
Abstract
Background:
The management of irreparable rotator cuff tears presents a surgical dilemma. However, supraspinatus muscle advancement (MA) could be used to convert irreparable to reparable tears without requiring a graft.
Purpose:
To compare the outcomes of patients with an irreparable tear who underwent rotator cuff repair with MA with those with a reparable large to massive cuff tear who underwent rotator cuff repair.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We enrolled 62 patients who underwent rotator cuff repair for a large to massive tear between January 2020 and May 2022. Among them, 29 patients underwent an MA procedure due to an inability to repair despite releases (MA group), whereas the other 33 patients did not require the procedure (NMA group). At 1 year postoperatively, follow-up assessments including magnetic resonance imaging were performed to evaluate group outcomes.
Results:
Despite there being more revision surgery cases and a poorer potential for cuff healing in the MA group, the retear rates in the MA and NMA groups were similar (31.0% vs 21.2%, respectively; P = .401), as were clinical outcomes, including the visual analog scale for pain (2.9 vs 1.9; P = .076), University of California, Los Angeles (27.0 vs 29.1; P = .185), Constant (70.1 vs 74.9; P = .063), and American Shoulder and Elbow Surgeons (74.5 vs 81.8; P = .168) scores. Postoperative muscle power during forward elevation was weaker in the MA group than in the NMA group (35.1 vs 45.8 N; P = .052), but external rotation power was comparable (49.3 vs 59.0 N; P = .121). Progress in fatty degeneration of the supraspinatus was not significantly different in the 2 groups (P = .43), although the MA group showed a nonsignificant decrease in supraspinatus atrophy (P = .092) due to the lateral shift produced by the procedure.
Conclusion:
The MA procedure for irreparable tears produced outcomes comparable with reparable tears, offering a valuable perspective on the efficiency of the procedure. The comparable but relatively high retear rates emphasize the need for further studies to compare with other treatment options for irreparable tears.
Irreparable rotator cuff tears (RCTs) are challenging and affect shoulder function and quality of life. The optimal treatment for these tears remains controversial, as conventional techniques, such as partial repair, have high failure rates.3,32 Therefore, in recent years, several alternative surgical options have been proposed and investigated with the aim of restoring shoulder joint biomechanics and stability. These options include superior capsular reconstruction with an autograft or allograft, repair with patch augmentation and interpositional grafting, tendon transfer from adjacent muscles, and subacromial balloon spacer implantation.1,18,24,25,34,36,41,42 However, evidence supporting the efficacy and safety of these techniques is limited and inconsistent, and procedure selection criteria and indications are not wellestablished. 4 Moreover, these techniques increase medical costs due to the costs of allograft or special implant requirements. Furthermore, reverse total shoulder arthroplasty, which is considered the final option for irreparable RCT, has its own drawbacks and complications, including infection, instability, scapular notching, and implant loosening.14,15,21 Given the lack of long-term durability of this procedure, reverse total shoulder arthroplasty is generally used only in older patients.
Supraspinatus muscle advancement (MA) is a potential option for the salvage of irreparable RCTs. First introduced by Debeyre et al, 10 this technique, which does not require a graft, involves lateral shifting of the supraspinatus tendon and has been modified and applied to arthroscopic rotator cuff repair.23,38 MA for arthroscopic rotator cuff repair has been reported to improve shoulder function and provide pain relief at short-term follow-up. 45 However, few reports have been issued on the postoperative outcomes of MA.
This study was performed to compare the clinical and radiological outcomes of irreparable RCTs treated by MA and those of reparable RCTs of similar severity. We hypothesized that repair with MA would provide outcomes comparable with primary repair of large and massive tears in terms of shoulder function, pain, satisfaction, repair integrity, and muscle quality.
Methods
Study Design and Patient Selection
This retrospective study was performed after obtaining approval for the study protocol from our institutional review board. An arthroscopic-assisted modified MA technique was first attempted in 2010 at our institution but implemented in earnest in 2018 after modification to reduce the learning curve. Before surgery, we assessed the patient's condition through physical examination and imaging to determine his or her suitability for the MA procedure. We specifically looked for cases where the retraction of the torn cuff extended medial to the glenoid and the fatty degeneration was graded ≥2 as seen in the conventional Y-view T1-weighted sagittal magnetic resonance imaging (MRI) scans. If these criteria were met, we prepared for MA treatment. During the surgery, we first attempted to repair the rotator cuff conventionally, after comprehensive releases of the cuff, including the coracohumeral ligament. If reduction to the footprint was achievable, we proceeded with the conventional repair. However, if this was not possible, we then indicated and proceeded with MA.
