
Abstract
Background:
The relationship between hip rotational abnormalities and hip labral size has not been fully investigated.
Purposes:
To (1) examine the correlation between rotational abnormalities of the hip and labral size, while also identifying other predictive values for hip labral size, and (2) explore whether femoral torsion will lead to increased labral size.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 180 patients (180 hips) with femoroacetabular impingement syndrome (FAIS) (mean age, 36.81 ± 10.17 years; 67 male, 113 female) who underwent hip arthroscopic surgery between January 2021 and May 2022 were included. The femoral version (FV), acetabular version, and combined version angles were measured on computed tomography, and the labral length and height at the 12-o’clock and 3-o’clock positions were measured on magnetic resonance imaging. The hips were categorized into 3 groups based on FV angle: small (SFV; <10°); moderate (MFV; ≥10° and ≤20°), and large (LFV; >20°), and group comparisons were performed. Linear correlation and regression analysis were employed.
Results:
Predictive factors for labral length were FV angle (β = 0.298; P = .02), sex (β = −0.302; P < .001), and age (β = −0.169; P = .016) at 3 o’clock and lateral center-edge angle (LCEA; β = −0.208; P = .005) and age (β = −0.186; P = .011) at 12 o’clock. FV angle was positively correlated with labral length at 3 o’clock (r = 0.267; P < .001) and negatively correlated with age (r = −0.222; P = .003) and female sex (r = −0.202; P = .006). LCEA (r = −0.227; P = .002) and age (r = −0.205; P = .006) were negatively correlated with labral length at 12 o’clock. Labral length at 3 o’clock was significantly different between the LFV (n = 49 hips), MFV (n = 65 hips), and SFV (n = 66 hips) groups (9.85 ± 2.28, 8.89 ± 2.44, and 8.30 ± 2.05 mm, respectively; P = .027 for LFV vs MFV; P < .001 for LFV vs SFV).
Conclusion:
Patients with FAIS who exhibited a higher FV angle were at a greater likelihood of having a larger anterior labral length. Increased femoral anteversion and decreased LCEA, male sex, and younger age were significantly associated with longer hip labral length.
The hip labrum is an important anatomic structure attached to the acetabular rim. It has many biomechanical roles, including deepening the acetabular volume, maintaining intra-articular fluid, protecting articular cartilage by spreading the contact load, and increasing axial distractive stability by means of the suction seal effect.26,29,34 Femoroacetabular impingement syndrome (FAIS) is a condition affecting the hip joint that is characterized by abnormal contact between the femoral head and acetabulum, 13 with the most frequently observed pathology being a tear in the labrum. Because of the limited ability of the labrum to heal on its own, surgical interventions are often required.5,24
The etiology of FAIS is still under investigation. It was previously believed to be either a congenital disorder or a gradually developing acquired lesion during adolescence.8,25,27-28 However, in the past decade, evidence has emerged suggesting that not all cases of FAIS can be attributed solely to developmental malformation, and functional impingement resulting from abnormal femoral or acetabular version (AV) should not be disregarded.3,21-22 Currently, it is widely acknowledged that a lower femoral version (FV) or femoral retroversion is strongly linked to FAIS, even in the absence of cam- or pincer-type features,5,6,15 while increased femoral anteversion, in contrast, may serve as a protective factor, facilitating normal or near-normal hip mechanics by enabling greater hip internal rotation.7,17,32 Additionally, excessive femoral anteversion has been considered one of the anatomic risk factors that aggravate hip microinstability, which leads to further intra-articular degeneration.18,35 Prior literature has suggested that variations in hip bone structure can lead to compensatory or secondary alterations in the surrounding soft tissues, such as muscles or capsules,4,14,19,39 but no studies have specifically examined the connection between abnormalities in hip version and the morphologic change of the labrum.
In light of this gap, we conducted this study to explore the possible correlations between hip rotational abnormalities and labral size. Our hypothesis was that increased femoral anteversion would be correlated with increased labral size due to soft tissue compensation for anterior instability.
