
Abstract
Background:
Previous studies have shown good clinical outcomes in patients with irreparable large or massive rotator cuff tears treated using arthroscopic partial repair (APR); however, few studies have evaluated both functional and structural outcomes in these patients.
Purpose:
To evaluate both functional and structural outcomes in patients with large or massive rotator cuff tears treated using APR.
Study Design:
Case series; Level of evidence, 4.
Methods:
Between March 2009 and November 2016, a total of 30 patients underwent APR because of the irreparability of their large or massive rotator cuff tears during surgery. Of these patients, 24 completed the minimum 24-month follow-up (mean, 61.8 ± 27.1 months; range, 24-112 months) and were included in this study. Functional outcome measures included the Japanese Orthopaedic Association (JOA) and University of California Los Angeles (UCLA) scores and the visual analog scale for pain. Structural outcome measures comprised preoperative fatty degeneration, mediolateral tear size, residual tendon attachment area, and glenohumeral (GH) arthritic changes evaluated on magnetic resonance imaging scans or plain radiographs before and after surgery. Functional and structural outcomes were evaluated preoperatively, at 3 months postoperatively, and at the final follow-up.
Results:
The JOA scores for all patients significantly improved from 67.9 ± 11.3 preoperatively to 85.4 ± 15.6 postoperatively (P < .0001). Similarly, the UCLA scores significantly improved from 15.8 ± 4.20 preoperatively to 29 ± 6.69 at final follow-up postoperatively (P < .0001). The mediolateral tear size were significantly decreased at 3 months postoperatively (P < .001) and at the final follow-up (P < .001). Compared with preoperative scores, the novel score evaluating the residual tendon attachment area improved from 3.08 ± 0.46 to 3.54 ± 0.41 (P < .001) after surgery overall, although it significantly deteriorated from 3 months postoperatively to the final follow-up. GH osteoarthritis progressed in 6 patients (25%). Patients who developed osteoarthritis had lower JOA and UCLA scores than did those who did not (JOA, P = .010; UCLA, P = .037).
Conclusion:
In irreparable large or massive rotator cuff tears treated using APR, functional outcome improved after surgery. Although the residual tendon attachment area improved, functional outcome after APR corresponded to the GH alterations at the midterm follow-up. Longer-term follow-up is needed to further elucidate the effect of APR on clinical outcomes in these patients.
Keywords
Arthroscopic rotator cuff repair (ARCR) is generally performed to treat rotator cuff tears (RCTs). In particular, the functional outcomes of ARCR for small- or medium-sized tears are satisfactory. 1,11,12,20,33,34 However, ARCR is not always acceptable for massive RCTs because of their irreparability, fatty degeneration, 7,30 muscle atrophy/adhesion, or severe retraction. 31,32 These are often associated with postoperative retear, low functional outcome, or low patient satisfaction. 33 For irreparable RCTs, various surgical options, such as arthroscopic partial repair (APR), arthroscopic debridement, graft augmentation, tendon transfer, biological augmentation, biceps augmentation, superior capsular reconstruction, and reverse total shoulder arthroplasty, are considered. 28 APR is less invasive than are other surgeries. 2,13
In 1993, Burkhart et al 5 first introduced the theoretical basis for partial repair; thereafter, several authors reported good functional outcomes despite structural failure. 3,14,18,23 Berth et al 3 compared the outcomes of arthroscopic debridement and APR in patients with massive RCTs. In their report, the 2 surgical methods were comparably effective for pain relief, but APR was superior in terms of functional outcome. These studies, however, focused on functional outcome and not on structural evaluation.
Previous studies have evaluated structural outcome on magnetic resonance (MR) imaging (MRI) scans showing only the presence or absence of retear. No previous study has evaluated the structural alterations of the attached tendon area after surgery in terms of tendon retention. Therefore, the purpose of the present study was to analyze both functional and structural outcomes in patients with irreparable large or massive RCTs treated using APR. We evaluated these measures 3 times via MRI to show how the propagation of the tendon attachment area progressed. We hypothesized that the functional outcome of the APR of irreparable cuff tears would be acceptable after surgery, despite a certain degree of structural change.
