
Abstract
Background:
The preservation of the anterior cruciate ligament (ACL) remnant during reconstruction or repair could offer advantages such as enhanced vascularity, proprioception, and biomechanical properties. However, research on the clinical factors influencing ACL remnant preservation at the time of surgery is limited.
Purpose/Hypothesis:
The purpose was to identify clinical factors influencing the amount of ACL remnant during surgery. It was hypothesized that not solely the delay from injury to surgery influences the amount of ACL remnant present at the time of surgery, but also other patient characteristics such as sex and age, as well as intraoperative findings.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A retrospective analysis of prospectively collected data was performed on patients who underwent arthroscopic ACL reconstruction between January 2013 and December 2022. ACL remnants were categorized based on their location into tibial attachment, midsubstance, and femoral attachment, accounting for 20%, 60%, and 20% of the total ACL length, respectively. A multivariate logistic regression was performed to identify factors predictive of the amount of ACL remnant.
Results:
In a cohort of 5725 patients, different variables were associated with an ACL remnant <20% at the time of surgery. Patients aged ≤20 years had an odds ratio of 1.748 (95% CI, 1.473-2.075; P < .0001), and those aged between 20 and 30 years had an odds ratio of 1.440 compared with those aged >30 years. Female patients had an odds ratio of 1.253 (95% CI, 1.087-1.446; P = .0019). A surgical delay >12 months was associated with an odds ratio of 3.134 (95% CI, 2.640-3.720; P < 0001). The presence of meniscal and chondral lesions had odds ratios of 1.784 (95% CI, 1.570-2.028; P < .0001) and 1.761 (95% CI, 1.426-2.171; P < .0001), respectively.
Conclusion:
Increased age at surgery was positively associated with a remnant size ≥20% of the ACL. Female sex, longer delay between accident and surgery, and associated injuries of intra-articular structures were risk factors for a remnant size <20%.
Anterior cruciate ligament (ACL) reconstruction traditionally involved the complete removal of the injured ligament. However, histological examinations have confirmed the presence of competent and viable mechanoreceptors, fibroblasts, myofibroblasts, proprioceptive nerve fibers, and a well-vascularized synovial sheet within the ACL remnants.16,25,26,30,32 While there is some controversy about the clinical benefits of ACL remnant preservation, available evidence suggests it may contribute to improved knee stability, proprioception, enhanced graft vascularization and healing, and potentially lower rates of graft rupture.1,9,10,12,22,23,29 Factors such as the timing of surgery from injury and patient’s age have been suggested to influence the extent of ACL remnant.19,23,24,30,31
With a renewed focus on primary repair of the ACL, it becomes important to understand factors that may improve preservation of the ACL remnant after rupture. Proximal ACL injuries and a sufficient ACL remnant length are deemed ideal and eligible for ACL primary repair. 14 Early surgical intervention is recommended to maximize the intrinsic healing potential of the ligament but also to avoid retraction of the residual ligament.6,11,30 Hence, it has been suggested that the combination of these factors is more prevalent in older patients who may be the most likely target group for acutely performed ACL primary repair. 30
With the size and quality of the ACL remnant being critical for ACL repair, an understanding of the factors that influence the size of the remnant is important for both modern ACL reconstruction and ACL repair.
Therefore, the aim of this study was to evaluate the clinical factors associated with the amount of ACL remnant present at the time of surgery. We hypothesized that the interval between injury and reconstruction was not the only factor influencing the amount of remnant at the time of surgery but various patient factors such as sex and age, as well as intraoperative findings, also played a significant role.
Methods
Patient Selection
A retrospective analysis of prospectively collected data from the SANTI database was performed. All patients who underwent ACL reconstruction performed by a single senior surgeon (B.S.-C.) between January 2013 and December 2022 were considered for study eligibility. Institutional review board approval (COS-RGDS-2023-02-004-SONNERY-COTTET-B) was granted for this study, and all patients provided informed consent to participate. All patients had a confirmed ACL rupture based on clinical examination and magnetic resonance imaging (MRI). Surgical indication was given because of the patients’ inability to return to their previous level of activity due to instability symptoms and pain. Patients were excluded if they underwent either ACL reconstruction revision or major concomitant surgery such as multiligamentous reconstruction (except for anterolateral ligament reconstruction). Data recorded in the database included patient and clinical variables relevant to ACL surgery, such as patient age at the time of surgery, sex, body mass index, sport activity, reason for injury, date of injury, date of surgery, percentage of ACL remnant, associated intra-articular injuries such as meniscal and chondral lesions, and anteroposterior laxity difference from side to side (in mm) as measured using a Rolimeter (Aircast Europe). In addition, the database included surgical details such as the type of graft used, surgical techniques used, and any complication.
