
Abstract
Background:
The labral suction seal has been shown to provide the majority of resistance in the initial phase of hip distraction. However, the effect of an unrepaired interportal capsulotomy and capsular repair on the initial phase of hip distractive stability in vivo is not well understood.
Purpose:
To investigate the effect of capsular repair on the initial phase of distractive stability of hip joints in patients with femoroacetabular impingement (FAI) syndrome.
Study Design:
Controlled laboratory study.
Methods:
Patients undergoing primary hip arthroscopy for FAI between March and August 2020 were prospectively enrolled. Total joint space was measured on fluoroscopic images at the medial and lateral edges of the sourcil at 12.5-lb (5.7-kg) axial traction intervals (up to 100 lb [45.4 kg]) in 3 capsular states: (1) native capsule, (2) interportal capsulotomy, and (3) capsular repair. Distraction on anteroposterior radiographs was calculated as the difference between total joint space at each traction interval and baseline joint space at 0 lb, normalized to millimeters. The native, capsulotomy, and capsular repair states were compared using Wilcoxon signed-rank and McNemar tests.
Results:
Included were 36 hips in 35 patients. The median force required to distract ≥3 mm was 75 lb (34.0 kg; 95% CI, 70-80 lb [31.8-36.3 kg]) in both the native and capsular repair states (P = .629), which was significantly greater than the median force required to distract ≥3 mm in the capsulotomy state (50 lb [22.7 kg]; 95% CI, 45-55 lb [20.4-24.9 kg]) (P < .001). The most rapid rates of change in joint space were observed at the traction interval at which hips first achieved ≥3 mm of distraction (n = 33 hips; 92%).
Conclusion:
The traction force at which hips distracted ≥3 mm was 75 lb (34.0 kg) in both the native capsular and capsular repair states. Significantly less traction force (50 lb [22.7 kg]) distracted hips ≥3 mm in the capsulotomy state. Complete capsular closure after interportal capsulotomy resulted in restoration of initial distractive stability relative to the unrepaired capsulotomy state at time zero after primary hip arthroscopy.
Clinical Relevance:
This study provides surgeons with an improved understanding of the additional stability to the hip joint from capsular repair after hip arthroscopy for FAI syndrome.
Keywords
The bony architecture of the ball-and-socket, diarthrodial hip provides significant stability to the joint. The hip is further stabilized by static and dynamic stabilizers, including the fibrocartilaginous labrum, ligamentous hip capsule, ligamentum teres, and the musculature that courses across the hip joint. Disruption to any of these stabilizing structures has the potential to result in symptomatic hip instability, which is an increasingly recognized cause of hip pain and dysfunction in the young adult hip-preservation population.2,21 Increased attention has been given to management of the hip capsule during hip arthroscopy in order to protect against capsular hip instability.10,11,13,20
Several cadaveric studies have investigated the relative contributions of the labral suction seal and the hip capsule to the distractive stability of the hip.3,6,7,9-11,15,19,22,23 The labrum and capsule work in conjunction with one another to provide improved distractive stability to the hip compared with the stability they would provide in isolation.9,10 The suction seal created by the congruity of the femoral head against the acetabulum and fibrocartilaginous labrum is a well-described phenomenon that has been demonstrated and reproduced in many studies.3,7,15,19,22 Common among these studies is the prevailing thought that the negative force created by the suction seal provides the greatest resistance to distraction in the first few millimeters of distraction. In a cadaveric study by Fagotti et al, 6 the authors proposed a 2-phase theory of distractive stability of the hip with the suction seal providing the majority of resistance during the initial phase (“labral suction seal phase”) and the hip capsule providing the majority of resistance in the latter phase (“capsular stability phase”). Prior literature has suggested that this shift from the initial to latter phase of distraction occurs at approximately 3 mm.8,7,10 A cadaveric biomechanical study by Suppauksorn et al 23 evaluated the labral suction seal’s peak resistance to distractive force and found that peak resistance occurred between 2.21 and 3.11 mm. Nepple et al 7 found that the labrum contributed to distractive stability the most at 1 and 2 mm of distraction in cadaveric models, and that the capsule plays an increasingly important role at distraction distances >3 mm and only a minor role at distances <3 mm.