Methods
Patient Selection
The protocol for this study was approved by the ethics committee of our institute. Our researchers retrospectively reviewed the records of patients with a clinical diagnosis of FAIS who underwent hip arthroscopic surgery at our institute between January 2021 and May 2022. All arthroscopic surgeries were performed by the senior author (Y.X.), an experienced surgeon who specializes in sport medicine and hip preservation surgery. All patients had been carefully diagnosed according to their clinical symptoms, physical examinations, and radiological findings including hip joint radiograph, computed tomography (CT), and magnetic resonance imaging (MRI), as described in our previous study. 22 Patients were excluded if they met the following criteria: (1) ipsilateral hip revision surgery history or total hip arthroplasty history; (2) hip traumatic history; (3) severe hip dysplasia, defined as a lateral center-edge angle (LCEA) of <20° (borderline dysplasia [20°≤ LCEA < 25°] was not excluded); (4) developmental hip osteoarthritis (Tönnis grade >1); (5) inadequate radiological evidence available and unmeasurable hip labrum on low-quality MRI; and (6) other hip conditions or diseases such as hip synovitis, Legg-Calve-Perthes disease, slipped capital femoral epiphysis, and femoral head avascular necrosis. Two authors (R.L. and H.D.) carefully reviewed the patients’ information to ensure that it closely aligned with the specific requirements of our study. The patient selection process is shown in Figure 1.

Flowchart of the patient selection process. FAI, femoroacetabular impingement; MRI, magnetic resonance imaging.
Imaging Measurements and Evaluation
We measured the alpha angle on 45° Dunn view and the LCEA on anteroposterior view radiographs. In this study, a cam lesion was defined as an alpha angle of >55° and pincer morphology was defined as an LCEA of >40°. In addition, radiographic signs that indicated acetabular retroversion (eg, the crossover sign and posterior wall sign) as well as coxa profunda and protrusion were also considered to indicate pincer-type femoroacetabular impingement. 2
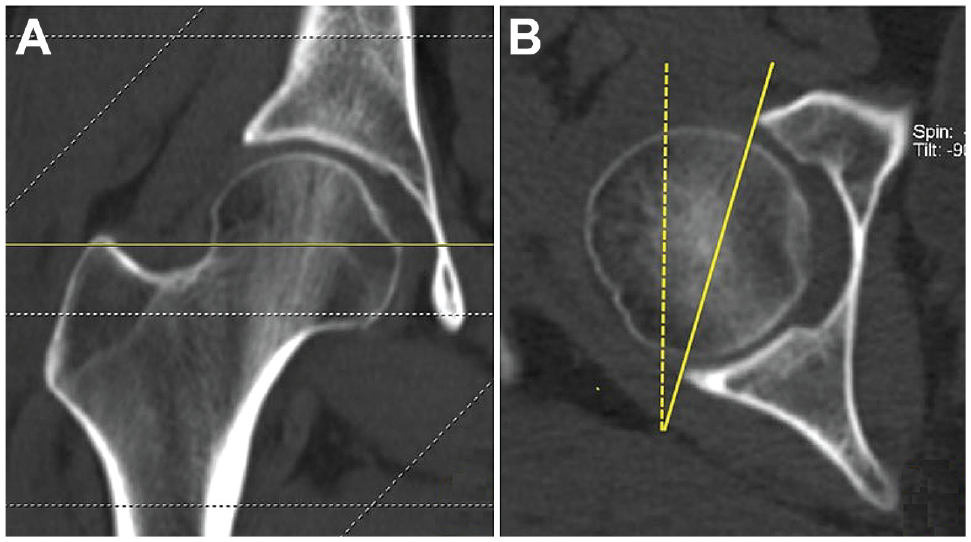
All included patients underwent simultaneous CT scans of both the operated hip and the ipsilateral distal femur, and the FV angle and AV angle were measured using axial CT images. As reported by Schmaranzer et al, 31 the FV angle was defined as the angle formed between the femoral head-neck axis and the posterior femoral condylar axis. In this study, the proximal head-neck axis was marked on the plane where the center of the femoral head and the closest point to the greater trochanter could be observed, according to the method of Lee et al 20 (Figure 2A). The distal condylar axis corresponded to a line connecting the apices of the medial and lateral femoral condyles (Figure 2B).22,31 Once the proximal and distal references were selected, the angles between these 2 axes and a horizontal reference line were recorded (angle 1 and angle 2). Subsequently, we superimposed the individual images. Since the distal axis often deviated from the horizontal due to the nonneutral positioning of the patients’ lower extremities during CT scanning, a horizontal adjustment was made to align the distal axis before the calculation process. For example, as illustrated in Figure 2B, we observed that the right distal femur rotated externally. Thus, the external rotation angle (angle 2) was subtracted by angle 1 to obtain the correct FV angle.

