
Abstract
Background:
Despite the effectiveness of reverse total shoulder arthroplasty (RSA) and arthroscopic rotator cuff repair (ARCR) for treating massive rotator cuff tears (MRCTs), controversies remain in patients without glenohumeral osteoarthritis (GHOA).
Purpose:
To compare clinical outcomes of ARCR or RSA in patients with MRCT with high-grade fatty atrophy without GHOA.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This was a retrospective study on patients with MRCTs without GHOA and with grades 3 or 4 Goutallier muscle changes who underwent ARCR or RSA, with a minimum 2-year follow-up. Range of motion (ROM) and patient-reported outcomes (PROs) were collected—including visual analog scale for pain, American Shoulder and Elbow Surgeons score, Veterans Rand 12-Item Health survey, and Subjective Shoulder Value. Postoperative results were compared based on rotator cuff tendon healing in the ARCR group.
Results:
A total of 81 patients met the study criteria—56 underwent ARCR and 25 underwent RSA. Patients in the RSA (age, 71.7 ± 7.7 years) group were older than those in the ARCR (age, 66.7 ± 7.4 years) group (P = .01) and more likely to have pseudoparalysis (52% vs 21.4%; P = .016). The mean follow-up for the ARCR and RSA groups was 56.5 ± 19 months and 36.1 ± 7.6 months, respectively (P < .001). The rate of patients with ≥2 tendons with grade 3 or 4 changes was higher in the RSA group compared with the ARCR group: 96% versus 47% (P < .001). PROs significantly improved after surgery in both groups (P < .05). Postoperative forward flexion (FF) and internal rotation were higher after ARCR compared with RSA—144°± 22° versus 113°± 25° and L3 ± L4 versus S1 ± S2, respectively (P <.001 and P = .002, respectively). Also, 31 of the rotator cuff repairs (55%) healed. PROs were similar between the healed and unhealed ARCR groups, with the only difference observed in postoperative FF—150°± 18° in the healed group versus 136°± 26° in the unhealed group (P = .044).
Conclusion:
Both ARCR and RSA improved functional outcomes in patients with MRCT without GHOA. While healing was moderate after ARCR, the postoperative ROM was greater after ARCR compared with RSA in appropriately selected patients. Moreover, healed rotator cuffs demonstrated improved postoperative FF compared with unhealed repairs.
Keywords
Massive rotator cuff tears (MRCT) are challenging to manage with a multitude of factors that may affect postoperative outcomes. Previous studies have reported reverse total shoulder arthroplasty (RSA) to be a reliable treatment option for MRCTs without glenohumeral osteoarthritis (GHOA), producing consistent improvement in terms of pain relief and restoration of function.19,22 With advances in arthroscopic surgical techniques, arthroscopic rotator cuff repair (ARCR) of MRCTs has also been shown to be a viable treatment option and improve functional outcomes in patients without GHOA.16,30 Although retears after ARCR of MRCT are a concern, outcomes after ARCR have generally exceeded those of RSA.19,21
Retear rates after ARCR of MRCT vary4,13,26 between 25% and 94%. Nonetheless, previous studies have shown functional improvements after ARCR, irrespective of tendon healing.4,13,30 Therefore, there is controversy regarding whether successful healing is associated with better functional outcomes compared with those with retears.6,11,25,34 RSA has been advocated based on the low healing rate of some MRCTs. However, RSA has been reported to have a high complication rate, particularly in younger patients. 2 Thus, decision-making between ARCR and RSA is challenging and requires further investigation.
This study aimed to compare clinical outcomes of ARCR and RSA in patients with MRCT and grades 3 or 4 Goutallier rotator cuff muscle changes without GHOA. Our secondary purpose was to compare function based on the healing status of the rotator cuff after ARCR. We hypothesized that ARCR, regardless of healing status, would lead to superior outcomes compared with RSA. Moreover, we expected that patients with healed rotator cuffs would exhibit better outcomes than unhealed patients.
