
Abstract
Background:
Race- and ethnicity-based differences in treatment access and outcomes have been reported in the orthopaedic sports medicine literature. However, the rate at which race and ethnicity are reported and incorporated into the statistical analysis of sports medicine studies remains unclear.
Purpose:
To determine the rate at which race and ethnicity are reported and analyzed in athlete-specific sports medicine literature.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
Using PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, articles published by the 3 journals of the American Orthopaedic Society for Sports Medicine between 2017 and 2021 were considered for inclusion. Original sports medicine research studies that focused on athletes were included. Outcome measures included reporting and analysis of patient demographics (age, sex, race, ethnicity). Studies that included demographic variables in a multivariate analysis or that performed a race-/ethnicity-based stratified analyses were considered to have analyzed that variable. Studies that reported and/or analyzed patient demographics were examined. Chi-square tests were performed to determine statistical significance.
Results:
A total of 5140 publications were screened, and 842 met the inclusion criteria. Age and sex were well reported (84.1% and 87.0%, respectively), while race (3.8%) and ethnicity (2.0%) were poorly reported. There was no difference in rates of reporting age, sex, race, or ethnicity between the American Journal of Sports Medicine (AJSM), the Orthopaedic Journal of Sports Medicine (OJSM), or Sports Health: A Multidisciplinary Approach (Sports Health). The rate of analysis was also calculated as a percentage of the studies that reported that variable. Of the studies that reported age, 38.5% analyzed age. Using this method, 26.2% of studies analyzed sex, 40.6% analyzed race, and 17.6% analyzed ethnicity. Although there was no difference in the overall rate at which studies from the 3 journals analyzed ethnicity, Sports Health studies analyzed age (P = .044), sex (P = .001), and race (P = .027) more frequently than studies published in AJSM and OJSM. Of the studies that analyzed race, most of those studies (8/13, 61.5%) found significant race-based differences in reported outcomes.
Conclusion:
This systematic review demonstrated that race and ethnicity are poorly reported and analyzed in athlete-specific sports medicine literature, despite the fact that a majority of studies analyzing race found significant differences between racial groups. Improved reporting of race and ethnicity can determine whether race- and ethnicity-based differences exist in patient interventions to ameliorate disparities in patient outcomes.
Race and ethnicity have been shown to affect clinical outcomes in a wide range of conditions, ranging from low back pain to chronic kidney disease.2,14 The relationship between race and the risk of musculoskeletal injury, socioeconomic status, access to care, and outcome for treatment requires further investigation in orthopaedic research and health care overall. Capogna et al 4 found that White race was an independent predictor for reoperation after anterior cruciate ligament (ACL) reconstruction. Furthermore, recent studies have suggested that there may be disparities in the demographics of patients who undergo ACL reconstruction in addition to the timing of operative treatment relative to injury onset.5,19 Although the data on this topic are limited, reporting race in clinical research can clarify the generalizability of results and highlight those with a lack of patient diversity. Clinicians often seek to assess the applicability of research to individual patients, and failing to report race may exacerbate the well-documented racial disparities in health care. 15
Demographic factors, such as race and ethnicity, have been poorly reported in orthopaedic literature. In a 2021 systematic review conducted by Paul et al, 20 the authors reviewed the top 10 impact journals in orthopaedics and found that across all randomized controlled trials assessing clinical outcomes, only 7.3% reported race. This starkly contrasted with the 95.4% of studies that reported age and the 94.6% that reported sex. Furthermore, when evaluating sports medicine studies specifically, only 2% of studies reported race. Racial disparities in health care have been well documented in a wide range of clinical research, and there is currently a significant paucity of literature that reports race in the orthopaedic sports medicine literature. Given these background data, it is possible that racial differences in outcomes after orthopaedic sports medicine surgery exist but have gone unnoticed as a result of low rates of race reporting.
The purpose of this study was to determine the rates of reporting and analyzing race and ethnicity in the athlete-specific population in the 3 journals of the American Orthopaedic Society for Sports Medicine: the American Journal of Sports Medicine (AJSM), the Orthopaedic Journal of Sports Medicine (OJSM), and Sports Health: A Multidisciplinary Approach (Sports Health). These articles were selected as broadly representative of the American Orthopaedic Society for Sports Medicine in accordance with previously published work. 24 The authors hypothesized that race and ethnicity would be infrequently reported and analyzed.
