
Abstract
Background:
Patients with isolated anterior cruciate ligament (ACL) reconstruction have demonstrated an increased risk of ACL graft failure and lower patient-reported outcome (PRO) scores when increased posterior tibial slope (PTS) is present. However, there is a paucity of literature evaluating the effect of PTS on outcomes after combined bicruciate multiligamentous knee reconstruction.
Purpose:
To determine whether differences exist for graft failure rates or PRO scores based on PTS after combined bicruciate multiligamentous knee reconstruction.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
All patients who underwent combined ACL and posterior cruciate ligament (PCL) reconstruction between 2000 and 2020 at our institution were identified. Exclusion criteria were age <18 years, knee dislocation grade 5 injuries, concomitant osteotomy procedures, and <2 years of clinical follow-up. Demographic and outcomes data were collected from our prospectively gathered multiligamentous knee injury database. Lysholm and International Knee Documentation Committee (IKDC) scores were analyzed in relation to PTS. Outcomes were compared for patients with a PTS above and below the mean for the total cohort, PTS >12° versus <12°, positive versus negative Lachman test at follow-up, and positive versus negative posterior drawer test at follow-up.
Results:
A total of 98 knees in 98 patients were included in the study, with a mean clinical follow-up of 5.1 years (median, 4.6 years; range, 2-16 years). The mean PTS was 8.7° (range, 0.4°-16.9°). Linear regression analysis showed no significant correlation between PTS and IKDC or Lysholm scores. Patients with a PTS above the mean of 8.7° trended toward lower IKDC (P = .08) and Lysholm (P = .06) scores. Four patients experienced ACL graft failure and 5 patients experienced PCL graft failure. There were no differences in graft failure rates or PRO scores for patients with a PTS >12°. Patients with a positive Lachman test trended toward higher PTS (9.6° vs 8.5°, P = .15).
Conclusion:
In this series of bicruciate multiligamentous knee reconstructions at midterm follow-up, no differences in graft failures, complications, reoperations, revisions, or PRO scores based on PTS were identified. Patients with a positive Lachman test were found to have a slightly higher PTS, although this did not reach statistical significance.
Multiligamentous knee injuries (MLKIs) typically occur due to significant trauma. They involve injuries to ≥2 knee ligaments including the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), lateral collateral ligament (LCL)/posterolateral corner (PLC), or medial collateral ligament (MCL)/posteromedial corner (PMC). Bicruciate MLKIs involve both the ACL and PCL and commonly at least 1 collateral ligamentous complex. Damage to the popliteal vessels and peroneal nerve may be present at the time of injury, especially if a knee dislocation occurred.21,25,35 Although MLKIs are relatively uncommon, they represent a significant challenge in the field of orthopaedic surgery. 42 Quality of life and functional outcomes after multiligamentous reconstruction surgery are limited in some cases by stiffness, pain, graft failure, and persistent instability. 18 The International Knee Documentation Committee (IKDC) and Lysholm scores are important metrics for assessing patient-reported outcomes (PROs) and provide a framework for long-term follow-up and evaluation of patients with MLKI. 32
Even though surgical techniques, biological risk factors (ie, tobacco use, diabetes, and generalized ligamentous laxity), and treatment protocols affect postoperative outcomes in MLKI, anatomic variables may play a role as well.13,24,30,38,44 Posterior tibial slope (PTS) has become a topic of interest in ligament reconstruction. 4 Cadaveric studies have shown that an increased PTS leads to a relative anterior translation of the tibia on the femur.15,16 This anterior shift of the tibia brings the PCL insertion on the tibia closer to its origin on the femur and decreases graft forces after PCL reconstruction.2,5 The inverse effect is present for PTS and ACL graft forces. Several studies have demonstrated increased stress on the ACL in patients with an increased PTS, predisposing patients to ACL rupture and graft failure.6 -8,29,31,34,45 In addition, altering the PTS via osteotomy has been shown to reduce the risk of graft failure after ligament reconstruction in certain patients.17,19,36 However, the competing interests regarding PTS for ACL versus PCL reconstruction may cause uncertainty in the appropriate management of the PTS at the time of bicruciate ligament reconstruction. Currently, there is a paucity of data analyzing PROs and knee laxity in relation to PTS after multiligamentous knee reconstruction for knee dislocation grades 2 to 4. The purpose of the present study was to analyze the effect of PTS on knee laxity, graft failure, and PRO scores after combined bicruciate multiligamentous knee reconstruction. We hypothesized that no difference would exist for graft failure rates or PRO scores based on PTS after combined bicruciate multiligamentous knee reconstruction.
