
Abstract
Background:
Limited knowledge exists regarding prognostic factors after rotator cuff repair.
Purpose:
To identify pre- and perioperative predictors for functional outcomes after arthroscopic rotator cuff repair.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
This study included patients who underwent arthroscopic rotator cuff repair between January 2013 and April 2019 and who had preoperative magnetic resonance imaging scans. The procedures were performed by 4 shoulder surgeons at a single institution. Excluded were patients who had previous surgeries, those who underwent open surgery, and those without 12- and 24-month follow-up clinical data. Patient-reported outcomes (American Shoulder and Elbow Surgeons [ASES] Standardized Shoulder Assessment Form and University of California, Los Angeles [UCLA] Shoulder Rating Scale scores) were assessed preoperatively and at 6, 12, and 24 months postoperatively. Using multiple linear regression analysis, the authors evaluated the influence of 29 variables relating to patient, lesion, and procedure characteristics on postoperative outcomes, with the 24-month ASES score as the dependent variable.
Results:
The study sample consisted of 474 patients (500 shoulders). The median ASES score increased from 41.6 preoperatively to 88.3 at 24 months (P < .001), and the median UCLA score increased from 14 preoperatively to 32 in the same period (P < .001). The following variables were found to be independent predictors for higher 24-month postoperative ASES score: male sex, absence of rheumatologic disease, older age, lower degree of supraspinatus muscle fatty degeneration, acromioplasty, and a higher preoperative ASES score.
Conclusion:
The prognostic factors for better clinical results at 24 months after arthroscopic rotator cuff repair were male sex, absence of rheumatologic disease, older age, lower degree of fatty degeneration of the supraspinatus muscle, concomitant acromioplasty, and higher preoperative ASES score.
Keywords
Rotator cuff syndrome is a major cause of shoulder pain. 25 There has been an increasing trend in the performance of rotator cuff repairs, 5,20,24 generating a high economic burden. 20 However, the functional results and the retear rate are still far from ideal. 26 Thus, it is important to determine prognostic factors for unsatisfactory results after rotator cuff repair, enabling the adoption of specific strategies for a subgroup of patients.
Randomized clinical trials are considered the gold standard in evidence-based medicine, making it possible to determine superiority between different treatments. However, there are limitations when extrapolating the results of a clinical trial to the general population. 18 Observational studies, although designed to predict risk, can lead to biases arising from differences between exposed and unexposed populations. 14 Thus, studies with multivariate prognostic models represent important tools in assessing the probability of occurrence of some outcome after an individual’s treatment. 28
Few studies have assessed prognostic factors for clinical outcomes after rotator cuff repair using a multivariate model, ∥ and only 2 so far did so with a sample of a few hundred patients undergoing arthroscopic treatment. 10,17
The aim of this study was to determine pre- and perioperative prognostic factors for clinical outcomes at 24 months after arthroscopic rotator cuff repair.
Methods
Study Design
We conducted a multivariate prognostic model for clinical outcome after arthroscopic rotator cuff repair, based on a retrospective cohort with prospectively collected data. The study was approved by the ethics committee of our institution.
Patients and Setting
Patients who underwent arthroscopic rotator cuff repair between January 2013 and April 2019 were included in the study. Surgery was indicated in symptomatic patients with partial tears with >50% of the tendon thickness or with full-thickness tears that did not improve with physical therapy for ≥3 months. The physical therapy treatment consisted of the Jackins program. 16 Corticosteroid injection was not routinely performed, being used only in patients with severe pain.
The surgical procedures were performed by 4 shoulder and elbow surgeons from the same institution (E.A.M., J.H.A., M.E.C.G. and F.B.A.-S.), all of whom had ≥6 years of experience performing the procedures. Inclusion criteria were primary arthroscopic rotator cuff repair (partial or complete); having undergone standardized pre-, peri-, and postoperative data collection; and having preoperative magnetic resonance imaging (MRI) scans. Debridement without rotator cuff repair, open or mini-incision surgeries, and patients who had undergone previous surgery in the same shoulder were not included. Patients who did not have clinical evaluation at both 12 and 24 months after surgery were also excluded.