Methods
Study Selection
This systematic review was completed following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 17
The 3 journals of the American Orthopaedic Society for Sports Medicine (AJSM, OJSM, and Sports Health) were systematically reviewed in January 2022. Five authors (J.H.S., A.T.H., R.W.P., G.C., E.E.J.) manually reviewed each article published between 2017 and 2021. The inclusion criteria were as follows: (1) clinical sports medicine study; (2) analyzed athletes of any level participating in any sport; and (3) included only athletes or provided an athletes-only sub-analysis. The exclusion criteria were as follows: (1) cadaveric or biomechanical studies; (2) review articles; and (3) <10 participants. For the purpose of this study, athletes were defined as those who engaged regularly in sporting activities of any level, whether organized or not.
Data Extraction
Studies were screened to determine if they reported a variety of demographic variables such as age, sex, body mass index, race, and ethnicity. Clinical variables, such type of injury and type of surgery, were also recorded. Within this review, race and ethnicity are not interchangeable and are defined as commonly used in health-related research. Race will be defined as any one of the groups that humans are often divided into based on physical traits among people of a shared ancestry. In contrast, ethnicity will be defined as a sociopolitical construct referring to the sharing of a common culture, including shared origin, attitudes, language, religion, and traditions. Similarly, sex in this study is defined using the biological and physiological characteristics of men and women, such as reproductive organs, chromosomes, and hormone profile.
Studies that explicitly stated a baseline demographic characteristic were considered to have reported that variable. Those that included demographic variables in a multivariate analysis or that performed a race-/ethnicity-based stratified analysis were considered to have analyzed that variable. Reporting patient demographics was calculated as a percentage of the total number of included studies. The analysis of patient demographics was presented as a percentage of the total number of studies and as a percentage of the studies that reported that variable.
