
Abstract
Background:
Bridge-enhanced anterior cruciate ligament restoration (BEAR) combines suture repair of the anterior cruciate ligament (ACL) with an extracellular matrix implant plus autologous blood to facilitate native ACL healing.
Purpose/Hypothesis:
The purpose of this study was to compare the 6-year follow-up outcomes of patients who underwent the BEAR procedure with those of a nonrandomized concurrent control group receiving autograft ACL reconstruction (ACLR) in the first-in-human safety study of the BEAR implant (BEAR I trial). Based on the 2-year results, it was hypothesized that isometric hamstring strength after the BEAR procedure would be greater than that after ACLR and that there would be no other differences in outcomes at 6 years.
Study Design:
Cohort study, Level of evidence, 2.
Methods:
Ten patients underwent BEAR and 10 received ACLR with a 4-stranded hamstring autograft. Outcomes assessed included the record of subsequent surgeries, the International Knee Documentation Committee (IKDC) Subjective Knee Score, IKDC physical examination grade, the Knee injury and Osteoarthritis Outcome Score, instrumented knee laxity, functional outcomes (ie, muscle strength assessments and hop testing), and qualitative magnetic resonance imaging assessment. Comparisons between treatments were based on computations of the mean differences and the associated 95% CIs.
Results:
One patient in the BEAR group and 3 patients in the ACLR group were lost to follow-up. In the period between 2 and 6 years, 1 patient in each group underwent revision surgery. There were no differences between groups at the 6-year follow-up in any of the outcome measures except for isometric hamstring strength, which was approximately equal to that of the contralateral knee in the BEAR group and <44% of that in the contralateral knee in the ACLR group (P < .01).
Conclusion:
This preliminary study suggests that the outcomes of BEAR and ACLR with a hamstring tendon graft may be similar at the 6-year follow-up and warrants investigation of the BEAR procedure in a larger cohort of patients.
Keywords
Anterior cruciate ligament (ACL) reconstruction (ACLR) is the gold standard treatment for active patients who sustain an ACL injury and are evaluated with functional disability. While ACLR is regarded as a successful procedure, knee biomechanics are not fully restored,42,47 the subsequent reinjury rate has been reported to be as high as 25% in young patients, 44 and patients remain at risk for posttraumatic osteoarthritis. 4 There is a need for new procedures that could potentially improve outcomes and reduce cartilage degradation after an acute ACL injury.
The bridge-enhanced ACL restoration (BEAR) procedure, which augments a suture repair with an extracellular matrix implant saturated with autologous blood to facilitate native tissue healing, 25 has recently been introduced as an alternative to ACLR. 32 Preclinical studies in the porcine model have demonstrated that the implant stimulates ACL healing, 25 produces biomechanical outcomes that are equivalent to ACLR,26,43 and results in less cartilage damage than that seen after ACLR.19,26 The mechanism of chondroprotection after the restoration procedure remains unknown. Nonetheless, these preclinical studies led to US Food and Drug Administration (FDA) approval 34 for the first-in-human BEAR I trial (NCT02292004),28,29 which was designed primarily to demonstrate that the implant was safe 28 and secondarily to provide preliminary data comparing outcomes between BEAR and ACLR. 29 The safety data from the BEAR I trial 28 provided the data necessary to obtain FDA approval for the first randomized controlled trial (BEAR II trial; NCT02664545) comparing BEAR versus ACLR at 2 years. 27
The 2-year follow-up data from the first 2 BEAR trials determined that the BEAR implant was safe,28,29 that the clinical and patient-reported outcomes of the BEAR procedure were noninferior to those of ACLR,27,29 and that hamstring function was improved after BEAR as this procedure does not require an autograft harvest from the hamstring tendon.27,29 However, long-term assessments were still needed to determine if the 2-year results of BEAR would be maintained. Therefore, the objective of the current study was to compare clinical, functional, patient-reported, and imaging outcomes of the BEAR cohort with those of the ACLR cohort at the 6-year follow-up in the patients enrolled in the BEAR I trial.28,29 Based on the 2-year results, 29 we hypothesized that isometric hamstring strength after BEAR would remain greater than that after ACLR and that there would be no other differences in outcomes at the 6-year follow-up.
Methods
Trial Design
An investigational device exemption (G140151) from the FDA and institutional review board approval from Boston Children's Hospital were obtained before initiating the study. All patients provided their informed consent before enrollment. Patient recruitment was initiated in February 2015 and completed in October 2015. The trial was registered at ClinicalTrials.gov (NCT02292004).
Details of the study design have been previously reported. 28 In summary, the BEAR I cohort study was constructed as an interventional, parallel-assignment, nonrandomized trial. All surgical procedures were performed at a single site (Boston Children's Hospital) by 1 surgeon (L.J.M.), and the postoperative assessments were performed by independent examiners blinded to surgical limb and treatment groups. Ten patients underwent primary surgery in each of the BEAR (interventional) and ACLR (control) groups and were evaluated preoperatively, intraoperatively, and postoperatively at 3, 6, 12, and 24 months (2 years), the data from which have been previously published.28,29 For the current report, the patients again gave consent and data were acquired at the 6-year follow-up to perform group comparisons at the later time point.
