 patients (76%) had data on subsequent dislocations from either chart review or subsequent patient contact at a minimum of 1 year postoperatively (range, 1.2-12.6 years); 95 patients completed PRO measures (Figure 1).
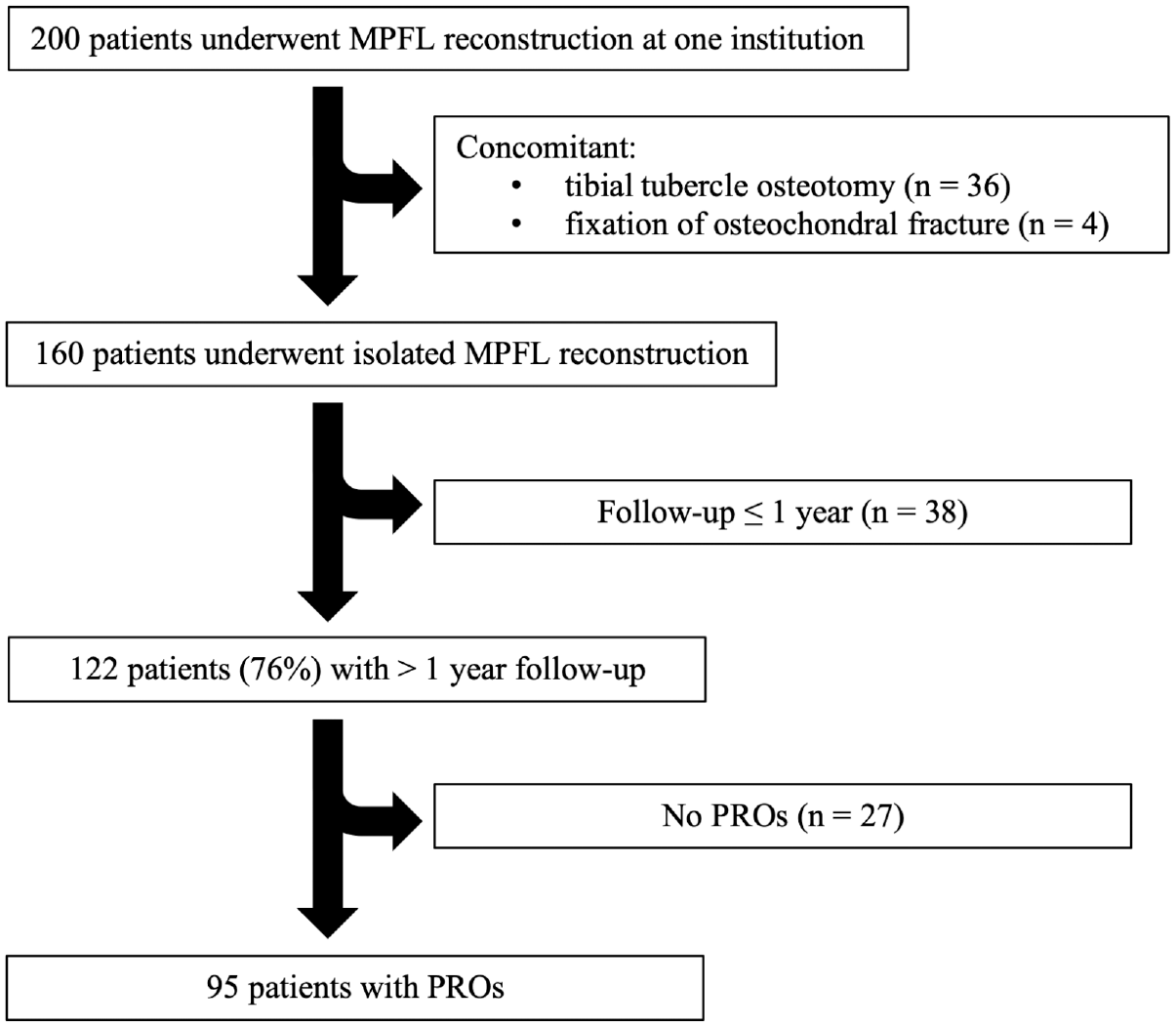
Flowchart of patient selection criteria. MPFL, medial patellofemoral ligament; PRO, patient-reported outcome.
