
Abstract
Background:
Multiligament reconstruction (MLR) has become the standard surgical approach for treating multiligament knee injuries (MLKIs).
Purpose:
To identify prognostic factors for patient-reported outcome measures, return to work (RTW), return to sports, and radiographic osteoarthritis (OA) (Kellgren-Lawrence grade ≥2) after MLR for MLKI.
Study Design:
Case-control study; Level of evidence 3.
Methods:
Included were 52 consecutive patients (age, 35.5 ± 11 years; 75% men), with MLKI sustained between 2013 and 2019 and treated with MLR. At a mean follow-up of 3.8 ± 1.6 years, patient-reported outcome measure scores—including the International Knee Documentation Committee (IKDC), the Knee injury and Osteoarthritis Outcome Score (KOOS), the Anterior Cruciate Ligament–Return to Sport after Injury (ACL-RSI), and the 12-Item Short-Form Health Survey—RTW, return to sports, and weightbearing radiographs were obtained. A total of 20 determinants were hypothesized and tested by univariate logistic regression for binary variables or linear regression for continuous variables. Only factors identified as significant (P < .10) were entered into a multivariate logistic regression model.
Results:
The prevalence of injury severity according to the Schenck knee dislocation (KD) classification was as follows: KD I (44%), KD III (36%), KD IV (10%), and KD V (10%). Increased KD grades resulted in decreased IKDC (P = .002) and all 5 KOOS subscales (P≤ .007 for all) scores. Medial meniscectomy (23%) was associated with a worse ACL-RSI score (P = .007) and RTW failure (odds ratio [OR], 36.8; P = .035). Peroneal nerve palsy (6%) was associated with a worse ACL-RSI score (P≤ .001). Radiographic OA was observed in 38%, with distribution predominantly patellofemoral (80%) and medial tibiofemoral (45%). Traumatic cartilage damage (Outerbridge grade >2 [37%]) was associated with secondary patellofemoral (OR, 10; P = .012) and medial tibiofemoral (OR, 10; P = .019) OA. Anterior cruciate ligament reconstruction failure (7%) was a risk factor for medial tibiofemoral OA (OR, 25.8; P = .006).
Conclusion:
Increased Schenck KD grade, permanent peroneal nerve palsy, and irreparable medial meniscus lesions were prognostic factors for worse functional outcomes 3.8 years after MLKI was treated with MLR. Traumatic cartilage damage and anterior cruciate ligament failure were associated with the development of early OA.
Provided that multiligament knee injuries (MLKIs) remain relatively rare, representing between 0.02% and 0.2% of all orthopaedic injuries, published reports on the subject are scarce. The ad hoc literature consists mainly of narrative reviews and expert opinions. This approach has gradually gained acceptance, with systematic reviews suggesting that surgical treatment by multiligament reconstruction (MLR) results in improved postoperative functional outcomes compared with ligament repair.4,16,20 Cohort studies analyzing MLR have gradually been reported, but only a few have presented a follow-up beyond 3 years with a sample size of >50 patients.7,19,21,30,33 They have described good functional outcomes based on patient-reported outcome measures (PROMs). These encouraging results contrast with the devastating nature of the initial injury. A closer look reveals considerable variability in the reported values of PROMs and that an objective assessment of functional ability by a return to work (RTW) and return to sports (RTS) after MLR has not been reported. In contrast to single-ligament injuries, patients with MLKIs are more likely to progress to early secondary osteoarthritis (OA), even when treated with MLR. High variability has also been described, with an incidence of OA on standard radiographs (Kellgren-Lawrence grade ≥2) at 5 and 10 years of follow-up ranging between 21% and 85%.7,9
Given the high variability in the postoperative functional and radiological outcomes for MLR-treated MLKI patients, gathering specific determinants for improving surgical therapeutic management has been identified as an area of research. Two cohort studies have investigated the influence of some determinants on functional outcomes: age, sex, bicruciate tears, meniscal tears, cartilage damage, graft type, and posterolateral corner (PLC) reconstruction.1,21 However, most of the determinants have been studied for their influence on PROMs, and identifying prognostic factors for RTW, RTS, and radiographic OA have not been reported. In addition, these cohort studies were based on only univariate statistical analysis.
The present study aimed to determine prognostic factors for the midterm postoperative functional and radiological outcomes of patients with MLKIs who were treated with MLR. The outcomes studied included PROM scores, patients’ ability to RTW and RTS, and radiographic OA. Identifying specific prognostic factors will enable clinicians to target patients with worse functional and radiological prognoses to improve their surgical management.
Methods
Patient Selection
After the study protocol received ethics committee approval, all patients recorded at a single hospital knee registry who had sustained MLKIs between 2013 and 2019 were considered. MLKI was defined as a complete tear of at least 1 of the cruciate ligaments and 1 of the collateral ligaments. Overall, 82 patients with a documented postoperative follow-up of >2 years were found to be eligible. Patients with MLKI treated nonoperatively (n = 4), ligament repairs only (n = 5), single-ligament reconstruction (n = 6), knee replacement (n = 1), and acute limb amputation for severe nonrepairable neurovascular damages (n = 3) were excluded from the study. MLKI patients >65 years (n = 2) and those with active drug dependency (n = 3) were also excluded. Two patients with deep infections leading to graft removal were withdrawn from the study.
A total of 56 patients meeting the study inclusion criteria were contacted by phone or email for prospective data collection. Only 4 patients were unavailable for follow-up ≥2 years postoperatively. Ultimately, 52 patients provided informed consent to participate in the study. Details are presented in Figure 1.
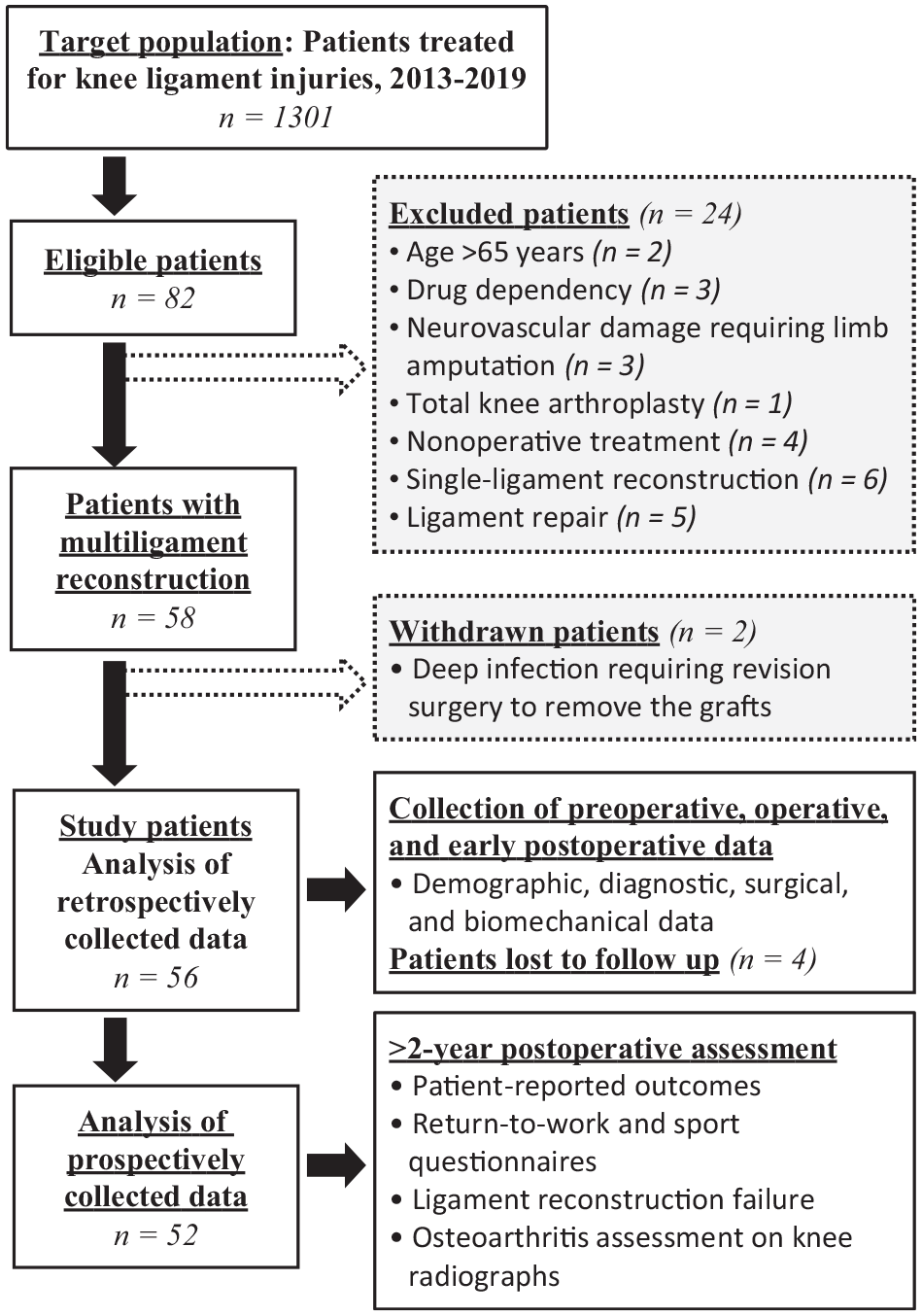
Flowchart of patient inclusion in the study.