Methods
Study Design
A retrospective study was performed on prospectively collected data from patients with MRCT without GHOA who underwent a primary ARCR or RSA between January 2015 and December 2018 at a single institution. Patients who underwent ARCR returned for an ultrasound assessment of rotator cuff healing at their latest follow-up. The inclusion criteria were a primary ARCR or RSA for an MRCT with high-grade fatty degeneration of at least 1 rotator cuff muscle—the subscapularis, supraspinatus, or infraspinatus—and a minimum 2-year follow-up. MRCT was defined as a complete 2-tendon tear 14 or a tear >5 cm in 1 dimension on preoperative magnetic resonance imaging (MRI) or on evaluation intraoperatively.3,5 High-grade fatty degeneration was defined as the presence of at least 1 rotator cuff tendon with a Goutallier grade12,15 of 3 or 4. The exclusion criteria included revision procedures, GHOA (Hamada >2), 18 partial repairs, and the use of superior capsular reconstruction to augment a rotator cuff repair construct or tendon transfer. Institutional review board approval was obtained before the study commencement.
Surgical Techniques
Although an individualized approach was always considered, patients with chronic pseudoparalysis (>6 months) and those aiming for overhead strength restoration were usually selected for RSA. Conversely, younger patients with acute pseudoparalysis, primarily seeking pain relief, were usually treated with ARCR.
All procedures were performed by a single high-volume, fellowship-trained shoulder surgeon (P.J.D.). ARCRs were performed with the patient placed in a lateral decubitus position. Diagnostic arthroscopy was performed, and the subscapularis was evaluated and repaired if torn along with a coracoplasty if the coracohumeral interval was <7 mm. The biceps tendon was then evaluated and either a biceps tenodesis or biceps tenotomy was performed unless the tendon was previously torn and completely retracted. A limited acromioplasty with preservation of the coracoacromial ligament was routinely conducted. Intraoperatively, the torn rotator cuff tendons were assessed, and posterosuperior cuff tear size was measured (in cm) in the anteroposterior and mediolateral planes. The retraction stage was also classified according to the Patte classification, with stages 3 and 4 categorized as high retraction stages.12,27 An anterior interval slide was routinely performed for mobilization. Posterior interval slides were added as needed. If at least 75% coverage of the greater tuberosity was possible, a double-row repair was performed. If the repair construct was felt to be under too much tension, then a single-row or single-row with rip-stop repair was performed. Postoperatively, patients were immobilized in a sling for 6 weeks. At 6 weeks, passive forward flexion (FF) and external rotation (ER) were allowed. Active range of motion (ROM) and strengthening began 3 months after surgery. Unrestricted return to activities was deferred until 6 to 12 months postoperatively.
All RSAs were performed through a deltopectoral approach with a subscapularis peel. The biceps tendon was tenodesed. The press-fit humeral stem was implanted (Univers Revers; Arthrex) with a 135° inclination angle. The length (short or standard) and size of the stem were based on the surgeon's preference and fixation. After standard glenoid exposure and preparation were complete, a baseplate was then placed (Universal Glenoid or Modular Glenoid Baseplate; Arthrex). Glenosphere diameters ranged from 33 to 42 mm in increments of 3 mm depending on patient size. Postoperatively, the arm was immobilized with a sling for 4 weeks to protect the subscapularis repair. During this period, the sling was removed for hygiene and the patient was allowed hand, wrist, and elbow motion for simple activities of daily living. No lifting was allowed. After 4 weeks, the sling was discontinued and ROM was allowed, advancing up as tolerated.
Study Variables
Patient factors—including age, sex, tobacco use, worker's compensation, pseudoparalysis, and follow-up—were recorded. Pseudoparalysis was defined as the inability to achieve at least 90° of active FF with full passive motion. Functional outcomes—including active ROM and patient-reported outcomes (PROs)—were documented at baseline and a minimum of 2 years postoperatively. ROM was measured in FF, ER, and internal rotation (IR). IR was numerically scaled based on the nearest spinal level achieved with the thumb (T10 = 10, T12 = 12, L2 = 14, L4 = 16, S1 = 18, hip = 20). PROs included the visual analog scale (VAS) for pain, the American Shoulder and Elbow Surgeons (ASES) score, the Veterans Rand 12-Item Health Survey (VR-12), and the Subjective Shoulder Value (SSV). Any complications related to surgery, as well as any additional surgical procedures, were noted. Patients were surveyed on return-to-previous activities and satisfaction.