While these studies suggest the capsule plays a limited role in the initial phase of distraction, they are limited by their cadaveric study design, and currently no in vivo data exist evaluating the relative contribution of the capsule to initial distractive stability. An in vivo study by O’Neill et al 15 demonstrated that the capsule plays an important role in overall distraction of the hip, showing that capsular repair decreases the distance of distraction at both low and high traction forces. However, these authors did not analyze resistance as a function of distance distracted, and thus their results could not differentiate between initial distraction (<3 mm) and late distraction (>3 mm) effects of capsular repair.
The purpose of this study was to investigate the effect of capsular repair on the initial phase of distractive stability of hip joints in vivo in patients with femoroacetabular impingement (FAI) syndrome. Our primary aim was to compare the axial traction force necessary to distract hip joints ≥3 mm between the native (presurgical instrumentation), capsulotomy, and capsular repair states. We hypothesized that significantly less traction force would be required to achieve initial distraction (≥3 mm) in the capsulotomy state relative to the native and capsular repair states.
Methods
Cohort Selection
The protocol for this study received institutional review board approval. A previously established cohort of patients prospectively enrolled in an axial distraction protocol 17 was reviewed and expanded to include individuals treated by the senior author (S.K.A.) for femoroacetabular impingement (FAI) syndrome between March 6 and August 27, 2020. Inclusion criteria were (1) primary hip arthroscopy for FAI syndrome and (2) completion of the study traction protocol. Exclusion criteria were (1) missing fluoroscopic images, (2) history of previous ipsilateral hip surgery, (3) ipsilateral hip dysplasia (sourcil lateral center-edge angle [LCEA] <20°), (4) capsulotomy type other than an interportal capsulotomy, and (5) hips that did not distract at 100 lb (45.4 kg) of axial force in the native state (requiring venting to obtain distraction). Demographic and operative data were obtained through chart review. Alpha angle, sourcil and bone-edge LCEA values, 8 and Tönnis grades were determined from preoperative radiographs.
Operative Procedure and Traction Protocol
After general anesthesia induction, patients were placed in the supine position and positioned in 0° to 15° of Trendelenburg with the hip in neutral position (0° abduction/adduction, 0° flexion/extension, neutral rotation) on a post-free distraction table (Guardian Hip Distraction System; Stryker). Axial traction was applied to the operative hip using traction controls on the distraction table. All cases utilized the same fluoroscopy machine (OEC 9900 Elite Mobile C-Arm; GE Healthcare) with standard image intensifier and identical magnification and collimation settings to minimize the parallax phenomenon. Before instrumentation of the operative hip, fluoroscopic images were obtained at axial traction intervals of 0, 12.5, 25, 37.5, 50, 62.5, 75, 87.5, and 100 lb (0, 5.7, 11.3, 17.0, 22.7, 28.3, 34.0, 39.7, 45.4 kg) for the native hip state. Each fluoroscopic image was obtained immediately after an increase in traction.
The operative hip was then prepared and draped, and the hip joint was accessed with the use of a spinal needle. An anterolateral portal was first established under the guidance of fluoroscopy, and a second modified anterior portal was established under direct visualization. An interportal capsulotomy was made by connecting these 2 portals between the 12- and 3-o’clock region of the hip capsule, approximately 1 cm distal to the acetabular rim. Capsulotomy length was adjusted within this region to allow adequate access to and visualization of hip pathology. All cases included a thorough diagnostic arthroscopy. All labral tears were repaired with suture anchors. After completion of all central compartment procedures, traction was released, and the femoral osteochondroplasty was performed. Traction was then reapplied to the operative hip for a second time at the same traction force intervals to obtain fluoroscopic images at each traction interval in the capsulotomy state. Traction was again released, and a capsular repair was performed using a previously published figure-of-8 capsular closure technique to create a watertight capsular seal. 1 Traction was then reapplied to the operative hip for a third time at the same traction force intervals to obtain fluoroscopic images at each traction interval in the capsular repair state.