Arthroscopic Evaluation of ACL Remnant
Remnant measurement was performed according to the method reported by Muneta et al 19 that, to the best of the authors’ knowledge, represents the approach described in the contemporary literature. The ACL was segmented into 3 zones for analysis: the tibial attachment, representing the distal 20% of the ACL; the midsubstance, representing the central 60%; and the femoral attachment, representing the proximal 20% 19 (Figure 1).

Example of anterior cruciate ligament (ACL) remnant and determination of its volume. A total volume of the ACL was divided into 3 parts: tibial attachment, medial substance, and femoral attachment. The total remnant was estimated to be 80%: tibial attachment, 20%; midsubstance, 60%; and femoral attachment, 0%. (Figure reprinted with permission from Muneta T, Koga H, Ju YJ, Horie M, Nakamura T, Sekiya I. Remnant volume of anterior cruciate ligament correlates preoperative patients’ status and postoperative outcome. Knee Surg Sports Traumatol Arthrosc. 2013;21(4):906-913. doi:10.1007/s00167-012-2023-5)
Statistical Analysis
All calculations were performed using SAS for Windows (Version 9.4; SAS Institute Inc), with the level of statistical significance set at P < .05 for the data sets from the SANTI database. Descriptive data analysis was performed according to the type of criteria considered. Descriptive analysis was performed distinguishing between qualitative and quantitative data. Frequencies and percentages are reported for qualitative data, and means and standard deviations are reported for quantitative data. For comparisons of categorical variables, such as sex, age group, and presence or absence of chondral or meniscal lesions, the chi-square test or Fisher exact test was used. For continuous variables, such as time from ACL rupture to surgery, the Student t test or Mann-Whitney-Wilcoxon test was used, depending on the distribution of the variable. For multivariate analysis, a logistic regression model was used to analyze significant variables, including delay between ACL rupture and surgery, age at surgery, sex, meniscal and chondrallesions as adjustment factors.
Variables were integrated into the preliminary multivariate model if they were significantly associated with the dependent variable (ACL remnant <20%) at a significance level of P = .20 or if they were known prognostic factors related to ACL remnant size from the existing literature. Variables included sex, age category, time from injury to surgery, presence of meniscal lesions, and presence of chondral lesions. Analyses were conducted on all patients excluding those with missing values. The final model resulted from a manual backward stepwise selection process, with a significance threshold set at P = .05 for variable retention. The 20% threshold was selected based on findings that a minimum volume equal to 20% of the tibial attachment, as defined by the Muneta classification, is required to consistently identify a viable remnant ACL.
Results
Patient Characteristics
A total of 5725 patients met the criteria for inclusion in the analysis. Patients were classified based on the amount of ACL remnant available for preservation during ACL reconstruction surgery: 1475 patients (25.8%) had <20% remnant, 3068 patients (53.6%) had between 20% and 60% remnant, and 1182 patients (20.6%) had >60% remnant. Of these, patients with <20% remnant were categorized as the less preserved remnant group, and those with ≥20% remnant were categorized as the moderately and well-preserved group; 4250 patients were included in the latter category (Figure 2).

Flowchart in line with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines. ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction.
Age, sex, time from injury to reconstruction, and activity level were significantly different among the 3 groups of patients (Table 1).
Patient Characteristics a
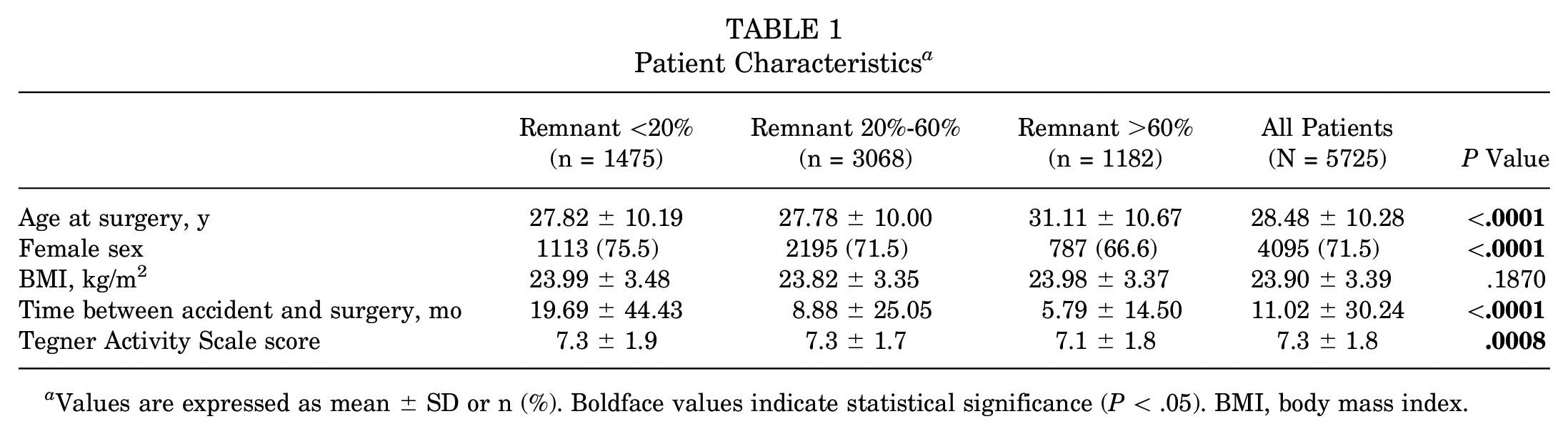
Values are expressed as mean ± SD or n (%). Boldface values indicate statistical significance (P < .05). BMI, body mass index.