Radiographic Evaluation
All MRIs were reviewed preoperatively by the operative surgeon (P.J.D.) who included the degree of tendon fatty infiltration and tendon retraction stage according to Goutallier and Patte.15,27 In the ARCR group, tendon healing of the rotator cuff was graded on ultrasound by the treating surgeon (P.J.D.) at the final follow-up using the Barth modification of the Sugaya classification.1,31 Grade 1 designates tendons with sufficient thickness (>2 mm) and normal echo structure. Grade 2 indicates sufficient thickness with partial hypoechogenicity. Grade 3 indicates insufficient thickness (2 mm) without discontinuity. Grade 4 repairs show minor discontinuity in the tendon. Grade 5 repairs show a major discontinuity. Grades 1, 2, and 3 repairs were considered healed. Complete healing was defined as the healing of all tendons involved. Partial healing was defined as healing of at least 1 of the tendons. Complete and partial healing were considered “healed.” Functional outcomes were compared based on ARCR healing status (“healed” vs “unhealed”) and RSA. Patients with RSA underwent radiological evaluations using radiographs at each follow-up appointment.
Statistical Analysis
Continuous data were reported as the mean ± standard deviation, and comparisons were made using the Student t test or the Mann-Whitney U test based on normality. Categorical data were reported as frequencies and percentages, with comparisons made by chi-square analysis. All statistical analyses were conducted using SPSS Version 25 (IBM). P≤ .05 was used to denote statistical significance.
Results
Baseline characteristics are summarized in Table 1. A total of 81 patients met the study criteria—56 underwent ARCR and 25 underwent RSA. Patients in the RSA (age, 71.7 ± 7.7 years) group were older than those in the ARCR (age, 66.7 ± 7.4 years) group (P = .01). The mean follow-up for the ARCR and RSA groups was 56.5 ± 19 and 36.1 ± 7.6 months, respectively (P < .001). Pseudoparalysis was noted more frequently in the RSA group with 13 patients (52%) compared with 12 patients (21.4%) in the ARCR group (P = .016). Patients in the RSA group had higher rates of high-grade fatty atrophy (Goutallier grades 3 or 4) in the SS compared with the ARCR group—96% versus 53.6%, respectively (P < .001). Similarly, in the IS, the high-grade fatty atrophy rates were 96% and 51.8% for the RSA and ARCR groups, respectively (P < .001). The high-grade atrophy in the subscapularis rate was similar between groups—51.8% in the ARCR group and 40% in the RSA group (P = .327). The rate of patients with ≥2 tendons with grade 3 or 4 Goutallier changes was higher in the RSA group compared with the ARCR group—96% versus 46% (P < .001). Patients in the RSA group had a higher rate of advanced retraction stage (Stage 3 or 4) compared with the ARCR group: 100% versus 85.7% (P = .047).
Baseline Patient Characteristics a

Data are presented as mean ± SD or n (%). Bold P values indicate statistical significance AP, anteroposterior; ARCR, arthroscopic rotator cuff repair; ML, mediolateral; MRI, magnetic resonance imaging; IS, infraspinatus; RSA, reverse shoulder arthroplasty; SS, supraspinatus; SSC, subscapularis. Dots indicate not applicable.
Arthroscopic fixation techniques are summarized in Table 2. In the ARCR group, the SS and IS tendons were repaired with a single-row construct in 61% of cases.
Arthroscopic Technique a

Data are presented as n (%).
Supraspinatus and infraspinatus repair.
Pre- and postoperative outcomes are summarized in Table 3. Overall, PROs showed significant improvements from baseline to the final follow-up in all groups (P < .05) (Table 3). Pre- and postoperative VR-12 were lower in the RSA group compared with the ARCR group—30.5 ± 6.9 versus 36.2 ± 9.4, respectively (P = .008), and 38.1 ± 11.8 versus 47.7 ± 10.5, respectively (P = .002). Pre- and postoperative VAS, ASES, and SSV scores were similar between groups (P > .05). Pre- and postoperative FF were higher in ARCR compared with RSA—117°± 48° and 144°± 22° versus 90°± 49° and 113°± 25°, respectively (P = .029 and P < .001, respectively). The RSA group had lower postoperative IR compared with the ARCR group: S1 ± S2 versus L3 ± L4, respectively (P = .002). Patients experienced an IR loss of 2 vertebral levels after RSA (95% CI, 1-4; P = .003), while they gained one vertebral level of IR after ARCR (95% CI, 0-2; P = .12). No difference was found in satisfaction between the ARCR and RSA groups at the 2-year follow-up—48 (85.7%) versus 23 (92%) patients, respectively (P = .445).