This study was performed on patients treated between January 2020 and May 2022 with a large to massive RCT who underwent arthroscopic rotator cuff repair (primary or revision surgery). The inclusion criteria were (1) a large to massive RCT (tear involving entire supraspinatus and more than half of the infraspinatus), the size of which was confirmed by both MRI and arthroscopy, and (2) the availabilities of 1-year postoperative MRI for the evaluation of tendon and cuff muscle statuses and functional assessment results.7,17 The exclusion criteria were (1) a procedure other than MA of the supraspinatus, (2) an isolated tear of the subscapularis or infraspinatus, (3) a history of shoulder surgery other than rotator cuff repair, and (4) incomplete follow-up data. Pre- and postoperative clinical and imaging data were retrospectively reviewed.
Preoperative Data Collection
Preoperative demographic and clinical data were collected. Various scoring systems were used to assess patient conditions, including the visual analog scale (VAS) for pain, as well as the University of California, Los Angeles (UCLA), Constant, and American Shoulder and Elbow Surgeons (ASES) shoulder function scores.8,13,35 Muscle powers for forward elevation (specifically, 90° flexion scaption), external rotation, and internal rotation in the side position were assessed pre- and postoperatively using a handheld dynamometer (FGN-100; Nidec-Shimpo).
Preoperative imaging data were also obtained through shoulder MRI scans. Anteroposterior tear sizes were measured, and the amount of tendon involvement was assessed. Tear retractions were evaluated using the Patte classification. 40 Fatty degeneration was assessed using the Goutallier classification 19 as modified by Fuchs et al. 16 Muscle atrophy was evaluated using the percentage of rotator cuff muscles affected and was graded into 3 categories: grade 1, ≥60%; grade 2, 30% to 59%; or grade 3, <30%. 30 All imaging evaluations were based on the standard radiologic reporting protocol of our institution. This routine reporting process was conducted through the consensus of 2 or 3 board-certified musculoskeletal radiologists who were not involved in our study and did not contribute to its authorship.
Surgical Procedure and Intraoperative Data Collection
Surgery was performed by a single surgeon (S.H.K.). With a patient in the lateral decubitus position, a drape was extended more proximally to include the medial border of the scapula. Diagnostic arthroscopy was performed to confirm the presence of a large to massive RCT, assess tendon status, and determine tear shape. Glenoid and humeral cartilage conditions were evaluated using the Outerbridge classification, and infraspinatus involvement was noted. 39 Acromioplasty was performed selectively, especially for a lateral subacromial spur. The biceps rerouting technique, referred to as biceps splinting for the purpose of better cuff healing, was performed when the long head of biceps tendon was available for rerouting. 27 Torn cuff tendon reparability was checked after thoroughly releasing the supraspinatus muscle (bursal, articular, and coracohumeral). Reparable tears were repaired using a routine single-row technique.
MA was performed in patients with irreparable torn cuff tendons. The procedure was initiated by arthroscopically releasing the transverse scapular ligament to free the suprascapular nerve for extensive supraspinatus reduction (Figure 1A). A horizontal skin incision was made parallel to the scapular spine near the medial scapular border (Figure 1B), and the superior trapezial insertion was then detached from the scapular spine. The supraspinatus was elevated from the suprascapular fossa, and the medial origin of the supraspinatus muscle was palpated and carefully released; a Cobb elevator was used for the proximal portion (Figure 1C), and blunt finger dissection was performed for the distal portion near the suprascapular nerve (Figure 1D).23,45

The procedure used for right shoulder supraspinatus muscle advancement. (A) The transverse scapular ligament (white arrow) is released to free the suprascapular nerve (yellow arrowheads). (B) After completing horizontal incision and dissection, the medial origin of the supraspinatus muscle is released (C) using a Cobb elevator for the proximal portion and (D) a blunt finger for the distal portion.
With the MA procedure, mobility was restored for reduction to the anatomic footprint in all of the patients with irreparable tear (Figure 2). The tear was then repaired using a single-row technique, as was performed for reparable tears.