Patients
The inclusion criteria for the BEAR I trial have been previously reported. 28 In summary, patients with a complete midsubstance tear were recruited if they were between the ages of 18 and 35, were <1 month from the time of injury, and had an ACL tibial stump of at least 50% on magnetic resonance imaging (MRI). Patients with a complete ACL tear and who were within 3 months of injury were eligible to enroll in the ACLR group; however, the 50% stump length was not an inclusion criterion. Patients were excluded from both groups if they had a history of other knee injuries or risk factors that could potentially affect healing, including a bucket-handle tear of the medial meniscus, a full-thickness chondral injury, a grade 3 medial collateral ligament injury, concurrent patellar dislocation, or a posterolateral corner injury.
Of the 20 patients who received the allocated interventions, 9 of the BEAR group and 7 of the ACLR group were successfully contacted to participate in the 6-year follow-up assessment (Figure 1). Therefore, 1 patient (10%) in the BEAR group and 3 (30%) in the ACLR group were lost to follow-up. Reinjury status was established for all patients contacted at 6 years. However, the number of patients who returned on-site for all follow-up assessments was as low as 5 per group, as shown in Figure 1.

STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) diagram for the BEAR I trial at the 6-year follow-up. ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; BEAR, bridge-enhanced anterior cruciate ligament restoration; Sx, surgery; eval, evaluation; IKDC, International Knee Documentation Committee Subjective Knee Score; KOOS, Knee injury and Osteoarthritis Outcome Score; KT/Exam, KT-1000 arthrometer examination; MRI, magnetic resonance imaging.
BEAR Procedure
The BEAR procedure used a resorbable implant that was saturated with the patient's blood to facilitate functional healing of the ACL. 32 The implant was composed of bovine extracellular matrix proteins, mainly collagen, which holds autologous blood between the torn ligament ends so that healing can occur. The scaffolding implants were manufactured at Boston Children's Hospital. 34 The implants were 22 mm in diameter and 45 mm in length and were inserted into the intercondylar notch through a mini-arthrotomy as the autologous blood was added to it.
Surgical details for the BEAR procedure have been previously published.28,29 In brief, an absorbable suture (Vicryl; Ethicon) was placed in the tibial stump via a whipstitch. A cortical button combined with a polyester suture stent (Ethibond; Ethicon) was passed through the femoral tunnel and secured to the distal lateral femoral cortex. The polyester sutures were threaded through the BEAR implant and a tibial tunnel and then secured to the tibial cortex using a second extracortical button (Endobutton; Smith+Nephew). The implant was saturated with 5 to 10 mL of the patient's blood, and the tibial stump was embedded in the saturated implant by pulling on the ends of the absorbable suture, which were then secured to the femoral cortical button to finish the procedure. The postoperative rehabilitation protocol was standardized 29 and followed that commonly prescribed for after ACLR.45,46
ACLR Procedure
A standard arthroscopically assisted hamstring tendon autograft procedure was performed using a quadrupled semitendinosus-gracilis graft and suspensory fixation with a cortical button on the femur. The knees were placed in extension, maximally tensioned by the surgeon, and fixed in the tibial tunnel using a bioabsorbable interference screw (BioRCI HA; Smith+Nephew). The same postoperative rehabilitation program used for the BEAR group was prescribed.
Outcome Assessments
Subsequent Knee Injury Assessment/Patient-Reported Outcome Measures
All patients who responded to the invitation to participate in the 6-year follow-up were asked about any subsequent knee surgeries to either limb. The postsurgical procedures were verified via the patient's clinical record. Subsequent knee injury and patient-reported outcome data from patients were obtained via a telephone call if they were unable to come into the clinic for their 6-year on-site follow-up visit.
The International Knee Documentation Committee (IKDC) Subjective Knee Score 14 and Knee injury and Osteoarthritis Outcome Score (KOOS) 37 were used to evaluate patient-reported outcomes at 6 years. 28 The IKDC subjective score was developed and validated to document health-related quality of life in patients with knee problems. 14 Similarly, the KOOS evaluates 5 knee-related domains: (1) Pain, (2) Symptoms, (3) Activities of Daily Living, (4) Sport and Recreation, and (5) Quality of Life. 37 Questionnaire data were recorded from all contacted patients even if they were unable to come into the clinic for their 6-year follow-up visit.
IKDC Physical Examination
The physical examination was performed following the guidelines of the IKDC. 16 For the patients who returned on-site, knee effusion (subjective grading), range of motion (goniometry), and knee stability measures (manual Lachman test and pivot-shift test) were recorded individually and then combined to generate an overall IKDC physical examination grade (A = normal, B = nearly normal, C = abnormal, D = severely abnormal). 16 The overall grade was defined as the worst of the effusion, range of motion, and knee stability grades. For range of motion, the difference between the surgical and nonsurgical knees for passive range of motion was used. The Lachman and pivot-shift tests were performed on both knees under anesthesia for the baseline values and without anesthesia at all follow-up visits. The differences between the surgical knee and contralateral knee were reported for all knee stability measures. An independent examiner performed the tests, and knee sleeves were used to cover both knees during testing to blind the examiner to the surgical side and study group assignment. Effusion was subjectively evaluated after removal of the sleeves at the end of the clinical examination.
Arthrometer Test
A commercial arthrometer (KT-1000; MEDMetric) was used to measure the anterior displacement of the tibia with respect to the femur under 130 N of applied anterior force. The anterior laxity measure was performed on each leg in duplicate, and the results were reported as a side-to-side difference between limbs (mean of the surgical knee minus mean of the contralateral knee). All arthrometer measurements were performed by an independent examiner blinded to surgical laterality and treatment using the knee sleeves.