Surgical Technique
After MLKI trauma, radiographs and closed reduction were acquired as appropriate. An external fixator was used temporarily only in rare cases (2/52) in which the knee was extremely unstable and redislocated after reduction. Magnetic resonance imaging, computed tomography angiograms, and radiographs with hip-knee-ankle (HKA) angle measurements were performed. If a medial collateral ligament (MCL) or posterior cruciate ligament (PCL) tear was diagnosed, a regular hinged-knee brace or a dynamic-knee brace (PCL Jack Brace; Albrecht) was used to stabilize the joint, respectively, and physical therapy was initiated. This conservative treatment was enforced until the sixth week after the trauma when stress radiographs were obtained. In cases of residual laxity on stress radiographs—PCL grade >2 insufficiency, posteromedial corner (PMC) insufficiency, side-to-side difference of >2 mm in medial joint line gapping for MCL reconstruction—surgical treatment of the affected ligaments was also performed. Moreover, 41% (13/32) of PCL tears and 11% (4/36) of MCL tears did not require surgical reconstruction because no severe residual laxity was reported.
Surgical treatment was scheduled after the resolution of soft tissue swelling and recovery of sufficient range of motion under physical therapy. The mean time from injury to first ligament reconstruction was 40 days. Full weightbearing was allowed during this time, except for patients who sustained injuries classified as Schenck knee dislocation (KD) V, who remained nonweightbearing and underwent surgery within a mean of 10 days. Surgical treatment was performed by the same orthopaedist (R.M.) in all clinical cases, with specific considerations applicable to all included patients, as listed below.
Diagnostic arthroscopy was performed in all patients, with cartilage damage defined as Outerbridge grade >2. For KD V injuries (10% [5/52]), a stepwise approach was adopted, with initial surgical management consisting of open reduction and internal fixation of the fracture (femoral side [2%; 1/52] or the tibial side [8%; 4/52]), followed by secondary ligament reconstruction after full fracture consolidation. Regarding limb alignment, if the HKA angle was assessed as ≥5° varus or valgus with lateral collateral ligament (LCL) or MCL tears, an open-wedge osteotomy was performed using a medial high tibial or distal lateral osteotomy approach, respectively. This allowed for neutral alignment before ligament reconstruction (17% of the cohort [9/52]). A Tomofix locking plate (DePuy Synthes) was used for fixation. Ligament reconstructions were performed after consolidation of the osteotomy site. The PCL was completed first, followed by medial and/or lateral ligament reconstruction during the same surgical procedure. A double-bundle PCL reconstruction and a PLC reconstruction were performed using the technique described by Chahla et al 5 and Serra Cruz et al. 35 An MCL with PMC reconstruction was performed using the method described by Marx and Hetsroni. 24 Anterior cruciate ligament (ACL) reconstruction was performed as a second-stage surgery in patients with KD III-L, KD III-M, and KD IV injuries, usually 8 to 10 weeks after PCL or collateral ligament reconstructions.
The choice of graft type used in the different ligament reconstruction procedures was left to the surgeon's discretion. However, an autograft was preferred for the ACL (93% [40/43]) and the PCL (84% [16/19]), whereas an allograft was preferred for the MCL (87.5% [28/32]) and the LCL (70% [14/20]). For the LCL, 25% (5/20) consisted of distal peroneal head avulsions and were treated by reinsertion. Meniscal repair or meniscectomy was performed simultaneously with the PCL/collateral ligament reconstructions.
Hypothesized Determinants
A total of 20 potential determinants were considered for functional and radiological outcomes, as listed in Table 1.
The 20 Determinants Hypothesized to Predict Functional and Radiological Outcomes of MLR for MLKI a

ACL, anterior cruciate ligament; KD, knee dislocation; LCL, lateral collateral ligament; MCL, medial collateral ligament; MLKI, multiligament knee injury; MLR, multiligament reconstruction; PCL, posterior cruciate ligament; PLC, posterolateral corner; PMC, posteromedial corner.
A low-energy injury was defined as a fall from a standing position or a trauma occurring during International Knee Documentation Committee level 3 or 4 sports activities; all other injuries were classified as high energy.
Data Collection
The clinical protocol comprised both retrospective and prospective arms, with patient engagement and data management being well-defined. Descriptive, diagnostic, surgical, and biomechanics data were retrospectively extracted from the hospital knee registry. At >2 years after surgery, the patients were contacted for appointments to assess functional and radiological outcomes.
PROMs were collected using electronic questionnaires, and the scores for each patient were calculated automatically and entered into a database. Four PROMs were used: the International Knee Documentation Committee (IKDC) Subjective Knee Evaluation form; the Knee injury and Osteoarthritis Outcome Score (KOOS) with Symptoms, Pain, Sport, Activities of Daily Living (ADL), and Quality of Life (QoL) subscales; the Anterior Cruciate Ligament–Return to Sport after Injury (ACL-RSI); and the 12-Item Short-Form Health Survey version 2 (SF-12v2), including the Mental Component Summary and Physical Component Summary.
Regarding RTW, the most intense type of work activity that patients participated in before MLKI (T0) and at the time of the latest clinical postoperative assessment (T1) was compared. Work activities were divided into sedentary and manual labor based on the Saltin-Grimby Occupational Activity scale. 32 Sedentary work included occupations involving sitting/standing or walking—eg, desk workers, watch makers, general office workers, and cashiers. Manual labor included walking and handling materials or heavy manual labor—eg, mailmen, servers, construction and machinery workers, and heavy tool operators. Failure to RTW in each occupational category was defined as patients in whom professional reorientation or permanent work disability was recorded at T1.
