
Abstract
Background:
Clavicle fractures are common orthopaedic injuries that frequently occur during sports and recreational activity.
Purpose:
To (1) determine the incidence rate of sports-related clavicle fractures among patients evaluated in emergency departments in the United States over a 5-year period, (2) determine the most common sports and risks associated with clavicle fractures, and (3) update the literature by comparing past and present injury trends.
Study Design:
Descriptive epidemiology study.
Methods:
The National Electronic Injury Surveillance System (NEISS) database was queried for patients evaluated with clavicle fractures in US emergency departments from 2015 to 2019. The authors evaluated the data by age, sex, race, and sport/recreational activity. Injuries were characterized based on sports-specific mechanism of injury. Using the NEISS weighted multiplier, the authors estimated annual incidence rates based on US Census data. Contingency table comparisons of categorical variables (ie, age groups vs sex distributions) were analyzed using either chi-square or Fisher exact tests as appropriate for the population size, while continuous variable comparisons were performed using 1-way analysis of variance statistical testing.
Results:
A total of 2386 athletic-related clavicle fractures were evaluated at participating emergency departments, translating to 304,211 clavicle fractures, with an annual per-year injury rate of 18.72 clavicle fractures per 100,000 persons at risk (95% CI, 15.28-23.67). Male athletes had disproportionately higher injury rates than female athletes (P < .001) for every year of the study and demonstrated a higher incidence of fractures compared with female athletes (injury proportion ratio, 5.54). Patients aged 10 to 19 years accounted for the highest overall incidence of injury (64.5%). The annual incidence rate of athletic-related clavicle fractures was not significantly different during the study period (P = .24). The most common mechanisms of injury were participation in football (26.87%), soccer (15.76%), snowboarding (5.03%), bicycling (3.77%), wrestling (3.65%), and snow skiing (3.52%).
Conclusion:
Study findings indicated that clavicle fractures sustained during sports and recreational activity disproportionately affect male athletes. Adolescent populations (10-19 years of age) had the highest overall incidence of injury, and the most common activities associated with clavicle fractures were football and soccer.
Clavicle fractures account for 2.6% to 5% of all reported fractures and are one of the most common orthopaedic injuries that occur during sports and recreational activity. 19 These fractures are categorized based on anatomic location, with approximately 69% occurring in the middle third of the clavicle, 10% to 30% in the distal third, and 3% in the proximal third. 10,21,22,25 Previous literature has reported a bimodal age distribution of clavicle fractures, with peak incidences in those younger than 25 years and older than 55 years of age. 28 Clavicle fractures are usually caused by direct or indirect high-energy trauma to the shoulder, a mechanism that is common to many sports and recreational activities that involve frequent high-impact collisions or falls. 5 While clavicle injuries are seen year-round across all sports, certain athletic groups are more frequently impacted, including cyclists, football players, hockey players, wrestlers, and winter sports athletes. 5,16,27 Several studies have estimated that sports-related injuries are responsible for 45% of clavicle fractures in the United States, and male athletes aged 10 to 19 years have the highest likelihood of injury. 4,19,21,26,27
Despite the prevalence of these injuries, there remains a paucity of literature regarding the population incidence of clavicle fractures and their correlation with sports and recreational activities. To date, no group has directly analyzed the incidence of clavicle fractures in athletic population across all ages in the United States with an activity-specific focus. Further, previous studies have been limited by small population size, single-center reports, and databases that combine both athletic and nonathletic injury mechanisms. 5,7 –12,14,15
The aims of the current study were to use the US Consumer Product Safety Commission’s National Electronic Injury Surveillance System (NEISS) database to (1) determine the incidence rate of sports-related clavicle fractures evaluated at emergency departments in the United States, (2) identify the most common sports and recreational activities and high-risk populations associated with clavicle fractures, and (3) compare the current rates and risk factors for clavicle fractures with previous trends in the literature. We hypothesized that male sex, younger age, and contact sports participation would increase the risk for clavicle fractures and display an increasing trend over the past 5 years.