Methods
This study was approved by the institutional review board of our institution, and informed consent was obtained from all patients preoperatively.
Sample Population
The patients with RCTs were diagnosed using MRI scans. First, they underwent conservative treatment for at least 2 months before surgery, including the administration of anti-inflammatory drugs, physical therapy, and intra-articular injections of corticosteroids or hyaluronic acid. The patients who did not improve with conservative treatment underwent surgery.
The inclusion criteria for this study were as follows: (1) large or massive RCTs with pain or functional disability refractory to conservative treatment; (2) intact teres minor; (3) functional and structural evaluation available preoperatively, at 3 months postoperatively, and at the final follow-up; (4) minimum 24-month follow-up after surgery; and (5) tendon repair attempted first, with conversion to APR when complete coverage failed, with the arm at the side. Exclusion criteria were as follows: (1) addition of open surgery; (2) history of nerve palsy, fracture, dislocation, or shoulder surgery; and (3) arthritic changes of the glenohumeral (GH) joint before surgery.
Between March 2009 and November 2016, 180 patients diagnosed with a large to massive tear underwent ARCR at our institution. The massive or large RCTs were diagnosed using preoperative MRI scans, with a tear defined as having an anteroposterior or mediolateral diameter of 3 cm or greater. Based on the criteria mentioned above, 38 patients were excluded from this study. Of the remaining 142 patients, 30 underwent APR. Six patients were lost to follow-up; thus, 24 patients who completed the minimum 24-month follow-up (mean, 61.8 ± 27.1 months; range, 24-112 months) were included in the analysis (follow-up rate, 80%) (Figure 1).
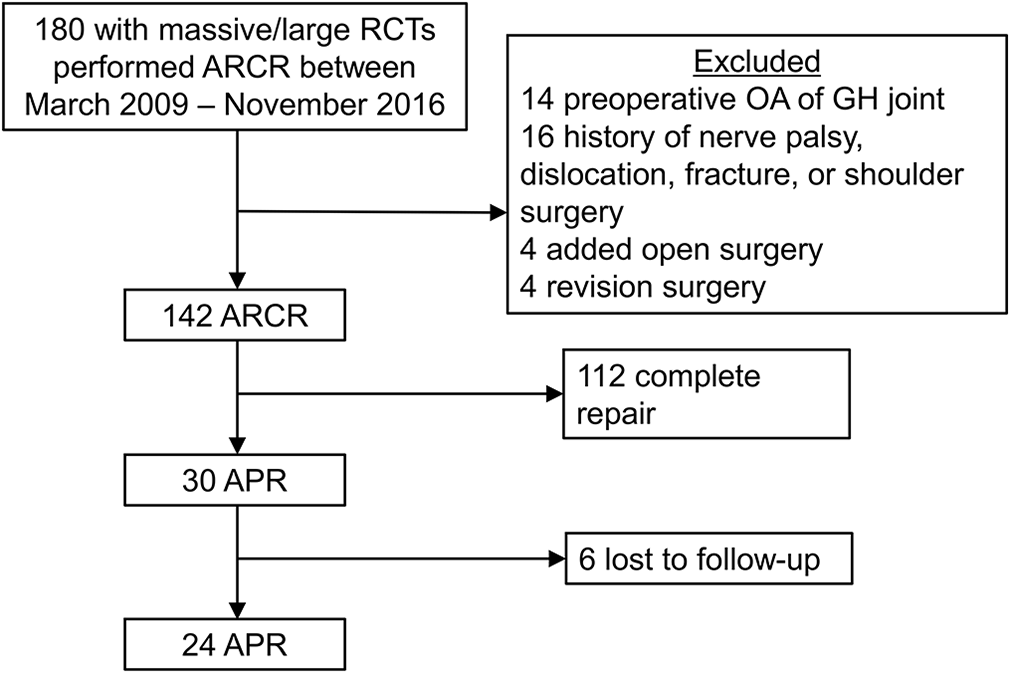
Patient selection flowchart. APR, arthroscopic partial repair; ARCR, arthroscopic rotator cuff repair; GH, glenohumeral; OA, osteoarthritis; RCT, rotator cuff tear.