Comparison of MRCT Functional Outcomes After ARCR and RSA a

Data are presented as mean ± SD, mean (95% CI), or n (%). Bold P values indicate statistical significance.ARCR, arthroscopic rotator cuff repair; ASES, American Shoulder and Elbow Surgeons; ER, external rotation; FF, forward flexion; IR, internal rotation; MRCT, massive rotator cuff tears; Postop, postoperative; Preop, preoperative; RSA, reverse shoulder arthroplasty; SSV, Subjective Shoulder Value; VAS, visual analog scale; VR-12, Veterans Rand 12-Item Health Survey.
Spinal level.
In the ARCR group, 5 complications (8.9%) were observed consisting of clinical failure with conversion to RSA between 18 and 60 months of follow-up. In the RSA group, 1 case (4%) of shoulder stiffness occurred and was treated by arthroscopic lysis of adhesions.
A comparison of functional outcomes based on ARCR healing status and RSA is shown in Table 4. Complete healing was achieved in 19 patients (34%), while partial healing was achieved in 12 (21%). Thus, 31 rotator cuffs (55%) were considered healed, and 25 (45%) unhealed. A separate analysis of functional outcomes based on tendon healing after ARCR only found a difference in postoperative FF: 150°± 18° in healed patients versus 136°± 26° in not healed (P = .044). Postoperative satisfaction was achieved in 25 (81%) of patients whose rotator cuff healed and in 23 (92%) of those whose did not, with no significant difference between subgroups (P = .269).
Comparison of MRCT Functional Outcomes After ARCR Stratified by Tendon Healing With RSA a
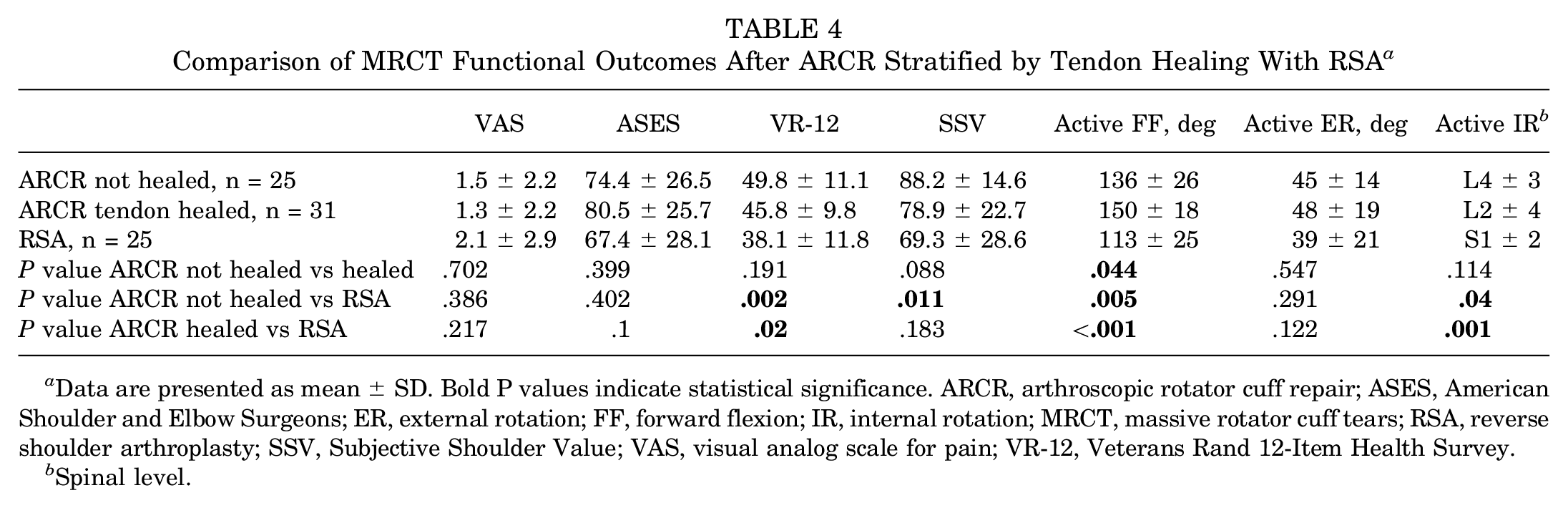
Data are presented as mean ± SD. Bold P values indicate statistical significance. ARCR, arthroscopic rotator cuff repair; ASES, American Shoulder and Elbow Surgeons; ER, external rotation; FF, forward flexion; IR, internal rotation; MRCT, massive rotator cuff tears; RSA, reverse shoulder arthroplasty; SSV, Subjective Shoulder Value; VAS, visual analog scale for pain; VR-12, Veterans Rand 12-Item Health Survey.