Comparing patients evaluated with less preserved remnant (<20%) with patients with moderately and well-preserved remnant (≥20%), the 2 groups were found to be significantly different in age, sex, and mean time between injury and surgery (Table 2).
Patient Characteristics Stratified by Remnant Found a

Values are expressed as mean ± SD or n (%). Boldface values indicate statistical significance (P < .05). BMI, body mass index.
Clinical and Surgical Findings
A greater incidence of chondral lesions and a higher incidence of meniscal lesions were found in the group with <20% remnant. This group also had a higher incidence of meniscal injuries involving both menisci (20.1% and 11.1% for the <20% and ≥20% remnant groups, respectively; P < .0001) and bucket-handle tears (7.9% and 2.3% for the <20% and ≥20% remnant groups, respectively; P < .0001). Patients with a remnant ≥20% had a significantly lower anteroposterior laxity with respect to patients with <20% remnant. Details of the surgical findings are represented in Table 3.
Clinical and Surgical Findings Stratified by Remnant Found a
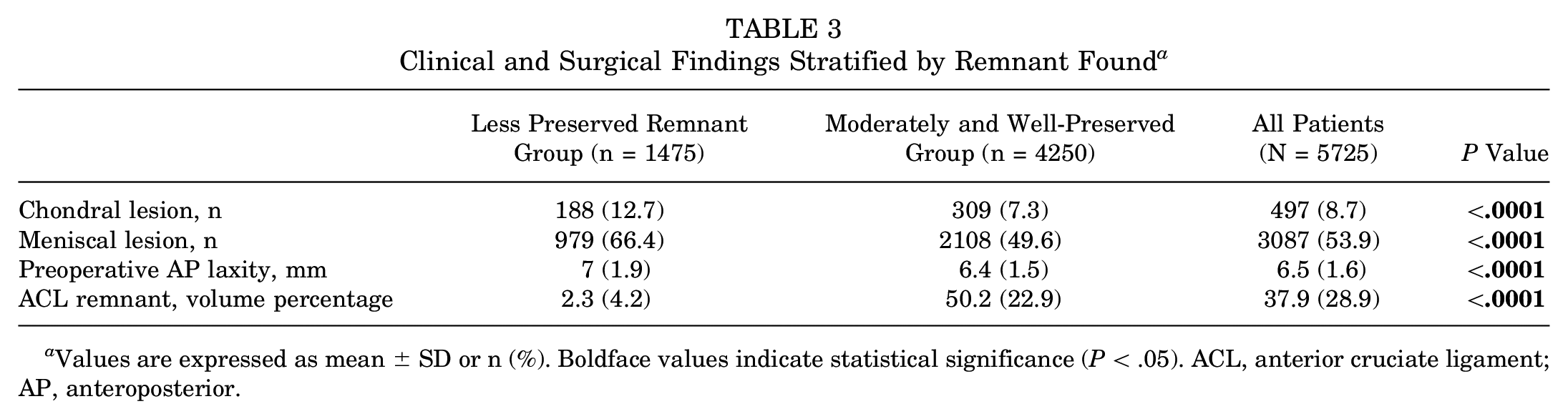
Values are expressed as mean ± SD or n (%). Boldface values indicate statistical significance (P < .05). ACL, anterior cruciate ligament; AP, anteroposterior.
Risk Factors Associated With a Less Preserved Remnant
Risk factors associated with remnant <20% were analyzed using multivariate analysis including sex, age class, time from accident to surgery, meniscal lesions, and chondral lesions. The analysis showed that several factors were significantly associated with a lower percentage of remnant. Age ≤30 years, female sex, delay of ≥3 months from injury to surgery, and the presence of meniscal and chondral lesions were identified as independent variables associated with an ACL remnant <20% at the time of surgery (Figure 3).