Radiographic and Fluoroscopic Measurements
Imaging measurements were made by 4 trained reviewers (A.J.M., K.M.T., A.K.M., D.L.F.) digitally on fluoroscopic and preoperative anteroposterior (AP) radiographs in our institution’s picture-archiving and communication system. Two measurements were made on each radiographic and fluoroscopic image for every patient, and the mean of the 2 values was used in analysis. Normalization of fluoroscopic images to preoperative AP radiographs was performed to convert fluoroscopic measurements to millimeters using previously published methodology14,16,17 as follows: The femoral head diameter on the preoperative AP radiograph and every fluoroscopic image was measured using the diameter of a best-fit circle. Total lateral joint space was defined as the shortest distance between the lateral edge of the acetabular sourcil and the superolateral aspect of the femoral head, and the total medial joint space was defined as the shortest distance between the medial edge of the acetabular sourcil and the superomedial aspect of the femoral head (Figure 1). Total lateral joint space and total medial joint space were measured on fluoroscopic images at each traction force interval in the native (presurgical instrumentation), capsulotomy, and capsular repair states. Units of measurement were millimeters for all radiographs and pixels for all fluoroscopic images. Total joint space was normalized to millimeters using the following equation:


(A) Preoperative anteroposterior radiograph of a left hip with a line measuring the diameter of the best-fit circle of the femoral head. (B) Fluoroscopic image of left hip demonstrating the same technique of measuring the diameter of the femoral head. (C) Fluoroscopic image measuring the joint space (bars) at the medial and lateral edges of the sourcil (arrows directing towards magnified view of the joint space).
Distraction was calculated as the difference between the baseline joint space at 0 lb of traction and the total joint space at each subsequent traction interval. 14 A distraction threshold of 3 mm was used as a surrogate for the hip suction seal.3,15,23 To evaluate the point at which the largest increase in distraction occurred, the difference in distraction between subsequent traction intervals (Δdistraction) was calculated according to the equation Δ distraction = Distraction(x+ 12.5 lb) –Distraction(x), where x is the traction force interval (in lb).
Statistical Analysis
All statistical analyses were performed using Excel Version 2019 (Microsoft); SPSS Version 27 (IBM); and R Core Team, Version 2023 (Foundation for Statistical Computing). Cohort patient characteristics were calculated and reported as means with standard deviations or counts with percentages. Mean distraction values and the corresponding 95% CIs were calculated for each traction force interval in the native capsular state. Traction force interval data corresponding to distraction ≥3 mm were assessed for normality with the Shapiro-Wilk test. Traction force interval data were determined to follow a nonparametric distribution; thus, Wilcoxon signed-rank tests were used to compare traction force interval data, which are reported as median values. The confidence interval of these median values was calculated based on sample mean, standard error, and critical value (Z value), based on a 95% CI, accounting for the margin of error and the upper and lower bounds of the interval. McNemar tests were used to compare the percentage of hips in the capsular repair and capsulotomy states that maintained <3 mm distraction at the same or greater traction force interval relative to the native state.
Intraclass correlation coefficients (ICCs) with 95% CIs were calculated based on an absolute-agreement, 2-way random-effects model to determine the interrater reliability between the 2 sets of measurements. An ICC value of >0.9 was considered excellent, 0.76 to 0.9 was considered good, 0.51 to 0.75 was considered moderate, and 0.00 to 0.50 was considered poor. 12 Statistical significance was set at α < .05 for all analyses.