Functional Outcome Measures
Muscle strength and functional assessments were performed on patients returning on-site. Isometric hamstring, quadriceps, and hip abductor muscle strengths were measured using a handheld dynamometer (Microfet 2; Hoggan Scientific, LLC). 23 The isometric hamstring strength was measured with the patient prone, the knee in 90° of flexion, and the dynamometer placed proximal to the ankle. The isometric hip abductor strength was measured from a side-lying patient with the dynamometer placed over the midlateral thigh. The isometric quadriceps strength was measured with the knee at 90° of flexion with the dynamometer located at the distal tibia. Isokinetic strength testing (Biodex 3; Biodex Medical Systems) was performed at 60 deg/s to measure the isokinetic peak knee extension and flexion torques. 8 Patients also performed single-hop, triple-hop, 6-m timed hop, and crossover hop tests as previously described. 30 All muscle and functional measures were performed on each leg in duplicate and averaged for further analyses. Results were normalized by expressing the injured knee result as a percentage of the uninjured contralateral knee result for all strength and hop testing measures.
MRI Assessment
The patients returning on-site at 6 years underwent standard MRI of the knee on a 3-T scanner (Tim Trio; Siemens), which included a sagittal proton-density (intermediate-weighted) sequence (Repetition Time/Time to Echo (TR/TE), 1000/38; flip angle, 120°; slice thickness, 0.8 mm, voxel size, 0.5 × 0.5 × 0.8) and a sagittal double-echo steady-state sequence (TR/TE, 16.1/5.4; flip angle, 30°; slice thickness, 0.8 mm; voxel size, 0.3 × 0.3 × 0.8) to qualitatively evaluate ACL or ACL graft integrity, synovitis, degree of effusion, and arthrofibrosis. A musculoskeletal radiologist (K.E.) reviewed the images to determine the continuity of fibers and signal intensity of the ACL (BEAR) or graft (ACLR) and to evaluate the extent of arthrofibrosis, effusion, and/or synovitis in the knee. For the 2 patients in whom the ipsilateral ACL or ACL graft failures were revised (1 BEAR, 1 ACLR), the MRI scan was used to verify failure at time of the reinjury.
Statistical Analysis
For each continuous outcome measure, cross-sectional comparisons between the BEAR and ACLR groups at 6 years were performed, as was consistent with the previously reported 2-year analysis. 29 The comparisons were based on the computations of the mean differences and associated 95% CIs. This analysis is more informative than presenting the observed significance level (ie, P values) as it provides an interval estimate for the plausible magnitude of the true difference between groups for each outcome. Statistical significance based on an α of .05 can be inferred based on the constructed 95% CI, excluding a mean group difference of zero. Missing data were not considered in the analysis as these data were not available. Because group means across time points are based on different sample sizes, the focus should be on cross-sectional comparisons, not longitudinal changes, as the latter are potentially confounded with individual patient effects. The power to detect group differences at the 6-year time point was estimated to be 80% for large effect sizes (Cohen d, 1.75-2.00), depending on the sample size associated with each outcome measure. Additionally, frequency distributions are presented for categorical outcomes at each assessment time point. All analyses were performed using SAS statistical software (SAS Institute).
Results
Baseline Characteristics
The baseline characteristics and intraoperative findings for the 2 groups have been previously reported.28,29 In summary, the 2 groups were similar in age, sex, race, and body mass index. It should be noted that the mean time from injury to surgery was significantly longer (P < .001) in the ACLR group compared with the BEAR group (52.9 vs 20.8 days, respectively), although this would unlikely affect the results as the injuries would still be considered acute. Preoperative side-to-side differences in the knee arthrometer measurements were similar between groups (BEAR: 5.2 ± 1.4 mm; ACLR: 5.0 ± 2.5 mm), and all patients had either a “glide” or “clunk” with pivot-shift testing under anesthesia. The mean preinjury Marx activity level was 12.8 ± 3.7 in the BEAR group and 10.9 ± 5.9 in the ACLR group. Nine of the 10 patients in both groups experienced a noncontact injury. The number of patients with concomitant meniscal tears, which were either repaired or excised, were similar between groups (4 BEAR, 5 ACLR).28,29 The degree of effusion at the time of surgery was also similar (BEAR: 1.3 ± 0.7; ACLR: 0.9 ± 0.8). 28
Subsequent Surgeries
At 6-year follow-up, the number of subsequent surgeries was similar between the 2 surgical groups (Table 1). There were 2 ipsilateral revision surgeries, 1 in each group, and a contralateral ACL surgery in the BEAR group. All the subsequent ACL or graft injuries that were revised occurred after the 2-year follow-up visit. 29 One patient in the ACLR group and 1 patient in the BEAR group had a subsequent medial meniscus resection for a meniscal injury. One patient in the ACLR group underwent arthroscopic debridement for arthrofibrosis, and 1 patient in the BEAR group underwent surgical removal of the tibial cortical button for discomfort (Table 1).
Additional Knee Surgeries at 6-Year Follow-up a

Data are presented as n (%). Four patients did not consent to long-term follow-up and did not have any data collected at the 6-year time point. ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; BEAR, bridge-enhanced anterior cruciate ligament restoration.
Patient-Reported Outcomes
The patient-reported outcome scores at baseline, 2 years, and 6 years are provided in Table 2 and detailed in the Supplemental Figures. For the IKDC subjective scores and the 5 domains of the KOOS, there were no significant differences between groups at 6 years.