Multivariate analysis of potential factors associated with remnant <20%. Numbers and percentages are based on all patients in the population analyzed, excluding those with missing values (7 and 10, respectively, per the less preserved remnant group and moderately and well-preserved group). ACL, anterior cruciate ligament; OR, odds ratio.
Discussion
The main findings of the current study were that the retraction of ACL stumps appears to be a normal biological response after ACL rupture, and different features may influence the biological response to ACL rupture. Murray et al 20 described 4 phases of the healing response of the retracted remnant in a complete ACL tear: the first few weeks after rupture are the inflammatory phase; from week 3 to week 8 is the epiligamentous regeneration phase; the proliferative phase occurs after week 8, with revascularization of the remnant; and the final phase is the remodeling and maturation phase, with retraction of the ligament remnant. Histologically, the authors found that the epiligamentous tissue was covered with synovium rich in contractile actin isoform cells, which may partially explain the retraction of these remnants. The results of this study confirm the importance of time as a key determinant of volume of ACL remnant after injury.
Recently, the central role of inflammation in the biological process of ACL injury has been emphasized.3,8,15,27 Immediately after ACL injury, resident immune cells are activated and release proinflammatory molecules, such as cytokines, chemokines, and lipid mediators.2,13 Although inflammation is critical for repair, excessive or prolonged inflammation can contribute to tissue degradation and impaired healing. 17 The biological response after ACL injury, which has a significant impact on remnant retraction, varies with the occurrence of associated injuries. In fact, meniscal and chondral lesions alter the biochemical milieu of the joint, leading to greater levels of proinflammatory and catabolic markers.4,5,27,28 The current study showed that patients with cartilage or meniscal injuries were indeed more likely to have a small remnant. Because cytological analysis was not performed in this study, whether an increase in proinflammatory and catabolic factors has a negative effect on the persistence of a viable ACL stump cannot be directly determined. Nevertheless, the presence of a more severe injury was shown to result in a smaller ACL remnant, suggesting a possible relationship between proinflammatory cytokines and ACL remnant volume. Our results indicate that younger individuals and female sex are associated with a reduced volume of ACL remnant, suggesting a more rapid and complete contraction of the remnant after injury in these patients. The cause of this observation is unclear but may be related to increased inflammatory factors that have previously been reported in patients with meniscal tears and female sex. 4
Studies focusing on ACL repair have highlighted the importance of patient characteristics and timely intervention in preserving a large ACL remnant. van der List et al 30 conducted a case-control study focused on identifying predictive factors for the feasibility of arthroscopic primary repair of proximal ACL tears. Suitable candidates for undergoing ACL repair were identified as patients in whom the distal portion of the ACL was of sufficient length for reattachment to the femoral footprint and whose tissue quality could adequately support suture passage and retention.
Notably, individuals >35 years of age and those undergoing surgery within 28 days of injury were found to be more likely candidates for primary repair. In addition, the likelihood of successful primary repair was significantly reduced in the presence of a lateral meniscal injury. 30 In another study, van der List et al 31 examined the prevalence of ACL tear types using MRI. The authors found that patients >35 years of age were more likely to have a distal remnant >90% of the total length of the ligament compared with those <35 years of age, with incidences of 23% and 8%, respectively (P < .001). Consistent with the observations of van der List et al, 31 the results of the current study also observed an increased presence of extended distal remnants within the older patient cohort.
Within the study population, individuals with <20% ACL remnant had increased preoperative anteroposterior laxity. The discrepancy in the incidence of meniscal injuries between the 2 cohorts may have played a role, despite the recognized influence of the ACL remnant in reducing passive anterior knee laxity. Specifically, certain scar types in which the scarred stump effectively crosses the joint have been identified as significantly reducing knee laxity, as the ligament heals to the roof or lateral wall of the femoral notch.7,18,21
Limitations
The current study has several limitations. First, the study was conducted at a single institution and by a single senior surgeon, which may introduce bias and limit the generalizability of the results. Second, the remnant assessment technique in this study relies only on subjective observation. Third, the statistical models were adjusted for specific variables such as age, sex, and associated lesions, but other unmeasured confounders may still influence the outcome. However, based on previous literature, all the known variables have been included in the statistical model.
Conclusion
Different clinical factors are associated with the amount of ACL remnant present at the time of surgery. Increased age at surgery was the only factor positively associated with a remnant size ≥20% of the ACL. Female sex, longer delay between accident and surgery, and associated injuries of intra-articular structures were risk factors for a remnant size <20%.
Footnotes
Final revision submitted May 24, 2024; accepted June 5, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.S.-C. has received financial support from Arthrex. C.L. has received consulting fees from Anika Therapeutics, Vericel, and Flexion Therapeutics; nonconsulting fees from Vericel, Aesculap Biologics, and Arthrosurface; and honoraria from JRF Ortho. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Ramsay Sante (IR00010835).