Surgical Procedure
Patients underwent ARCR in the beach-chair position under general anesthesia. Five routine arthroscopic portals (anterior, anterosuperior, lateral, posterolateral, and posterior) were used during surgery. After inspection of the GH joint and subacromial bursa, the torn tendons were mobilized with or without margin convergence. For all patients, we attempted primary repair with the arm at the side. When we could not repair the tendons even in these positions, partial repair was attempted.
The torn cuff was repaired to the footprint as much as possible using a single-row or suture bridge technique depending on tendon mobility and tear configuration. Various anchors were used in the present study: Panalok RC loop anchor (DePuy Mitek), Healix Advance BR 3 suture anchor with Orthocord (DePuy Mitek), Versalok anchor (DePuy Mitek), and suture anchor with PEEK SwiveLock C (Arthrex). Additionally, we used the Fastin RC anchor (DePuy Mitek), especially for patients with osteoporosis.
For single-row repairs, 1 row of anchors was placed on the lateral aspect of the footprint, and the torn cuff was fixed using interrupted sutures. For suture bridge repair, 1 row of anchors was placed on the medial aspect of the footprint, and the torn cuff was fixed using the knotless anchors on the lateral aspect of the footprint.
Postoperatively, patients' arms were immobilized in a sling for 6 weeks to maintain the shoulder in neutral rotation and 20° of abduction. Self-assisted passive motion was permitted at 4 weeks only during supervised physical therapy. At week 7, active assistive motion of the shoulder was started. Subsequently, isometric muscle strengthening exercises were permitted at week 8. Isotonic training was permitted at week 13.
Functional Assessment
The Japanese Orthopaedic Association (JOA) and University of California Los Angeles (UCLA) scores were used as functional outcome measures. A 10-cm visual analog scale (VAS) was used to assess pain (0 cm, no pain; 10 cm, worst imaginable pain). These functional evaluations were performed before and after surgery. Range of motion (ROM) of active elevation, abduction, and external rotation were assessed using a goniometer, and the active ROM of internal rotation (back reach) was measured in vertebral levels. 24,27 Muscle strength of elevation, abduction, and external and internal rotation were measured using a handheld dynamometer (MicroFET2; Hogan Health Industries). Physical examinations were performed by an independent physical therapist blinded to the study. The measures were assessed preoperatively and postoperatively.
Structural Assessment
The status of the rotator cuff tendons was examined using MRI scans (1.5-T, T1- and T2-weighted oblique-coronal, axial, and sagittal images, 3 mm in thickness). For imaging, patients were placed in a supine position with their arm at their side. All patients underwent MRI and plain radiography preoperatively, 3 months postoperatively, and at the final follow-up. The images were reviewed by 2 experienced orthopaedic surgeons H.M and K.T who had expertise in shoulder surgery and imaging.
Fatty degeneration of the supraspinatus, infraspinatus, teres minor, and subscapularis was evaluated on oblique-sagittal T2-weighted MRI scans taken 2 cm medial from the joint line, on which the scapular spine was seen in contact with the scapular body (Y-view). 15 A general fatty degeneration index was calculated as the mean of the fatty degeneration scores for the supraspinatus, infraspinatus, subscapularis, and teres minor.
