
Abstract
Background:
Increased attention has been directed toward the ligamentum teres (LT) and its association with acetabular coverage, labral pathology, and hip microinstability; however, few studies have evaluated whether LT pathology influences the rate of clinically significant outcome improvement after hip arthroscopy.
Purpose:
To determine if patients with femoroacetabular impingement syndrome (FAIS) undergoing labral repair and concomitant LT debridement achieve outcomes similar to patients without LT pathology undergoing labral repair.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We conducted a retrospective review of a prospectively maintained multicenter database for hip arthroscopy. Included were patients with FAIS who underwent primary labral repair and who had preoperative and minimum 2-year postoperative outcome scores. Patients diagnosed with concomitant partial LT tear were identified and matched 1:3 according to age, sex, and body mass index (BMI) to patients without LT pathology. The following clinical outcomes were compared between groups: modified Harris Hip Score, Hip Outcome Score–Activities of Daily Living, Hip Outcome Score–Sport Subscale, International Hip Outcome Tool, and visual analog scale for pain and satisfaction. Achievement of the minimal clinically important difference and patient acceptable symptomatic state was also compared between groups.
Results:
This study included 124 patients with FAIS with labral tear and concomitant partial LT tear and 372 patients with labral tear and no LT pathology. The age, BMI, and sex of the matched cohort were 38.0 ± 12.0 years (mean ± SD), 24.3 ± 3.6 kg/m2, and 62.0% female, respectively. No significant difference in age, BMI, sex, workers’ compensation status, or duration of pain was observed at baseline. Analysis of radiographic parameters indicated that patients who underwent isolated labral repair had a lower preoperative Tönnis angle (4.8° ± 4.4° vs 6.3° ± 5.4°; P = .006). There were no significant differences between groups on any pre- or postoperative outcome measure, and there were no significant differences in the proportion of patients who achieved the minimal clinically important difference or patient acceptable symptomatic state on any outcome measure.
Conclusion:
Patients with labral tear and concomitant partial LT tear experienced similar preoperative scores and achieved similar outcomes as patients with isolated labral tears after hip arthroscopy.
Since its initial description in 100 BC the ligamentum teres (LT) has historically been considered a vestigial structure and has frequently been excised during reductions of the hip for developmental dysplasia or during open surgical hip dislocation procedures. 28 However, recent studies have suggested that the LT may confer biomechanical and neurological properties to the hip. The LT is innervated by the obturator nerve, which can explain knee pain referred from the hip. Additionally, proprioceptive and nociceptive roles of the ligament may be explained by the presence of mechanoreceptors and free nerve endings. 24 Hypothetically, these free nerve endings could play a role in a reflex arc as the hip reaches extremes of range of motion that act to stabilize the hip joint and prevent chondrolabral damage. In torn and degenerative LTs, the enthesis loses its organized structure, and fibrocartilage develops in the midsubstance of the ligament, leading to a decreased ability to accommodate mechanical forces, which may also contribute to hip pain. 29
Prior studies have reported that risk factors for LT tears include microinstability of the hip, 13 reduced lateral coverage, 8 acetabular retroversion, 13 and younger age 13 and may occur secondary to repetitive stretching 13 or trauma. 32 Unfortunately, it can be difficult to determine if LT tears are a primary or secondary cause of pain, but a history of pediatric hip conditions, trauma, participation in high-impact sporting activities, or a history of surgery may be helpful. 28 Pain can be described as a dull, deep groin pain but may refer to the medial thigh or knee because of obturator nerve innervation. 25 Catching and popping may occur because of a complete tear and cyclops lesion, but this sensation can be present with other intra-articular pathology, such as labral tears or chondral flaps. 28 In terms of LT pathology and microinstability, Beighton signs of hyperlaxity as well as global stability of the hip should be tested, with emphasis placed on the anterior and posterior shuck tests. 28 O’Donnell et al 22 described a test for LT tears, with the hip at 70° of flexion and 30° of abduction and the knee at 90° of flexion. The hip is brought through full internal and external rotation range of motion. A positive test is one in which patients experience pain in one direction and relief in the other. This test places the ligament at maximal tension with the femoral head centered in the acetabulum while minimizing impingement, and it had a sensitivity of 90% and a specificity of 85% in 75 patients undergoing hip arthroscopy.