Surgery and Rehabilitation
The surgery was performed in the beach-chair or lateral decubitus position, depending on the surgeon’s preference, under general anesthesia associated with brachial plexus block. Bursectomy was routinely performed. Acromioplasty was sometimes performed according to the surgeon’s preference. Patients with symptomatic arthrosis in the acromioclavicular joint underwent distal resection. Symptomatic acromioclavicular arthrosis was defined as pain on local palpation with MRI findings, such as capsuloligamentous thickening and osteophytosis. The long head of the biceps was treated when it presented instability (subluxation or dislocation) or partial lesions >25%, or was in the presence of type 2, 3, or 4 superior labral anterior-posterior lesions. 41 Tenotomy was performed in patients aged ≥60 years, and tenodesis was performed on younger patients and on athletes or those with a body mass index <25, regardless of age.
The majority of the posterosuperior tears and all the subscapularis tears were repaired using the single-row technique. Postoperative immobilization with a sling was maintained for a total of 4 to 6 weeks. Movements with the elbow, wrist, and fingers were allowed from the first day after surgery. After the end of the third week, passive exercises were started. Active assisted and free active exercises were started after the sling was removed. Muscle strengthening was performed only after a significant gain in movement, around the 12th week. Patients were released for sports activities at 6 months, as long as the range of motion and strength were reestablished.
Magnetic Resonance Imaging
All the preoperative imaging was performed using MRI scanners with magnet strengths of at least 1.5 T. Axial, oblique coronal, and oblique sagittal fat-suppressed intermediate-weighted images and oblique coronal and oblique sagittal T1-weighted images were used. In most cases, intra-articular or intravenous paramagnetic contrast was not used.
Outcome Measures
The primary outcome measure was the American Shoulder and Elbow Surgeons (ASES) Standardized Shoulder Assessment Form score. 37 Scoring by the modified University of California, Los Angeles (UCLA) Shoulder Rating Scale 6 was a secondary outcome. The scales were applied 1 week before surgery and after 6, 12, and 24 months by a research assistant.
Prognostic Factors
We evaluated the influence of 29 prognostic factors relating to patient, lesion, and procedure characteristics, with the 24-month postoperative ASES score acting as the dependent variable.
Factors Related to the Patient
The patient characteristics that we evaluated were age, sex, dominant side affected, diabetes, rheumatologic disease, smoking status, previous trauma to the shoulder, workers’ compensation status, previous injection in the shoulder, and preoperative function according to the ASES score. Data were obtained through an interview with the patient, which was carried out by the same research assistant 1 week before surgery.
Factors Related to the Lesion
Variables related to supraspinatus tear were tendon thickness (partial or full-thickness tear), retraction at the coronal plane (<3cm or ≥3cm), anteroposterior extension (affects part of the tendon or the entire extension affected), and tear of the anterior portion. Infraspinatus tear was evaluated according to tendon thickness (intact, partial tear, or full-thickness tear), retraction (<3cm or ≥3cm), and anteroposterior extension (intact, superior portion, or the entire tendon). A subscapularis tear was categorized as an intact, partial tear of the upper third; a full-thickness tear of the upper third; or a tear involving the upper two-thirds or the entire tendon. Fatty degeneration of the supraspinatus, infraspinatus, and subscapularis was classified as grades 1 to 3 according to Fuchs et al. 11 The long head of the biceps was evaluated for tear (absent, partial tear, or complete tear) and instability (located, subluxated, or dislocated depending on its position in the biceps sulcus, or not applicable in cases of complete tear). We also evaluated arthrosis of the glenohumeral joint (absent or present). Data were obtained when the MRI was analyzed by the surgeon responsible for the surgical procedure, together with the radiological report. In all cases, imaging occurred within 12 months of the surgical procedure.
Factors Related to the Surgical Procedure
Intraoperative factors included acromioplasty, distal clavicle resection, procedure performed on the long head of the biceps (none, tenotomy, tenodesis, or not applicable [in cases of complete rupture]), repair technique for the posterosuperior lesion (single or double row), and whether complete repair was performed.