Sports activities were divided into 4 levels based on the activity assessment scale described by the IKDC 12 : level 1 activities involved jumping, pivoting, and hard cutting with contacts between players (eg, football or basketball), level 2 activities involved jumping, pivoting, and cutting without contacts between players (eg, skiing or tennis), level 3 activities involved straight-plane activities (eg, cycling or running), and level 4 activities involved straight-plane activities with low cardiovascular input (eg, walking). Failure to RTS was considered if patients’ participation in level 1 or 2 activities at T0 decreased by ≥1 activity level at T1.
Regarding radiological outcomes, Schuss (weightbearing posteroanterior radiograph with the knee at 30° of flexion), skyline Merchant, and weightbearing lateral radiographs enabled analysis of OA at T1 in each knee compartment (patellofemoral, medial, and lateral tibiofemoral). A diagnosis of radiographic OA was defined as a Kellgren-Lawrence grade ≥2.
MCL, LCL, and PCL reconstructions were assessed using stress radiographs. For the PCL, a force of 150 N was applied on the test knee at 90° of flexion using the Telos device (Telos Medical). A constant varus/valgus stress force of 12 N·m was applied with the knee at 20° of flexion for the LCL and MCL. Failure was defined as a side-to-side difference in laxity of >2 mm for MCL/LCL reconstruction and >10 mm for PCL reconstruction (grade 3 insufficiency). An independent orthopaedic surgeon (R.M.) assessed radiographs.
ACL reconstruction was evaluated by anterior laxity measured using a KT-1000 arthrometer (MEDmetric Corp) and by pivot-shift testing. The laximetry was performed at 20° of knee flexion with a manual force of 134 N. The mean value of 3 repetitions was used for analysis. Graft failure was defined as ≥4 mm side-to-side difference in laxity or a positive pivot-shift test grade 2+ or 3+.
The range of motion was measured using a goniometer. Arthrofibrosis was defined as <110° of knee flexion range of motion or flexion contracture of >10° compared with the contralateral side. Arthroscopic arthrolysis was considered if nonoperative measures failed to restore range of motion at 3 months after ligament reconstruction. Swelling and crepitus were not assessed.
Statistical Analysis
Retained factors were initially screened via univariate logistic regression for binary variables or linear regression for continuous variables. The objective was to select the number of factors that could potentially be associated with the variable of interest since we were faced with many factors in relation to the size of the sample. Only factors identified as significant functional outcome predictors in univariate analyses (using P < .10 as a limit for statistical significance determination) were entered into a multivariate logistic regression model. Only significant and independent correlates of adverse events were retained through backward elimination in the final models. Stata software (StataCorp; Version 17) was used for all analyses.
In addition to these analyses, the Fisher exact test was used to determine whether there was a significant association between RTW at T1 and the work activity category in which the patient was engaged at T0, as well as RTS at T1 and the sports activity in which the patient was engaged at T0. The threshold for significance was set at P≤ .05. No power analysis was performed for this study, as these analyses were exploratory.
Results
Cohort Characteristics
The 52 study patients were evaluated at a mean follow-up time of 3.8 ± 1.6 years (range, 2-8 years) after MLR. Details regarding cohort characteristics are presented in Table 2. Regarding injury patterns, 56% (29/52) were classified as KD III or above, and 19% (10/52) were KD IV and underwent combined PCL followed by ACL reconstruction; 4% (2/52) were classified as KD I-M+L because their injury pattern included MCL, LCL, and 1 of the cruciate ligaments. No vascular or open injuries were reported. Although 12% (6/52) of the patients sustained immediate traumatic peroneal nerve palsy associated with a PLC injury, only half had permanent disability, defined as palsy with/without neuropathic pain (6%, 3/52). Their footdrop was treated by posterior tibial tendon transfer (3/3). Graft failure rates are presented in Table 2. Also, 17% (9/52) of patients had at least 1 ligament reconstruction failure. No patient in our cohort required revision ligament reconstruction or functional bracing at 3.8 years, even in graft failure.
Cohort Characteristics (N = 52) a
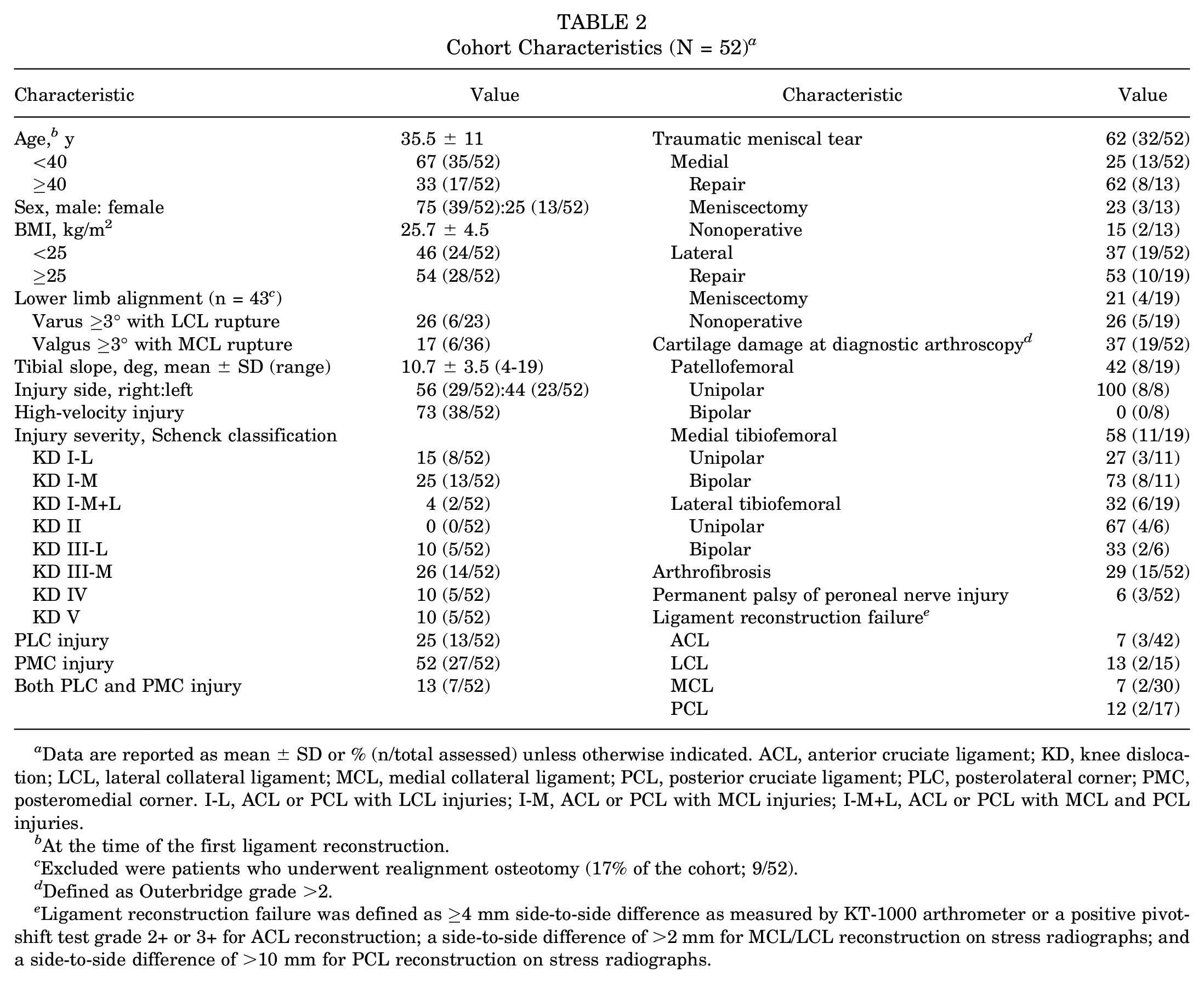
Data are reported as mean ± SD or % (n/total assessed) unless otherwise indicated. ACL, anterior cruciate ligament; KD, knee dislocation; LCL, lateral collateral ligament; MCL, medial collateral ligament; PCL, posterior cruciate ligament; PLC, posterolateral corner; PMC, posteromedial corner. I-L, ACL or PCL with LCL injuries; I-M, ACL or PCL with MCL injuries; I-M+L, ACL or PCL with MCL and PCL injuries.