Spinal level.
Discussion
The main findings of this study were that patients with MRCTs and high-grade fatty atrophy without GHOA can achieve significant short-term postoperative improvements in VAS, ASES, SSV, and VR-12 scores with either ARCR or RSA. Improvements in ROM were observed in FF for both groups, with the ARCR group achieving greater values. No significant differences were noted in terms of complications, reintervention, return to previous activities, or satisfaction among groups. Although there was a 45% retear rate with ARCR, postoperative functional outcomes were comparable between the healed and unhealed groups. These findings suggest that both ARCR and RSA can provide clinical improvement and patient satisfaction in the treatment of MRCT with high-grade fatty atrophy without GHOA.
Patient-related factors—such as age, function, and goals of care—must be considered during clinical decision-making before managing MRCTs without GHOA. 7 Advanced age may be a factor in considering RSA for MRCTs, to avoid a second procedure. We found that patients from the RSA group were older than patients who underwent an ARCR. However, it is important to note that age alone was not the only factor guiding the decision to opt for RSA. Other than age, assessing a patient's preoperative function provides nuance to the decision-making. In our study, patients in the RSA group had significantly lower preoperative FF compared with the ARCR group. Previous authors have suggested that patients with pseudoparalysis in the setting of MRCT should be treated with RSA to regain overhead function.32,33 Others have suggested that pseudoparalysis itself is not an absolute indication for RSA, particularly if the duration of pseudoparalysis is <6 months.8,9,24 Denard et al 8 reported that ARCR of MRCTs resolved pseudoparalysis in 90% of patients among whom the mean duration of pseudoparalysis was approximately 3 months. Furthermore, Oh et al 24 found that postoperative function and rotator cuff healing after ARCR of MRCT was not different when considering pseudoparalysis. Despite these improvements, Denard et al 9 found that increased duration of pseudoparalysis correlated with a failure to recover overhead function after ARCR of MRCTs. While pseudoparalysis has been frequently reported as a factor that contributes to surgical decision-making between RSA and ARCR, the procedure should be based on a conglomerate of patient factors and not solely on the presence of preoperative pseudoparalysis.
Previous studies have demonstrated improvements in shoulder function after RSA in patients with MRCT without GHOA.19,22 In their retrospective study of 64 patients with a mean age of 73 years who underwent RSA for MRCT without GHOA, Hartzler et al 19 showed that VAS for pain scores improved from 5.5 ± 2.5 to 2 ± 2.5 (P < .001), ASES from 41.6 ± 17.3 to 74 ± 22 (P < .001), FF from 60°± 33° to 122°± 39° (P < .001), and ER from 21°± 28° to 29°± 26° (P < .01). Notably, preserved overhead motion was a risk factor for poor improvement. Liu et al 21 reported similar outcomes after RSA in line with previous authors 19 but found statistically significant differences in postoperative ASES, shortened version of the Disabilities of the Arm, Shoulder and Hand (QuickDASH), Simple Shoulder Test, Constant scores, and ROM in favor of ARCR after matching groups for global fatty degeneration index. Consistent with these previous studies, our results also revealed improvement in functional outcomes after RSA. However, in contrast to Liu et al, 21 we found similar functional outcomes between ARCR and RSA, with statistically significant differences only in FF and IR. One possible explanation for this is that in their study, both groups presented a mean global fatty degeneration index of 2, while more than half of our patients in the ARCR group had a Goutallier grade of 3 or 4 in all tendons, with most of them having a high retraction stage. The worse baseline characteristic may potentially explain the lack of differences between our groups compared with their study. In addition, some studies have reported that RSA has a higher complication rate compared with ARCR, especially among younger patients at long-term follow-ups.10,28 A study 19 of RSA in the setting of MRCT demonstrated a major short-term complication rate of 12% and a revision rate of 1.4%. Our RSA group results showed a lower complication rate compared with this study. Although we did not find differences in complications and reoperation rates between groups, the relatively small sample size and the short-term follow-up must be considered. Nonetheless, our results suggest that ARCR remains a viable option for treating MRCT, yielding at least similar results compared with RSA in carefully selected patients.