Results
A total of 56 hips in 55 patients underwent primary hip arthroscopy and the traction study protocol with the senior author during the study period. One patient was excluded for a history of ipsilateral periacetabular osteotomy surgery, 1 patient was excluded for a sourcil LCEA <20°, 1 patient was excluded for a T-type capsulotomy, 8 patients were excluded for missing fluoroscopic images associated with traction force intervals, and 9 patients were excluded for not distracting at 100 lb (45.4 kg) of axial force in the native state. Thus, 36 hips in 35 patients were ultimately included in the study. Patient characteristics of the cohort are presented in Table 1.
Patient Characteristics (N = 35 patients, 36 hips) a
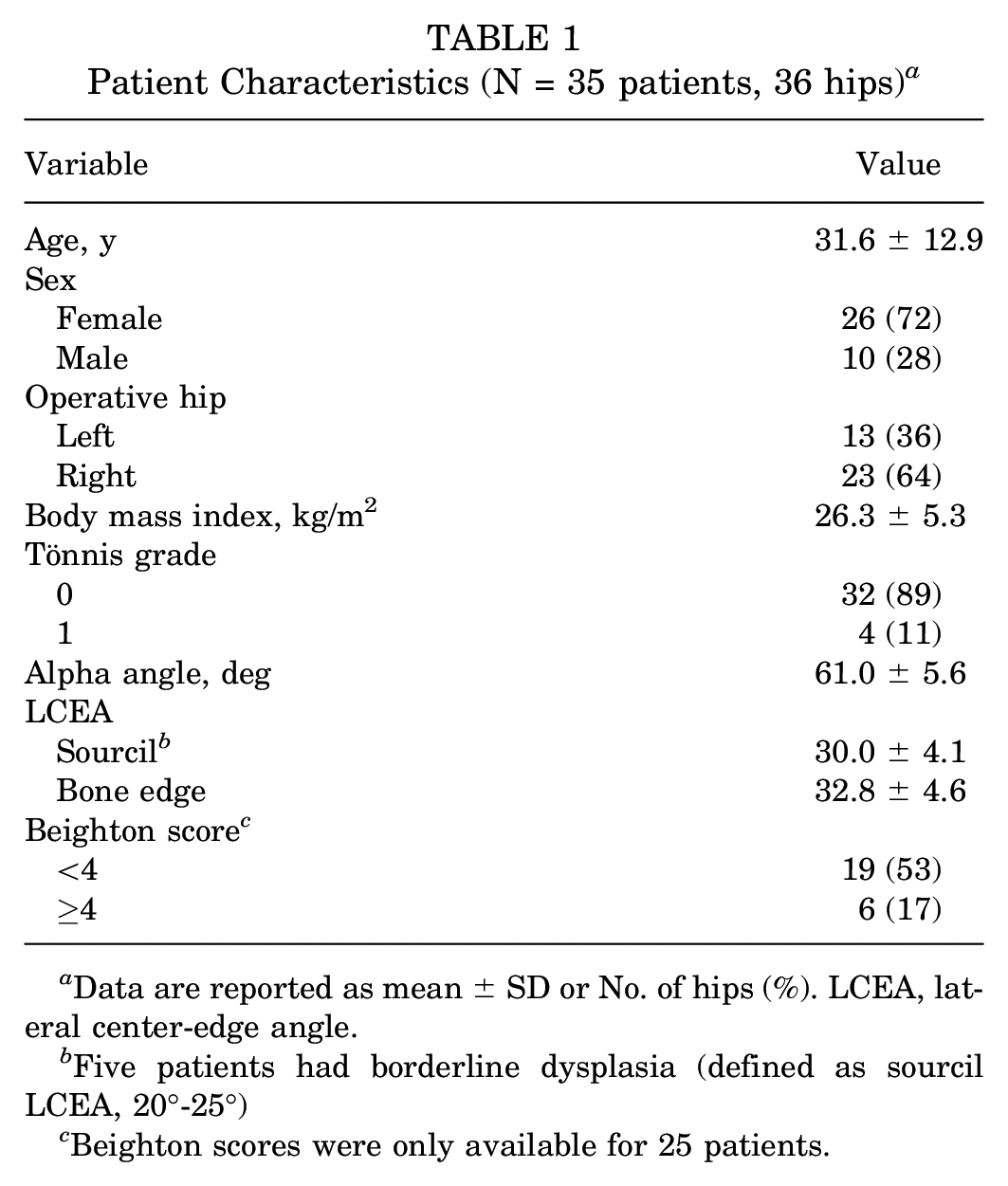
Data are reported as mean ± SD or No. of hips (%). LCEA, lateral center-edge angle.