Missing Data
For the variables studied as prognostic factors, no imputation technique was used. Regarding the outcomes (ASES and UCLA scores), the strategy of the final observation carried forward was adopted. Patients who did not have the results referring to 24 months, although they had already completed ≥2 years of the procedure, had the 12-month data imputed as the final result. When the 24-month result was present but the preoperative or 6- or 12-month result was missing, these were imputed by the mean. Patients whose scores at both 12 and 24 months were not registered were excluded.
Statistical Analysis
Continuous variables were evaluated for normality using the Kolmogorov-Smirnov test and for homogeneity using the Levene test. Continuous variables showed nonparametric distribution, so the general characteristics of the sample were calculated as means with standard deviations and/or medians with interquartile ranges. Categorical variables were reported as absolute values and percentages.
We compared differences in scores across assessment times (preoperatively and at 6-month, 12-month, and 24-month follow-ups) separately for the ASES and the UCLA using the Friedman test, with post hoc analysis using the Wilcoxon signed-rank test.
Multiple linear regression analysis was used to test the influence of predictor variables on the dependent variable (ASES score at 24 months). We used the following assumptions for this analysis: independence of residues; linearity between dependent and independent variables, collectively and individually, verified through graphical analysis; homoscedasticity of data; multicollinearity between variables; analysis of outliers; influential and leverage points; and normality of waste. All these assumptions were checked for the possible need to adjust the data. We initially chose to include all the variables in the database that had presuppositions of biological plausibility and/or clinical significance. Later, to analyze how well-adjusted the model was, statistical criteria were used, excluding all independent variables that presented P ≥ .1. The model with the best correlation coefficient (r) and total explained variation (R 2 adjusted) was used. The level of significance was 5%. Statistical analysis was performed using SPSS Version 21.0 for Mac (IBM).
Results
Participants
During the period evaluated, 651 surgeries were performed for rotator cuff repair. A total of 84 open procedures, 10 debridement procedures, 26 cases with previous shoulder surgery, 12 patients without postoperative clinical evaluation, and 19 patients with incomplete pre- or perioperative evaluation data were excluded. The analyzed sample consisted of 474 patients (500 shoulders) (Figure 1). Data imputation was necessary in the functional assessment in 31 cases (6.2%) at 6 months, 39 cases (7.8%) at 12 months, and 76 cases (15.2%) at 24 months.
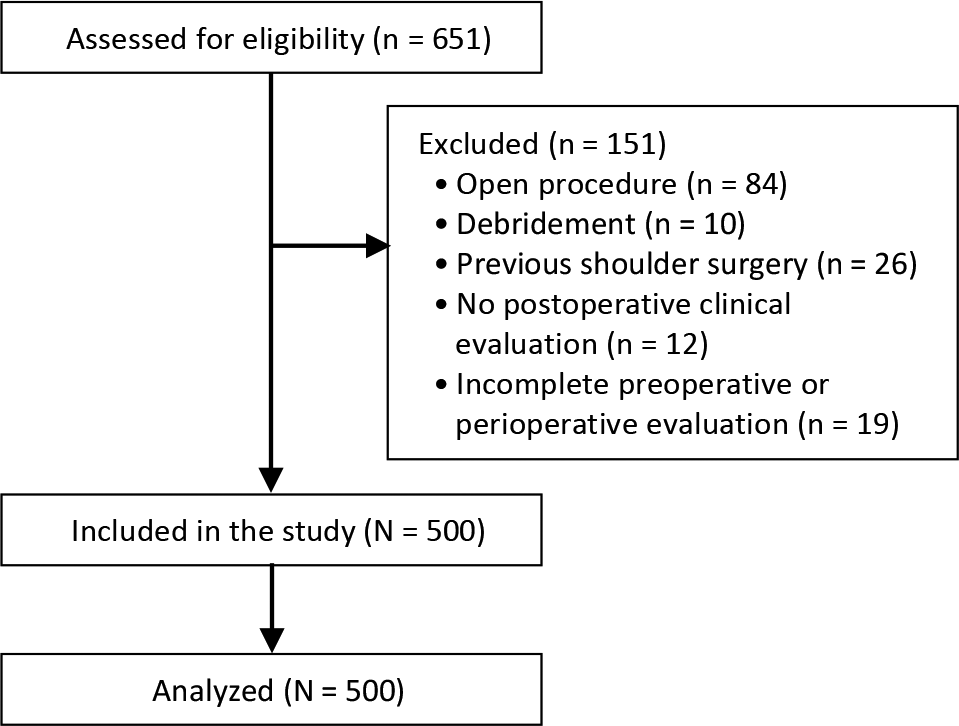
Flowchart of participant enrollment.