At the time of the first ligament reconstruction.
Excluded were patients who underwent realignment osteotomy (17% of the cohort; 9/52).
Defined as Outerbridge grade >2.
Ligament reconstruction failure was defined as ≥4 mm side-to-side difference as measured by KT-1000 arthrometer or a positive pivot-shift test grade 2+ or 3+ for ACL reconstruction; a side-to-side difference of >2 mm for MCL/LCL reconstruction on stress radiographs; and a side-to-side difference of >10 mm for PCL reconstruction on stress radiographs.
Arthrofibrosis was the most common adverse event (29% [15/52]) and successfully managed with arthroscopic arthrolysis, which had to be repeated in 40% (6/15) of patients to restore range of motion. The final range of motion in this subgroup of patients was 128° of flexion and 0° of extension, compared with 131° of flexion and 0° of extension in the patients who did not experience arthrofibrosis. Other adverse events included compartment syndrome of the thigh (2% [1/52]) related to a diaphyseal femoral fracture and treated with fasciotomy with good results; nonunion of a marginal fracture of the medial tibial plateau (2% [1/52]), which underwent medial open-wedge high tibial osteotomy at 1.5 years; and complex regional pain syndrome type 1 (2% [1/52]). No hardware removal was required.
Functional and Radiographic Outcomes
Mean PROM scores were 68.5 ± 14.3 for the IKDC, 58.6 ± 23.1 for the ACL-RSI, 48.9 ± 8.9 for the SF-12v2 Physical Component Summary, 51.8 ± 8 for the SF-12v2 Mental Component Summary, 84.2 ± 17.4 for the KOOS-Pain, 76.2 ± 21.7 for the KOOS-Symptoms, 62.1 ± 28.5 for the KOOS-Sport, 90.8 ± 16.1 for the KOOS-ADL, and 63.7 ± 27.2 for the KOOS-QoL. Only 1 patient remained on analgesics (selective serotonin reuptake inhibitors) after 3.8 years. This patient had neuropathic pain secondary to peroneal nerve injury.
RTW and RTS data are shown in Figure 2. At T1, 86% (45/52) of patients returned to preinjury work activities. Professional reorientation was relatively more common in the manual labor group (31%, 5/16) than in the sedentary group (6% [2/36]) (P = .05). At T0, 83% of patients within the cohort were involved in IKDC level 1 and 2 sports activities. At T1, 39% of patients were involved in IKDC level 1 and 2 sports activities. The return rate to the same preinjury sports activities was 47% for those in IKDC level 2 before MLKIs, compared with only 25% for those in IKDC level 1, but this was not statistically significant.
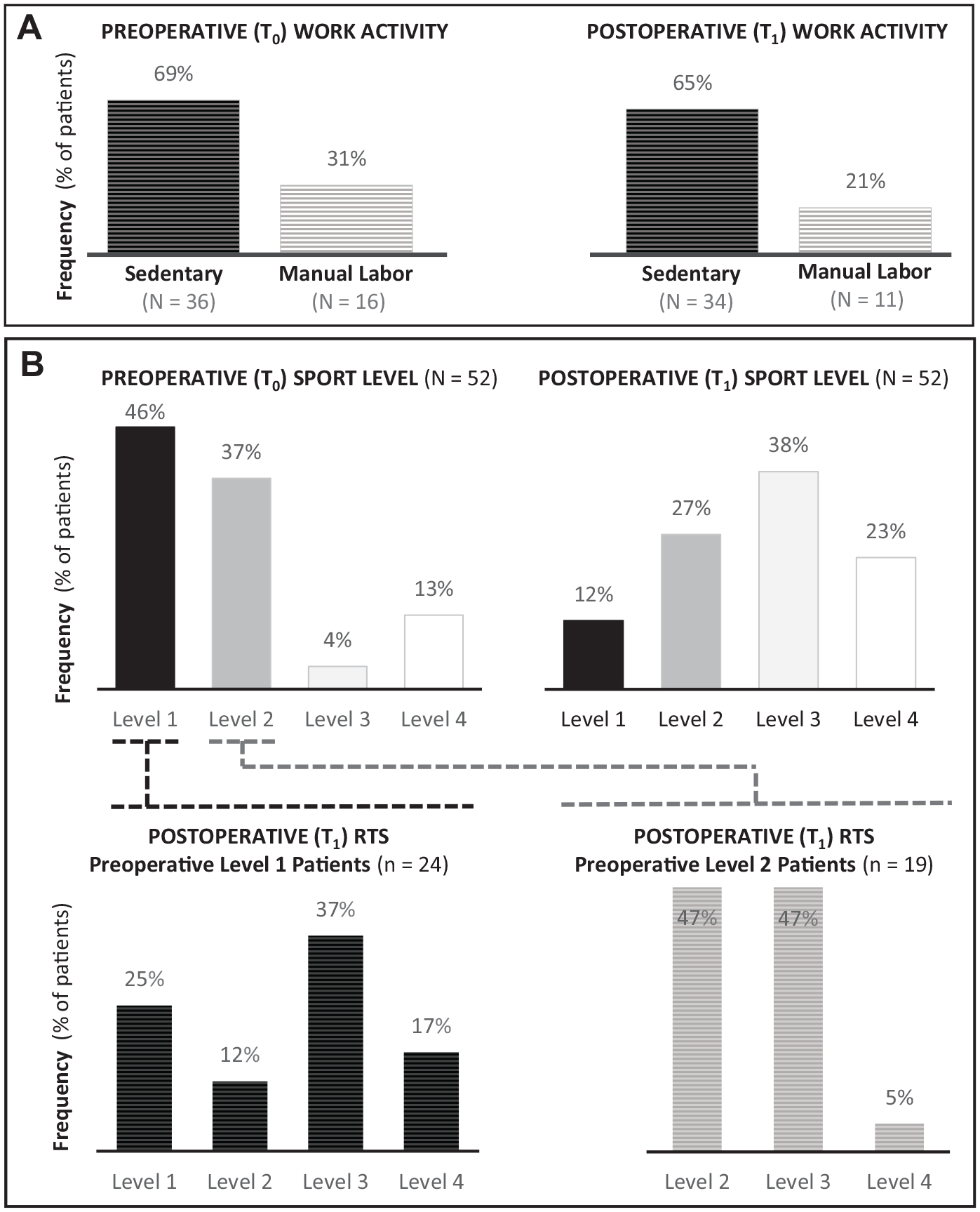
Level of work and sports activities in the study cohort, with a comparison of preoperative (T0) and 3.8-year postoperative (T1) levels. (A) Assessment of patient RTW, comparing sedentary and manual labor according to the Saltin-Grimby Occupational Activity scale. 31 (B) Assessment of patient RTS by levels according to the activity assessment scale. Also shown is the status at T1 of patients involved in sports levels 1 and 2 at T0. IKDC, International Knee Documentation Committee; RTS, return to sports; RTW, return to work.