PRO Scores a
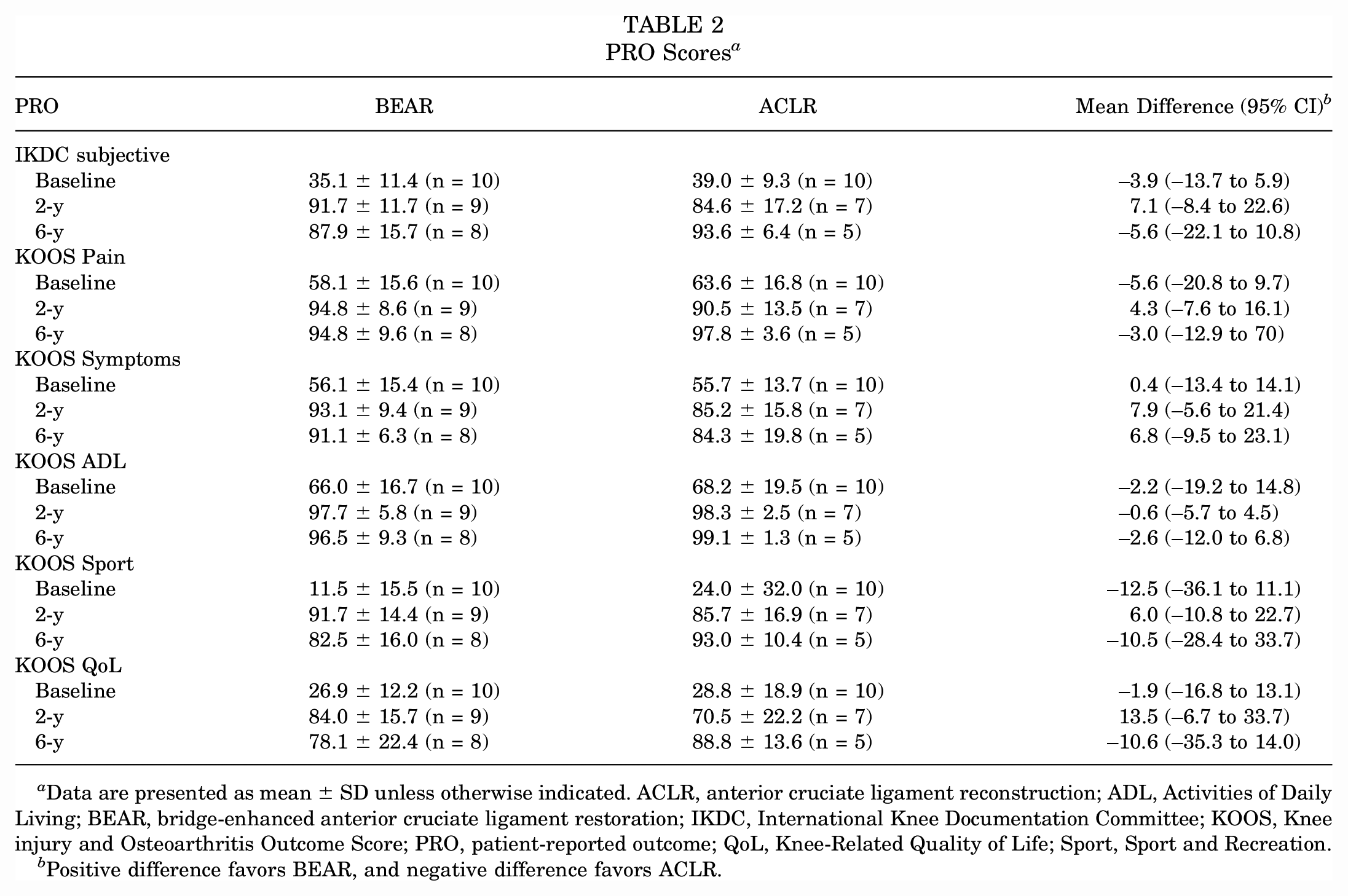
Data are presented as mean ± SD unless otherwise indicated. ACLR, anterior cruciate ligament reconstruction; ADL, Activities of Daily Living; BEAR, bridge-enhanced anterior cruciate ligament restoration; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; PRO, patient-reported outcome; QoL, Knee-Related Quality of Life; Sport, Sport and Recreation.
Positive difference favors BEAR, and negative difference favors ACLR.
Clinical Outcomes
The IKDC physical examination grades at baseline, 2 years, and 6 years are presented in Table 3. Preoperatively, all patients in the BEAR and ACLR groups were evaluated with abnormal or severely abnormal knees. At 6 years, 4 of the 5 patients in the BEAR group who returned for the physical examination were evaluated with a normal surgical knee (grade A) and 1 was evaluated with a nearly normal surgical knee (grade B). To the contrary, 4 of the 5 patients in the ACLR group were evaluated with a nearly normal knee (grade B) and 1 was evaluated with a normal knee (grade A). For the instrumented laxity testing, there were no differences in anterior knee laxity between the BEAR and ACLR knees at the 6-year follow-up (Table 4, Supplemental Figures).
IKDC Objective Grades a

Data are presented as n (%). ACLR, anterior cruciate ligament reconstruction; BEAR, bridge-enhanced anterior cruciate ligament restoration; IKDC, International Knee Documentation Committee.