Patient, Lesion, and Surgery Characteristics
The study sample predominantly comprised female patients with a median age of 57 years, with most injuries involving the dominant side (Table 1).
Variables Related to Patients a

a Data are reported as n (%) unless otherwise indicated. IQR, interquartile range.
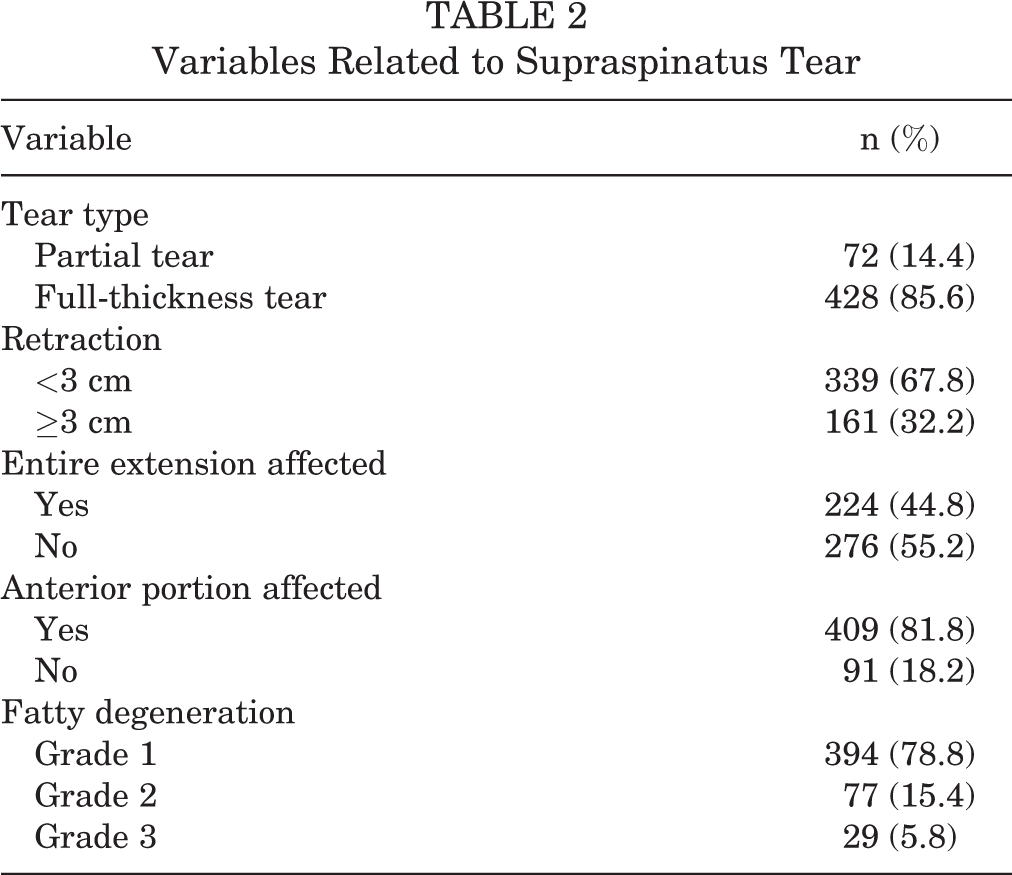
The supraspinatus tendon was involved in all cases, with full-thickness tear in 85.6% of the cases, and in 67.8% of the shoulders the retraction was <3cm (Table 2). Full-thickness tear of the infraspinatus occurred in 20.2% and of the subscapularis in 16.2%. The muscle bellies were mostly classified as Fuchs grade 1, with minimal or no fatty degeneration (Table 3). Most patients had the long head of the biceps intact and had no glenohumeral arthrosis (Table 4).