Nonoperative treatment of LT tears consists of activity modification, core and dynamic hip strengthening, anti-inflammatory medications, and intra-articular injections. Operative treatment may consist of debridement of the tear and coexisting synovitis, central acetabular osteophyte resection, or reconstruction, with comprehensive treatment of other intra-articular hip pathology (eg, labral tears, chondral defects, and femoroacetabular impingement syndrome [FAIS]) and capsular repair or plication for microinstability. 16 Although several authors have described LT debridement as the operative treatment of choice for most tears, these studies are limited.
The purpose of this study was to determine whether patients with FAIS undergoing labral repair and concomitant LT debridement achieve similar outcomes to patients undergoing labral repair without LT pathology. We hypothesized that patients undergoing concomitant labral repair and LT debridement would achieve worse outcomes than patients undergoing labral repair alone.
Methods
Patient Selection
A matched-control study design was used to determine the effect of partial LT tear on minimum 2-year outcomes in patients with FAIS and labral tearing. Patients were retrospectively selected from a prospectively maintained database from a multicenter study group composed of 7 hip arthroscopic surgeons from 7 medical centers throughout the United States. All participating surgeons had at least 9 years of experience in hip arthroscopy and performed a minimum of 100 cases per year. All surgeons had fellowship training in hip arthroscopy, except for 2 surgeons who began their practices before the establishment of formal hip arthroscopy fellowships. Before data collection, all surgeons agreed on a collection of characteristics, diagnostic imaging, physical examination, patient-reported outcomes (PROs), and intraoperative records. In addition, the surgeons and supporting research staff met quarterly to discuss the inevitable limitations of multicenter data collection and routinely worked to minimize differences in preoperative diagnostics, physical examination findings, 12 intraoperative grading systems, 9 rehabilitation protocol, and other shortcomings of multicenter studies. Patient-specific data were collected using a commercial data collection service (Outcomes Based Electronic Research Database, Universal Research Solutions).
Institutional review board approval was obtained to review the deidentified encrypted data set. Inclusion criteria were (1) patients undergoing hip arthroscopy for labral repair and concomitant partial LT tear treated by partial debridement, (2) clinical and radiographic diagnosis of symptomatic FAIS, (3) failure of nonoperative management (oral anti-inflammatories, physical therapy, intra-articular cortisone injection), and (4) completion of minimum 2-year postoperative outcome scores. Patients diagnosed with labral tear and concomitant partial LT tear were included. Exclusion criteria were revision surgery, labral reconstruction, lateral center-edge angle (LCEA) <20°, concomitant gluteus medius/minimus repair, core decompression, workers’ compensation status, osteoarthritis (Tönnis grade >1), and no specified body mass index (BMI).
Patients with FAIS with labral tear and concomitant partial LT tear were identified and matched 1:3 according to age, sex, and BMI to patients without LT pathology. Age, BMI, and sex for the entire cohort before matching were 33.7 ± 12.4 years (mean ± SD), 24.4 ± 4.2 kg/m2, and 66.1% female, respectively. Matching was performed in R (Version 1.2.5042, R Core Team) with implementation of Mahalanobis distance.