Side-to-Side Differences in Anterior Knee Laxity a
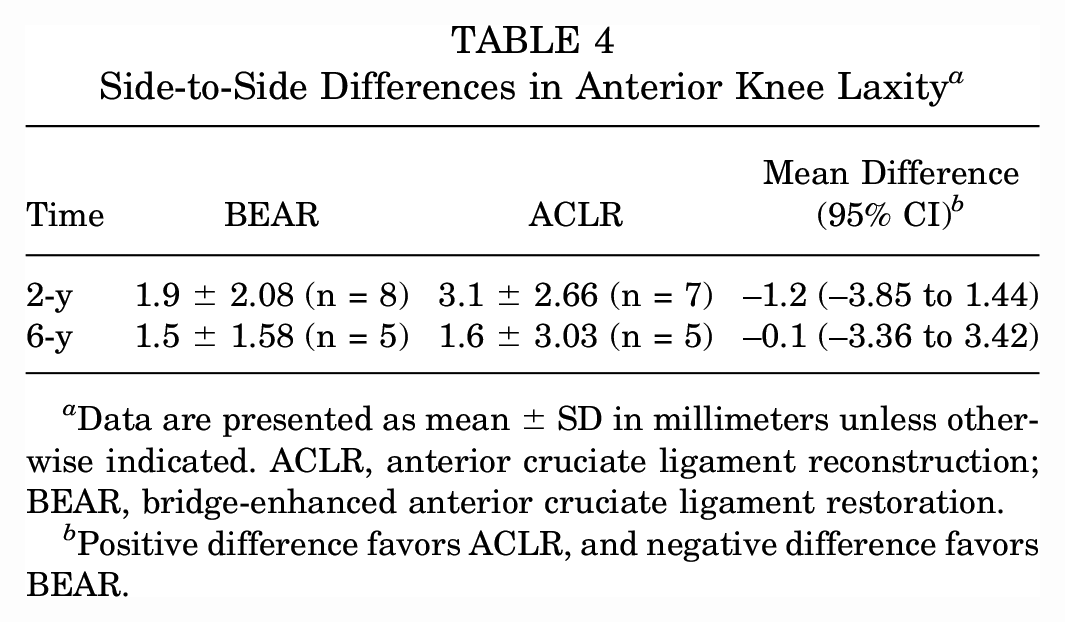
Data are presented as mean ± SD in millimeters unless otherwise indicated. ACLR, anterior cruciate ligament reconstruction; BEAR, bridge-enhanced anterior cruciate ligament restoration.
Positive difference favors ACLR, and negative difference favors BEAR.
Functional Outcomes
The functional outcomes at the 2- and 6-year follow-ups are presented in Table 5 and detailed in the Supplemental Figures. As was seen at 2 years, the isometric hamstring strength was significantly different between groups at 6 years (P < .01). The mean isometric hamstring strength of the BEAR group relative to the contralateral knee was >100%, while that of the ACLR group was 56% at the 6-year follow-up. For the other functional assessments and muscle strength measures, there were no significant differences between treatment groups (Table 5).
Functional Outcomes After ACL Surgery at 2- and 6-Year Follow-up a

Data are presented as mean ± SD unless otherwise indicated. Strength and hop testing results are presented as percentages of the contralateral leg. ACLR, anterior cruciate ligament reconstruction; BEAR, bridge-enhanced anterior cruciate ligament restoration; Iso, isometric.
Positive difference favors BEAR, and negative difference favors ACLR, for all outcomes except the 6-m timed single-leg hop and single-leg squat >60°.
Hamstring strength was significantly better in the BEAR group than in the ACLR group at both time points (P < .05 for comparison between groups at all time points).
MRI Findings
In the 2 patients (1 BEAR and 1 ACLR) who reinjured their ipsilateral knee and had a revision surgery, the MRI readings at the time of reinjury confirmed graft/ligament failure. As these knees were subsequently revised, they were excluded from the 6-year outcomes analyses other than the subsequent injury assessment.
In all patients who did not sustain an ipsilateral ACL reinjury and who were imaged at the 6-year follow-up visit, most of the ligaments (BEAR) or grafts (ACLR) were reported as intact and were deemed to exhibit “postoperative changes that would be expected” after ACL surgery (Figure 2). One of the patients in the BEAR group had evidence of discontinuous fibers (ie, a partial ACL tear). Note that this patient had an IKDC examination score of A, a negative arthrometer finding, an IKDC subjective rating of 95, but a KOOS Knee Related Quality of Life of 69. Of the 6 patients in the BEAR group with intact ligaments, 4 exhibited low ACL signal intensity (ie, indicative of a stronger ligament 7 ), while the ACLs of the remaining 2 patients were heterogeneous (ie, indicative of a weaker ligament 7 ). Five of 6 patients exhibited mild evidence of effusion/synovitis (Figure 3), and 1 had minor signs of arthrofibrosis. Of the 5 patients in the ACLR group with intact grafts, 3 exhibited low graft signal intensity (indicative of a stronger graft 7 ), while the grafts of 2 patients were heterogeneous (indicative of a weaker graft 7 ). Three of the 5 patients in the ACLR group exhibited mild evidence of effusion/synovitis, and 3 had minor signs of arthrofibrosis.