Femoral version (FV) assessment on axial computed tomography images. The solid lines in (A) and (B) indicate the proximal head-neck axis and the distal condylar axis, respectively. The dashed lines indicate horizontal reference lines. The FV angle was calculated as angle 1 – angle 2.
The study patients were categorized into 3 groups based on the FV angle: small (SFV; <10°); moderate (MFV; ≥10° and ≤20°), and large (LFV; >20°).
The measurement of the AV angle was conducted on the axial CT slice that intersected the center of the femoral head, 15 referred to as the “central acetabular version.” As shown in Figure 3, we connected the anterior and posterior edges of the acetabulum, and the angle between this line and a vertical line represented the AV angle. The combined version (CV) angle was determined by summing the FV and AV angles.
(A) The central acetabular version (AV) angle was measured on the transverse slice that crosses the center of the femoral head. (B) The central AV angle was the angle between a line connecting the anterior and posterior acetabular edge (solid line) and a vertical reference line (dashed line).
Labral size was measured via MRI with a 3.0-T scanner (Magnetom Trio with TIM system; Siemens Healthcare), with 5-mm slice thickness. The patients were positioned supine, and separate acquisitions of fat-saturated proton density sequence and T2-weighted sequences were obtained in the axial, coronal, and oblique sagittal planes. The measurement of labral size (ie, labral length and height) was conducted on the sagittal and oblique sagittal proton density sequences, assessing 2 positions: superior (12 o’clock) and anterior (3 o’clock) based on the acetabular clockface model. The labral length was defined as the distance from the chondrolabral junction area to the free edge along the inner surface of the labrum, while the labral height was measured from the cartilage-side labral surface to the adjacent outer surface near the hip capsule (Figure 4). 14

Hip labral length and height measurement at the (A) 12-o’clock and (B) 3-o’clock positions observed on magnetic resonance imaging. Using fat-saturated proton density sequences, the triangular section of the hip labrum can be observed on coronal and oblique sagittal views. The labral length (thickened solid yellow line) is the distance from the chondrolabral junction to the labral free edge along the inner surface of the labrum, and the labral height (thickened solid red line) is the distance from the cartilage-side labral surface to the outside surface near the hip capsule.
Both CT and magnetic resonance images were evaluated by 2 of our authors (G.L. and S.Z.) independently, and the mean value of FV angle, AV angle, CV angle as well as labral size measured by the 2 reviewers was calculated and used for analysis.
Statistical Analysis
Continuous variables were reported as means ± SDs, and categorical variables were reported as numbers (percentages). The Shapiro-Wilk test and F test were used to assess the normality and variance, respectively. Differences between the LFV, MFV, and SFV groups were compared using 1-way analysis of variance, with the least significant difference method used for subsequent multiple comparisons. The interobserver reliability of the imaging measurements between the 2 reviewers was calculated using the intraclass correlation coefficient (ICC), with ICCs of <0.20 indicating slight agreement; 0.21-0.40, fair agreement; 0.41-0.60, moderate agreement; 0.61-0.80, substantial agreement; and >0.80, almost perfect agreement.
Univariate and multivariate linear regression models were used to find the predictive factors for labral length and height at the 3-o’clock and 12-o’clock positions. The Pearson and Spearman rank correlation tests were then used to calculate the association between labral size and the predictive factors. We also performed a comparison of labral size between male and female patients, conducted with the Student t test or Wilcoxon signed-rank test based on the normal distribution of the data. For all comparisons, the threshold for statistical significance was set at P < .05. All data analysis was performed on SPSS statistical software (Version 26.0; IBM Corp), with histograms made via GraphPad Prism (Version 9.0; GraphPad Software Corp).
Results
A total of 180 hips in 180 patients (67 male and 113 female; mean age at surgery, 36.81 ± 10.17 years) satisfied our study criteria and were included. The characteristics of the patients and injuries are listed in Table 1.