Radiographic Parameters, Procedures Performed, and Intraoperative Findings
Radiographic parameters included routine clinical radiographs: anteroposterior alpha angle, 45° Dunn lateral view alpha angle, LCEA, anterior center-edge angle, and Tönnis angle. The intraoperative procedures performed for each patient were also recorded. Intraoperative labral pathology included degeneration and/or calcification of >50% of the labrum (binary), labral bruising (binary), and complexity of labral tearing. The complexity of tearing grading was based on the following criteria: mild, stable rim configuration with some fraying of the substance; moderate, either rim stability and intrasubstance damage greater than fraying but still <50% of the substance at the tear site or instability at the rim with intrasubstance damage <50% of the substance at the tear site; or severe, complex multiplane injury >50% of substance at the tear site with or without stability at the rim. Acetabular articular cartilage damage was assessed and graded as previously described by Beck et al. 2
Clinical Outcomes
Characteristic data were collected from patients, including age, sex, BMI, tobacco use, workers’ compensation status, and duration of symptoms. All patients completed at least 1 pre- and postoperative hip-specific PRO measure, including the modified Harris Hip Score (mHHS), 4 Hip Outcome Score–Activities of Daily Living (HOS-ADL), 19 Hip Outcome Score–Sport Subscale (HOS-SS), 20 International Hip Outcome Tool (iHOT-12), 11 and visual analog scale (VAS) for pain and satisfaction. The minimal clinically important difference (MCID) and the patient acceptable symptomatic state (PASS) for the HOS-ADL, HOS-SS, mHHS, iHOT-12, and VAS for pain and satisfaction were analyzed. The MCID was calculated based on one-half of the standard deviation of the difference between the pre- and postoperative scores for each measure: mHHS (threshold, 9.09), HOS-ADL (8.85), HOS-SS (13.92), and iHOT-12 (12.51). The PASS was based on previous literature: mHHS (threshold, 74), 5 HOS-ADL (87), 5 HOS-SS (75), 5 iHOT-12 (63), 21 and VAS for pain (21.6). 1
Surgical Technique
An interportal capsulotomy was performed, and the capsulolabral recess was reflected to allow for visualization of the acetabular labrum. Central compartment procedures were performed as indicated: acetabular rim trimming, acetabuloplasty, chondral lesion debridement to stable margins, and labral repair. Patients in the partial LT tear group were identified intraoperatively under direct arthroscopic visualization and underwent LT debridement of the degenerative tissue with an arthroscopic shaver and flexible electrocautery (Figure 1). No patients underwent complete resection of the LT. The appearance of the acetabular was addressed, and a healthy bone bleed was created using an arthroscopic bur. The labrum was fixed using a suture passing device. In cases of extensive cam deformity, a T-capsulotomy was performed to access the peripheral compartment. A comprehensive cam resection was performed to confirm complete resection of abnormal bony appearance. A combination of intraoperative fluoroscopy as well as a dynamic hip examination was performed to ensure complete removal of cam impingement. A suture-shuttling device was used to close the T-capsulotomy, starting at the base of the vertical portion and followed by the interportal segment.

Arthroscopic view from the viewing portal displaying a ligamentum teres (LT) partial tear and adjacent femoral head (FH).
Statistical Analysis
The Shapiro-Wilk test of normality was used to assess data distribution for all continuous variables. The Levene statistic was used to assess homogeneity of variances. Continuous variables were analyzed with an independent-sample t test or Mann-Whitney U test for parametric and nonparametric data, respectively. Continuous variables were reported as means and standard deviations. Categorical variables were analyzed by χ2 analysis. P values <.05 were considered statistically significant. All statistical analysis was performed using SPSS (Version 26, IBM).
An a priori power analysis using a medium effect size (Cohen F = 0.5), alpha probability of 0.05, power of 0.80, and a 1:3 ratio between groups indicated that 170 patients were required to achieve appropriate power.
Results
Characteristics
Of the 2530 patients undergoing hip arthroscopy, 177 underwent labral repair and concomitant partial LT tear debridement. Fourteen patients did not meet inclusion criteria, leaving 124 patients diagnosed with FAIS, labral tearing, and partial LT tear with minimum 2-year follow-up. These patients were matched to 372 patients with FAIS with labral tearing and no LT pathology. The mean follow-up time was 24.5 ± 3.0 months. Analysis of baseline patient characteristics revealed no significant differences between the groups in age, BMI, sex, smoking history, duration of pain, or FAI type (Table 1). The procedures performed on the cohort are summarized in Table 2.
Baseline Patient Characteristics a

a Results are reported as mean ± SD or percentage. BMI, body mass index; FAI, femoroacetabular impingement; LT, ligamentum teres.
Procedures Performed a

a Data are reported as percentages. LT, ligamentum teres.