Radiographic OA (Kellgren-Lawrence grade ≥2) at 3.8 ± 1.6 years was compared with initial cartilage damage observed at diagnostic arthroscopy (Outerbridge grade >2) and is summarized in Figure 3. At T0, 37% (19/52) of patients had initial cartilage damage, mainly involving the medial tibiofemoral compartment (58% [11/19]). At T1, 38% (20/52) of the cohort had radiographic OA, with 80% (16/20) of these knees showing changes in the patellofemoral joint and 45% (9/20) showing changes in the medial tibiofemoral joint. Tricompartmental OA was present in 25% (5/20) of the OA knees at T1, whereas no tricompartmental cartilage damage was observed in any patients at T0.
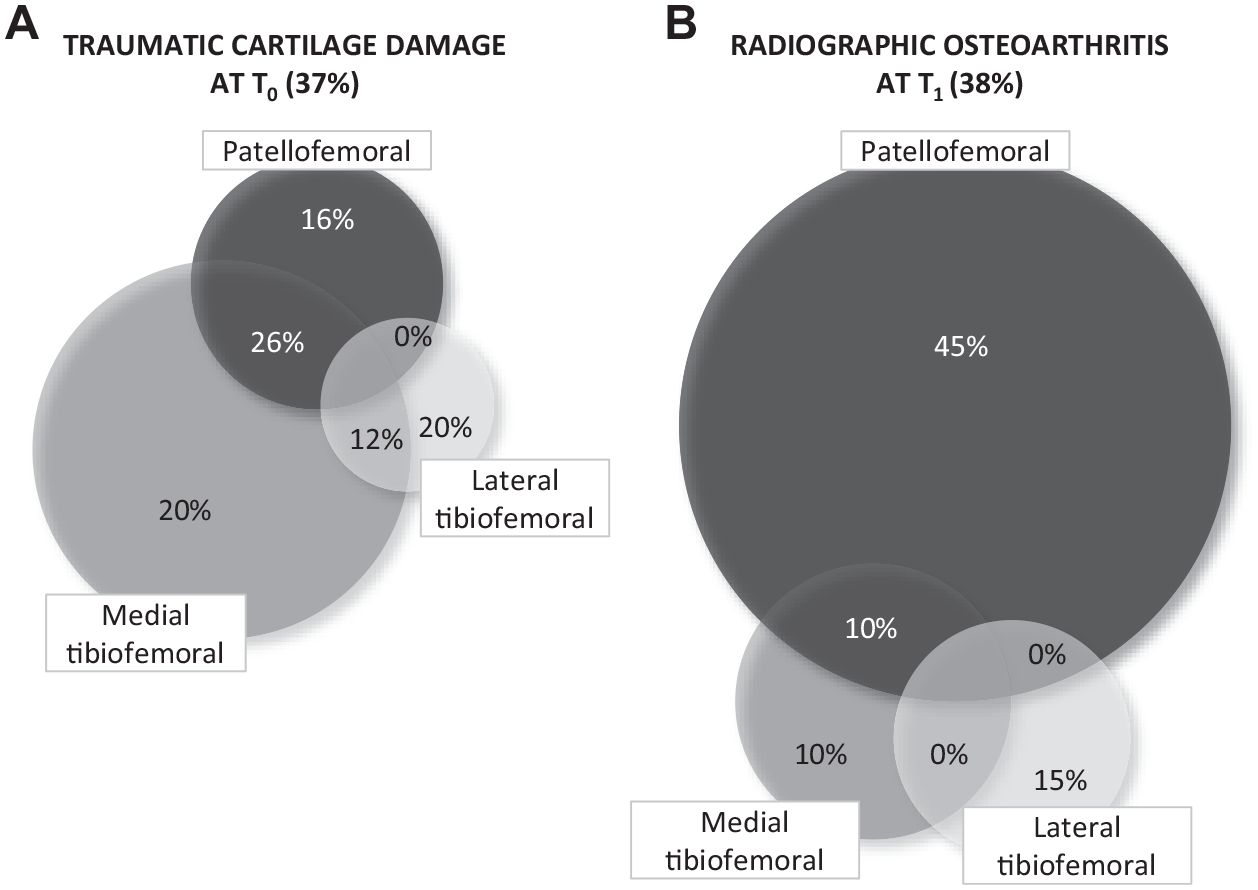
(A) Initial cartilage damage (Outerbridge grade >2) was observed in 37% of the patients at diagnostic arthroscopy (T0). (B) Early osteoarthritic changes (Kellgren-Lawrence grade ≥2) were observed in 38% of the cohort at 3.8 ± 1.6 years of follow-up (T1). Shown are the distributions according to the patellofemoral, medial, and lateral tibiofemoral knee compartments at each time point.
Identified Prognostic Factors for Poor Postoperative PROM Scores
Statistically significant associations between PROM scores and prognostic factors using multivariate analyses are reported in Appendix Table A1.
Multivariate analysis results showed that a patient age >40 years, patient body mass index >25 kg/m2, increased Schenck KD grade, bipolar medial tibiofemoral cartilage damage at T0, medial meniscectomy, and permanent peroneal nerve palsy were associated with lower PROM scores. Compared with KD I lesions, KD III and KD V lesions were associated with relatively lower PROM scores, whereas KD IV lesions revealed similar PROM scores (Figure 4).
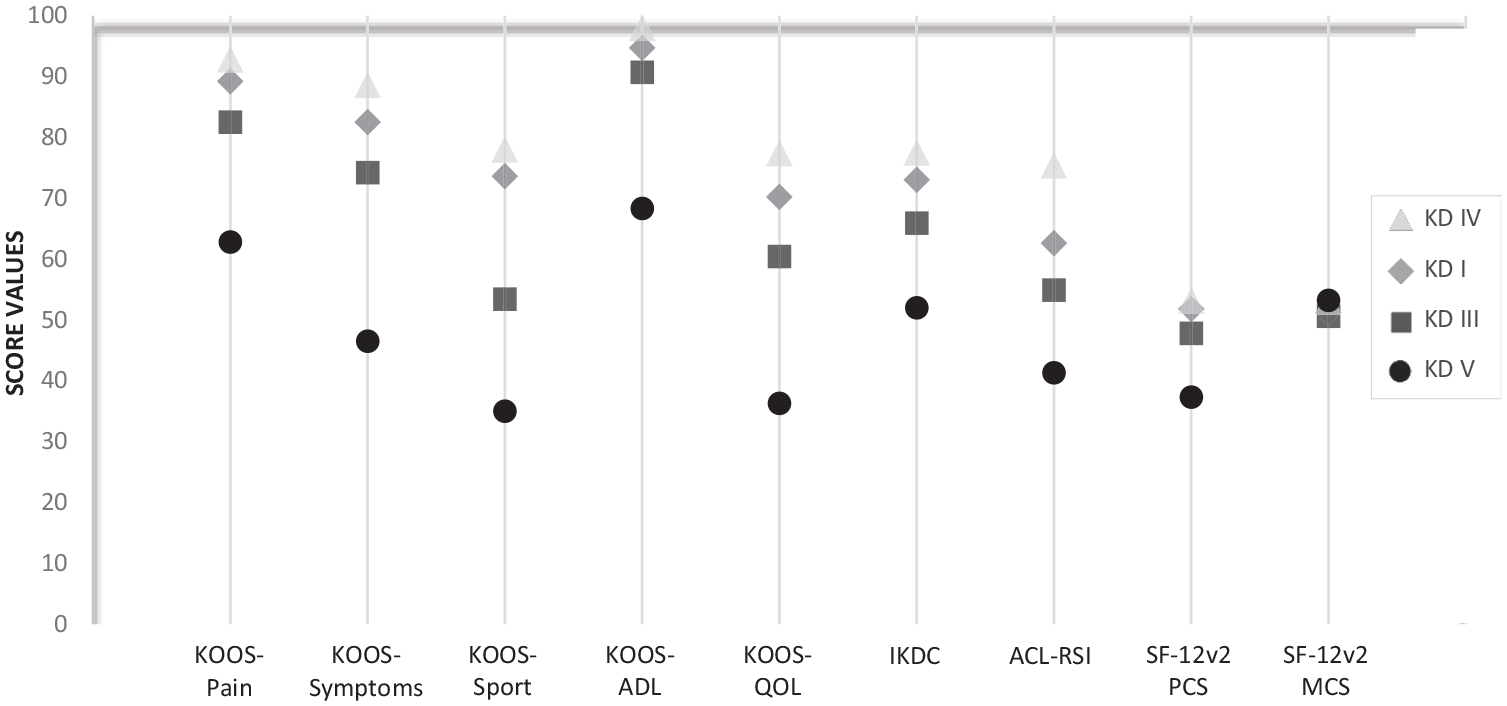
Patient-reported outcomes by multiligament knee injury severity: Schenck knee dislocation (KD) grade 1 versus grades 3, 4, and 5. ADL, Activities of Daily Living; ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; IKDC, International Knee Documentation Committee Subjective Knee Form; KOOS, Knee injury and Osteoarthritis Outcome Score; MCS, Mental Component Summary; PCS, Physical Component Summary; QoL, Quality of Life; SF-12v2, 12-Item Short Form Health Survey version 2.