Patient and Injury Characteristics (N = 180) a
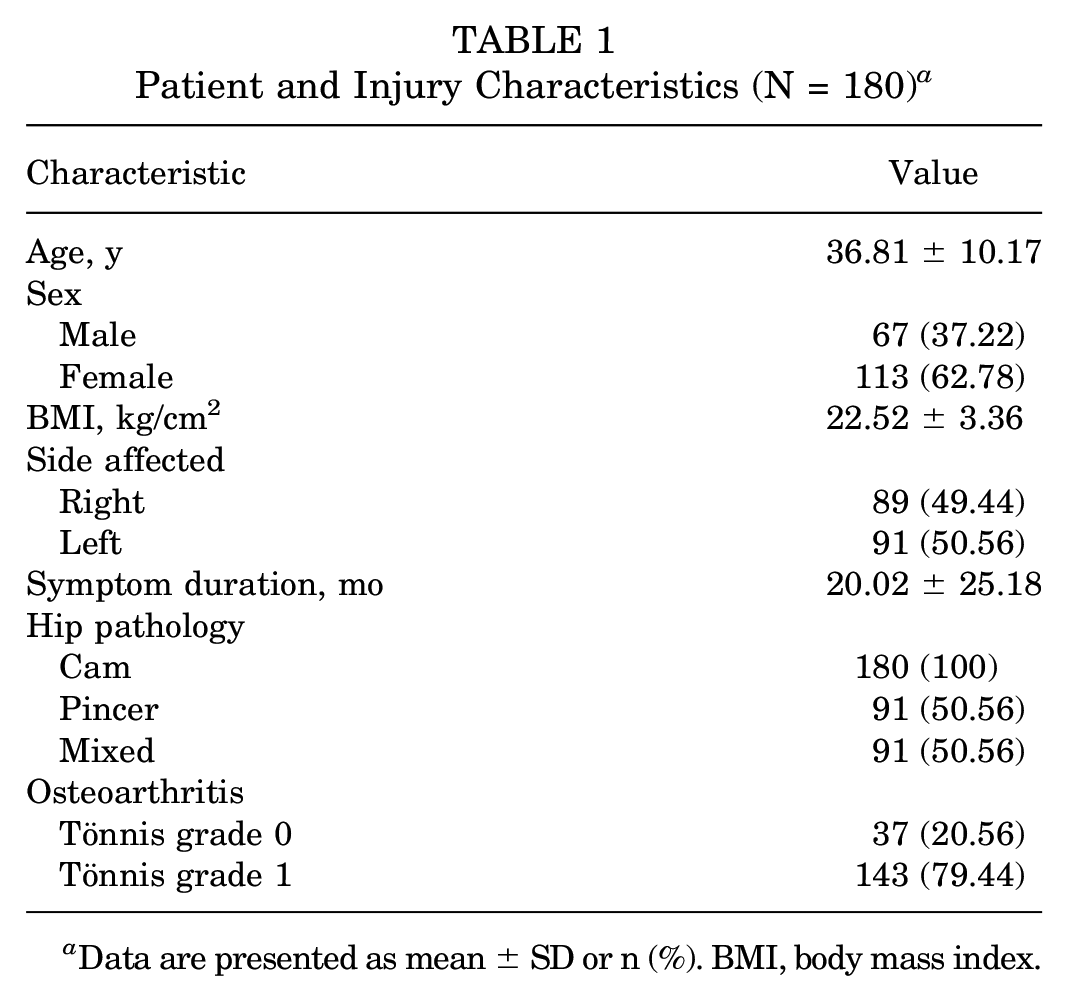
Data are presented as mean ± SD or n (%). BMI, body mass index.
Table 2 presents the values for the various angles and measurements. The labral length was found to be larger than the labral height, measuring 6.41 ± 1.92 mm at the 12-o’clock position and 8.93 ± 2.33 mm at the 3-o’clock position. The interrater reliability for labral size and version measurements are listed in Table 3. The ICCs for each parameter were >0.80, indicating almost perfect agreement between the 2 reviewers.
Radiographic Parameters a

Data are presented as mean ± SD. AV, acetabular version; CV, combined version; FV, femoral version; LCEA, lateral center-edge angle.
Interobserver Reliability of the Labral Size and Version Measurements a

Data are presented as intraclass correlation coefficient (95% CI). Values <0.20 indicated slight agreement; 0.21-0.40, fair agreement; 0.41-0.60, moderate agreement; 0.61-0.80, substantial agreement; >0.80, almost perfect agreement. AV, acetabular version; CV, combined version; FV, femoral version.