SST mobility on a right shoulder restored with MA. (A) Before MA, SST traction was limited to the glenoid level. (B) After MA, SST reduction was possible to the anatomic footprint (asterisk). SST, supraspinatus; MA, muscle advancement; LHBT, long head of biceps tendon.
Postoperative Rehabilitation
The same rehabilitation protocol was used for patients who underwent MA (MA group) and those with no MA (NMA group). Immobilization was maintained with a sling and abduction pillow for 5 weeks in all 62 cases. After weaning from a brace, patients were instructed how to conduct passive assisted stretching exercises (forward elevation, external rotation, and internal rotation). Return to sports was not allowed until ~5 months after surgery.
Postoperative Data Collection
On 1-year postoperative MRI, retear of a repaired tendon was defined as discontinuity at the footprint (Sugaya grades 4 and 5). 43 Fatty degeneration and muscle atrophy were compared with those on preoperative MRI. Postoperative changes of supraspinatus origins were assessed using extended T1-weighted sagittal images. Similar to the preoperative assessment, our postoperative imaging evaluations adhered to the standard radiologic reporting protocol of our institution.
Postoperative clinical outcomes were assessed 1 year after surgery using VAS pain, UCLA, Constant, and ASES scores. Muscle power was also evaluated for forward elevation, external rotation, and internal rotation. Pre- and postoperative data were compared to determine changes in pain, function, and strength after rotator cuff repair, for patients in both the MA and the NMA groups.
Statistical Analysis
The statistical analyses were performed using R package Version 4.3.1 (R Foundation for Statistical Computing), and data normality was tested using the Shapiro-Wilk test. Demographic, preoperative, and intraoperative data of the MA and NMA groups were compared using the t test or the Mann-Whitney test, and postoperative changes in the 2 groups were compared using the paired t test or Wilcoxon test, depending on normality. The chi-square or Fisher exact test was used to compare categorical variables. Statistical significance was accepted for P values <.05.
Results
Patient Demographics
Of 133 eligible patients, 62 patients were ultimately included in the study: 29 in the MA group and 33 in the NMA group (Figure 3). The patient characteristics were comparable between the groups, with no significant difference in sex, age, body mass index, underlying diabetes mellitus, or smoking history (Table 1). Notably, 14 of 62 patients (22.6%) underwent revision rotator cuff repair, 10 patients in the MA group (34.5%) and 4 patients in the NMA group (12.1%). The rate of revisional repair tended to be higher in the MA group but did not reach statistical significance (P = .066).
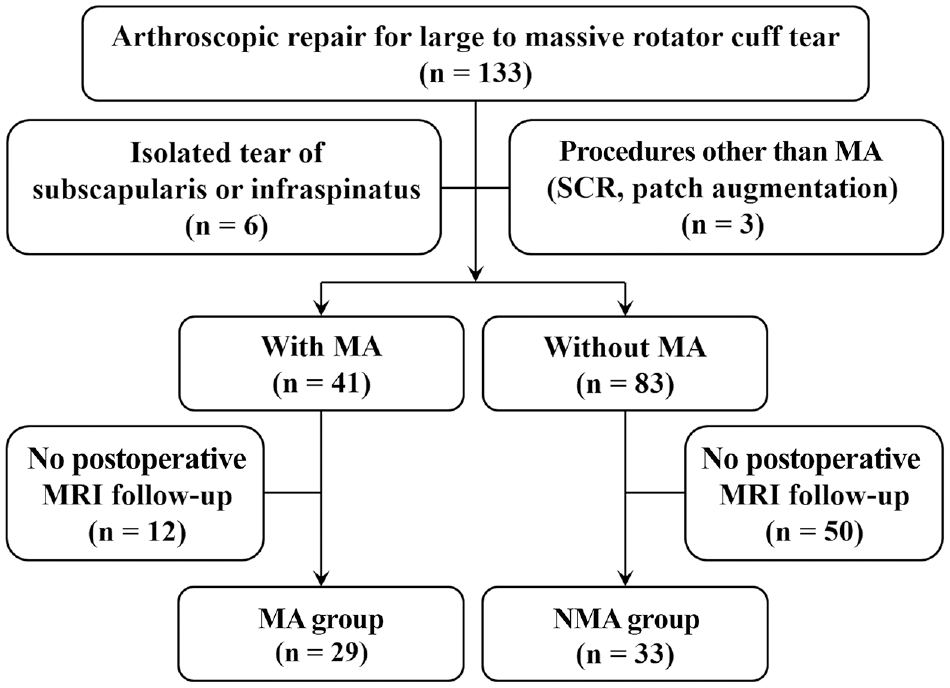
Flowchart of patient enrollment. MA, muscle advancement; MRI, magnetic resonance imaging; NMA, no muscle advancement; SCR, superior capsular reconstruction.