Variables Related to Supraspinatus Tear
Variables Related to Infraspinatus and Subscapularis Tear

Variables Related to Biceps and Glenohumeral Arthrosis

Acromioplasty was performed in 73% of cases, and complete repair of the rotator cuff was possible in 91.4% of cases (Table 5). In the posterosuperior tears (supraspinatus and infraspinatus), the repair was performed with 1 anchor in 143 cases, 2 anchors in 279 cases, 3 anchors in 61 cases, and 4 anchors in 17 cases. In the subscapularis tears, 176 cases used 1 anchor and 30 cases used 2 anchors. In 294 cases, there was no repair.
Variables Related to Surgical Procedure

Clinical Outcomes
Significant postoperative improvement was seen according to both clinical scores. The ASES score improved from a median of 41.6 preoperatively to 88.3 at 24 months (P < .001), and the UCLA score improved from a median of 14 to 32 (P < .001) (Table 6).
Comparison of ASES and UCLA Scores by Evaluation Time a

a ASES, American Shoulder and Elbow Surgeons standardized shoulder assessment form; IQR, interquartile range; UCLA, University of California, Los Angeles shoulder rating scale.
b Statistically significant difference in all comparisons (P < .05, Wilcoxon signed-rank test).
c Statistically significant difference in all comparisons (P < .05, Wilcoxon signed-rank test) except between 12 and 24 months (P = .078).
Prognostic Factors: Multiple Linear Regression Analysis
We observed that the independent factors for higher 24-month ASES scores were male sex, absence of rheumatologic disease, older age, lower degree of supraspinatus fatty degeneration, concomitant acromioplasty, and higher preoperative ASES score (Table 7). The exclusion of the independent variables with P ≥ .1 did not improve the model, and the independent variables that showed prediction remained the same. Thus, we chose to consider the model with the best correlation coefficient (r) and total explained variation (R 2 adjusted), which was the one with all the independent variables included. The r value obtained was 0.384, R 2 was 0.147, and the adjusted R 2 was 0.093.
Results of Multivariate Analysis a

a ASES, American Shoulder and Elbow Surgeons standardized shoulder assessment form.
b Statistically significant (P < .05).
Discussion
Our results showed that male sex, the absence of rheumatologic disease, older age, lower degree of supraspinatus fatty degeneration, concomitant acromioplasty, and higher preoperative ASES score are independent prognostic factors for better functional results after rotator cuff repair.
Previous studies with univariate 9,32 and multivariate 10 analysis demonstrate that male sex is related to higher postoperative scores, in agreement with our finding. Jenssen et al 17 and Pécora et al, 34 however, did not find a correlation between sex and functional results. We believe that the use in other studies of scales with a more objective assessment of strength, such as the Constant-Murley and UCLA scores, or those with more specific questions about physical activity, such as the Western Ontario Rotator Cuff Index (WORC), can partially explain this difference compared with our results, which were based on the ASES scale. Our institution applies the ASES and UCLA scores in postoperative rotator cuff evaluations. These are the second and third most used scales in the main scientific publications. 23 The ASES scale is highly correlated with the WORC and has less responder and administrator burden, 2 which at least partially supports the scale used as the main outcome in our study.
Our finding regarding the negative influence of rheumatologic diseases contrasts with the data from Jenssen et al, 17 who did not find a correlation using the WORC. We believe that the small sample of rheumatologic patients in both series (5.6%) may justify these variations. Furthermore, the severity of the disease and the medications used are not specified in the studies, where the variable is treated in a binary way. With the effective treatment for rheumatologic diseases becoming more available, perhaps the influence of these comorbidities on rotator cuff repair outcomes may not be as great in the future.