Methods
This retrospective cross-sectional descriptive epidemiological study was determined to be exempt from institutional review board approval. Data were obtained using the NEISS database. The NEISS is a statistically valid injury surveillance system that collects data on initial visits to approximately 100 emergency departments in the United States as a probability sample of all US hospitals. These data include sociodemographic variables (age, sex), injury diagnosis (represented as “consumer product codes”), and disposition characteristics that are then used to provide a national estimate of the total incidence of specific injuries. Patients are assigned unique record numbers, injury codes, and location codes representing the activity engaged in at the time of injury. This allows the NEISS to generate a statistically valid and reproducible epidemiological database. The NEISS has been used previously to generate epidemiological trends for many common orthopaedic conditions. 3 –5,13,18,22
We performed a query of the NEISS for all cases of clavicle fractures with a recreational or sports-related code (location code 9) for children and adults aged 5 to 99 years from 2015 to 2019. This 5-year span encompasses the most recent longitudinal data available from the NEISS database and captures the comprehensive study cohort. There was no distinction made between injuries occurring during organized sports or recreational athletic play. To ensure reliability, we reviewed the chief complaint to ensure that the injury was sustained only during athletic/recreational events. Cases that did not present with a sports-related cause and those with any concurrent secondary injury (ie, fracture and a dislocation) were excluded. After this stratification, the NEISS database yielded 2386 sports-related clavicle fractures from 2015 to 2019.
The following independent variables were collected: age, sex, race/ethnicity code, time period (by 1-year intervals from 2015 to 2019), and specific sports-related mechanism of injury (consumer product codes). These data were utilized for both raw calculations and nationally estimated weighted injury counts that were automatically generated by the NEISS database using built-in algorithmic estimates.
All descriptive statistical analyses were conducted using IBM SPSS Statistics (Mac Version 27.0; IBM). Upper and lower bounds of a 95% CI as well as the coefficient of variation were automatically generated for all national weighted estimates of injury by the NEISS query database. US Census Bureau population data and NEISS national estimates were used to calculate the overall incidence rate per 100,000 at-risk persons in the United States for all sports-related clavicle fractures during the study period. Similarly, incidence was calculated per 100,000 at-risk persons in the United States for per-year intervals. For all incidence rates, 95% CIs are included. Contingency table comparisons of categorical variables (ie, age groups vs sex distributions) were analyzed using either chi-square or Fisher exact tests as appropriate for the population size, while continuous variable comparisons were performed using 1-way analysis of variance statistical testing. Statistical significance was set at P ≤ .05 a priori.
Results
Demographic Characteristics
Overall, there were 2386 athletic-related clavicle fractures identified from 2015 to 2019. Through use of the weighted national estimate provided by the NEISS, this equates to 304,211 clavicle fractures evaluated at emergency departments in the United States from 2015 to 2019, with a mean incidence of 60,842 fractures per year. Through use of the US Census Bureau population estimates, these data result in an annual per-year injury rate of 18.72 (95% CI, 15.28-23.67) clavicle fractures per 100,000 at-risk persons.
The demographic characteristics for the entire cohort (N = 2386 patients) are listed in Table 1. The mean patient age at time of injury was 18.16 ± 16.93 years, and the mean BMI was 32.48 ± 32.41. Information on race and ethnicity was available for 1648 individuals (69.07%), although this variable is extremely limited within the NEISS database as patient responses were incomplete and unreliable and thus prevented detailed analysis. The injury incidence was highest among White patients (55.4%), followed by Black patients (9.3%) and Hispanic patients (2.47%) (P < .01). Of note, there was no significant difference in fractures reported among American Indian, Asian, and Native Hawaiian/Pacific Islander populations, who cumulatively accounted for <1.8% of the study cohort.