Quality Assessment
The Methodological Index for Non-Randomized Studies (MINORS) instrument, which grades noncomparative studies on a scale of 0 (poor quality) to 16 (high quality) and comparative studies on a scale of 0 (poor quality) to 24 (high quality), was used to assess the quality of nonrandomized clinical studies. The Cochrane risk-of-bias tool, which analyzes various types of bias, was used to evaluate the quality of randomized controlled trials. Both scoring systems have been validated in the literature.8,23
Statistical Analysis
Reporting patient demographics was calculated as a percentage of the total number of included studies, whereas analysis of patient demographics was presented both as a percentage of the total number of studies and as a percentage of the studies that reported that variable. For patient sex, this was calculated as a percentage of studies that included both male and female athletes. Chi-square tests were performed to determine statistical significance. P values <.05 were deemed significant.
Results
Literature Search
A total of 5140 articles were screened for inclusion (Figure 1). After title and abstract screening, there were 1038 studies available for full-text screening. Of these, 196 were excluded: 24 were review articles, 36 were not relevant to sports medicine, 70 did not isolate athletes, and 24 included <10 participants. A total of 842 studies remained for quantitative analysis and were included in the study (see Online Appendix for a list of included studies).
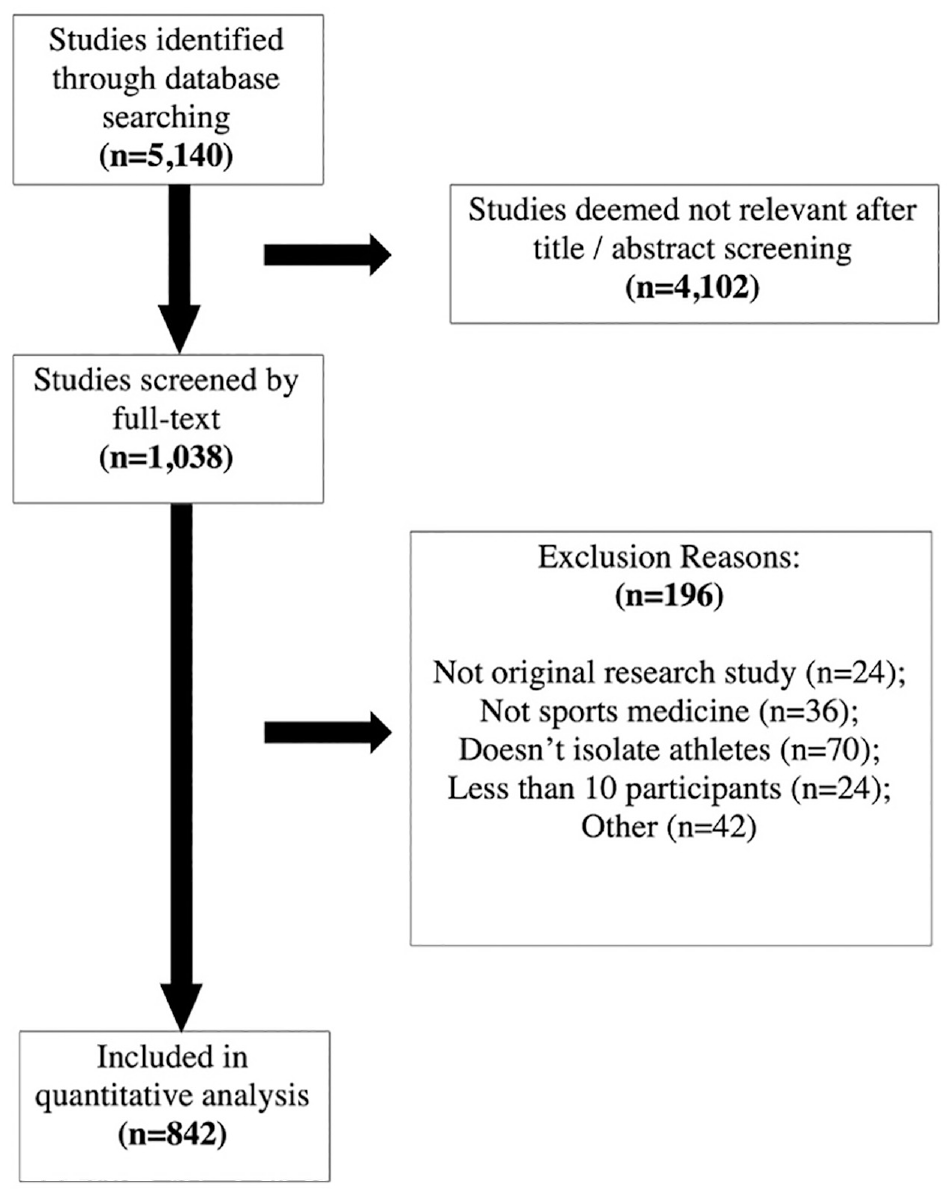
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) diagram of study inclusion.
Reporting Race and Ethnicity
Of the 842 included studies (n = 1,190,264 athletes), 733 (87.0%) reported sex, 709 (84.2%) reported age, 32 (3.8%) reported race, and 17 (2.0%) reported ethnicity. There was no significant difference in the rate at which race was reported in AJSM, OJSM, or Sports Health (Table 1). Similarly, rates of reporting race and ethnicity did not significantly vary between 2017 and 2021 (Table 2).
Rates of Reporting Demographic Variables by Journal a

Data are reported as n (%).
Rates of Reporting Demographic Variables by Year a
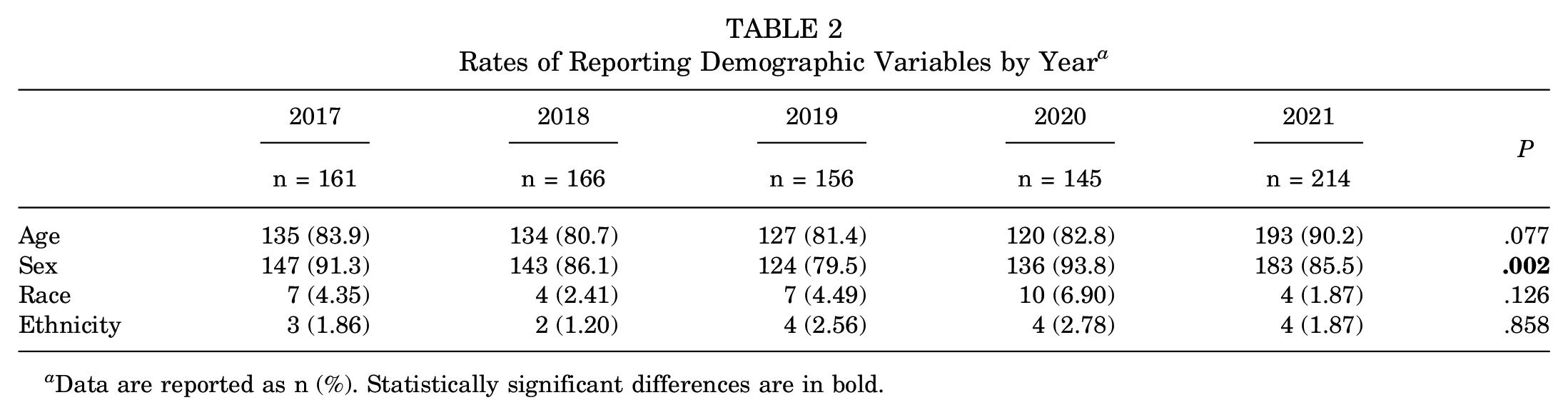
Data are reported as n (%). Statistically significant differences are in bold.