The mediolateral tear size was evaluated based on the methods described by Davidson and Burkhart. 10 The longest length was measured on the coronal-oblique plane on T2-weighted images. The residual tendon attachment area was evaluated instead of anteroposterior tear size, using a novel scoring system adapted from the Collin 8,21 and Nakamura 24 classifications. In this system, the rotator cuff footprint was divided into 5 components as follows: zone 1 as the lesser tubercle crest, zone 2 as the lesser tubercle, zone 3 as the superior facet, zone 4 as the middle facet, and zone 5 as the inferior facet. Each component was scored 0, 0.5, or 1.0 according to the extent of the residual tendon attachment (0 points for none, 0.5 points for tendon attachment of half or less than half of the component, and 1 point for full tendon attachment or more than half of the component) (Figure 2). The total score of the 5 components was calculated and used to represent the tendon attachment area (maximum score, 5). Representative data are shown in Figure 3. To assess the reproducibility of this grading system for the tendon attachment area, a random sample of 150 components (zones 1 to 5) from 30 patients was reviewed twice by 2 observers (H.M., K.T.).
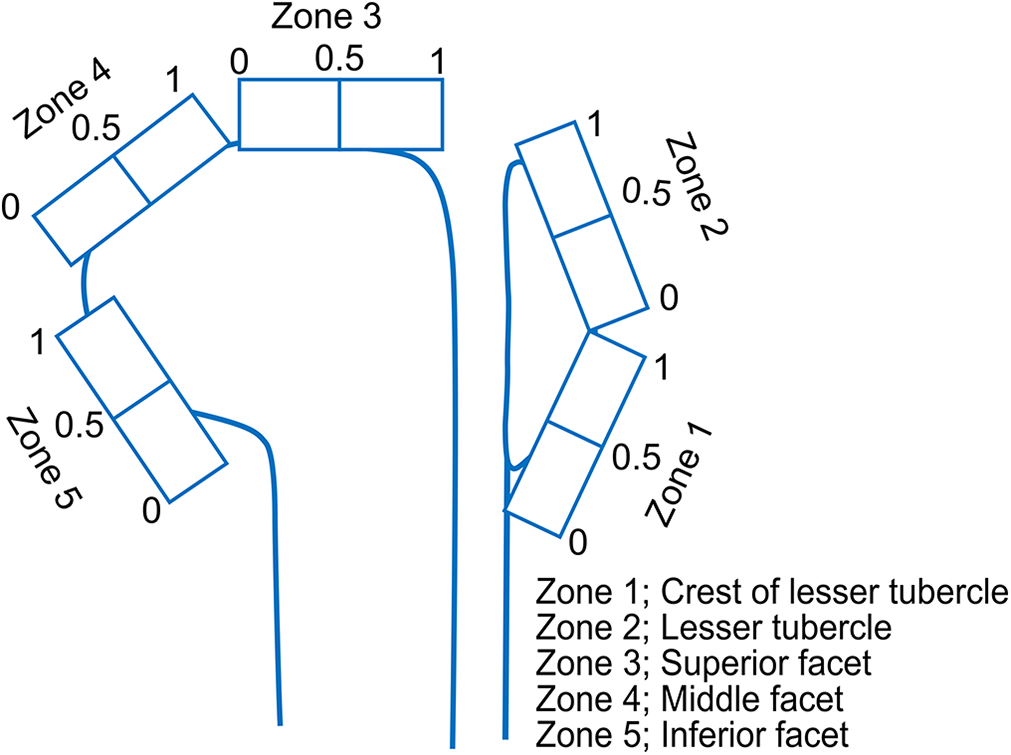
Schema of rating scores for the residual tendon attachment area.

Zone 4 (middle facet) are scored according to the extent of the residual tendon attachment: (A) 0 points for none, (B) 0.5 points for tendon attachment of half or less than half of the component, and (C) 1.0 point for full tendon attachment or more than half of the component. ISP, infraspinatus.