Demographic Data for the Study Cohort (N = 2386) a
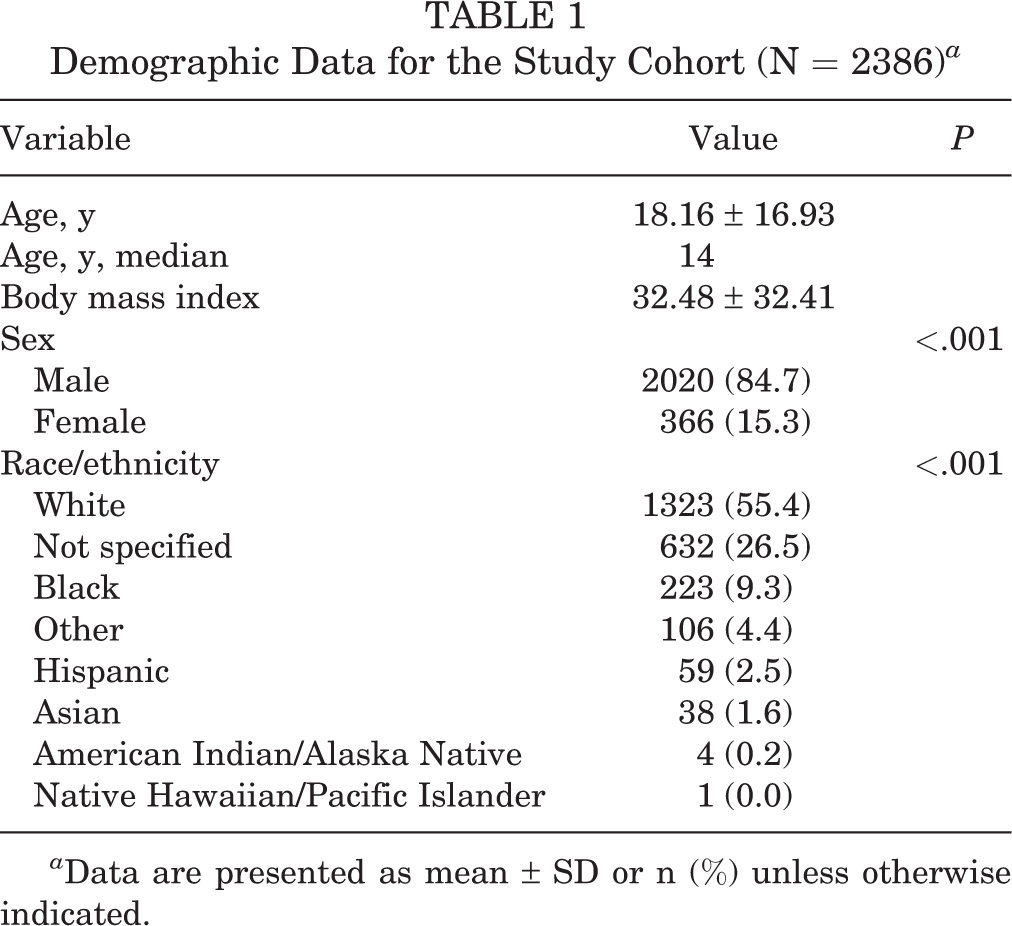
a Data are presented as mean ± SD or n (%) unless otherwise indicated.
Five-Year Injury Trends and Distribution
From 2015 to 2019, the per-year incidence rate gradually decreased until 2019, when the highest overall incidence was observed (20.41 fractures per 100,000 person-years; 95% CI, 15.9-24.9). The number of fractures was not statistically different over time (P = .23) (Figure 1).

Yearly incidence rates of sports-related clavicle fractures from 2015 to 2019.
Sex- and Age-Based Differences
In evaluating cohort differences by sex, we found that male athletes were disproportionately represented among those evaluated with athletic-related clavicle fractures (84.7% male vs 15.3% female; P < .001). This represented a male-to-female injury proportion ratio (IPR) of 5.54. For every year of the study, male athletes were significantly more likely (P < .001) to sustain a clavicle fracture than female athletes. During the study period, the highest rate of clavicle fractures for both male and female athletes was in 2019 (male, 33.74 per 100,000 at-risk persons; female, 7.84 per 100,000 at-risk persons). Year-to-year differences in injury incidence rates were not statistically significant for either cohort (male, P = .11; female, P = .34) (Figure 2).

Annual incidence rates of sports-related clavicle fractures for male versus female athletes from 2015 to 2019. Year-to-year differences are not significant within each sex cohort (male, P = .11; female, P = .34). Differences between sexes were statistically significant in each year (P < .001 for all).
The total incidence of clavicle fractures significantly decreased as age increased (P < .001), with the oldest age group (80-89 years) having the lowest incidence of clavicle fractures (0.1%). Patients of younger age were disproportionately affected, as those in the first 2 decades of life (5-19 years of age) represented 81.0% of all clavicle fractures from 2015 to 2019. Similarly, the age groups most likely to sustain a clavicle fracture during sports or recreational activity were 10 to 19 years (n = 1538; 64.5%), >5 to 9 years (n = 361; 15.1%), and >20 to 29 years (n = 216; 9.1%). When stratified by decade of occurrence, peak incidence was observed in the patients 10 to 19 years of age, as these patients constituted 64.5% of all clavicle fractures from 2015 to 2019. Both male and female athletes demonstrated a peak incidence of injury in the second decade of life (Figure 3).