Statistical Analysis
Summary statistics including proportions for categorical variables and means and standard deviations or medians and interquartile ranges (IQRs) for continuous variables were calculated depending on or normality of continuous variables as assessed with Shapiro-Wilk tests. Group comparisons based on the number of patellar dislocations in the index knee before surgery (≤2 vs >2) were performed with t tests, Mann-Whitney U tests, and Fisher exact tests as appropriate. The impact of the number of previous patellar dislocations in the index knee on postoperative PROs was analyzed using multiple linear regression models, adjusting for patient age, sex, BMI, CDI, TT-TG distance, sulcus angle, and articular cartilage status at surgery (the presence of ICRS grade 3 or 4 damage). P < .05 was defined as statistically significant. To minimize risk of selection bias, comparisons of baseline data were performed between those patients who completed PROs and those who did not. A power analysis demonstrated that a minimum of 37 patients per group were required to detect a clinically relevant 10-point difference in KOOS subscales with an expected standard deviation of 15 points with 80% power and alpha set to .05. 32
Results
Medical record review revealed 160 patients who underwent isolated MPFL reconstruction (71 with ≤2 dislocations and 89 with >2 dislocations. The 122-patient study group included 50 patients with ≤2 preoperative patellar dislocations in the index knee and 72 patients with >2 preoperative patellar dislocations. One postoperative patellar dislocation (2.0%) was noted in the ≤2 dislocations group and 4 postoperative dislocations (5.6%) were noted in the >2 dislocations group (P = .41) at a median follow-up of 4.6 years (IQR, 3.2-6.0 years; range, 1.0-12.6 years).
In the subset of 95 patients who completed PROs, there were 32 males (34%) and 63 females (66%), with a mean age of 25.3 ± 9.7 years and a mean BMI of 26.7 ± 5.9 kg/m2. The mean CDI was 1.13 ± 0.17, the mean sulcus angle was 144.2°± 9.2°, and the mean TT-TG distance was 17.0 ± 4.9 mm. Patellofemoral articular cartilage damage of ICRS grade 0, 1, or 2 was noted in 45 patients (47%) and grade 3 or 4 in 50 patients (53%). Median follow-up was 4.8 years (IQR, 4.0-6.5 years; range, 1.2-12.6 years). Patients with ≤2 patellar dislocations were younger (20.7 ± 7.3 years) than those with >2 patellar dislocations (28.5 ± 10.0 years) (P < .001), but no other significant differences were noted between the 2 groups (Table 1).
Patient Demographics and History a

Data are presented as n (%) unless otherwise indicated. Bold value indicates significance at P < .05. BMI, body mass index; ICRS, International Cartilage Repair Society; IQR, interquartile range; TT-TG, tibial tubercle-trochlear groove.
Significant differences were noted between the ≤2 and >2 dislocations groups for all KOOS subscales: Symptoms, P = .007; Pain, P < .001; Activities of Daily Living, P = .011; Sports and Recreation, P < .001; and Knee-Related Quality of Life, P = .004; the Norwich Patellar Instability score, P = .022; and the Marx activity score: P = .021 (Table 2). Adjusting for age, sex, BMI, CDI, TT-TG distance, sulcus angle, and cartilage status, patients with >2 dislocations had lower KOOS Pain (P = .003), Activities of Daily Living (P = .025), Sports and Recreation (P = .009), and Knee-Related Quality of Life (P = .008) subscales compared with those with ≤2 dislocations (Table 3).
PROs by Number of Dislocations a

Bold values indicate significance at P < .05. ADL, Activities of Daily Living; KOOS, Knee injury and Osteoarthritis Outcome Score; NPI, Norwich Patellar Instability; PROs, patient-reported outcomes; QoL, Quality of Life; Sports/Rec, Sports and Recreation.
Linear Regression Coefficients for >2 Versus ≤2 Previous Patellar Dislocations on PROs a

Data adjusted for age, sex, body mass index, Caton-Deschamps index, TT-TG distance, sulcus angle, and cartilage status (n = 95). Bold values indicate significance at P < .05. ADL, Activities of Daily Living; KOOS, Knee injury and Osteoarthritis Outcome Score; NPI, Norwich Patellar Instability; PROs, patient-reported outcomes; QoL, Quality of Life; Sports/Rec, Sports and Recreation; TT-TG, tibial tubercle-trochlear groove.
Discussion
The most important finding of this study is that patients who sustained ≤2 patellar dislocations reported significantly better outcomes after MPFL reconstruction compared with patients with >2 patellar dislocations in this study population. This novel finding will allow surgeons to better counsel patients regarding expected outcomes after isolated MPFL reconstruction and has the potential to guide treatment decisions in this population as well as future research. The poorer PROs in those who have sustained >2 patellar dislocations make this population ideal to study the effects of additional bony procedures on outcomes. It remains unknown whether the addition of a bony procedure in this patient population would improve PROs or reduce recurrent instability risk.