The results of the linear regression analysis are provided in Table 4. Predictive factors for labral length at the 3-o’clock position were FV angle (β = 0.298; P = .02), sex (β = −0.302; P < .001), and age (β = −0.169; P = .016), and predictive factors for labral length at the 12-o’clock position were LCEA (β = −0.208; P = .005) and age (β = −0.186; P = .011). The correlation coefficients, R2 values, and P values are listed in Table 5. FV angle was positively correlated with labral length at the 3-o’clock position (r = 0.267; R2 = 0.071; P < .001), while age and female sex exhibited a negative correlation with labral length at 3 o’clock (age: r = −0.222, R2 = 0.049, P = .003; female sex: r = −0.202, R2 = 0.086, P = .006). LCEA and age showed negative correlations with labral length at the 12-o’clock position (LCEA: r = −0.227, R2 = 0.051, P = .002; age: r = −0.205, R2 = 0.043, P = .006). No significant correlations were found between labral height and the factors listed in Table 4.
Linear Regression Analysis for Labral Length at the 3-O’Clock and 12-O’Clock Positions a

Dashes indicate areas not applicable. Boldface P values indicate statistical significance (P < .05). AV, acetabular version; BMI, body mass index; CV, combined version; FV, femoral version; LCEA, lateral center-edge angle.
Correlations Between Labral Length and Predictive Factors a

Boldface P values indicate statistical significance (P < .05). FV, femoral version; LCEA, lateral center-edge angle.
Pearson rank coefficient.
Spearman rank coefficient.
According to our grouping standard, we categorized 49 hips into the LFV group, 65 hips into the MFV group, and 66 hips into the SFV group. The group comparison revealed a significant difference in labral length at the 3-o’clock position (9.85 ± 2.28, 8.89 ± 2.44, and 8.30 ± 2.05 mm in the LFV, MFV, and SFV groups, respectively), in which we found that the mean labral length at 3 o’clock in the LFV group was significantly larger compared with the other 2 groups (LFV vs MFV, P = .027; LFV vs SFV, P < .001) (Figure 5).
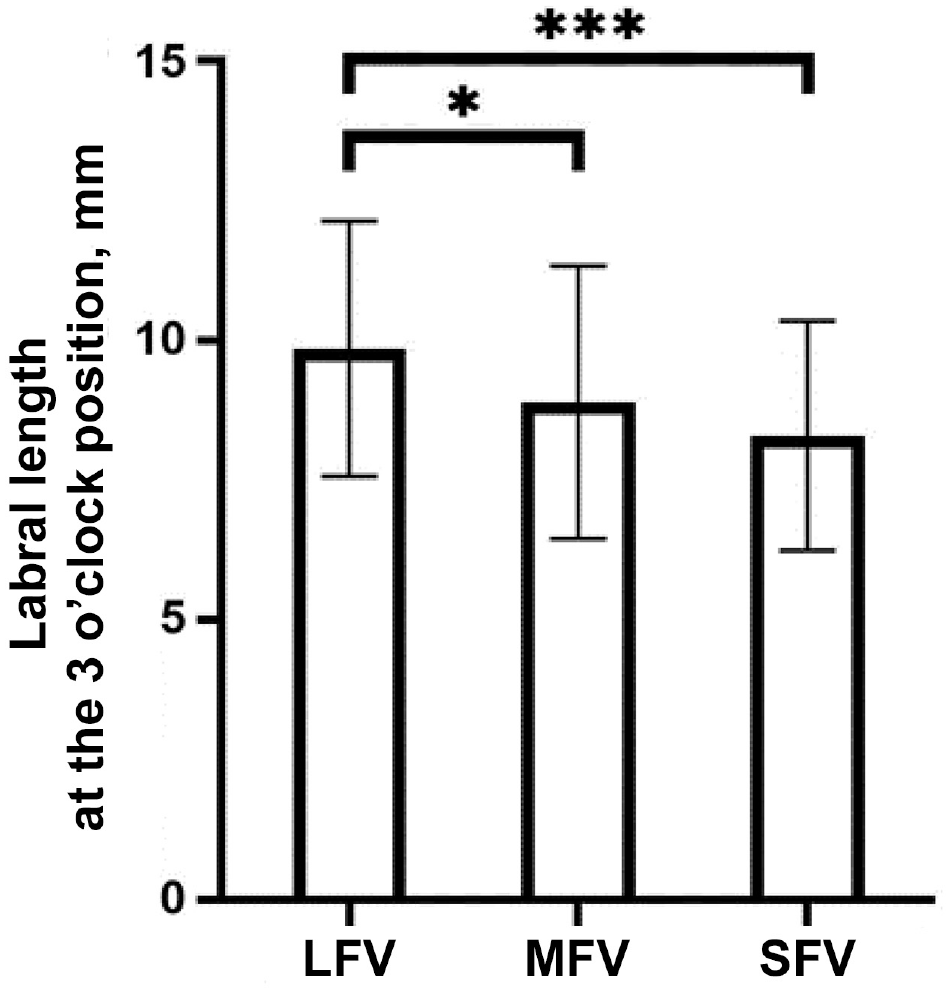
Labral length at the 3-o’clock position between the large, moderate, and small femoral version (LFV, MFV, and SFV, respectively) groups. Statistically significant difference between groups: *P < .05; ***P < .001.