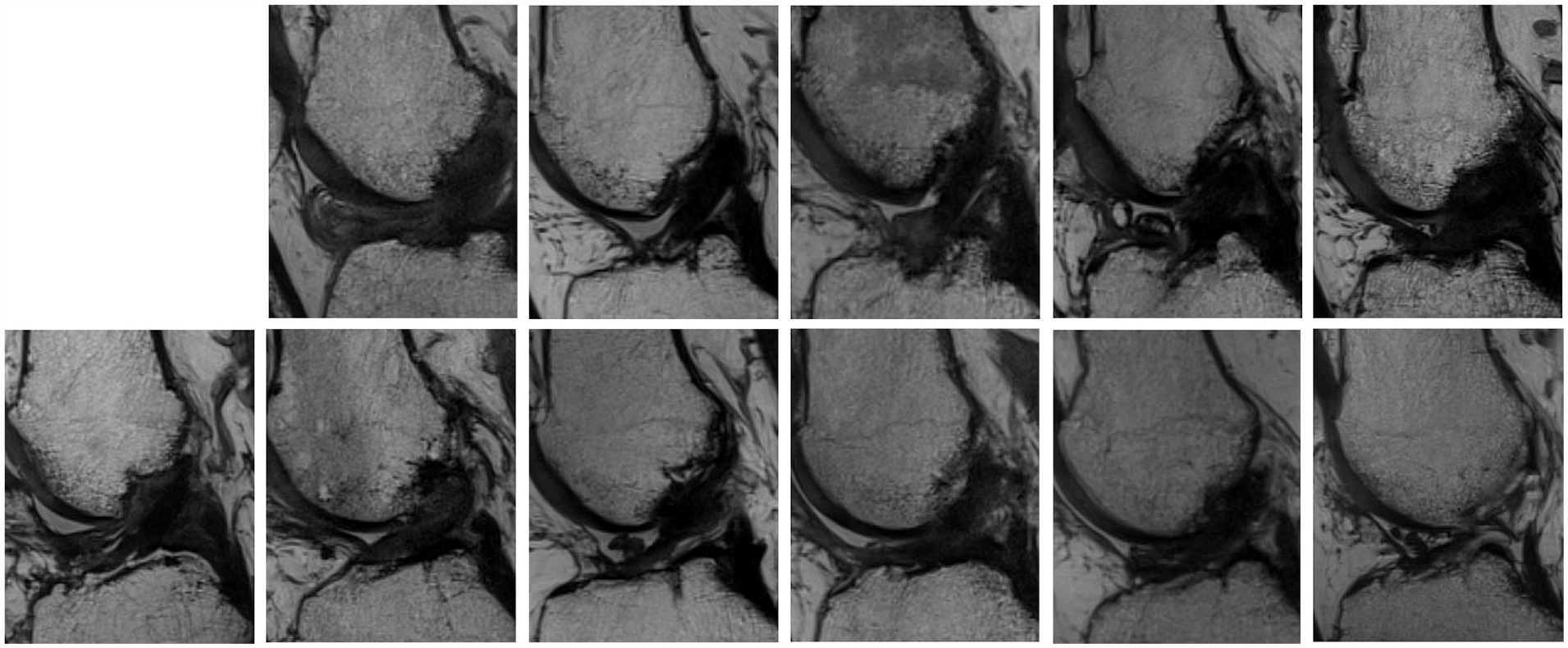
Magnetic resonance imaging scans (proton-density sequence, sagittal view) of the healing anterior cruciate ligament (ACL) or ACL grafts from the 5 ACL reconstructions (top row) and 6 patients in the bridge-enhanced ACL restoration group (bottom row).

Sagittal magnetic resonance imaging scans showing (A) mild (arrow) and (B) normal synovitis on the proton-density sequence and (C) mild (arrow) and (D) normal effusion on the constructive interference in a steady-state sequence taken from the bridge-enhanced anterior cruciate ligament restoration cohort. Magnetic resonance imaging scans from the anterior cruciate ligament reconstruction cohortt (E) with (arrow) and (F) without arthrofibrosis.
Discussion
The most important finding of this study was that patients who underwent the BEAR procedure had outcomes similar to those after ACLR with a hamstring tendon autograft at the 6-year follow-up. The study supported the hypotheses that the isometric hamstring strength after BEAR was greater than that after ACLR at the 6-year follow-up, 29 and there were no other significant differences found between the 2 groups for the other outcome measures. Although the sample sizes for both groups were small, these preliminary data provide the first insight into how patients undergoing the BEAR procedure may fare longer term and support the need for larger studies comparing outcomes of the procedure with the standard of care.
The 6-year BEAR I data were generally similar to the results reported at the 2-year follow-up. 29 Isometric hamstring tendon strength remained significantly greater in the BEAR group compared with the ACLR group, as was the case at the 2-year follow-up. The deficit in the ACLR group is likely because the BEAR procedure does not require graft harvest. IKDC physical examination grades for BEAR were also superior to those after ACLR, another finding that was present at the 2-year follow-up. Approximately two-thirds of patients in each group had ligament or graft tissue with low signal intensity on the 6-year MRI scans. Instrumented anterior laxity values for BEAR and ACLR were similar at the 2- and 6-year follow-ups. While the IKDC and KOOS patient-reported outcomes were not significantly different, it should be noted that the mean KOOS Sport and Recreation and KOOS Knee-Related Quality of Life were 10 points lower for the BEAR group than the ACLR group at 6 years and less than those documented at 2 years. This finding was driven by a large increase in IKDC score and KOOS of 1 patient in the ACLR group (Supplemental Figures). It is interesting to note that the 2-year results of the BEAR I trial were similar to those reported in the 2-year follow-up of the larger BEAR II trial (NCT02664545), in which patients were randomized to receive BEAR or ACLR. 27 It will be interesting to see if the 6-year BEAR II results will follow suit when those data become available.