Analyzing Race and Ethnicity
Across all studies, 273 (32.4%) analyzed age, 192 (50.1% [percentage calculated using studies that included both male and female patients]) analyzed sex, 13 (1.5%) analyzed race, and 3 (0.4%) analyzed ethnicity. There was no difference in the rate at which AJSM, OJSM, and Sports Health analyzed ethnicity. However, Sports Health studies analyzed age (P = .044), sex (P = .001), and race (P = .027) more frequently than OJSM and AJSM studies (Table 3). Rates of analyzing these variables did not significantly vary by year (Table 4).
Rates of Analyzing Patient Demographics by Journal a

Data are reported as n (%). Statistically significant differences are in bold.
Percentage calculated using only studies that included both male and female patients.
Rates of Analyzing Patient Demographics by Year a

Data are reported as n (%).
Percentage calculated using only studies that included both male and female patients.
Rate of analysis was also calculated as a percentage of the studies that reported that variable. Of the studies that reported age, 38.5% analyzed age. Using this method, 26.2% of studies analyzed sex, 40.6% analyzed race, and 17.6% analyzed ethnicity (Table 5).
Overall Rates of Analyzing Demographics

Injury-Specific Rates of Reporting and Analyzing Race
The most frequently studied orthopaedic injuries are listed in Table 6. Of these studies, none reported or analyzed ethnicity. Rates of reporting race were similarly low but were highest in studies of Achilles tendon (AT) injuries (1/12, 8.3%) and ACL injuries (4/130, 3.1%). Only 2 studies analyzed race: 1 concussion study and 1 AT study.
Rates of Reporting Race by Orthopaedic Pathology a

Data are reported as n (%). ACL, anterior cruciate ligament; FAI, femoracetabular impingement; UCL, ulnar collateral ligament.
Results of Studies that Reported Race
Of the studies that reported race, 67.6% of participants were White, 21.5% were Hispanic, 8.1% were Black, 2.2% were Asian, and 0.3% were Pacific Islander. The percentage of White participants ranged from 30.8% to 100%, 0.3% to 18.4% for Hispanic, 1.9% to 100% for Black, 0.2% to 9.9% for Asian, and 0.3% to 1.5% for Pacific Islander or Alaskan Native.
Results of Studies that Found a Difference
There were 8 studies that reported a statistically significant racial difference in their analyses.1,6,9,10,12,13,18,26 Jayanthi et al 9 surveyed a cohort of young athletes looking at the impact of socioeconomic status and race on injury rates and sports specialization. The researchers found that White athletes started competitive sports at a younger age, were more likely to have private health insurance, and spent more months of the year training for their main sport; thus, they had higher rates of sports specialization (P < .05). 9 Lemme et al 12 retrospectively analyzed the epidemiology of AT ruptures between 2012 and 2016 in the United States. They calculated incidence rate ratios for age, sex, race, sport participation, and so on and found that compared to White patients, the incidence rate ratio was 4.7 (95% CI, 4.1-5.4) for Native Hawaiians/Pacific Islanders, 2.0 (95% CI, 2.0-2.1) for African Americans, 0.7 (95% CI, 0.6-0.7) for Asians, and 0.5 (95% CI, 0.48-0.51) for Hispanics (P < .01). Another study by Drezner et al 6 prospectively analyzed survival rates for young athletes who experience exercise-related sudden cardiac arrest. When comparing White non-Hispanic/Latino athletes to Black/African American athletes, survival was significantly higher for White athletes (40/67; 60%) versus Black athletes (13/39; 33%Among Hispanic / Latino athletes, only 20% (3/15) survived. Survival was higher in White non-Hispanic/Latino athletes compared to all minority athletes(18/59; 31%) athletes. 6