Regarding the comparison of labral size according to patient sex, labral height and length at both the 12- and the 3-o’clock positions were greater in male patients than in female patients, although the values reached statistical significance for just 2 of the variables: labral height at the 12-o’clock position (4.86 ± 0.95 mm for men vs 4.48 ± 0.90 mm for women; P = .008) and labral length at the 3-o’clock position (9.82 ± 2.21 mm for men vs 8.41 ± 2.25 mm for women; P < .001) (Table 6).
Labral Size According to Sex a

Data are presented as mean ± SD. Boldface P values indicate statistically significant difference between groups (P < .05).
Discussion
The present study showed some meaningful results: (1) Patients with increasing femoral anteversion had a larger anterior labral length. (2) Male patients had greater labral size than female patients, especially labral height at the 12-o’clock position and labral length at the 3-o’clock position. (3) Age was also a predictive factor that influenced labral length. In this study, patients’ labral length was found to gradually reduce as their age increased. (4) There was a negative correlation between LCEA and labral length at the 12-o’clock position, which corresponds to the findings of Garabekyan et al. 14
The structural variations of the hip have a definite impact on the surrounding soft tissues. In the case of dysplastic hips, studies by Kuroda et al 19 and Garabekyan et al 14 revealed that patients with hip dysplasia tend to have larger anterior and lateral labral length. On the other hand, Yang et al 39 and Bai et al 4 reported a correlation between hip bony morphology and hip capsular thickness. To the best of our knowledge, this is the first study to specifically investigate the relationship between hip version abnormalities and labral size. The reliability of assessing hip labral size using MRI was previously established in a clinical study conducted by Kaplan et al. 16 Although Comfort et al 9 demonstrated that the actual labral length is smaller than what is observed on MRI, MRI remains the most commonly utilized noninvasive technique for in vitro measurement of the hip labrum. Previous studies have presented 2 different definitions for labral length (also known as labral width). One method, which we adopted in our current study, involves measuring the distance from the acetabular rim to the free edge of the labrum along its inner surface. 14 Another approach measures the distance along the outer surface of the labrum. 16 It is challenging to determine which method is more representative or sensitive. Ultimately, we chose the former method because we believed that the inner surface of the labrum, being in close proximity to the femoral head, better reflects its functional role.
Our findings were partially consistent with our initial hypothesis that femoral anteversion angle would positively influence the anterior labral length, although the correlation intensity was relatively weak. One possible explanation is that the anterior labrum may increase its length as a compensatory mechanism to counteract the potential instability caused by a larger FV, thereby preserving the suction seal effect. As described by Dwyer and colleagues, 11 in weightbearing postures, hip flexion and internal rotation can alleviate the resistance of intra-articular fluid flow from the central compartment to the peripheral compartment, which can lead to joint degeneration. Individuals with a larger FV have been shown to exhibit compensatory hip internal rotation. 36 Taking this evidence into account, we hypothesized that the change in anterior labral length is another innate adjustment that helps restore articular fluid, reduce hip contact forces, and protect the joint cartilage.