In the setting of MRCT, determining tendon reparability is challenging. Fatty degeneration, tear size, and tendon retraction have been correlated with reparability and tendon healing.20,23,29 Liu et al 21 compared patients undergoing ARCR or RSA and found larger tears in the RSA groups—32.7 ± 9.1 mm versus 43.2 ± 10.1 mm anteroposteriorly (P < .001) and 35.8 ± 11.6 mm versus 44.8 ± 14.8 mm mediolaterally (P = .001), respectively. The authors also reported a higher global fatty degeneration index for RSA compared with ARCR—2.2 ± 1.8 versus 1.8 ± 0.5 (P = .002). Similarly, we found that patients who underwent RSA were more likely to have >1 tendon with a high atrophy grade and had higher SS and IS tendon atrophy, as well as a higher retraction stage compared with ARCR. The greater atrophy grade and retraction stage in our RSA group are likely explained by selection bias based on the understanding that significant atrophy increases the difficulty of repair and correlates negatively with tendon healing.17,23 RSA has been recommended for young adults with MRCT and no GHOA when tendon-related factors suggest poor healing potential.10,28 In the setting of MRCT treated with ARCR, retears are not uncommon, with rates reported4,13,26 ranging between 25% and 94%. However, previous studies have demonstrated functional improvements after ARCR even in unhealed cases.4,13,30 Chung et al 4 reported comparable postoperative ASES scores after ARCR for MRCT between healed and unhealed groups at a minimum 1-year follow-up—88.24 ± 15.6 and 80.21 ± 21.23, respectively (P = .055). Similarly, the authors found no significant differences between groups in Constant score, VAS, or ROM. The authors suggested that a decrease in tear size, even in failed repairs, alongside subacromial decompression with acromioplasty, may contribute to functional improvement. This was attributed to a restored force couple and increased stability within the glenohumeral joint. We observed comparable postoperative results between the healed and unhealed groups. However, patients in the healed group exhibited better FF at the most recent follow-up. The literature addressing long-term follow-ups after ARCR of MRCT is limited. Nevertheless, while ARCR leads to long-term sustained improvements, some studies have shown that patients with an intact repair tend to achieve superior outcomes compared with those with a retear.6,34 Collin et al 6 reported higher Constant and SSV scores in patients with an intact repair compared with those with a retear at the 20-year follow-up—75 ± 11.1 versus 57.8 ± 21.2 (P = .01) and 79 ± 16 versus 64 ± 23 (P = .03), respectively. Similar findings were reported by Zumstein et al 34 at the 3- and 10-year follow-ups. Despite our reported retear rate, which could be linked to the inclusion of patients with high-grade fatty atrophy, our data indicate that repair did not hinder functional improvements.
Limitations
This study has several limitations. First, the decision to proceed with ARCR or RSA was made based on a combination of rotator cuff tear characteristics, surgeon assessment, and patient preference and thus subject to selection bias. Second, because of the small sample size, patients were not matched by demographic characteristics, follow-up duration, and rotator cuff tear characteristics. For instance, patients with RSA had worse tears, limiting the comparability between groups. Third, the generalizability of our findings may be limited since all surgeries were performed by a single high-volume shoulder surgeon at a single institution. Fourth, pre- and postoperative strength measurements were not collected, which could have provided additional insight into managing this condition. Fifth, the pre- and postoperative imaging assessments conducted by the surgeon, without multiple graders and an interrater correlation study, are susceptible to biases. Sixth, we did not investigate potential predictors for rotator cuff healing and function, such as pre- and postoperative acromiohumeral distance, which could have added value to the study. Last, given the short-term nature of this study's follow-up, predicting the mid- and long-term comparative results remains uncertain. Additional comparative studies, focusing on Goutallier grades and tendon involvements with extended follow-up periods, are necessary for a more conclusive assessment.
Conclusion
Both ARCR and RSA improved functional outcomes in patients with MRCT without GHOA. While healing was moderate after ARCR, postoperative ROM was greater after ARCR compared with RSA in appropriately selected patients. In addition, healed rotator cuffs demonstrated improved postoperative FF compared with unhealed repairs.
Footnotes
Final revision submitted May 14, 2024; accepted May 28, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.B.N. has received education payments from Rock Medical Orthopedics. L.A.G. has received education payments from Arthrex, Pinnacle, and Steelhead Surgical; hospitality payments from Stryker and Aesculap Biologics; and nonconsulting fees from Arthrex. P.J.D. has received consulting fees from Arthrex and Pacira Pharmaceuticals, nonconsulting fees from Arthrex, royalties from Arthrex, and education payments from Steelhead Surgical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Salus IRB (102).