Regarding age, Jenssen et al 17 observed the same pattern found by us, showing a direct correlation between age and clinical results. Frangiamore et al, 10 in turn, did not observe a correlation between age and the ASES score. Several studies using univariate analysis 9,32,33,35,38 have observed that increasing age is correlated with worse clinical outcomes. However, this is possibly caused by confounding factors, since elderly patients may have larger lesions, greater fatty degeneration, and other changes that may negatively influence the clinical outcome. Raman et al, 36 in a meta-analysis of prognostic studies, observed that age did not influence clinical outcomes. However, this article, published in 2017, did not assess data from the most recent articles, 10,17 which are precisely the ones with the largest samples. We believe that possible explanations for a clinical improvement with age are a lower functional demand of the elderly and the fact that the scales used in our study do not specifically assess muscle strength.
Fatty degeneration of the supraspinatus muscle was shown to be an independent factor for worse functional results in our study. Other studies, involving univariate 9,33 and multivariate 8,19 analysis, reach the same result. However, for more recent studies and with a larger sample, 10,17 this variable did not prove to be an independent factor for the functional results. Jenssen et al 17 observed that infraspinatus atrophy correlates with worse clinical results, a variable that we did not assess. Similarly to Frangiamore et al, 10 we emphasize that patients with advanced fatty degeneration are often not ideal candidates for rotator cuff repair and may undergo muscle transfers or arthroplasties. Thus, there is a selection bias that can reduce the impact of this variable. It is noteworthy that only fatty degeneration of the supraspinatus was shown to be a risk factor in our study, without influence of subscapularis and infraspinatus involvement. A possible explanation for this is the frequency of supraspinatus full-thickness tear, which is much higher than that of other tendons.
The performance of acromioplasty proved to be an independent factor associated with better functional results, a finding compatible with that presented by Jenssen et al. 17 Conversely, randomized trials demonstrate that performing acromioplasty together with rotator cuff repair does not interfere with functional results. 1,12,22,27 Sun et al, 43 in a meta-analysis, did not observe differences in postoperative scores between patients undergoing acromioplasty or not, according to the ASES, UCLA, and visual analog scale for pain scores. The findings obtained by studies of prognostic factors open the possibility that acromioplasty may have a beneficial, albeit marginal, effect on rotator cuff repair, which is eventually only observed in large samples, not possible in most randomized studies. Another possibility is that the multivariate analysis does not include all confounding factors in its model, which can lead to bias in data analysis. Also, there could have been a bias in the indication of acromioplasty, being less performed in more complex cases. We believe that acromioplasty facilitates rotator cuff repair, as it improves visualization and reduces impingement between the tendon and the acromion.
Regarding the positive correlation found between pre- and postoperative scores, our data are compatible with those presented by Jenssen et al, 17 who used the WORC scale. Frangiamore et al, 10 in turn, did not observe the influence of preoperative scores by the ASES scale on clinical results. They note that a lower score obtained in the 12-Item Short Form Health Survey correlates with worse postoperative results by this scale. As functional assessment in shoulder surgery involves subjective measures, the perception of results by patients may have influenced the scores, and the responsiveness of the shoulder outcome scales is variable and could explain the different results found in previous studies.
In our sample, smoking was not identified as a risk factor for worse functional results. Frangiamore et al 10 did not assess this variable, and our result contrasts with that presented by Jenssen et al. 17 The literature also diverges when analyzing comparative studies. Naimark et al, 29 in a retrospective cohort study, observed that smoking leads to worse functional outcomes, while Baumgarten et al 3 observed that smokers and nonsmokers showed similar improvement with rotator cuff repair. A possible explanation for this discrepancy concerns the criteria for considering a patient as a smoker. Jenssen et al considered this variable as present when consumption was >10 cigarettes per day, while in our study the comparison groups were composed of nonsmokers, former smokers, and smokers, regardless of daily consumption and time of use. It is expected that tobacco consumption negatively affects tendon healing because of the toxins present in its composition. Nicotine is a potent vasoconstrictor, which can reduce blood supply at the tendon insertion. Carbon monoxide, in turn, reduces the levels of oxygen available for cellular metabolism. 29
Workers’ compensation status was also not shown to be a risk factor in our sample. Jenssen et al 17 did not assess this variable, and in the study by Frangiamore et al, 10 this was an independent risk factor for worse clinical outcomes. A previous systematic review 36 demonstrated that workers’ compensation status was correlated with worse functional results. The discrepancy between our findings and other studies may be due to characteristics of the population of our country, including the mean age for retirement and percentage of manual workers, data that were not particularized in the studies.