To assess osteoarthritic (OA) change from the preoperative period to the postoperative final follow-up, the Hamada classification was used. Radiographs of 3 directions (anteroposterior, axial, and scapular Y-view) were obtained preoperatively, 3 months postoperatively, and at the final follow-up. Patients showing grade 4A or more were defined as exhibiting positive OA change. 16
Statistical Analysis
The JMP13 software (SAS Institute) was used for statistical analysis. Data are expressed as mean values with SDs. Repeated measures of retraction and anterior-posterior length were analyzed separately by using repeated-measures analysis of variance. Compound symmetry was used as a correlational structure. Multiple comparisons between means were performed using the Tukey-Kramer honest significant difference test. The paired t test was used to compare JOA and UCLA scores, ROM, VAS score, and muscle strength (relative strength ratio of the involved side to the uninvolved side) between the preoperative period and the postoperative final follow-up. A t test was used to compare the final evaluation of JOA and UCLA scores between patients with and patients without GH arthritis. Intraobserver and interobserver agreements for the tendon attachment area were evaluated using Cohen kappa statistic, and agreements were evaluated using the intraclass correlation coefficient (ICC). A P value <.05 was considered statistically significant. 7,22
Results
Eleven patients had the anterosuperior type, 4 had the posterosuperior type, and 9 had the 3-tendon rupture type. Patient characteristics are shown in Table 1.