Five patients had borderline dysplasia (defined as sourcil LCEA, 20°-25°)
Beighton scores were only available for 25 patients.
The mean distraction distances at each traction force interval in the native capsular state are presented in Figure 2, and Table 2 shows the traction forces required to achieve initial distraction in the 3 capsular states. The median traction force at which hips in the native state distracted ≥3 mm was 75 lb (95% CI, 70-80 lb [34.0 kg; 31.8-36.3 kg]), which was significantly greater compared with the capsulotomy state (median, 50 lb; 95% CI, 45-55 lb [22.7 kg; 20.4-24.9 kg]) (P < .001). The median traction force at which hips in the capsular repair state distracted ≥3 mm was 75 lb (95% CI, 70-80 lb [34.0 kg; 31.8-36.3 kg]), which was also significantly greater compared with the capsulotomy state (P < .001). There was no significant difference in the traction force at which hips distracted ≥3 mm between the native and capsular repair states (P = .629). The percentage of hips that maintained <3 mm distraction at the same or greater traction force interval relative to the native state was 72.2% in the capsular repair state and 30.6% in the capsulotomy state (P < .001).

Mean distraction values at each 12.5-lb (5.7-kg) traction force interval between 0 and 100 lb (0-45.4 kg) in the native capsular state. Error bars represent 95% CIs.
Traction Force Required to Achieve ≥3 mm of Distraction for Each Capsular State a

Boldface P values indicate statistically significant difference (P < .05; Wilcoxon signed-rank test).
The largest Δdistraction occurred at the same traction interval at which hips first achieved ≥3 mm of distraction (n = 33 hips; 92%). Mean values of lateral and medial distraction immediately before the largest Δdistraction were 1.29 ± 0.83 and 2.25 ± 1.27 mm, respectively. Mean values of lateral and medial distraction immediately after the largest Δdistraction were 5.37 ± 1.79 and 8.06 ± 1.68 mm, respectively. Mean values of the largest Δdistraction for lateral and medial joint space locations were 4.08 ± 1.85 and 5.81 ± 2.14 mm, which corresponded to a mean of 49.4% and 50.9% of total distraction achieved at 100 lb (45.4 kg), respectively (Table 3).
Key Distraction and Δdistraction Values of the Cohort a

Data are reported as mean ± SD. Δdistraction, difference in distraction between a traction force interval and the interval immediately before it.
Single-measures and mean-measures ICC values for lateral joint space measurements were 0.986 (95% CI, 0.963-0.993) and 0.993 (95% CI, 0.981-0.996), respectively. Single-measures and average-measures ICC values for medial joint space measurements were 0.990 (95% CI, 0.961-0.996) and 0.995 (95% CI, 0.980-0.998), respectively. All ICC measures were within the range of excellent interrater agreement.