Identified Prognostic Factors for Failure to RTW or RTS
Statistically significant associations found between failure to RTW and prognostic factors using multivariate analyses are reported in Table 3. Multivariate analysis results indicated that medial meniscectomy was associated with the incapacity to maintain work activity levels, with the differences reaching statistical significance. As assessed using univariate statistics, low-velocity injuries and the occurrence of bipolar medial tibiofemoral cartilage damage resulted in failure to RTW. No significant associations between prognostic factors and failure to RTS were found in the multivariate analysis.
Significant Associations Between Failure to RTW and the Hypothesized Prognostic Factors a

Failure to RTW was defined as patients who reported professional reorientation or work disability at T1 (n = 7). Dashes indicate nonsignificant association. OR, odds ratio; RTW, return to work.
Identified Prognostic Factors for Early Radiographic OA
Increased Schenck KD grade was associated with radiographic OA (Kellgren-Lawrence grade ≥2) in each of the 3 knee compartments in univariate analyses, but this was not subsequently confirmed in multivariate analysis. Similarly, univariate analysis suggested that partial medial or lateral meniscectomy at initial surgery was associated with an increased risk of radiographic OA; nonetheless, this was not supported by multivariate analysis in either the medial or lateral compartments.
The multivariate model retained 2 prognostic factors. First, ACL reconstruction failure was associated with the development of radiographic medial tibiofemoral compartment OA (odds ratio [OR], 25.8 [95% CI, 2.6-259.1]; P = .006). Second, unipolar and bipolar cartilage damage at diagnostic arthroscopy was associated with the development of radiographic OA in the patellofemoral (OR, 10 [95% CI, 1.3-200]; P = .012) and medial tibiofemoral (OR, 10 [95% CI, 1.1-142.8]; P = .019) compartments.
Discussion
The main findings of this cohort study were that functional outcomes after MLR were negatively influenced by the increased Schenck KD grade, permanent peroneal nerve palsy, irreparable medial meniscus lesions, and initial bipolar medial tibiofemoral cartilage damage. Radiological outcomes were negatively influenced by initial cartilage damage and also by early ACL failure. We also confirmed the previous findings of Levy et al 21 and Watrinet et al, 37 who reported that older age and higher body mass index were associated with worse PROM scores after treatment for MLKI.
In 1994, Robert Schenck proposed an anatomic classification based on the pattern of ligament injury that has been used by surgeons to guide surgical treatment but not to predict outcomes after treatment for MLKI. 34 Recently, a consensus of experts has reviewed the Schenck classification and highlighted the importance of 4 factors for MLKI management, namely the number of ligaments involved, vascular damage, common peroneal nerve injuries, and open fractures. 13 According to these experts, these factors may be important in surgical management and predicting outcomes. However, this consensus did not evaluate the clinical impact of these prognostic factors on outcomes by using a cohort study. Herein, we confirmed that increased Schenck KD grade and peroneal nerve palsy were prognostic factors for lower PROM scores in MLKI patients after undergoing MLR.
This study revealed that the increase of anatomic MLKI severity in patients with KD I, KD III, and KD V lesions was associated with poorer PROM scores after MLR. KD IV lesions were surprisingly not associated with a significant difference in PROM scores compared with KD I injuries. This could partly be explained by the low proportion (n = 5) of KD IV patients included in the current clinical study since the main study population consisted of patients presenting with KD I and KD III injuries. A study by Kanakamedala et al 17 analyzed the outcomes of patients with KD V, but the authors compared them to all other dislocations taken together. In this study, we investigated patients with MLKIs combined with fractures (KD V) in a stratified analysis for all Schenck KD classifications. As Kugelman et al 18 noted, fracture dislocations are usually assessed from a traumatological point of view, highlighting bone damage according to the Hohl and Moore classification, 15 with limited analysis of the ligamentous aspects as proposed by Schenck. Finally, with regard to the KD I and KD III patterns, some authors have suggested a negative effect of lateral injury (KD I-L and KD III-L), particularly on the PLC. Alentorn-Geli et al 1 (n = 39; mean follow-up, 2.25 years) described an 8% rate of PLC failure as assessed by clinical examination and suggested that PLC reconstruction was associated with lower PROM scores after MLR. Our study described a comparable rate of 13% LCL failure as assessed by stress radiographs; however, we did not observe an influence of the lateral compartment on functional outcomes. Nevertheless, surgical management was different, as we proposed systematic osteotomy for varus deformity ≥5° in case of complete LCL tears. Previous studies have concluded that in patients with PLC injuries and varus deformity, undergoing valgus osteotomy in addition to PLC reconstruction prevented PLC failure and improved functional outcomes.14,27
Permanent peroneal nerve injury was associated with worse PROM scores in the present study. Neurolysis at the time of ligament reconstruction was followed by complete recovery of the posttraumatic deficit in half of the patients. In the other half, revision surgery by posterior tibial tendon transfer was considered. Peroneal nerve palsy continues to be a therapeutic challenge, and other authors have also reported a persistent lack of ankle dorsiflexion resulting in poor functional outcomes despite posterior tibial tendon transfer or peroneal nerve grafting to avoid permanent foot drop. 38
Injury to the medial joint line was a determinant of outcomes. Both irreparable meniscal tears and initial cartilage damage have been identified as prognostic factors for worse outcomes after MLR. For meniscus injuries, this study showed that irreparable medial meniscus lesions were associated with a worse functional prognosis in terms of RTW and several PROMs. Richter et al 29 reported an incidence of 15% of traumatic meniscal tears associated with MLKI in 63 patients, while Moatshe et al 26 reported 37% in 303 patients. Both studies described an equivalent rate of injury between the medial and lateral sides. The present study reported a higher rate of traumatic meniscal tears, with an incidence rate of 62%. Although lateral meniscal tears were more common, it was medial meniscal tears that were the determining factor. Despite the fact that most medial meniscal tears (62%) were treated with repair, a minority of medial meniscus lesions were irreparable and required meniscectomy (23%), which was associated with lower PROM scores and failure to RTW. A meta-analysis has already reported that meniscectomy, compared with meniscal repair, was associated with worse PROM scores in patients with concomitant ligament injuries. 39 However, RTW after meniscectomy, compared with meniscal repair, in the setting of ligament injuries (or not), has not yet been reported. In addition, most authors have reported that lateral meniscectomy resulted in greater shear stress on the cartilage than medial meniscectomy and was, therefore, associated with worse functional outcomes.28,31 However, we concluded that medial meniscectomy affected the functional prognosis of patients. This finding may be explained by the loading stress on the cartilage after medial meniscectomy as well as concomitant initial cartilage damage in the medial compartment.