Patient Characteristics

Functional Outcome
The JOA score of all patients significantly improved from 67.9 ± 11.3 preoperatively to 85.4 ± 15.6 at the final follow-up postoperatively (P < .0001) (Figure 4A). Similarly, the UCLA score significantly improved from 15.8 ± 4.20 preoperatively to 29 ± 6.69 at the final follow-up postoperatively (P < .0001) (Figure 4B). The ROM, VAS score, and muscle strength changes are shown in Table 2.

Preoperative and postoperative (final follow-up) (A) Japanese Orthopaedic Association (JOA) scores and (B) University of California Los Angeles (UCLA) scores. *Statistically significant (JOA, P < .0001; UCLA, P < .0001) difference from preoperative scores.
Functional Outcomes a
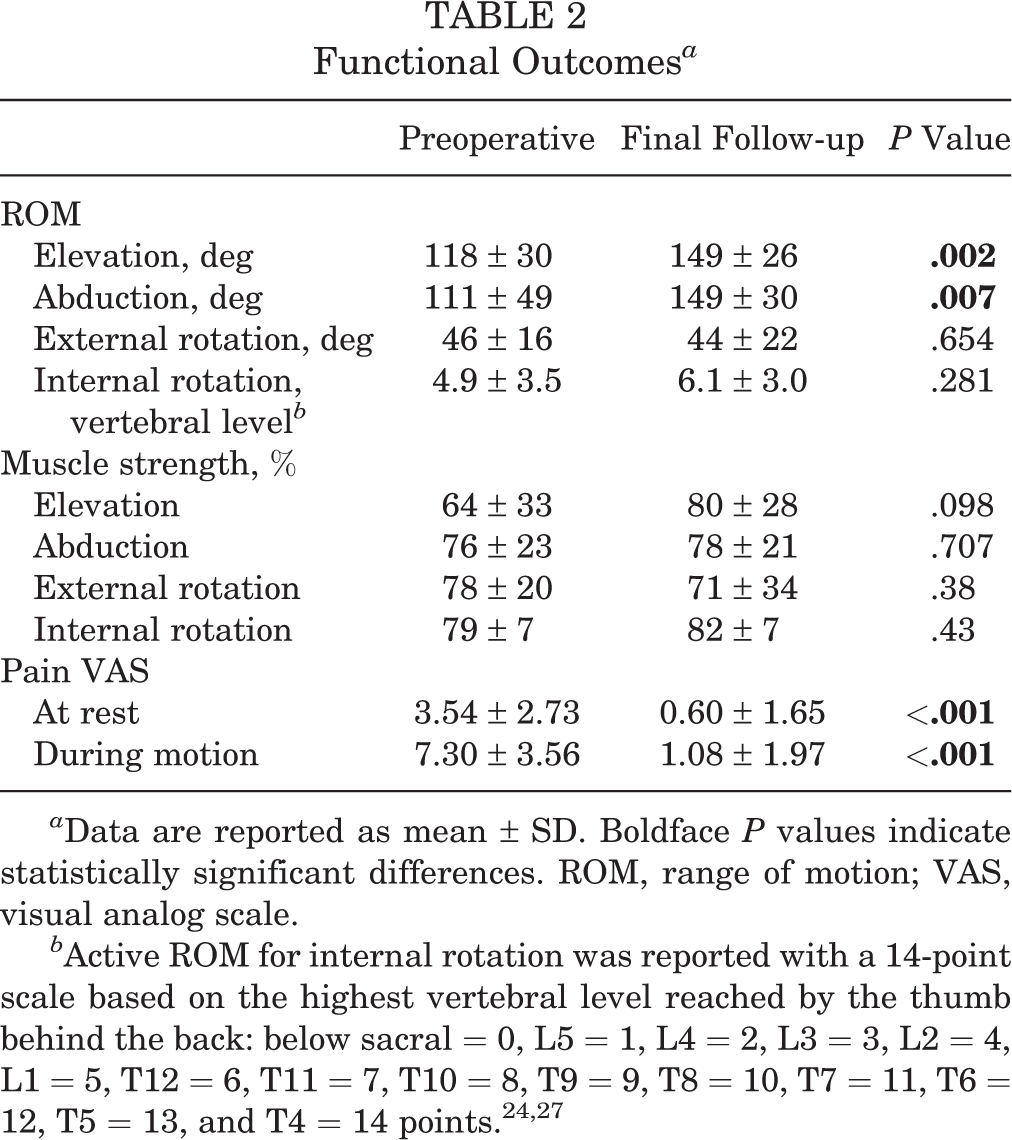
a Data are reported as mean ± SD. Boldface P values indicate statistically significant differences. ROM, range of motion; VAS, visual analog scale.
Structural Outcomes
The mediolateral tear size for all patients significantly decreased from 42.49 ± 7.66 mm preoperatively to 33.6 ± 7.07 mm 3 months postoperatively (P < .001) and to 31.9 ± 12.9 mm at the final follow-up (P < .001) (Figure 5).
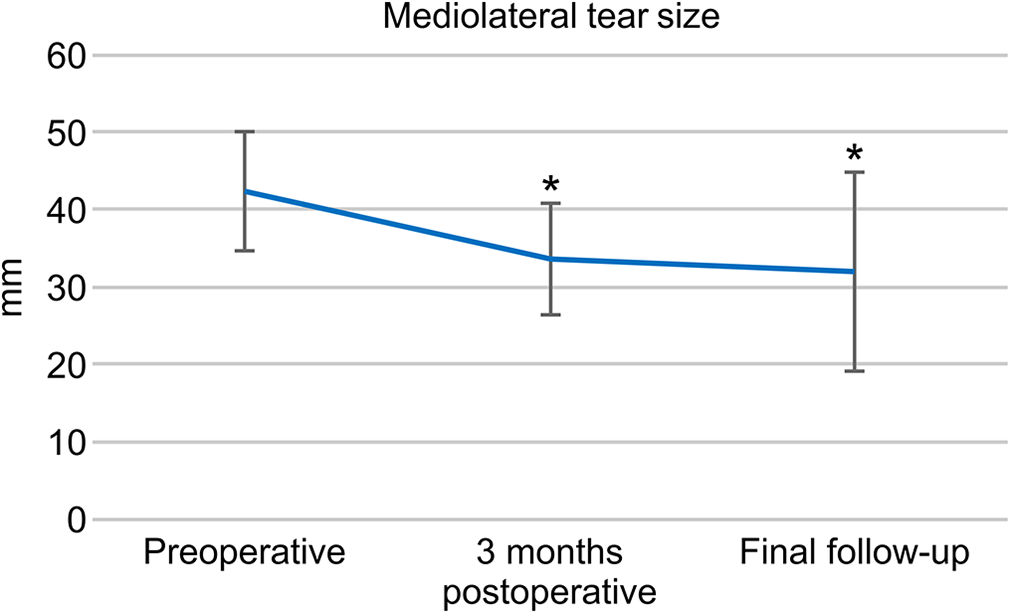
Preoperative, 3-month postoperative, and final follow-up mediolateral tear sizes. *Statistically significantly different from preoperative scores. The mediolateral tear size significantly decreased at 3 months postoperatively (P < .001) and the final follow-up (P < .001).