Patient Characteristics a

Data are presented as mean ± SD or mean (range) unless otherwise indicated. BMI, body mass index; DM, diabetes mellitus; MA, muscle advancement; NMA, no muscle advancement.
Preoperative Clinical and Imaging Data
No significant intergroup differences were observed regarding preoperative muscle power in forward elevation, external rotation, or internal rotation, and functional scores were also comparable in the MA and NMA groups (Table 2). Preoperative MRI results are presented in Table 3. Anteroposterior tear size and retraction were significantly greater in the MA group (P = .017 and P < .001, respectively). Fatty degeneration was similar in the 2 groups, but atrophy of the supraspinatus and infraspinatus muscles was more severe in the MA group (P < .001 and P = .014, respectively).
Preoperative Muscle Powers and Clinical Scores a

Data are presented as mean ± SD. ASES, American Shoulder and Elbow Surgeons; ER, external rotation; FE, forward elevation; IR, internal rotation; MA, muscle advancement; NMA, no muscle advancement; UCLA, University of California, Los Angeles; VAS, visual analog scale.
Preoperative MRI Findings a

Data are presented as mean ± SD unless otherwise indicated. Boldface P values indicate statistically significant difference between groups (P < .05). MA, muscle advancement; MRI, magnetic resonance imaging; NMA, no muscle advancement.
Graded as described by Patte. 40
Calculated as described by Goutallier et al. 20
Graded based on atrophy percentages: grade 1, >60%; grade 2, 30-60%; grade 3, <30%.
Intraoperative Findings and Procedures
The comparison of intraoperative findings and procedures between groups is detailed in Table 4. There was a higher incidence of severe chondral lesions of the humeral head in the MA group (P = .020) as well as significantly poorer tendon quality (P = .025). Additionally, the patterns of RCTs varied between the groups, with U- and V-shaped tears being more prevalent in the MA group (P < .001). Furthermore, tears of the infraspinatus were more commonly observed in the MA group (P = .042). Regarding intraoperative procedures, the notable distinction was the lower frequency of acromioplasty performed in the MA group (P = .049), which could be attributable to the higher number of revision cases in that group.
Intraoperative Findings and Procedures a

Boldface P values indicate statistically significant difference between groups (P < .05). IST, infraspinatus; L, L-shape; reverse-L; reverse L-shape; MA, muscle advancement; NMA, no muscle advancement; U, U-shape; V, V-shape.
Graded as described by Outerbridge and Dunlop. 39
Classified as described by Millstein and Snyder. 37
Rerouting technique as described by Kim et al. 27
Retear Rate
The retear rates were not significantly different between the MA and NMA groups overall or when comparing the primary surgery cases; however, when comparing the revision surgery cases, the retear rate was higher in the MA versus the NMA group (40.0% vs 25.0%) (Table 5). No other complications were reported in either group during the 1-year follow-up.
Retear Rates a

Data are presented as n unless otherwise indicated. MA, muscle advancement; NMA, no muscle advancement.
Postoperative Clinical Outcomes
Postoperative clinical scores and muscle powers were also compared (Table 6). When comparing postoperative muscle power, results showed no significant differences between the groups, but there was a trend toward lower postoperative forward elevation power in the MA group (P = .052). Regarding clinical scores, the postoperative VAS pain scores were not significantly different between the groups, but the NMA group saw significantly more pre- to postoperative improvement (P = .036).
Postoperative Muscle Power and Clinical Scores a

Data are presented as mean ± SD. Boldface P value indicates statistically significant difference between groups (P < .05). ASES, American Shoulder and Elbow Surgeons; ER, external rotation; FE, forward elevation; MA, muscle advancement; NMA, no muscle advancement; UCLA, University of California, Los Angeles; VAS, visual analog scale.