Radiographic Parameters, Procedures Performed, and Intraoperative Findings
Analysis of preoperative radiographic parameters indicated that patients undergoing isolated labral repair had a lower Tönnis angle (4.8° ± 4.4° vs 6.3° ± 5.4°; P = .006) (Table 3). There were no differences in anteroposterior alpha angle, 45° Dunn alpha angle, anterior center-edge angle, or LCEA. Analysis of labral characteristics revealed no significant differences between the 2 groups differences in frequency of labral degeneration, bruising, or complexity of tearing (Table 4). Analysis of the frequency of acetabular articular cartilage damage revealed no significant differences between groups.
Preoperative Radiographic Parameters a

a Data are reported as degrees (mean ± SD). Bold P value indicates statistically significant difference between groups (P < .05). AP, anteroposterior; LT, ligamentum teres.
Intraoperative Findings a
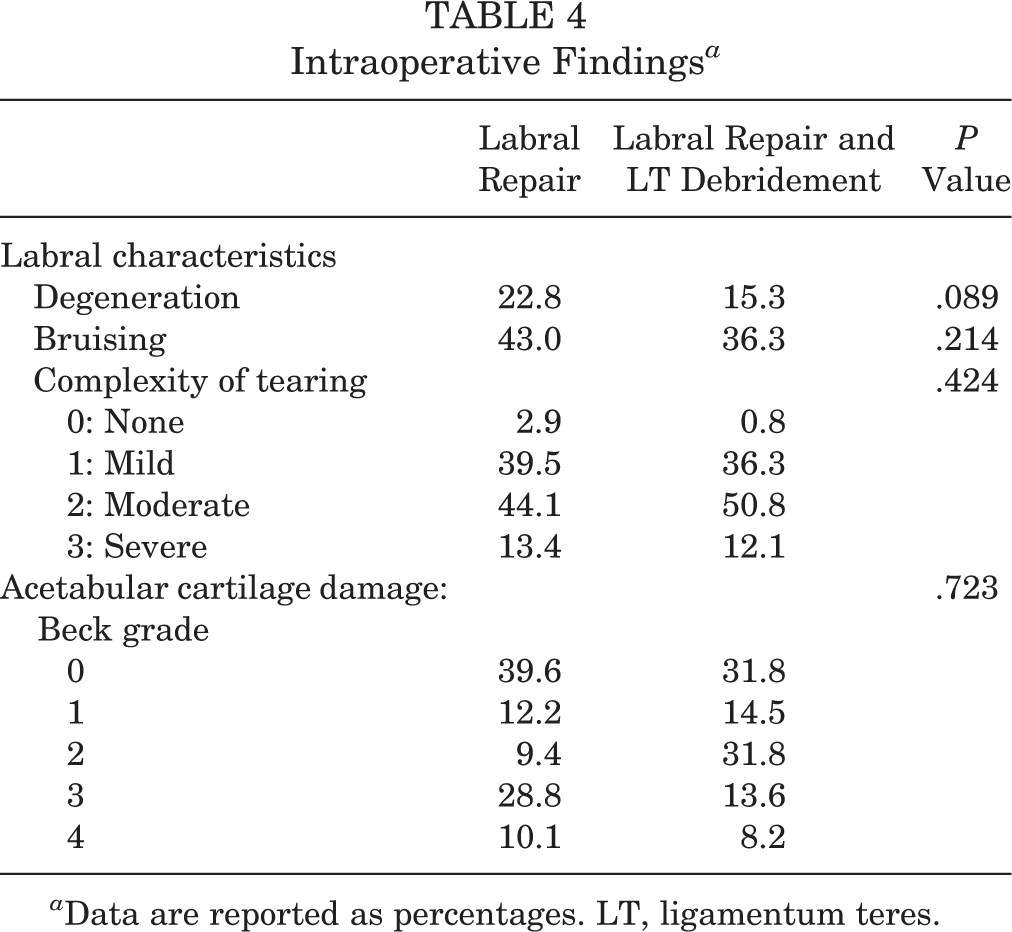
a Data are reported as percentages. LT, ligamentum teres.