In addition, bipolar medial tibiofemoral cartilage damage was associated with worse PROM scores, which was important because the most common site of initial cartilage damage was the medial tibiofemoral compartment. First, this could be explained by the fact that the proportion of bipolar lesions relative to unipolar lesions was higher in the medial tibiofemoral compartment (73%, 8/11) than in the lateral tibiofemoral compartment (2/6, 33%). Second, it has been previously reported that the medial compartment experiences more load than the lateral compartment, with an average load of 60% to 70%. 2 Third, Bellemans et al 3 concluded that in the European population, almost 50% of the patients have an HKA angle in varus >3°, with a higher incidence in men than in women. This is important because varus deformity has been associated with increased medial knee loading and cartilage damage in previous studies. 6 In the present study, we did not analyze whether the proportion of medial defects occurred in knees with varus malalignment. Furthermore, we studied 3 times more men than women in this cohort.
Finally, medial meniscectomy, bipolar medial tibiofemoral cartilage damage and overloading due to varus deformity in the medial compartment may have a synergistic effect on poorer functional outcomes.
Overall reported rates of OA vary widely after MLKIs treated by MLR. Whereas Engebretsen et al 7 (n = 85; mean follow-up = 5.3 years) and Fanelli et al 9 (n = 44; mean follow-up = 10 years) reported Kellgren-Lawrence grade ≥2 OA in 85% and 20% of their cohorts, respectively, we observed an overall prevalence of 38%. Variations might be related to differences in initial cartilage damage and in the length of the follow-up period. We found that 37% of the patients already had cartilage damage (Outerbridge grade >2) at diagnostic arthroscopy and that this was a risk factor for secondary radiographic OA at a 3.8-year follow-up in both medial tibiofemoral and patellofemoral compartments. Furthermore, while the pattern of initial cartilage damage was predominant in the medial compartment (58%), the pattern of postoperative radiographic OA was predominant in the patellofemoral compartment. The patellofemoral compartment was involved in 80% of knees with OA and was twice as likely to be affected as the lateral and medial compartments. Finally, although no initial tricompartmental cartilage damage was reported at the time of diagnostic arthroscopy, tricompartmental OA was observed in one-fourth of OA knees at 3.8 years.
PCL and MCL tears could be initially managed with conservative treatment. Indeed, we found that 41% of PCL tears and 11% of MCL tears did not require surgical reconstruction because no residual laxity was reported. In MLKIs that were treated surgically, reconstruction failure was observed in 7% of ACL, 12% of PCL, 7% of MCL, and 13% of LCL. Even if it was not associated with worse functional outcomes, ACL failure was associated with early medial tibiofemoral OA changes. Previous long-term studies have concluded that ACL residual laxity was associated with secondary medial meniscal tears and medial tibiofemoral cartilage damage, with a higher risk of developing secondary posttraumatic OA after ACL injuries.36,40
Regarding RTW, we reported a high overall rate of 86%, a figure that is influenced by the fact that two-thirds of our cohort had low-demand sedentary occupations and returned to their previous work in almost all cases. This result is comparable to a systematic review that concluded that 88.4% of patients RTW after MLKIs are managed conservatively or surgically, most commonly by repair. 8 Furthermore, we reported that one-third of manual laborers were unable to maintain their work activities after MLR. Groot et al 11 showed that heavy knee-demanding work was a negative factor for RTW after ACL reconstruction. Finally, the only prognostic factor negatively affecting the overall RTW was partial medial meniscectomy. We suspect that partial meniscectomy has a negative impact on RTW in manual laborers. However, because of the small number of patients in this subgroup, it was not possible to identify prognostic factors.
Concerning RTS, almost half of the patients who were involved in IKDC level 2 activities before MLKIs returned to their preinjury level, whereas only 25% of the patients involved in IKDC level 1 activities were able to return to their preinjury level of sports. These results were inferior to isolated ACL reconstruction reported by Lindanger et al, 22 who concluded that 53% of the patients were able to return to level 1 sports activities, and by Grindem et al, 10 who reported that 61.9% of patients returned to level 1 sports activities and 77.8% to level 2 sports activities. We were unable to confirm the association of our hypothesized prognostic factors to the level of RTS. Systematic reviews after ACL reconstruction have concluded that graft type, graft site, quadriceps strength, and fear of reinjury were associated with a lower RTS.23,25 Knowing that MLKIs are severe injuries, a future analysis of these factors could be interesting.
Limitations
This study has some limitations. First, our mean follow-up of 3.8 years (min-max, 2-8 years) is relatively short, particularly when looking at radiographic or symptomatic OA findings. Even when treated with MLR, MLKIs may be an evolving disease with further increases in degenerative joint disease expected. Our results may not be accurate in the long term. Second, despite a similar therapeutic management for each patient, there is a potential selection bias. Graft selections were not standardized, patients >65 years old and with an active drug dependency were excluded, patients with deep infections leading to graft removal were withdrawn, almost half of the PCL ruptures were treated conservatively, and bicruciate ligament reconstructions were performed in only a quarter of patients. Third, although the mean sample size was relatively larger than in previous studies, the number of patients in the different subgroups was sometimes relatively small and could lead to statistical errors. Last, we analyzed 20 possible determinants of these outcomes and may therefore have obtained some spurious significant associations. The selected determinants were also based on those already identified in the literature using univariate analysis. However, certain factors highlighted by Held et al 13 and Alentorn-Geli et al 1 were not analyzed, such as open fracture, which was not found in our cohort, neurovascular damage, which was excluded, and bicruciate injuries, which were not compared with single cruciate injuries. Similarly, the outcomes of bicruciate ligament reconstructions compared with single cruciate ligament reconstructions were not reported.
Conclusion
Increased Schenck KD grade, permanent peroneal nerve palsy, and irreparable medial meniscus lesions are prognostic factors for worse functional outcomes at 3.8 years after MLKI treated with MLR. Traumatic cartilage damage and ACL failure were associated with the development of early OA.