Incidence of sports-related clavicle fracture by age group and sex.
Sports and Recreational Activities
Overall, the most common sports and recreational activities occurring at the time of clavicle injury were football (26.87%; n = 641), soccer (15.76%; n = 376), snowboarding (5.03%; n = 120), bicycling (3.77%; n = 90), wresting (3.65%; n = 87), and snow skiing (3.52%; n = 84). Importantly, the sports with the highest rates of interpersonal contact (ie, football, soccer, wrestling, hockey, basketball, lacrosse, and martial arts) accounted for 58.56% of fractures (P < .001). Male athletes experienced a higher rate of fracture occurrence in all sports except soccer, snow skiing, basketball, and martial arts. Statistical significance (P < .05) was met in terms of sex differences of injury incidence for the sports of football, soccer, snowboarding, wrestling, hockey, motorized bicycle, martial arts, baseball, and skateboarding (Table 2).
Top 15 Most Common Sports and Recreational Clavicle Injuries by Sex

Discussion
In the present study, our hypothesis was correct in that patients evaluated at US emergency departments with sports-related clavicle fractures were disproportionately male adolescents (age, 10-19 years; 84.7% male vs 15.3% female [P < .001]; IPR, 5.54). Further, higher injury rates were found in those participating in sports with high levels of interpersonal contact (P < .001). These include sports such as football and soccer, in which direct shoulder contact in person-to-person collisions is the likely mechanism of action. Finally, the annual incidence rate of athletic-related clavicle fractures gradually decreased during the study period, until 2019, when clavicle fractures were highest on a per-year basis.
While several groups have reported the annual incidence of clavicle fractures to be between 20 and 50 per 100,000 persons at risk, these studies have largely been conducted at single institutions outside of the United States and are limited by small sample size. 10,15,22 Further, the proportion of these injuries directly attributed to sports and recreation and their epidemiological trends remain largely understudied. In the present study, we report a mean incidence of 18.72 sports-related clavicle injuries per 100,000, ranging from 16.51 to 20.41 per 100,000 persons over a 5-year period. This finding is similar to that of DeFroda et al, 5 who reported an incidence of 24.4 sports-related clavicle fractures per 100,000 person-years from 2002 to 2006, demonstrating that the epidemiological trends of these injuries within sports have remained fairly constant over the past 2 decades.
Overall, we found that male athletes had a significantly higher proportion of sports-related clavicle fractures than female athletes (5.54:1 male-to-female ratio; P < .001). Further, for every year analyzed, male athletes were significantly more likely to sustain a clavicle fracture than female athletes (P < .001). These results are in line with previous studies, as DeFroda et al 5 and McCarthy et al 12 both demonstrated that injury rates were significantly higher in male versus female athletes overall and for sex-comparable sports, respectively. Moreover, in their large multicenter study examining rates of clavicle injury, Kihlström et al 10 found that men represented 68% of clavicle fractures. Several groups have hypothesized that this disproportionate injury rate in men may be due to sports-specific mechanisms such as level of contact and differences in rules and regulations. For example, McCarthy et al highlighted that body checking is legal in men’s lacrosse, whereas no body-to-body contact is allowed in women’s lacrosse; rules such as these help explain sex-based differences in injury rates seen in both our study and theirs.