Clinical Outcomes
Analysis of PROs revealed no significant differences in mHHS, HOS-ADL, HOS-SS, iHOT-12, and VAS for pain or satisfaction at baseline or latest follow-up (Table 5). Subsequently, the proportion of patients achieving the MCID and the PASS at latest follow-up were also analyzed. This analysis revealed no differences in the rate of MCID or PASS achievement for any outcome measure (Table 6).
Pre- and Postoperative Outcomes a

a Data are reported as mean ± SD. HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sports Subscale; iHOT-12, International Hip Outcome Tool; LT, ligamentum teres; mHHS, modified Harris Hip Score; VAS, visual analog scale.
Rates of MCID and PASS a

a Data are reported as percentages. HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sports Subscale; iHOT-12, international Hip Outcome Tool; LT, ligamentum teres; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; PASS, patient acceptable symptomatic state; VAS, visual analog scale.
b MCID was calculated by one-half the standard deviation of the difference between pre- and postoperative scores for the entire cohort.
Association Between Acetabular Coverage and LT Debridement
In patients undergoing LT debridement, the association between acetabular coverage quantified by the LCEA and the achievement of clinically significant outcome improvement was analyzed. Bivariate correlation analyses indicated no correlation between LCEA and achievement of MCID or PASS in patients undergoing LT debridement for any clinical outcome measure (P > .05) (Table 7).
Correlation Between LCEA and MCID/PASS Achievement in Patients Who Underwent LT Debridement a

a HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sports Subscale; iHOT-12, international Hip Outcome Tool; LT, ligamentum teres; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; PASS, patient acceptable symptomatic state; VAS, visual analog scale.
Discussion
The present study demonstrated no difference in PROs or achievement of the MCID or PASS when comparing patients undergoing labral repair with LT debridement versus labral repair alone. This study utilized a large, prospectively collected database of patients indicated for hip arthroscopy at different centers, managed by 7 fellowship-trained hip arthroscopic surgeons and showed that patients with partial tears of the LT can expect to have similar outcomes as those with isolated labral pathology. These findings may help with patient counseling pre- and postoperatively and may guide intraoperative decision-making. Smaller, single-institution studies support our findings. Similarly, Pergaminelis et al 23 reported on 37 hips that underwent radiofrequency debridement of the LT tears over a 2-year period. The authors found statistically significant improvement in the iHOT-33 score, with all patients achieving the MCID, indicating that debridement of LT tears can result in good midterm outcomes.
Understanding of the LT and its function continues to improve. Three cadaveric studies have examined the stabilizing role of the LT in hips with conserved capsules in the squatting position, with 2 studies 14,18 finding this stabilizing force to be substantial and 1 study 31 reporting only a secondary stabilizing effect. In the squat position, the iliofemoral ligament, which typically controls external rotation in this position, is lax. Martin et al 18 proposed that the LT stabilizes the femoral head at extremes of range of motion. In hip flexion and abduction, the authors believed that the LT prevents inferior subluxation, while in internal and external rotation, the LT prevents posterior and anterior subluxation, respectively.
Furthermore, several authors have attempted to classify types of LT tear, as well as subsequent management based on tear severity. In 1997 Gray and Villar 10 first classified LT tears in 20 patients treated arthroscopically. The authors described 3 main cases: complete tears as a result of major trauma (dislocation) or prior surgery, partial tear clinically represented by long-standing indolent hip pain, and degenerative rupture with underlying osteoarthritis. Botser et al 3 expanded on this classification in 2011. This study reviewed 558 surgical cases and revealed LT tears in 284. Tears were classified by the Gray and Villar system and by a new descriptive method in which grade 0 was no tear; grade 1, <50% tear; grade 2, >50% tear; and grade 3, 100% tear. The majority of tears were grade 1 or 2 (91%). This study also showed that patients with LT tears were significantly older and had worse preoperative functional scores. There was an intraoperative association with larger labral tear size and amount of chondral damage as well, which was not seen in the present study. Postoperative PROs were not reported. In the present study, we did not find any relationship between extent of labral tear or chondral damage and LT tears, indicating that surgeons should remain suspicious of LT tear regardless of the state of the labrum and acetabular cartilage.