Comparison of postoperative data between the MA and NMA groups
Paired comparison of preoperative and postoperative data between the MA and NMA groups.
Other Postoperative Imaging Outcomes
We also examined pre- to postoperative changes in fatty degeneration and supraspinatus muscle atrophy. Fatty degeneration of 8 (27.6%) patients in the MA group and 5 (15.2%) patients in the NMA group worsened similarly after surgery (P = .430) (Table 7). A subgroup analysis of healed patients also showed no significant group differences regarding changes in fatty degeneration (P = .565). Regarding changes in supraspinatus muscle atrophy, although analysis showed no significant group differences, the MA group showed a tendency toward muscle atrophy recovery after surgery, while the NMA group showed a worsening tendency (P = .092) (Table 7). In the subgroup analysis of healed patients, a higher though nonsignificant rate of muscle atrophy recovery was observed in the MA group (38.1% [8/21] vs 11.1% [3/27]; P = .065).
Comparison of Postoperative Changes in Fatty Degeneration and Muscle Atrophy a

Data are presented as % (n). MA, muscle advancement; NMA, no muscle advancement.
In addition to the trend of increased muscle volume in scapular Y-view sagittal MRI, assessments also showed a postoperative change in muscle origin with extended T1-weighted sagittal images (Figures 4 and 5). The mean of ~2.1 cm of medial aspect (7 slices with 3-mm slice thickness from the most lateral junction of the scapular spine with the scapular body) demonstrated an absence of the muscle at the suprascapular fossa.
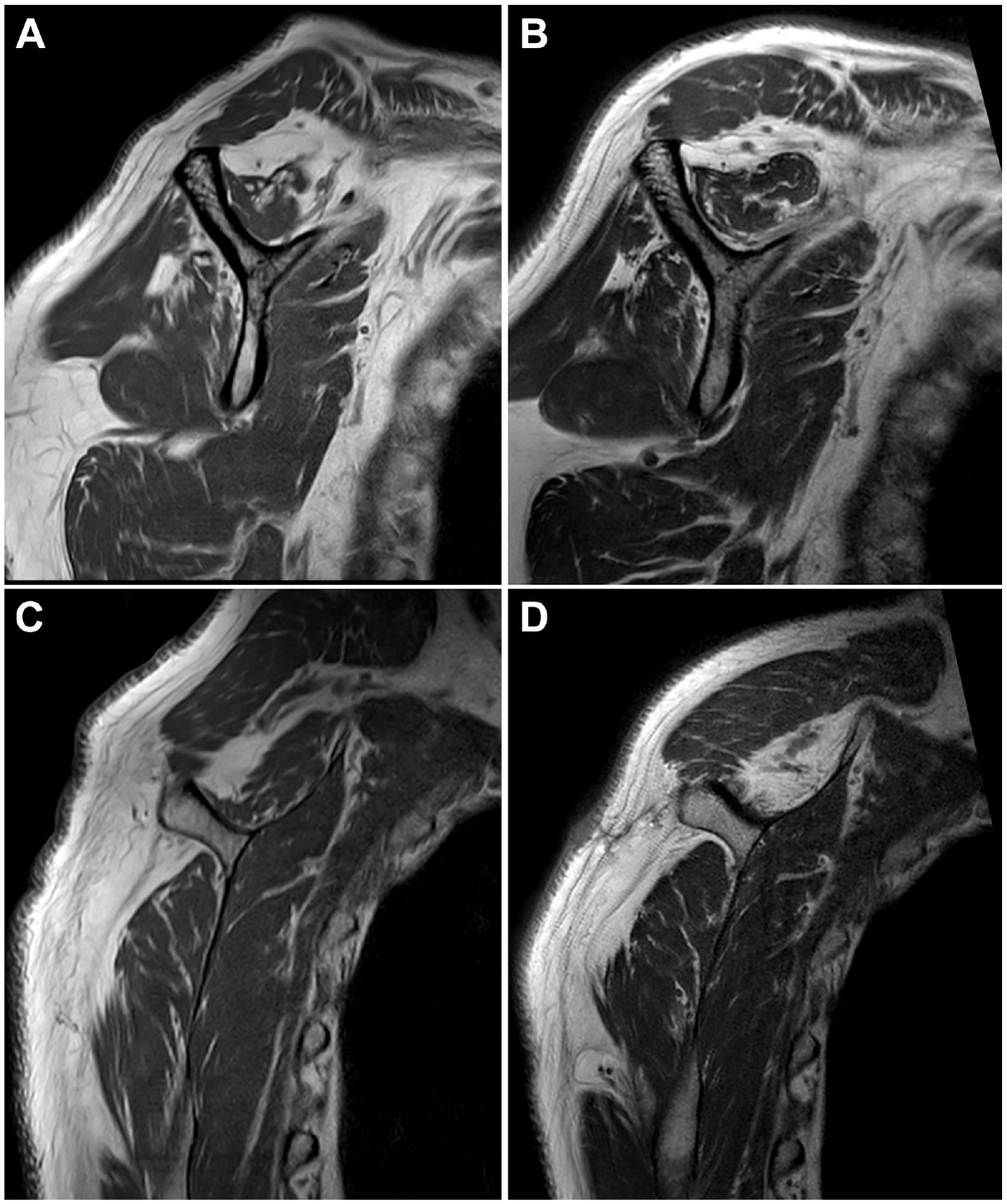
Repair with muscle advancement in a 69-year-old male patient as shown on T1-weighted sagittal magnetic resonance imaging. Compared with the (A) preoperative Y-view image, the (B) postoperative image shows the same degree of fatty degeneration but an increase in supraspinatus (SST) volume. When comparing with the more medial section (C) preoperative image, the (D) postoperative image shows a reduction in SST volume.

Repair without muscle advancement in a 65-year-old female patient as shown on T1-weighted sagittal magnetic resonance imaging. Compared with the (A) preoperative Y-view image, the (B) postoperative image shows the same degree of fatty degeneration and the same supraspinatus (SST) volume. When compared with the more medial section (C) preoperative image, the (D) postoperative image showed no change in SST volume.
Discussion
The main findings of this study were that clinical and radiological outcomes of patients with an irreparable tear who underwent MA advancement were comparable with those of patients with a reparable large to massive RCT. Although the MA group had a higher proportion of revision surgeries and more serious tears, retear rates, functional scores, muscle powers, fatty degeneration, and muscle atrophy were comparable in the 2 study groups. These results suggest that MA is a viable option for treating irreparable RCTs.