Kugelman et al 10 prospectively followed 169 patients recovering from operative fixation of tibial plateau fractures and determined certain demographic predictors for successful return to sports. Logistic regression found White race to be the only independent predictor of returning to recreational athletics at 6-month follow-up (odds ratio: 3.026; 95% CI, 1.254-7.350; P = .014). In addition, at the final follow-up, White race was significantly associated (P < .001) with return to sport at final follow-up. 10 The Moon Knee Group 18 analyzed different variables that may predict graft type chosen by surgeons for ACL reconstruction surgery. The researchers found that Black patients were at significantly higher odds of receiving a bone-patellar tendon-bone graft during reconstruction when compared to White patients (95% CI, 0.10-0.93). 18 Another study conducted by Brett et al 1 analyzed race with regard to its impact on young athletes beginning to play American football. They found race, along with age, attention-deficit/hyperactivity disorder diagnosis, and history of sports-related concussion, significantly predicted whether a participant had begun to play American football before the age of 12 years (P < .001). 1
Li et al 13 researched the impact of preseason anxiety and depressive symptoms on the risk of injuries in college athletes during their season. The researchers found that racial and ethnic minority athletes were significantly more likely to report preseason anxiety symptoms, depressive symptoms, and co-occurring anxiety and depressive symptoms compared with White athletes (P < .05). 13 Weber et al 26 documented risk factors for decreased vitamin D levels in Division I football players over a 5-year span. They found that White athletes consistently had the highest measured serum 25-hydroxyvitamin D levels among all races, with a mean of 43.47 ng/mL (SD, 11.91 ng/mL) (P < .001). Black players had the lowest mean serum 25-hydroxyvitamin D levels at 31.02 ng/mL (SD, 7.66 ng/mL) (P < .001). 26
Discussion
The main findings of this study suggest that race and ethnicity were reported at extremely low rates of 3.8% and 2% respectively, and they were analyzed 1.5% and 0.4% of the time, respectively, within athlete-specific sports medicine literature. Notably, of those that analyzed race and ethnicity, 61.5% (8/13) reported significant race-based differences in outcomes. The study by Paul et al 20 found that out of 150 sports medicine clinical trials, only 2% reported race and none analyzed either race or ethnicity. The results of the current study corroborated their findings. When compared to the reporting rates of sex and age, 87% and 84.1%, respectively, race and ethnicity are severely underreported. This finding raises the question whether other significant race-based differences would be found if more studies reported race and ethnicity. Improved reporting of race and ethnicity can determine whether race- and ethnicity-based differences exist in patient interventions to ameliorate disparities in patient outcomes.
There are several examples in our sample where race, when reported and analyzed, were found to have a profound impact on the results. Although AT injuries are commonly studied in the orthopaedic literature, only 1 AT study in our analysis reported race (8.3%). 12 That article found a statistically significant racial difference in the incidence rate of AT ruptures, as Black patients were twice as likely to rupture their AT compared to White patients. 12 Similarly, ACL ruptures are another common orthopaedic injury, but only 4 of 130 ACL studies reported race (3.1%). One study, conducted by Trojian et al, 25 analyzed the ACL tear rate by race in the Women's National Basketball Association (WNBA). They calculated the odds ratio for ACL tears for White European Americans versus racial and ethnic minority European American WNBA players to be 6.55 (95% CI, 1.35-31.73), suggesting that White WNBA players have a much higher chance of tearing their ACL than Black WNBA players. 25 A third study found that Black patients had a significantly higher odds ratio of loss to follow-up after ACL reconstruction surgery. 21 Given the paucity of race/ethnicity reporting in Achilles and ACL studies, and that the tiny subset of studies that reported race still found statistically significant racial differences, there is value in examining whether other existing clinically significant racial differences have yet to be found.