Once an LT tear is identified, either pre- or intraoperatively, there may be disagreement among hip arthroscopic surgeons regarding its optimal management. Portho Salas and O’Donnell 27 proposed a new classification system in 2015, expanding on that of Gray and Villar 10 and Botser et al, 3 which not only described LT pathology but offered guidance regarding its management. Classification was performed arthroscopically at the time of surgery and is defined in Table 8. For types 1 through 5, the authors recommend debridement with the treatment of associated pathology as needed, while reconstruction may be considered in the case of type 6 tear with ongoing hip instability. Unfortunately, the authors did not report on PROs when utilizing this treatment algorithm; therefore, it is unable to be validated. However, it does clarify that debridement is currently the mainstay of treatment in the management of LT tears. Our study indicates that debridement of LT tears does not have a negative effect on PROs or achievement of a clinically significant outcome at 2 years after surgery.
Ligamentum Teres Tear Classification a
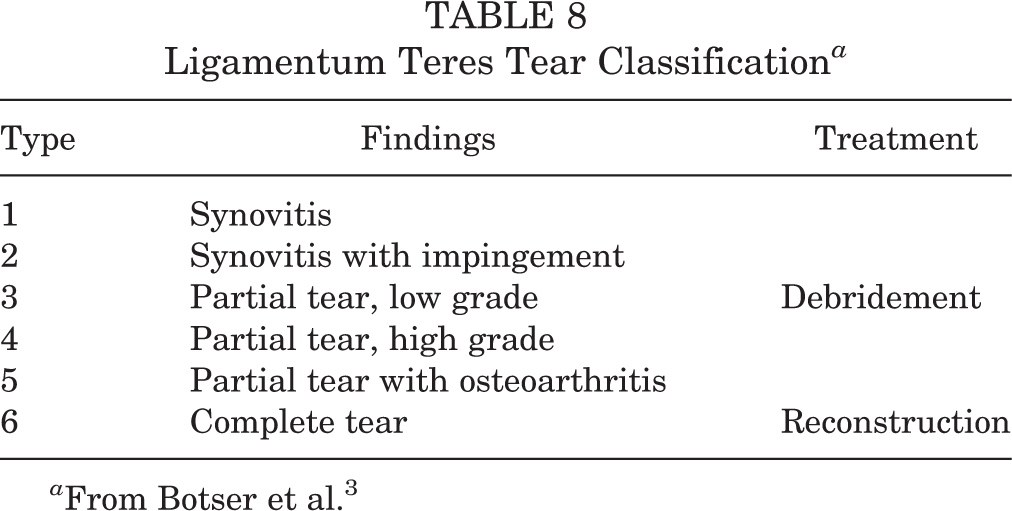
a From Botser et al. 3
For patients with LT tears and concomitant FAIS, studies have revealed associations with particular chondral wear patterns. One study 15 showed increased inferior medial acetabular and apical femoral head damage, and another study 16 demonstrated an association between central acetabular osteophytes and an increase in femoral cartilage wear and LT tears when compared with a matched control group. At a minimum 2-year follow-up of patients undergoing hip arthroscopy for FAIS, Maldonado et al 17 reported that patients with completely torn LT had a threefold higher rate of conversion to total hip arthroplasty in a matched-control study. These 2 studies are in contrast to our study, which did not find a difference in 2-year outcomes between patients with and without LT tears. However, the present study included patients treated for partial LT tears, whereas Maldonado et al treated patients with complete LT tears. The present study cannot show whether the LT debridement was actually necessary or beneficial—only that it did not seem to lead to inferior results at 2-year midterm follow-up.