In our study, rotator cuff tear size was not shown to be a risk factor for worse clinical outcomes. These findings are in agreement with those of other authors. 10,17 The findings of these 2 studies 10,17 and our present study carried out with large samples differ from those pointed out in other studies with multivariate analysis, which involve smaller samples, 4,8,19,31,44,45 where tear size 19,31,44,45 and infraspinatus retraction 4 are described as independent risk factors for worse clinical outcomes. We believe that more robust samples lead to less bias and that the repairability of the lesion is more important than its dimension. However, it is important to highlight that our sample has a small number of large or massive tears and that the presence of complete repair was not shown as a prognostic factor in our study, different from what was pointed out by Jenssen et al. 17
We did not find that tear or instability of the long head of the biceps was an independent factor for worse clinical results. The data regarding the influence of the biceps tear agree with those of Jenssen et al 17 and disagree with those of studies with lower sample sizes, in which involvement of the long head of the biceps was correlated with worse clinical results. 15,45 We did not find studies that assessed the influence of biceps stability on clinical results. Regarding the procedures performed on the long head of the biceps, we observed that they are not a factor that influence the surgical results, as reported by Saccomanno et al. 40
Dominant-side injury, history of trauma to the shoulder, and diabetes were not correlated in our study with worse functional results. These findings are similar to those pointed out by Jenssen et al, 17 while Frangiamore et al 10 did not assess those variables. As for diabetes, Lu et al, 21 in a meta-analysis, observed that the ASES and UCLA scores did not differ in the postoperative period between patients with diabetes and those without, while according to the Constant-Murley scale, patients without diabetes had a higher score, but it did not reach clinical relevance. We also observed that the performance of previous injections in the shoulder does not influence the clinical result. This variable has not been analyzed by other studies of prognostic factors. We also noted that the presence of arthrosis in the shoulder did not influence the clinical results. This variable has not been studied by other authors. 10,17 It is noteworthy that we included in our study only patients with mild arthrosis, and the data should not be generalized to cases of moderate or severe arthrosis. Furthermore, this event was present in only 7.8% of our sample, and therefore, the finding must be viewed with caution.
In our sample, partial repair was not shown to be a factor related to worse clinical outcomes. This finding was unexpected and contrasts with what was reported by Jenssen et al. 17 A possible reason for this disagreement is the low number of partial repairs in both studies (8.6% and 4.6%, respectively). A low frequency of events increases the possibility of bias. It is noteworthy that the structural result of the repair does not necessarily correlate with clinical outcomes. 13
Distal clavicle resection did not influence the clinical results in our sample, similarly to Jenssen et al. 17 Similarly, Wang et al, 46 in a meta-analysis, did not find an influence of distal clavicle resection on the results of rotator cuff repair. This suggests that an excision of the distal clavicle in a symptomatic acromioclavicular joint does not lead to worse results, but we cannot say whether equal results would be obtained if the procedure were not performed. The suture technique (single or double row) also did not influence the result in our study, which is compatible with the meta-analysis by Sobhy et al. 42 The studies by Jenssen et al 17 and Frangiamore et al 10 did not assess these data, as they performed essentially single- and double-row repairs, respectively. It is worth emphasizing again that the frequency of cases with distal clavicle resection and double-row repair is low in our study.
In the multiple linear regression analysis, the R 2 value observed by us was 0.147. This indicator demonstrates how much of the final functional result can be explained by the statistical model. Jenssen et al 17 reported a value higher than ours (R 2 = 0.360 ). Frangiamore et al, 10 although reporting the importance of this indicator, did not include it in their results. We believe that the difficulty of prognostic models in obtaining a high predictability index is because rotator cuff syndrome is a multifactorial disease, with several influencing factors not yet known or only partially known. An advance in knowledge about risk factors, associated with broader databases and evaluation of multiple studies in meta-analyses, may lead to more robust models in the future.