Footnotes
Appendix
Statistically Significant Associations Between PROM Scores and Hypothesized Prognostic Factors a

| Prognostic Factor | n | PROM Score b | Coefficient | P | |
|---|---|---|---|---|---|
| Univariate | Multivariate | ||||
| IKDC | |||||
| Multiligament knee injury severity | −21 | .002 | .002 | ||
| KD I | 23 | 73 (67.3 to 78.3) | |||
| KD V | 5 | 52 (33.2 to 65.8) | |||
| Age, y | −12.2 | .003 | .001 | ||
| <40 | 35 | 72.5 (68 to 77) | |||
| ≥40 | 17 | 60.3 (47.9 to 72.7) | |||
| Permanent peroneal nerve palsy | −18.3 | .031 | NS | ||
| No | 49 | 69.6 (65.6 to 73.6) | |||
| Yes | 3 | 51.3 (30.8 to 71.9) | |||
| LCL failure | −16.7 | .062 | NS | ||
| No | 13 | 71.5 (65.2 to 77.9) | |||
| Yes | 2 | 54.8 (30.9 to 77) | |||
| Cause of injury | −7.6 | .090 | NS | ||
| High-energy injury | 38 | 70.6 (66 to 75.2) | |||
| Low-energy injury | 14 | 63 (49.5 to 76.4) | |||
| Multiligament knee injury severity | −7.1 | .085 | NS | ||
| KD I | 23 | 73 (67.3 to 78.3) | |||
| KD III | 19 | 65.9 (52.1 to 79.3) | |||
| KOOS-Symptoms | |||||
| Multiligament knee injury severity | −36 | <.001 | .001 | ||
| KD I | 23 | 82.5 (74.0 to 90.9) | |||
| KD V | 5 | 46.5 (18.7 to 74.6) | |||
| Age, y | −12.9 | .043 | .024 | ||
| <40 | 35 | 80.5 (73.4 to 87.6) | |||
| ≥40 | 17 | 67.6 (47.9 to 87.2) | |||
| MCL failure | −27.6 | .086 | NS | ||
| No | 28 | 79 (71.4 to 86.8) | |||
| Yes | 2 | 51.4 (12.2 to 90.8) | |||
| Cause of injury | −16.2 | .016 | NS | ||
| High-energy injury | 38 | 80.6 (73.9 to 87.3) | |||
| Low-energy injury | 14 | 64.4 (44.8 to 84.1) | |||
| KOOS-Pain | |||||
| Multiligament knee injury severity | −26.3 | .002 | .002 | ||
| KD I | 23 | 89.2 (82.2 to 96.1) | |||
| KD V | 5 | 62.9 (40 to 85.6) | |||
| Age, y | −10.9 | .033 | .022 | ||
| <40 | 35 | 87.8 (82.2 to 93.5) | |||
| ≥40 | 17 | 76.9 (61.4 to 92.6) | |||
| Permanent peroneal nerve palsy | −22.6 | .027 | NS | ||
| No | 49 | 85.6 (80.8 to 90.4) | |||
| Yes | 3 | 63 (38.2 to 87.7) | |||
| Medial tibiofemoral cartilage damage | −18.7 | .074 | NS | ||
| None | 41 | 85.3 (46.8 to 99.7) | |||
| Bipolar | 8 | 66.6 (44.9 to 86.5) | |||
| Cause of injury | −13.8 | .010 | NS | ||
| High-energy injury | 38 | 88 (82.7 to 93.3) | |||
| Low-energy injury | 14 | 74.2 (58.6 to 89.8) | |||
| Sex | −10.4 | .061 | NS | ||
| Men | 39 | 86.9 (66.6 to 99.2) | |||
| Women | 13 | 76.5 (67.1 to 85.9) | |||
| KOOS-Sport | |||||
| Multiligament knee injury severity | −38.6 | .004 | .005 | ||
| KD I | 23 | 73.6 (62.2 to 84.9) | |||
| KD V | 5 | 35.0 (–2.3 to 72.2) | |||
| Age, y | −25.4 | .002 | .001 | ||
| <40 | 35 | 70.4 (61.6 to 79.3) | |||
| ≥40 | 17 | 45 (29.5 to 69.4) | |||
| Multiligament knee injury severity | −20.2 | .015 | .016 | ||
| KD I | 23 | 73.6 (62.2 to 84.9) | |||
| KD III | 19 | 53.4 (25.9 to 80.9) | |||
| KOOS-ADL | |||||
| Multiligament knee injury severity | −26.3 | .001 | .006 | ||
| KD I | 23 | 94.6 (88.3 to 99.1) | |||
| KD V | 5 | 68.3 (47.4 to 89.1) | |||
| Permanent peroneal nerve palsy | −25.6 | .006 | .003 | ||
| No | 49 | 92.3 (88 to 96.6) | |||
| Yes | 3 | 66.7 (44.3 to 89) | |||
| Medial meniscus | −23.7 | .012 | .009 | ||
| Repair | 8 | 91.4 (86.7 to 96.2) | |||
| Meniscectomy | 3 | 67.7 (44.6 to 90.7) | |||
| Age, y | −10.8 | .022 | .005 | ||
| <40 | 35 | 94.4 (89.1 to 99.6) | |||
| ≥40 | 17 | 83.6 (69.1 to 98) | |||
| Medial tibiofemoral cartilage damage | −24.8 | .009 | NS | ||
| None | 41 | 87.9 (56.8 to 99.8) | |||
| Bipolar | 8 | 63.1 (50.4 to 87.9) | |||
| Cause of injury | −16.3 | <.001 | NS | ||
| High-energy injury | 38 | 94.9 (87.8 to 99.8) | |||
| Low-energy injury | 14 | 78.6 (60.9 to 94) | |||
| Corner injury | −9.6 | .056 | NS | ||
| PMC | 27 | 93.2(89.0 to 97.4) | |||
| PLC | 13 | 83.6 (71 to 96.3) | |||
| KOOS-QoL | |||||
| Multiligament knee injury severity | −34 | .011 | .007 | ||
| KD I | 23 | 70.2 (58.9 to 91.5) | |||
| KD V | 5 | 36.2 (0 to 73) | |||
| ACL-RSI | |||||
| Permanent peroneal nerve palsy | −38.9 | .004 | <.001 | ||
| No | 49 | 60.9 (54.7 to 67.1) | |||
| Yes | 3 | 22 (–9.9 to 53.7) | |||
| Medial meniscus | −22.1 | .022 | .007 | ||
| Repair | 8 | 52.4 (27.2 to 77.6) | |||
| Meniscectomy | 3 | 30.3 (–3.4 to 63.9) | |||
| BMI, kg/m2 | −14.1 | .028 | .004 | ||
| <25 | 24 | 66.4 (57.1 to 75.7) | |||
| ≥25 | 28 | 52.3 (30.4 to 74.1) | |||
| Multiligament knee injury severity | −21.3 | .061 | NS | ||
| KD I | 23 | 62.6 (52.6 to 72.6) | |||
| KD V | 5 | 41.3 (9 to 73.7) | |||
| SF-12v2 PCS | |||||
| Multiligament knee injury severity | −14 | .001 | .002 | ||
| KD I | 23 | 51.2 (48.3 to 58.3) | |||
| KD V | 5 | 37.2 (25.7 to 48.7) | |||
| Medial tibiofemoral cartilage damage | −12 | .029 | .011 | ||
| None | 41 | 49.9 (30 to 69) | |||
| Bipolar | 8 | 37.9 (27.9 to 47.9) | |||
| Age, y | −7 | .006 | <.001 | ||
| <40 | 35 | 51.2 (48.4 to 58.1) | |||
| ≥40 | 17 | 44.2 (36.4 to 51.9) | |||
| Permanent peroneal nerve palsy | −10.1 | .056 | NS | ||
| No | 49 | 49.5 (47 to 52) | |||
| Yes | 3 | 39.4 (26.7 to 51) | |||
| ACL failure | −8.8 | .015 | NS | ||
| No | 39 | 50.3 (47.7 to 53) | |||
| Yes | 3 | 41.5 (30.8 to 52.4) | |||
No significant associations were found between the prognostic determinants and SF-12v2 MCS scores. ACL, anterior cruciate ligament; ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; ADL, Activities of Daily Living; BMI, body mass index; IKDC, International Knee Documentation Committee; KD, knee dislocation; KOOS, Knee injury and Osteoarthritis Outcome Score; LCL, lateral collateral ligament; MCL, medial collateral ligament; MCS, Mental Component Summary; NS, not significant; PCS, Physical Component Summary; PLC, posterolateral corner; PMC, posteromedial corner; PROM, patient-reported outcome measure; QoL, Quality of Life; SF-12v2, 12-Item Short-Form Health Survey version 2.
Data are presented as mean (95% CI).
Final revision submitted December 4, 2023; accepted January 10, 2024.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Canton de Vaud (ref No. 2019-02413).