The outcomes reported for both treatment groups were similar to those previously reported for ACLR. The Multicenter Orthopaedic Outcomes Network (MOON) knee group reported the incidence of subsequent ipsilateral knee surgery at the 6-year follow-up to be 20%, with a graft revision rate of 7.5%. 24 In the Tension trial, the incidence of a subsequent ipsilateral knee surgery was 15% at the 7-year follow-up, with a graft revision rate of 7%. 5 The revision rates of 11 and 14% for the BEAR and ACLR groups at the 6-year follow-up, respectively, are similar to those of the aforementioned studies. It is interesting to note that at the 2-year follow-up, there were no ipsilateral ACL reinjuries within either group in the BEAR I trial. 29 Since the 2-year follow-up, an additional patient in each group underwent another knee surgery: a partial meniscectomy in the ACLR group and hardware removal in the BEAR group. Thus, the overall ipsilateral knee surgery rates (Table 1) were similar to those reported in previous studies.5,10,24 It should also be noted that another patient in the BEAR group had sustained a partial ipsilateral ACL tear that was documented on MRI. However, this was not surgically revised as the reinjured knee was determined to be stable via clinical examination (ie, an IKDC examination rating of grade A and a negative arthrometer laxity side-to-side difference assessment). This patient had an IKDC subjective rating of 95, and a KOOS Knee-Related Quality of Life score of 69.
The IKDC score and KOOS of both groups were also similar to those reported by others after ACLR at similar time points.17,31 The median IKDC subjective score at 6 years for the 2488 patients who underwent ACLR enrolled in the MOON cohort was reported to be 77. 17 At the 5-year follow-up, the mean IKDC subjective score of the early ACLR group of the Delaware-Oslo cohort was 89. 31 The mean IKDC subjective scores at 6 years for the BEAR and ACLR groups were 88 and 94, respectively and not significantly different from each other. While the IKDC subjective score of the MOON cohort was less than that of either group in the current study, the MOON cohort included a greater age range and multiple graft types, including allografts, which may explain the difference. The mean difference in IKDC scores between the BEAR and ACLR groups of the current study was also less than the reported minimal clinically important difference of 11.5. 15
For the current study, the mean 6-year KOOS Sports and Recreation and KOOS Knee-Related Quality of Life for the BEAR group were 83 and 78, respectively. At the 5-year follow-up, the 5 KOOS domains of the early ACLR group of the Knee Anterior Cruciate Ligament Nonsurgical versus Surgical Treatment trial ranged from 71 to 91, 10 and those of the Delaware-Oslo cohort ranged from 80 to 94. 31 At the 7-year follow-up, the 5 KOOS domains of the Tension trial ranged from a mean of 76 to 91. 5 It should be noted that the KOOS Knee-Related Quality of Life resulted in the lowest score of the 5 domains across all of these previous studies, as was the case for the BEAR I cohort of the present study. However, the KOOS symptoms contained the lowest mean score (Table 2) for the ACLR group. Similarly, the median KOOS Sport and Recreation and KOOS Knee-Related Quality of Life for the MOON cohort at 6 years were 90 and 81, respectively. 17 In the present study, the reported values for the BEAR group ranged from 37 to 100, while those of the ACLR group ranged from 69 to 100 (Supplemental Figures). The minimal clinically important difference for the KOOS has been reported to be 8. 36
The clinical examination findings were also similar to those reported in other ACLR outcome studies. In a study with a 7-year follow-up, the distribution of IKDC examination scores for autograft ACLR was reported at 24% for grade A, 61% for grade B, 13% for grade C, and 0% for grade D. 5 The distribution of IKDC scores for the ACLR group of the present study was 20% for grade A, 80% for grade B, and 0% for grades C and D. Although the sample size of the BEAR I Trial was small, the distribution of IKDC scores for the BEAR group is also worth noting (80% for grade A, 20% for grade B, and 0% grades for C and D).
As for knee laxity assessment via arthrometer, the graft has been shown to stretch out relative to the uninjured contralateral limb after ACLR in most other studies.2,5,6,20,33,40 For example, Adravanti et al 2 reported an anterior laxity difference between limbs of 1.6 mm at 6 years after single-bundle ACLR, and Akelman et al 5 reported a mean difference of 1.7 mm at a 7-year follow-up. The mean anterior laxity values for both groups in the BEAR I cohort study at similar follow-up time points were 1.5 and 1.6 mm, respectively.