There are few studies evaluating prognostic factors for clinical outcomes after rotator cuff repair, involving multivariate analysis to control confounding factors and a large sample. As highlights, we can mention Jenssen et al, 17 who analyzed 647 patients, and Frangiamore et al, 10 with a sample of 449 shoulders. Other authors, such as Flurin et al 9 and Feng et al, 7 although using large samples of patients (576 and 1067, respectively), did not perform multivariate analysis to control confounding factors for the clinical outcome.
We chose to evaluate only arthroscopic rotator cuff repairs, similarly to other authors. 10,17 However, our sample included only previously unoperated shoulders, unlike other studies, which account for 5% to 13% of reoperations in their samples. 10,17 In addition, we included injuries in which at least partial repair was possible, similar to Jenssen et al, 17 but different from the study performed by Frangiamore et al. 10 The choice to include these cases was because certainty about the repairability of the lesion is often only possible during the surgical procedure, and we believe that a prognostic factor that can be applied before surgery is more useful than one during the procedure. Another factor that brings our sample closer to that of Jenssen et al but departs from that of Frangiamore et al is that we included any rotator cuff tear and not just full-thickness tears that necessarily involved the supraspinatus. The path adopted by us decreased the homogeneity of the sample but increased the external validity of the study. Cases of open surgery, revision procedures, or isolated repair of the subscapularis or infraspinatus may not be adequately predicted by our model.
The procedures in our study were performed by several surgeons, and repairs were predominantly single row, similar to the study of Jenssen et al, 17 but different from that of Frangiamore et al, 10 who analyzed a cohort operated on by a single surgeon performing double-row repairs. Finally, we applied the clinical scales at defined periods, with the last assessment taking place at 24 months. Jenssen et al, despite having a mean follow-up of 25 months, applied the scales between 17 and 66 months after the procedure, while Frangiamore et al used a minimum follow-up time of 2 years but included follow-up of up to 11 years in the sample. We consider that the evaluation at predetermined times generates greater data consistency.
Limitations
This study has some limitations. First, it was based on a retrospective cohort, and although we collected the data prospectively, our study may have biases inherent to this design. Although several perioperative factors have been evaluated, they do not represent all the variables that can influence the clinical outcome. Most of the patients in our sample had isolated supraspinatus tears, without major retraction. Therefore, extrapolation of the results to massive tears with involvement of multiple tendons should be viewed with caution. We emphasize that some variables analyzed, such as double-row repair, distal clavicle resection, and rheumatologic disease, have a low occurrence, and the results obtained in these findings should be viewed with caution. Each surgeon evaluated the MRI of the surgery he performed, which did not allow for the assessment of inter- and intraobserver agreement. We also did not use a disease-specific outcome measure, nor did we assess the number of patients achieving the minimal clinically important difference. Because of the loss to follow-up, approximately 15% of the patients had random and nonsystematic loss and required data imputation based on the 12-month assessment. This approach does not generate a significant bias in our understanding, since it has been shown that the clinical evaluations do not differ markedly between 12 and 24 months. 47 Finally, the prognostic factors for the structural outcome were not evaluated in this study, since it is not our routine to perform postoperative MRI. It is noteworthy that retears after rotator cuff repair are frequent, affecting approximately 27% of patients, 26 and clinical results do not correlate with structural integrity. 39 We emphasize as a favorable point of our study the use of a wide sample, comparable with the best published articles on the subject, 10,17 evaluating a considerable number of pre- and perioperative factors. Broad inclusion criteria and different patterns of rotator cuff lesion allow the study to have high external validity. We believe that the data provided in this study can be useful for both orthopaedists and patients, collaborating with decision making on surgery for rotator cuff repair.
Conclusion
The prognostic factors for better clinical results after arthroscopic repair of the rotator cuff were male sex, absence of rheumatologic disease, older age, lower degree of fatty degeneration of the supraspinatus muscle, concomitant acromioplasty, and higher preoperative scores, according to the ASES scale at 24 months.
Footnotes
Final revision submitted December 8, 2022; accepted January 17, 2023.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Hospital das Clinicas HCFMUSP, Faculdade de Medicina, Universidade de São Paulo (protocol No. 2.778.930).