Regarding the residual tendon attachment area, the ICCs for intraobserver and interobserver reliabilities are provided in Table 3. They were very good. The scores for each zone are shown in Table 4. At zones 1 and 5, the score was consistently 1 point (full to more than half preserved) throughout the follow-up periods. At zone 3, no significant change in the mean score was seen between any of the times. At zones 2 and 4, the mean score significantly improved from preoperatively to 3 months postoperatively and from preoperatively to the final follow-up (P < .001 for all). In both of these zones, the scores decreased from 3 months postoperatively to the final follow-up; this decrease was statistically significant for zone 2 (P = .008) but not for zone 4 (P = .420). The mean total score of the tendon attachment area significantly improved from preoperatively to 3 months postoperatively (P < .001) and from preoperatively to the final follow-up (P < .001), and there was a statistically significant decrease from 3 months postoperatively to the final follow-up (P = .032). The percentage of patients with 0, 0.5, and 1 points identified in each zone is shown in Table 5.
Intraobserver and Interobserver Reliabilities for the Tendon Attachment Area a

a Intraclass correlation coefficient (ICC) values: very good, 0.81-1.00; good, 0.61-0.80; moderate, 0.41-0.60; fair, 0.21-0.40; poor, 0.00-0.20. Zone 1 = lesser tubercle crest; Zone 2 = lesser tubercle; Zone 3 = superior facet; Zone 4 = middle facet; Zone 5 = inferior facet.
Summary of Scores Rating the Residual Tendon Attachment Area a

a Data are reported as mean ± SD. Zone 1 = lesser tubercle crest; Zone 2 = lesser tubercle; Zone 3 = superior facet; Zone 4 = middle facet; Zone 5 = inferior facet.
b Statistically significantly different from preoperatively to 3 months postoperatively (P < .001).
c Statistically significantly different from preoperatively to the final follow-up (P < .001).
d Statistically significantly different from 3 months postoperatively to the final follow-up (P < .05).
Details of the Residual Tendon Attachment Area Using the Novel Scoring System a

a Data are reported as number of patients (%). Adapted from the Collin 8,21 and Nakamura 24 classifications for extent of residual tendon attachment: 0 points (Pt) = none, 0.5 Pt = tendon attachment of half or less than half of the component, 1 Pt = full tendon attachment or more than half of the component.
OA changes (Hamada stage 4A or more) were seen in 0 patients (0%) preoperatively and 6 patients (25%) at the final follow-up. For the OA group, the JOA score improved from 60.4 ± 8.6 preoperatively to 72.9 ± 20.6 postoperatively (P < .01); the UCLA score improved from 13.3 ± 4.1 preoperatively to 23.3 ± 9.8 postoperatively (P < .001). For the non-OA group, the JOA score improved from 70.4 ± 11.1 preoperatively to 89.6 ± 11.4 postoperatively (P < .001); the UCLA score improved from 16.6 ± 4.0 preoperatively to 30.9 ± 4.2 postoperatively (P < .01). Consistently, postoperative JOA and UCLA scores were significantly decreased in the OA group compared with the non-OA group (JOA, P = .010; UCLA, P = .037).
Discussion
Overall, functional outcome improved after surgery in this series. The tendon attachment area at 3 months postoperatively and at the final follow-up was significantly better than was the preoperative attachment area, although this area deteriorated at the final follow-up compared with that at 3 months postoperatively. GH arthritis progressed in 25% of this study population, and its coexistence was significantly associated with poorer functional outcome. These results suggest that functional outcome after APR corresponds to the GH alterations at the midterm follow-up.