Patients with FAIS and a hypertrophic labrum may experience additional benefits compared with their counterparts after hip arthroscopic surgery. For example, Liu et al 23 reported that patients with FAIS with a hypertrophic labrum achieved more satisfactory patient-reported outcomes after arthroscopic labral repair or reconstruction over 2-year follow-up, highlighting the importance of considering preoperative labral volume. Based on these findings, we speculated that patients with FAIS with a larger FV are more likely to experience favorable clinical outcomes, despite previous researchers’ not consistently demonstrating a significant impact of femoral anteversion.32,33,37-38 Notably, according to Ejnisman et al, 12 hips exhibiting an FV angle of >15° were 2.2 times more prone to experiencing a labral tear at the 3-o’clock position, possibly attributed to an overtightened psoas tendon resulting from increased femoral anteversion. This suggests that while femoral anteversion may affect various surrounding soft tissues differently, not all changes can be regarded as beneficial; on the contrary, some alterations may pose a risk and contribute to secondary lesions to some extent.
Both labral length and labral height are important factors in maintaining hip stabilization. 34 However, in our study, we only observed a correlation between labral length at 3 o’clock and FV angle. Surprisingly, no significant differences or correlations were found when considering labral height. It was also unexpected that there was no correlation between AV, CV, and hip labral size. Theoretically, changes in labral morphology are expected to be influenced by the orientation of both the femoral head and the acetabulum, suggesting that isolated changes in FV may be insufficient. In a study by Curly et al, 10 a mild correlation was found between acetabular anteversion and anterior labral length (r = 0.343). However, in our current study, neither AV angle nor CV angle was a predictive factor for larger labral size.
We also observed a negative correlation between the LCEA and the labral length at 12 o’clock. This finding is in keeping with earlier results. Garabekyan et al 14 found a strong negative correlation between lateral acetabular coverage and lateral labral length (r = −0.706; P < .001). They predicted that for every degree reduction in LCEA, the length of the lateral labrum would increase by 0.14 mm. In our study, we similarly found a weak but significant negative correlation (r = −0.227; P = .002). The reason why our r value was smaller may be due to our study exclusion criterion of patients with hip dysplasia with an LCEA of <20°. This exclusion may have weakened the correlation to some extent. It appears that the compensatory effect of the labrum is more apparent when there is insufficient acetabular coverage rather than excessive coverage.
Last, we observed sex- and age-related differences in hip labral size. The labrum of male patients was generally larger compared with that of their female counterparts. Given that the alpha angle in male patients is usually higher than in female patients, indicating a higher degree of cam lesions, sex-based differences may partially explain why male patients have larger labral tear size. 30 Another finding was that the hip labrum was predicted to be reduced as patients aged, and age-related atrophy mainly happened on labral length, which was also observed by Abe et al. 1
In terms of clinical implications, we recommend that surgeons carefully evaluate patients for any abnormalities in version and consider the compensatory effect of the acetabular labrum before performing hip arthroscopic surgeries. This is particularly important when determining graft size during labral reconstruction. Based on the findings of the current study, patients with increased femoral anteversion may require a wider allograft or autograft to achieve optimal clinical outcomes.
Limitations
This study is not without limitations. First, we did not match covariates such as age, sex, or BMI when we compared the labral size between the LFV, MFV, and SFV groups. We actually found patients with LFV angle (>20°) were younger than those in the other 2 groups. Thus, the significant difference in labral length may be exaggerated by age. Second, we only evaluated the labral size at the 12-o’clock and 3-o’clock positions, and we did not use any anatomic landmarks when identifying the reference planes we used, which may reduce the follow-up measuring accuracy. Third, although both CT-based and MRI-based femoral torsion measurements showed high agreement and reproductivity as mentioned by Schmaranzer et al, 31 there is still controversy concerning which method is the most accurate when measuring FV angle. Additionally, to date, there has been no medical brace available that can effectively immobilize a patient’s lower extremities in a completely neutral position when undergoing CT examination. As a result, all the methods may introduce certain inaccuracies, necessitating further refinement and improvement. Finally, future studies should focus more on the cross-sectional area of the hip labrum rather than length or height only.
Conclusion
Our study demonstrated that patients with FAIS who had a higher femoral anteversion angle were more likely to have a larger anterior labral length. Increased femoral anteversion, decreased LCEA, male sex, and younger age were all significantly associated with longer hip labral length.
Footnotes
Final revision submitted December 10, 2023; accepted February 12, 2024
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding was received from Beijing Natural Science Foundation (Z200003) and the Key Clinical Project of Peking University Third Hospital (BYSYZD2019003). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Peking University Third Hospital (ref No. M2019193).