The reasons behind poorer PROs in this population are not yet known. One could hypothesize that outcomes could be driven by additional intra-articular injury (such as articular cartilage damage), preexisting differences in patient or anatomic factors, or more damage leading to less functional existing medial restraints.
Articular cartilage damage is known to be relatively common in the setting or recurrent patellar instability,19,33 with some authors demonstrating increased damage with increasing number of patellar dislocations. 11 Articular cartilage damage has been shown to adversely affect outcomes after patellar dislocation.8,10 In this study, no significant differences in articular cartilage damage were noted in the ≤2 dislocations group when compared with the >2 dislocations group, and the difference in outcomes based on number of dislocations persisted when adjusting for cartilage status. Increased articular cartilage damage does not appear to be a major driver of the poorer outcomes in the multiple dislocation group in this study.
Certain anatomic factors including trochlear dysplasia, patella alta, and elevated TT-TG distance are known to contribute to risk of patellar instability 9 and have been hypothesized by multiple authors to impact outcomes after isolated MPFL reconstruction.13,20 One might expect more severe anatomic abnormalities in the >2 previous dislocations group; however, no significant differences in anatomic factors were noted between the 2 groups in this study and differences in outcomes between the groups persisted when adjusting for these factors. The only patient demographic factor that was noted to differ between the groups was patient age, with the >2 dislocations group demonstrating an increased mean age at the time of surgery. This factor could be important as previous work has shown that increased age is associated with poorer outcomes after MPFL reconstruction. 12 Importantly, the differences in outcomes between dislocation groups persisted when adjusting for age.
Progressive damage to medial structures with multiple dislocation events may be one factor driving poorer outcomes in the >2 dislocations group. The occurrence of multiple patellar dislocations would be expected to result in increased damage and stretching of medial restraints to patellar dislocation, 18 as evidenced by the increased ease of dislocations with time and lower degree of symptoms with recurrent dislocations versus first-time events. While the MPFL is the major soft tissue restraint to lateral patellar dislocation, it is not the only important structure. 30 Reconstruction of the MPFL alone in patients in whom other structures are more stretched and less functional could contribute to poorer outcomes. More work is necessary in this area to clearly elucidate the contribution of medial soft tissue laxity to outcomes of MPFL reconstruction.
Limitations
The current study has several limitations. It is a retrospective cohort study and bias may have been introduced due to loss of some patients to follow-up or due to the study population not being an accurate representation of the general population. It is important to recognize that there may be additional, unknown differences between the 2 groups of patients compared in this study. It would not be accurate to conclude from this work that earlier intervention in the group with >2 dislocations would have resulted in better outcomes. More work is needed to evaluate this important question. Further, the minimum follow-up of 1 year and median follow-up of nearly 5 years is still relatively short. There is also heterogeneity in the overall length of follow-up. Longer follow-up is needed to determine potential influences of the number of previous dislocations on long-term risk of osteoarthritis or deterioration of outcomes.
Conclusion
Patients who have had >2 patellar dislocations before MPFL reconstruction demonstrated poorer PROs at a median of 4.8 years postoperation when compared with those who have had ≤2 dislocations before surgery, adjusting for age, sex, BMI, and patellofemoral anatomy.
Footnotes
Final revision submitted February 1, 2024; accepted March 1, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.D.M. has received education payments from CDC Medical, Smith+Nephew, and United Orthopedics; hospitality payments from Medical Device Business services; and a grant from Arthrex. A.C.D. has received education payments from Smith+Nephew and CDC Medical. R.A.D. has received hospitality payments from Arthrex, Stryker, and Smith+Nephew; education payments from Elite Orthopedics, ImpactOrtho, CDC Medical, and Arthrex; and a grant from Arthrex. D.C.F. has received consulting fees from DePuy Synthes, Linvatec, Medical Device Business Services, Smith+Nephew, Vericel, Bioventus, Zimmer Biomet Holdings, and Ceterix Orthopaedics; nonconsulting fees from Smith+Nephew, Vericel, Karl Storz Endoscopy, Linvatec, Pacira Pharmaceuticals, and Trice Medical; and honoraria from Vericel. R.A.M. has received a grant from DJO and education payments from CDC Medical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from The Ohio State University (ref No. 2015H0446).