Our findings revealed comparable functional outcomes between the MA group and NMA group, despite a relatively high retear rate and modest improvement in outcome scores in both groups. Notably, the postoperative VAS pain score did not show a significant difference between groups, but improvement was significantly greater in the NMA group. While the UCLA and Constant scores achieved the minimal clinically important difference and postoperative scores reached the indicated Patient Acceptable Symptom State, the VAS pain score and ASES score did not reach these thresholds.26,28 Our analysis suggests that ASES outcomes may be influenced by factors such as VAS pain scores and tear size, potentially affecting the achievement of clinically significant improvements. Further studies are warranted to explore the complex nature of the VAS pain score and its various contributing factors, providing a more comprehensive understanding of its role in postoperative assessments.
In terms of radiologic changes, we observed no significant difference between the groups in the worsening of fatty degeneration in the supraspinatus or infraspinatus muscles. This lack of disparity indirectly suggests that suprascapular nerve damage or dysfunction does not occur after the muscle advancement procedure. However, we observed a slight improvement in supraspinatus atrophy within the MA group. This could potentially be attributed to a more pronounced lateral shift resulting from the muscle advancement procedure, as compared with the NMA group. 46 Such an effect may indicate the impact of the MA technique on muscle morphology, suggesting the importance of 3-dimensional volumetric assessment rather than 2-dimensional cross-sectional assessment for reliable evaluation of cuff muscles.6,44 As shown in the result, extended T1-weighted sagittal images showed a shift in supraspinatus origin at the medial aspect of the suprascapular fossa. Considering a mean length of 9.2 cm from the medial scapular border to the most lateral part of the base of the scapular spine and an error summation of 1 cm, the estimated effect of lateral shifting would be ~6 cm. 22 Nevertheless, we were unable to conclusively determine whether suprascapular nerve irritation contributed to the higher postoperative VAS scores in the MA group. While the difference in pain VAS scores between the groups was not statistically significant, the decrease in pain VAS was less pronounced in the MA group compared with the NMA group (pre- and postoperative pain VAS: from 3.8 ± 2.2 to 2.9 ± 2.3 in the MA group, and from 4.1 ± 2.3 to 1.9 ± 1.8 in the NMA group). Moreover, we observed nonsignificant differences in postoperative external rotation power improvements between the MA and NMA groups, implying a low potential of suprascapular nerve injury.