Discussion
In the present study, we investigated the effect of capsular repair on the initial phase of axial distraction of hip joints in patients with FAI syndrome. The median traction force at which hips distracted ≥3 mm was 75 lb (34.0 kg) in both the native and capsular repair, which was significantly greater than the median traction force of 50 lb (22.7 kg) at which hips in the capsulotomy state distracted ≥3 mm (Figure 3). Previous in vivo research has shown that performing a complete capsular closure of an interportal capsulotomy reconstitutes resistance to axial distraction intraoperatively compared with the native, intact hip capsular state. 15 The results of the present study add to these findings and suggest that labral repair alone, with an unrepaired interportal capsulotomy, is not as effective at restoring distractive stability of the hip in the initial phase of distraction compared with labral repair and complete capsular closure. These results suggest that the capsule plays a more important role in initial hip distraction stability in contrast to previously published studies attributing initial distraction stability to the labral suction seal.7,8,12

Fluoroscopic images of the right hip of the same patient each obtained at 50 lb (22.7 kg) of axial traction in the (A) native state, (B) capsulotomy state, and (C) capsular repair state. The capsulotomy state shows a substantial increase in distraction relative to the native and capsular repair states, which both show minimal to no distraction.
A distraction threshold of 3 mm was chosen based on previous research that suggested the significant role the labrum and suction seal contribute to resisting axial traction in this range of hip joint displacement.3,15,23 In the present study, the largest Δdistraction occurred at the same traction interval at which hips surpassed the 3-mm threshold in 33 hips (92%). Furthermore, immediately before the largest Δdistraction, mean lateral and medial distraction were both <3 mm (1.29 and 2.25 mm, respectively), and immediately after the largest Δdistraction, mean lateral and medial distraction were both >3 mm (5.37 ± 1.79 and 8.06 ± 1.68 mm, respectively). These findings suggest a distraction threshold of 3 mm effectively characterizes the initial suction seal phase of distraction. In other words, as traction is applied to the hip and negative pressurization of the central compartment suction seal is overcome, a sudden and large increase in distraction is observed in the majority of hips (Figure 4).
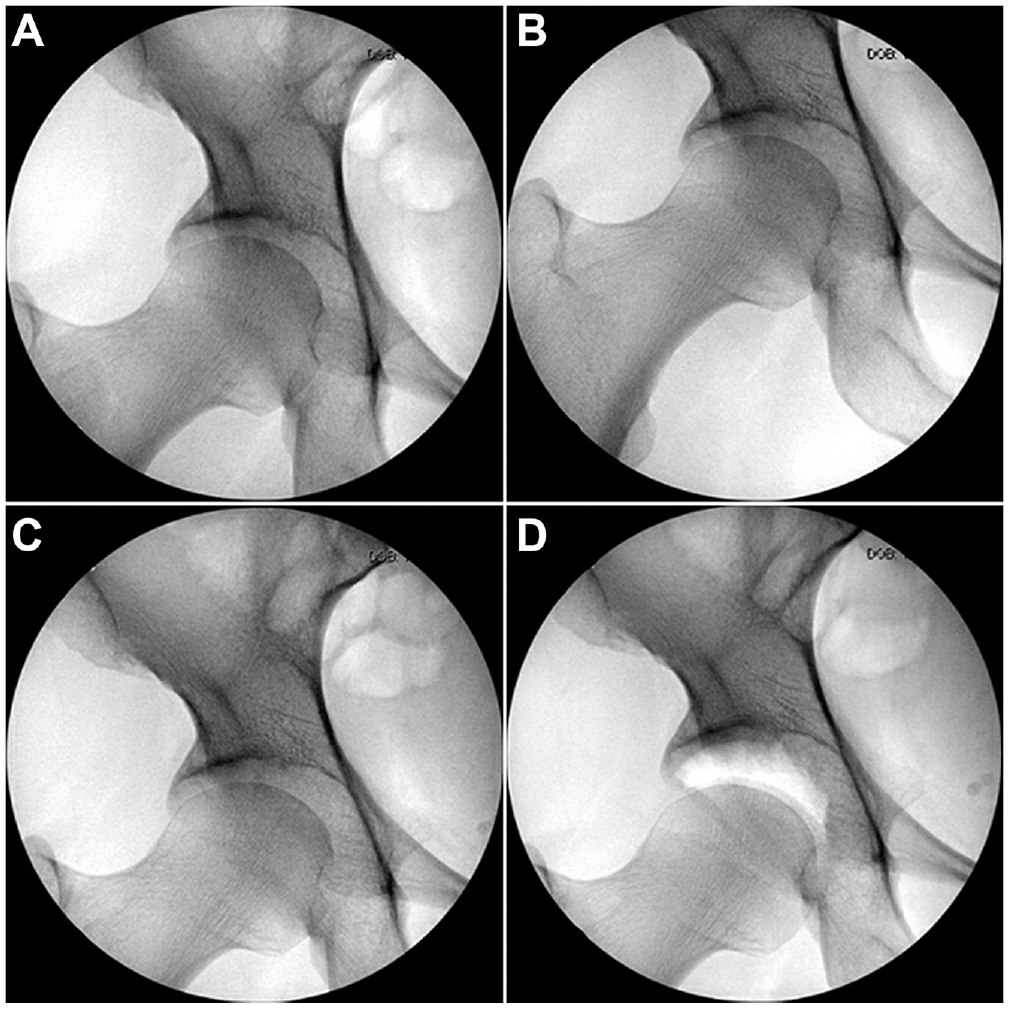
Fluoroscopic images of the right hip of a patient showing no change in distraction up to 87.5 lb (39.7 kg), followed by a sudden, large increase in distraction at 100 lb (45.4 kg). (A) 0 lb (0 kg); (B) 50 lb (22.7 kg); (C) 87.5 lb (39.7 kg); and (D) 100 lb (45.4 kg).