In the present study, the incidence of sports-related clavicle fractures was highest in the second decade of life (age, 10-19 years) and male athletes were disproportionately affected by injury. Several other groups have also reported this finding and suggested that this 10- to 19-year age group is particularly at risk (91.7 per 100,000 athlete-exposures) given that sports participation rates are highest among adolescent populations. 5,6,15,22,27 The overall incidence of sports-related clavicle injuries was studied by Van Tassel et al, 27 who reported 9428 fractures over a 5-year period in the United States. They found that sports-related injuries were responsible for 45% of fractures and that male participants aged 10 to 19 years had the highest likelihood of sustaining an injury. Court-Brown et al 4 also reported that clavicle fractures represented a large proportion of sports-related injuries and were more common in men. This pattern has been well supported in the literature, as men are estimated to represent 70% of all clavicle fractures. 15,16,19,21 Similarly, the peak incidence of clavicle fracture has been observed in children and young adults (age, 13-20 years), with one-third of all clavicle fractures seen in boys and men between 13 and 20 years of age and one-fourth of all clavicle fractures seen in girls and women between ages 13 and 20 years. 15,16,19,21,24
Given the increased physical demands and competition level coupled with the inherent biological changes seen in bone development and growth plate vulnerability, the rise in sports-related clavicle injuries within this adolescent population may be expected. 6,27 Similarly, other groups have hypothesized that high school–aged athletes (13-18 years old) have the highest risk for clavicle fractures because of their pubescent-related growth spurts and corresponding increase in size, strength, velocity, and competitive level in sport. 2,6,12,27 Of note, previous studies have observed a bimodal age distribution of clavicle injury, with the first peak in those younger than 25 years and second in patients older than 55 years. 15,22 Interestingly, we did not observe the latter peak in the present study. This may be attributed to this study’s focus on sports and recreational-related injuries only, since the majority of clavicle fractures seen in the population >55 years of age are likely a sequela of low-energy falls or osteoporotic bone changes. 18,23
Previous studies have reported that clavicle fractures account for approximately 10% of all sports injuries and comprise up to 10% of all sports-related fractures. 1,20 Fanter et al 6 found that approximately 85% of pediatric clavicle fractures are a direct result of sports or recreational activities. Despite this growing incidence, very few have analyzed the sports-specific mechanisms of clavicle fractures (Table 2). Our results align with similar studies, in that the most common overall sports and recreational activities occurring at the time of injury were football (26.87%; n = 641), soccer (15.76%; n = 376), snowboarding (5.03%; n = 120), bicycling (3.77%; n = 90), wresting (3.65%; n = 87), and snow skiing (3.52%; n = 84). Interestingly, while male athletes were found to have a higher occurrence of fracture in the majority of activities, female athletes participating the following sports had a higher rate of injury occurrence than male athletes: soccer, snow skiing, basketball, and martial arts. Van Tassel et al 27 reported similar findings, with the majority of sports-related fractures having been sustained during bicycling (16%), football (12%), and soccer (5.6%). Many other studies have found similar results, with high rates of fracture seen in high-contact sports. 5,14,17,18 Further, in examining data trends over a 10-year period from 2002-2005 to 2012-2015, DeFroda et al 5 found that the overall incidence of clavicle fractures has continued to occur at similar rates within active populations participating in collision sports.
Limitations
While the NEISS database is a useful tool for estimating injury data and epidemiological trends for injuries evaluated at emergency departments in the United States, it has a few inherent limitations. Since the overall incidence of queried injury rates is calculated directly from NEISS-predictive models based on a weighted probability sample of emergency department visits, the numerical estimates could be subject to sampling bias and may not represent the true incidence of injury in the given study population. However, NEISS does account for these inherent biases in its algorithmic model. Additionally, since the database only includes patients who are evaluated at the emergency department, those who did not seek medical care or were evaluated at another location (primary care office, specialists, etc) are not represented. Further, we were unable to control for repeat fractures in the present study because each patient injury is coded as a separate event within the NEISS system. Finally, the database lacks important variables that are of interest in orthopaedic care (ie, specific clavicle fracture location, mechanism of injury, surgical vs nonoperative management, and return-to-play data). While this may limit the generalizability in comparing clavicle fractures, it is the first of its kind to attempt a specific sports-specific comparison of clavicle fractures evaluated at the emergency department across all age groups in the United States. Therefore, the findings of this study have important implications for elucidating the sports-specific mechanisms of clavicle fractures for high-risk populations and provide initial data for informing sports-specific injury prevention and care.
Conclusion
Participants in sports and recreational activities evaluated at the emergency department with clavicle fractures were disproportionately male adolescents (age, 10-19 years). Sports that require high levels of person-to-person contact, high-force person-to-ground contact, or high physical demands were more likely to result in clavicle fractures across all age groups. From 2015 to 2019, the per-year incidence rate of athletic-related clavicle fractures gradually decreased for a maximum peak in incidence in the terminal year of the study period.
Footnotes
Final revision submitted April 14, 2022; accepted July 25, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: O.A. has received education payments from SouthTech Orthopedics, consulting fees and honoraria from Encore Medical, and hospitality payments from Stryker, Wright Medical, and Zimmer-Biomet. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.