Various alternative procedures, such as partial repair, superior capsular reconstruction, patch augmentation, interposition grafting, and subacromial balloon spacer implantation, are considered when addressing irreparable RCTs. Superior capsular reconstruction is a notable treatment option, with reports of significant benefits for patients, but its implementation has been associated with certain limitations. For example, allograft utilization is hampered by cost concerns and a high failure rate, while autografts introduce the issue of donor-site morbidity.11,29,33 In addition, superior capsular reconstruction may act as a valuable static restraint or spacer rather than a dynamic stabilizer and fail to restore active external rotation. 9 MA provides another treatment approach, which potentially reduces tensile forces and fulfills a pivotal role as a dynamic stabilizer. Importantly, in the present study, MA was associated with minimizing the progression of fatty degeneration, which suggested that suprascapular nerve injury might not be a significant concern in MA. Additional research is required to assess and compare the efficacy of different procedures proposed for treating irreparable RCTs.
Previous studies that investigated MA procedures have consistently described promising results for irreparable RCTs. Early research conducted by Debeyre et al 10 on 44 patients who underwent MA for open cuff repair indicated favorable functional outcomes characterized by an increase in abduction range and pain alleviation. More recently, Morihara et al 38 reported a retear rate of 23% (8 of 34 patients) for arthroscopic rotator cuff repair with MA. Yokoya et al 45 performed a comparative study on 26 RCT cases that underwent MA and 21 control RCT cases and demonstrated a lower failure rate in the MA group (23.1% vs 52.4%; P = .03). Likewise, the current study also supports similar radiographic and functional outcomes in these patient groups. While our study indicates a slightly higher retear rate, it's important to note that previous research focused on potentially repairable tears matching the tear size.
Limitations
This study has some limitations that should be acknowledged. First, the control group was composed of patients with reparable RCTs. Further studies are needed to compare the outcomes, including long-term morbidities and the cost-effectiveness of different procedures for irreparable tears.5,29,31 Nevertheless, this study shows that patients with an irreparable tear and a higher rate of revision surgery achieved outcomes comparable with those achieved by patients in the reparable group. Second, while our findings suggest that MA and NMA groups had similar outcomes, despite the MA group's having more severe preoperative conditions, it is important to note that these conclusions are limited by the small sample sizes of each group. The statistical power is low in comparison of retear rate, which was the primary outcome of our study (power = .112), suggesting that our study may not effectively detect significant differences in retear rates, potentially underestimating true effects. The prevalence of irreparable RCTs is relatively low, even in tertiary hospitals, which necessitates a longer duration to accumulate a sufficient sample size for study. Consequently, our study requires further research with a larger sample size to draw more definitive conclusions. Third, follow-up losses and short follow-up period for adequate assessment of the outcomes. Twelve patients in the MA group and 50 patients in the NMA group were excluded due to the nonavailability of postoperative MRI and results of the 12-month postoperative evaluation. Although patients were recommended to undergo routine MRI 1 year postoperatively, many patients were reluctant to bear the cost of an MRI evaluation after symptoms had subsided. We are uncertain whether this introduced selection bias, but a follow-up loss of ~40% at 1 year is typical at our institution. Additionally, 1 year might be too brief to capture the complete range of recovery and long-term effects. Last, suprascapular nerve status was not evaluated postoperatively, especially in the MA group. Since MA involves considerable lateral shifting of retracted cuff muscle, it introduces the risk of suprascapular nerve damage. However, we did not observe any neurologic sign of muscular condition change in the cohort and considered a routine electrophysiologic study unethical after evaluating cuff status.
Conclusion
This study gave insight into the application of MA for irreparable RCTs and showed that MA can achieve comparable outcomes by restoring reparability in patients with large to massive RCTs. The comparable but relatively high retear rate, however, necessitates long-term follow-up and comparisons with other procedures to confirm the effectiveness of MA.
Footnotes
Final revision submitted February 8, 2024; accepted February 13, 2024.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Seoul National University College of Medicine and Seoul National University Hospital (ref No. H-2306-102-1438).