When studying race and ethnicity there are inherently confounding variables present. Socioeconomic status, zip code, and occupation are major variables that give more information on social determinants of care. The socioeconomic status of an individual is influenced by a myriad of factors, such as insurance status, education, race, ethnicity, and sex. These variables together contribute to form the social determinants of health that underlie disease development, access to health care, and patient-reported outcomes. 3 A snapshot from the 2019 Medicaid report shows that the percentage of individuals enrolled in noncommercial insurance is greater in Black and Latino populations than it is for White groups. 16 These underlying variables may explain certain racial differences found in the orthopaedic literature and are important to consider.7,11,22,27 In a randomized control trial, Butler et al 3 reported that preoperative socioeconomic status had a greater impact on the clinical outcomes after cementless total hip arthroplasty than did implant-related factors. Specifically, Black race, an education level less than high school, and a household income below the poverty level were associated with lower outcome scores. 3 In examining these variables, it is clear that the impact of socioeconomic status plays a crucial role in patient outcomes. Newman et al 19 examined factors that related to delayed surgical treatment of ACL injuries in pediatric and adolescent patients and found that among those from lower socioeconomic status households, covered by a noncommercial insurance plan, and who were younger were more likely to have a delay in receiving appropriate treatment. In the same cohort, sex, obesity, ethnicity, and race were not significantly related to the risk of delayed ACL reconstruction. 19
The relationship between socioeconomic status and race are intertwined and must be controlled in order to adequately assess the efficacy and generalizability of treatments. Undertaking the task of controlling for these confounding variables becomes increasingly difficult due to the scarcity in the reporting of race and ethnicity. The substantially low rate of reporting that is shown in our study emphasizes the notion that readers are left to assume that baseline demographics for each study fall within the normal distribution of the population when, in fact, this is most likely not the case. Therefore, it stands to say that there is an evident impact on outcomes in terms of socioeconomic status and access to care; however, there remains much to be revealed about the influence of race in the orthopaedic literature.
Since race and ethnicity are broad terms that encompass many factors, it is easy to confuse an underlying biological or social explanation for a racial difference. The complexity of the human experience can never truly be controlled for and thus we must be aware of the socioeconomic health disparities that may skew medical evidence toward therapies with understudied efficacy in minority populations. In future research, it is important to attempt controlling for these variables before making conclusions about racial and ethnic differences. In the meantime, clinicians should know that race and/or ethnicity may not be the true or primary factor contributing to observed differences in the literature.
Limitations
This study is not without limitations. First, we only reviewed sports medicine–specific clinical studies in the 3 journals of the American Orthopaedic Society for Sports Medicine. Many studies published outside of these 3 journals may emphasize race and ethnicity reporting more than these journals. Second, no comparisons were made to other subspecialties within orthopaedics or fields outside of orthopaedics. It may be valuable to compare sports medicine to other subspecialties as well as other fields to further deduce possible reasons for the scarcity of racial reporting. Last, we did not evaluate potential confounding variables such as socioeconomic status, zip code, and occupation. Without these variables, it is impossible to isolate the importance of race and ethnicity reporting and definitively say that race and ethnicity need to be reported at higher rates.
Conclusion
Our systematic review demonstrated that race and ethnicity are poorly reported and analyzed in athlete-specific sports medicine literature, despite the fact that a majority of studies analyzing race found significant differences between racial groups. Improved reporting of race and ethnicity can determine whether race- and ethnicity-based differences exist in patient interventions to ameliorate disparities in patient outcomes.
Supplemental Material
sj-xlsx-1-ojs-10.1177_23259671241261679 – Supplemental material for Rates of Reporting and Analyzing Race and Ethnicity in Athlete-Specific Sports Medicine Research: A Systematic Review
Supplemental material, sj-xlsx-1-ojs-10.1177_23259671241261679 for Rates of Reporting and Analyzing Race and Ethnicity in Athlete-Specific Sports Medicine Research: A Systematic Review by John Hayden Sonnier, Carlo Coladonato, Irfan A. Khan, Gregory Connors, Ryan W. Paul, Anya T. Hall, Emma E. Johnson, Meghan E. Bishop, Fotios P. Tjoumakaris and Kevin B. Freedman in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted October 12, 2023; accepted February 2, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: F.P.T. has received consulting fees from DePuy Synthes Products and Medical Device Business Services; hospitality payments from MicroVention and Smith+Nephew; and holds stock options from Trice Medical. M.E.B. has received a grant from Arthrex; education payments from Gotham Surgical Solutions & Devices, Arthrex, and Smith+Nephew; and hospitality payments from Stryker. K.B.F. has received a grant from Vericel; education payments from Liberty Surgical; consulting fees from Vericel, Innocoll, and Medical Device Business Services; nonconsulting fees from Vericel; and honoraria from Vericel. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.