Quadriceps and hamstring muscle weakness after ACLR surgery has been well documented.3,11,12,19,21,41 In an adolescent population, it was reported that patients receiving hamstring tendon grafts have a 32% deficit in hamstring muscle strength at the 6- to 9-month follow-up. 41 Morphological and strength deficits of the hamstring muscles after hamstring tendon reconstruction in adults are present at 2-year follow-up. 19 In the current study, patients receiving BEAR did not exhibit significant muscle strength deficits at 6 years, while those in the ACLR group, all of whom received a hamstring tendon graft, had a significant reduction in isometric hamstring strength. In contrast, there was no difference in the mean isokinetic flexor torque in either group. The strength deficiency detected during isometric testing may be due to testing the hamstring muscles in isolation at 90° of flexion as opposed to isokinetic testing, which evaluates the flexor muscles of the lower limb in concert over the full range of motion. Nonetheless, isometric strength deficits are important as they have been shown to be associated with altered knee mechanics during walking and running gait. 1
Likewise, the hop testing data did not detect any differences between the 2 groups, and the mean values for the ACLR group were similar to those reported in the literature for ACLR.5,9,31,35 At the 7-year follow-up, patients who underwent autograft ACLR had a single-leg hop index of 92%, 5 while the BEAR and ACLR groups of the present study had indices of 93% and 94%, respectively. The values for all 4 hop tests were also similar to those reported for the nested cohort of the MOON group at the 2-year follow-up 35 and slightly lower than those of the Delaware-Oslo early ACLR cohort at 5 years. 31
The data presented in this paper provide the first insight into how patients undergoing the BEAR procedure may fare long-term. These data suggest that the BEAR procedure is at least as good as ACLR. Studies are underway to identify which patients will do better with BEAR. 38 Animal studies suggest that the posttraumatic osteoarthritis after BEAR is less than that seen after ACLR.18,26 It will be interesting to see if these findings translate to humans. Larger long-term clinical follow-up studies are needed to demonstrate the potential of BEAR to provide chondroprotection.
Limitations
There are several study limitations that should be considered. Patients were not randomized, which may have introduced a selection bias. However, we believed that it was important to recruit patients into the interventional group who wanted to undergo the new procedure since the implant had not been previously used in humans. It should be noted that the times between injury and surgery were different between groups since the patients were not randomized. However, these were unlikely to have a major impact on the results as they would still be considered acute injuries (<2 months).
Additionally, the sample size was limited to 10 patients in each group as the study was designed primarily to assess safety. It was important to limit the number of patients for the first-in-human study in case there were any severe adverse event (ie, infection and/or rejection), as has been shown in previous scaffolds for rotator cuff repair.13,22,39
Patient attrition was another limitation in that 3 patients (30%) in the ACLR group and 1 patient (10%) in the BEAR group were lost to follow-up. Thus, we do not know how these lost patients were doing 6 years after their surgery. Of those patients who were contacted, only 6 of the BEAR group and 5 of the ACLR group were able to come in for the on-site evaluations. Nonetheless, we were able to get subsequent injury/surgery data from all patients contacted.
Other procedural limitations could have been at play as the BEAR procedure requires a mini-arthrotomy to introduce the implant into the knee, while the ACLR procedure was done arthroscopically. Likewise, ACLR requires a graft harvest, which compromises the graft source, at least initially, while BEAR does not. Thus, these procedural biases may have influenced the results, although these factors are part of the respective procedures. Given that the patients in the ACLR group underwent reconstruction with hamstring tendon autografts, the initial isometric hamstring strength deficit was not surprising. However, it was interesting to note that the deficit was still present in the patients in the ACLR group at the 6-year follow-up.
The optimal rehabilitation procedure after the BEAR procedure is unknown. For this first-in-human study, it was assumed that the postoperative rehabilitation protocol typically prescribed after ACLR would be the best starting point for BEAR. Given that BEAR requires healing to bridge the injury site, 25 further optimizing the postoperative BEAR rehabilitation protocol in an effort to improve outcomes is a topic under investigation.
Finally, at the time the BEAR I trial was designed, the risk factors for subsequent failure after BEAR were assumed to be the same as those for ACLR. Patient selection may be a factor that could improve outcomes for both procedures. 38 Nonetheless, the 6-year data provide valuable insight into how the first patients who received BEAR are doing long-term. Long-term follow-up data from larger clinical trials are still needed to fully assess the efficacy, applicability, and cost-effectiveness of the BEAR procedure, 2 of which are currently underway (NCT02664545 and NCT03776162).
Conclusion
This preliminary study suggests that the outcomes of BEAR and ACLR with a hamstring tendon graft may be similar at the 6-year follow-up and warrants further investigation of the BEAR procedure in a larger cohort of patients.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671241260632 – Supplemental material for Bridge-Enhanced Anterior Cruciate Ligament Restoration: 6-Year Results From the First-in-Human Cohort Study
Supplemental material, sj-pdf-1-ojs-10.1177_23259671241260632 for Bridge-Enhanced Anterior Cruciate Ligament Restoration: 6-Year Results From the First-in-Human Cohort Study by Braden C. Fleming, Ben Baranker, Gary J. Badger, Ata M. Kiapour, Kirsten Ecklund, Lyle J. Micheli and Martha M. Murray in Orthopaedic Journal of Sports Medicine
Footnotes
Acknowledgements
The content is solely the responsibility of the authors and does not necessarily represent the official views of Harvard Medical School, Harvard University or its affiliated academic health care centers, the National Football League Players Association, Boston Children's Hospital, Brown University, or Rhode Island Hospital.
Final revision submitted October 16, 2023; accepted February 2, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding was received from the Translational Research Program at Boston Children's Hospital, the Children's Hospital Orthopaedic Surgery Foundation, the Children's Hospital Sports Medicine Foundation, the National Institutes of Health (R01-AR065462), the Lucy Lippitt Endowment of Brown University, and the Football Players Health Study at Harvard University (which is funded by a grant from the National Football League Players Association). B.C.F. is a founder of Miach Orthopaedics, the spouse of M.M.M., and an associate editor for the American Journal of Sports Medicine. A.M.K. has received consulting fees from Miach Orthopaedics. M.M.M. has received consulting fees from Miach Orthopaedics and is a founder and equity holder in Miach Orthopaedics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Boston Children's Hospital (IRB-P00012985).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.