The findings of the present study support the concept of 2 phases of distractive stability proposed by Fagotti et al 6 in their cadaveric study. In their study, the median distance required to rupture the suction seal was 2.3 mm, which is the same as the mean distraction immediately before the largest Δdistraction in the medial joint space in the present study (2.25 mm). Therefore, the initial phase of distraction occurred before this limit, whereas the latter phase of distraction occurred past this threshold. The results of the present study highlight the significant role of the capsule, particularly the role of capsular repair, in providing resistance to hip distraction throughout the initial phase of distraction and suggest this effect may be greater in the in vivo hip than previous cadaveric literature has suggested.
In a cadaveric study, Crawford et al 3 determined the force required to distract the hip joint 3 mm in the intact state (not vented and no labral tear) to be 264 N, which was reduced to 150 N in the vented state, and further reduced to 106 N in the torn state (15 mm anterosuperior labral tear). These were 43% and 60% reductions in traction force required to achieve 3 mm of distraction in the vented and torn states, respectively. They also demonstrated that the greatest difference in applied forces between the intact and vented states was observed in small hip joint displacements between 1 and 3 mm, supporting the significant role provided by the fluid suction seal in this initial phase of distraction. 3 In a cadaveric study by Nepple et al, 15 the labrum was shown to be the primary contributor to the strength of the suction seal in the first 1 to 2 mm of distraction. Furthermore, they showed that as distraction distance increased, the capsule provided increasingly greater resistance to distraction relative to the resistance provided by the labrum, with the capsule providing 53% of the resistance to distraction at 5 mm. Additionally, they showed that peak distraction force occurred at 3 mm of distraction. 15
A cadaveric study by Suppauksorn et al 23 demonstrated that in the intact labral state, with all other surrounding capsular and soft tissue removed, the peak axial traction force occurred at a mean of 3.11 mm (range, 1.8-4.9 mm) of distraction. The relatively large range of distraction presented in their study may be explained in part by the findings of Storaci et al 22 in their cadaveric study, which showed a correlation between labral height and distance to suction seal rupture, specifically that a smaller labral height (<6 mm) was associated with decreased distances to suction seal rupture. In their study, the mean and median distances to rupture the suction seal were 4.9 and 5.0 mm, respectively. The current study did not evaluate the influence of labral size on distractive stability; however, this may be an interesting topic for future in vivo hip distraction studies to further elucidate.