APR for irreparable cuff tears leads to a significant improvement in functional outcome and is a satisfactory treatment option. 17,25,26,29 Partial repair provides good functional scores at the midterm follow-up 12 as well as the short-term follow-up. 19,20 Several studies have evaluated tendon structural integrity in patients undergoing APR. In the present study, we examined not only functional outcomes but also structural outcomes, with the changes of the tendon attachment area, using our novel scoring system via MRI.
Compared with the preoperative scores, the JOA and UCLA scores significantly improved after surgery, and the residual tendon attachment area significantly improved at the final follow-up. One study revealed more frequent retears in APR than in completely repaired tears (48.8% vs 20%). 14 Heuberer et al 18 reported a similar rate of retear in partial and complete repairs (53% vs 29%). Furthermore, Iagulli et al 19 observed “significant retear” more frequently in partial repairs than in complete repairs (7% vs 2%). In short, several authors have reported a high retear rate after APR. However, these studies did not detail how rerupture was evaluated after APR. In the present study, rerupture in patients with irreparable large or massive cuff tears treated using APR was evaluated and the extent of residual tendon attachment in these patients was successfully demonstrated using a novel scoring system with a high intra- and interobserver reproducibility. Thus, although the residual tendon attachment area had deteriorated at the final follow-up, these areas were significantly increased compared with those preoperatively.
In 1994, partial repair was originally conceived by Burkhart et al 6 as an open repair of the inferior half of the infraspinatus to create a force couple. An arthroscopic modification of this technique was described in 2001. 4 This balancing of force can allow for the compression of the humeral head into the concave glenoid fossa, even if a significant residual cuff defect is present in the superior rotator cuff. Furthermore, the compression into the glenoid fossa caused by the subscapularis and infraspinatus tendons aids the centralization of the humeral head and resists the superior translation of the head despite the superior pull of the deltoid muscle during abduction. 29 This may partly explain why partial repair produced good functional outcomes in the present study.
Shon et al 31 described a correlation of the substantial fatty infiltration of the teres minor (stage 2 or more in the Goutallier classification) with outcome deterioration and poor satisfaction after APR. In the present study, the fatty infiltration of the teres minor consistently rated low (stage 0 or 1 in the Goutallier classification), with its footprint preserved. This may have also contributed to the good functional outcomes in the present study.
Cuff et al 9 reported that 36% of patients had a progression of the Hamada stage after partial repair, although a relationship between this progression and clinical outcome was not noted. In our study, 25% of the patients had progressed past Hamada stage 4A, with worsened functional outcome after surgery.
This study has several limitations. First, it had inadequate statistical power to evaluate the outcome because of the small number of patients (N = 24). Therefore, the correlations between the novel scoring system and functional outcomes were not analyzed. Second, this study included a retrospective cohort in which 24 of 30 APRs in 180 consecutive massive or large RCTs were evaluated; that is, 6 patients were lost to follow-up. Third, a longer follow-up window may have shown different outcomes because of tear progression or GH arthritis. Fourth, 2 surgical techniques or their combination was employed in the present study. The suture bridge technique was used in tendons with high mobility, and the single-row technique was used in those with low mobility. We also performed 1 of 2 different procedures for the long head of the biceps tendon (tenotomy or tenodesis) or none. Finally, functional evaluation was insufficient; only JOA and UCLA scores were used, not Constant or American Shoulder and Elbow Surgeons scores.
One strength of the present study is that we confirmed the serial changes of both structural and functional outcomes in patients with irreparable RCTs treated via APR, with a mean follow-up period of 5 years after surgery.
Conclusion
In irreparable large or massive rotator cuff tears treated using APR, functional outcome improved after surgery. Although the residual tendon attachment area improved, functional outcome after APR corresponded to the GH alterations at the midterm follow-up. Longer-term follow-up is needed to further elucidate the effect of APR on clinical outcomes in these patients.
Footnotes
Final revision submitted September 6, 2020; accepted October 2, 2020.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Kurume University Hospital (reference No. 19072).