Unfortunately, prior literature on the long-term outcomes after LT debridement are limited. Haviv and O’Donnell 13 reported a 17% rate of patients requiring revision debridement owing to ongoing symptomatic hip pain and instability. Patients with persistent symptoms of microinstability after LT debridement may be considered candidates for LT reconstruction, although clear indications for this procedure remain controversial. First described in 2011 by Simpson et al, 30 this procedure is currently being performed by very few centers, and there is a lack of high-quality evidence to support its use. 6,26 In a systematic review by de Sa et al 7 of case series and reports of patients undergoing debridement or reconstruction, both groups had significantly improved PROs, pain, and return to sports. The authors concluded that debridement should be indicated for partial-thickness tears, while reconstruction is indicated for complete tears that cause instability or failed previous debridement. To our knowledge, only 2 case series with short-term follow-up have been published on the outcomes of LT reconstruction. Chandrasekaran et al 6 examined 4 hips in 3 patients with Ehlers-Danlos syndrome. Of the 4 hips, 3 experienced significant improvement in mHHS, and 1 patient who underwent bilateral procedures had graft failure on 1 side with continued worsening in pain and function. Philippon et al 26 reported on 4 patients, with 3 citing notable improvement and the other going on to total hip arthroplasty. Future studies should strive to provide outcomes of LT treatment to better delineate the best indications and treatments for patients with this pathology. Despite the limited literature present for reconstruction, our study found that in a large multicenter cohort, patients who underwent concomitant LT debridement at the time of arthroscopic management of FAIS and labral tear can expect outcomes equivalent to a matched cohort without LT tear.
Limitations
This study is not without limitations. The multicenter group did not evaluate all patients’ magnetic resonance scans for LT pathology. In addition, physical examination findings to evaluate patients for microinstability were not reported in the present study. Partial LT tear was assessed as a binary measure as opposed to a validated classification system. Therefore, the partial LT tear group may include a range of tear severity. Additionally, this was a multicenter study of 7 high-volume hip arthroscopic surgeons with different preferences in treatment for LT tears and FAIS. There was no agreed-on standard of care for LT debridement in the primary hip arthroscopy setting, despite classification systems incorporating treatment recommendations. Next, while capsular management was recorded for all patients, these data did not include information regarding capsular advancement.
This study failed to address the surgeon’s role in outcomes. In addition, this 2-year follow-up did not capture mid- and long-term follow-up outcomes and did not report complications or revision surgery, such as postoperative microinstability, revision hip arthroscopy, LT reconstruction, conversion to total hip arthroplasty, or hip resurfacing. Also, our study was unable to clearly distinguish whether LT debridement was necessary or whether the LT was the patients’ primary pain generator; the study solely demonstrates that outcomes after LT debridement were not inferior to patients who were not indicated for LT debridement. Moreover, patients in the partial LT tear group were treated for concomitant labral repair. Therefore, the influence of partial LT tear debridement cannot be directly associated with improvement in pain and functional outcomes. Future studies are warranted to compare patients with partial LT tear managed with partial debridement and patients with partial LT tear without treatment. Last, although data from this study group were collected prospectively, the present study was still subject to the weaknesses of retrospective review.
Conclusion
Patients with labral tear and concomitant partial LT tear experienced similar preoperative scores and achieved similar outcomes as patients with isolated labral tears after hip arthroscopy.
Footnotes
Final revision submitted April 29, 2021; accepted May 13, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.F.D. has received education payments from Medical Device Business Services and Zimmer Biomet. A.B.W. has received consulting fees from Stryker and Arthrex. D.S.C. has received education payments from Pylant Medical; consulting fees from Biomet, DePuy, and Linvatec; nonconsulting fees from Wright Medical and Biomet; royalties from Linvatec; and hospitality payments from Arthrex, Smith & Nephew, and Stryker. J.J.C. has received education payments from Mid-Atlantic Surgical and Pylant Medical and consulting fees, nonconsulting fees, and royalties from Arthrex. D.K.M. has received consulting fees from Zimmer Biomet, nonconsulting fees from Pacira, and royalties from Smith & Nephew and Zimmer Biomet. J.P.S. has received education payments from Liberty Surgical and consulting fees from Stryker. B.R.K. has received consulting fees from Kilo and speaking fees from Performance Dynamics. S.J.N. has received research support from Allosource, Arthrex, Athletico, DJO, Linvatec, Miomed, Smith & Nephew, and Stryker; education payments from Elite Orthopaedics; consulting fees from Ossur and Stryker; and royalties from Springer and Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Rush University Medical Center (12022108-IRB01-AM12).