In a cadaveric study, Ito et al 9 demonstrated that the labrum provides more resistance to axial distraction in the first 3 mm of distraction than at 5 mm of distraction when working in isolation. Similar to the results of the present study, their findings at 1, 3, and 5 mm of distraction also suggest the capsule plays a significant role in resisting small axial displacement. In their discussion, they commented on how the labrum and capsule may work in conjunction with each other to provide synergistic resistance to distraction. Johannsen et al 10 demonstrated in a cadaveric study how the labrum and capsule work in tandem to control femoral head motion within the acetabulum in multiple planes. In particular, they showed a significant increase in superoinferior plane motion, or axial distractibility, in the combined labral deficiency and capsular laxity states when compared with the labral deficiency state alone. These findings further suggest the synergistic relationship between the labrum and capsule in providing distractive stability.
The present study was designed as a follow-up to a previously published in vivo study by O’Neill et al 17 that demonstrated greater mean distraction at traction force intervals between 25 and 100 lb (11.3 and 45.4 kg) in hips with an unrepaired interportal capsulotomy when compared with both the native (precapsulotomy) and the capsular repair states. The findings of the current study build upon those of O’Neill et al 17 by describing the influence of the capsular state on the initial phase of distraction. The present study utilizes a different methodology to define distraction as the distance between articular cartilage measured at both the medial and lateral aspects of the hip joint in order to detect small changes in distraction and control for articular cartilage thickness differences as well as for morphological differences between participants. Additionally, the present study provides a focused analysis of the force required to overcome the initial distractive phase (initial 3 mm of distraction), which stands in contrast to O’Neill et al 17 , who analyzed overall distraction at fixed traction force intervals.
Limitations
There are several limitations of the present study that warrant consideration. First, the millimetric values presented in this study were obtained by normalizing to preoperative AP radiographs, which have some degree of magnification. Thus, distraction values in this study are likely slightly larger than the true millimetric values. Second, central compartment hip joint pressure could not be directly measured in this in vivo study, thus necessitating that our design use a distraction threshold and Δdistraction as surrogates to estimate the traction force interval at which the suction seal effect was lost. Third, we only assessed distractive stability of the hip and did not assess for the stability of the hip in other planes of motion such as external rotation or anterior translation. While there are several physical examination maneuvers used to evaluate hip stability, 24 there is a growing body of literature supporting the use of the intraoperative axial stress exam under anesthesia in an attempt to objectively determine hip stability.4,5,18,24
A fourth limitation was that we assessed capsulotomy and capsular repair states at time zero and therefore did not account for any potential capsular healing/failure and associated changes that may occur at future time points. Fifth, labral and osteochondroplasty conditions differed between the native and latter states. The labrum was torn and unrepaired in all native states, and it was repaired with suture anchors in all capsulotomy and capsular repair states. Further, the native state was assessed before osteochondroplasty of the femoral head-neck junction, whereas capsulotomy and capsular repair states were assessed after osteochondroplasty. Last, synovial fluid was present in the central compartment in the native state, and synovial fluid was replaced with saline in the capsulotomy and capsular repair states. Given the differences in viscosity between synovial fluid and saline fluid, it is likely that the suction seal effect is weaker with saline fluid in the central compartment of the hip joint.
Conclusion
The traction force at which hips distracted ≥3 mm was found to be 75 lb (34.0 kg) in both native capsular and capsular repair states. Significantly less traction force (50 lb [22.7 kg]) distracted hips ≥3 mm in the capsulotomy state. Complete capsular closure after interportal capsulotomy resulted in restoration of initial distractive stability relative to the unrepaired capsulotomy state at time zero after primary hip arthroscopy.
Footnotes
Final revision submitted October 22, 2023; accepted November 13, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.K.A. has received consulting fees from Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Utah (ref No. 00074533).