Methods
After institutional review board approval, all patients who underwent combined ACL and PCL reconstruction with or without other ligamentous reconstructions (LCL/PLC and/or MCL/PMC) between 2000 and 2020 at our institution were identified. Exclusion criteria included age <18 years, knee dislocation grade 5 injuries, concomitant osteotomy procedures, and <2 years of clinical follow-up.
Of the 329 multiligamentous knee reconstructions performed during the study period, 125 knees had bicruciate reconstruction. Three patients were excluded due to proximal tibial osteotomies as part of their surgical management (all 3 were valgus-producing high tibial osteotomies at the time of revision ligament reconstruction), 9 were excluded due to age <18 years, and 15 had <2 years of follow-up. Therefore, 98 knees in 98 patients were included in the study. Each surgery was performed by 1 of the 2 senior authors (M.J.S. or B.A.L.)
Multiple techniques for ACL reconstruction were used over the 20-year study period. Surgical decisions were based on presence of previous bone tunnels, evolving surgical techniques, previous surgeries such as fasciotomies or external fixation, and injury-specific factors such as the presence or absence of meniscus root tears requiring additional bone tunnels. ACL fixation included suspensory, interference, and hybrid techniques. PCL fixation included suspensory, interference, and hybrid techniques.1,14,26,27,33,39 ACL and PCL reconstructions were all single bundle. Reconstruction rather than repair was performed for the MCL/PMC.20,24 For the LCL/PLC, reconstruction or repair with augmentation were performed using a previously described technique. 23 During cruciate reconstruction, the tibial station was set, and provisional tensioning of the ACL and PCL grafts was performed with the knee in extension. Next, final tensioning and fixation of the PCL graft was performed with the knee in flexion with a slight anterior drawer. The tibial step off was checked manually and with intraoperative fluoroscopy to ensure appropriate tibial station. Next, final tensioning and fixation of the ACL graft were accomplished in a similar way with the knee in extension. After fixation of both grafts, the tibial station as well as anterior and posterior drawers were checked to confirm adequate anatomic restoration. The senior surgeons used similar treatment protocols and surgical techniques. Postoperative rehabilitation was based on standardized institutional protocols and varied depending on the injury pattern and surgeries performed.
Demographic, surgical, and outcomes data were collected retrospectively from our prospectively gathered MLKI database. Patient demographic data documented in the registry at the time of care included sex, age at the time of surgery, laterality, body mass index (BMI), presence or absence of generalized ligamentous laxity (Beighton score of ≥4), tobacco use, and diabetes. The time from injury to surgery was recorded as well as the presence or absence of a knee dislocation requiring a formal reduction, vascular injury, or neurologic injury at the time of initial presentation. Surgical data documented in the registry at the time of surgery included primary or revision ligament reconstruction, concomitant procedures on the menisci or cartilage, and concomitant LCL/PLC or MCL/PMC procedures. PRO data included Lysholm and IKDC scores, which were filled out by patients at regular intervals (ie, 1 year, 2 years, 5 years, and 10 years after surgery). Routine postoperative follow-up included in-person visits at a minimum of 2 weeks, 3 months, 6 months, 1 year, and 2 years. Many patients were seen in clinic further out than 2 years. Physical examination data for this study were obtained from the most recent in-person follow-up visit and were documented by the surgeon. All patients received PRO questionnaires either at their in-person follow-up visits or via mail at regular intervals as described above. These scores were recorded in the registry prospectively.
Outcomes including complications, reoperations, graft failures, revisions, and physical examination data were collected prospectively and confirmed retrospectively at the time of data review for this study. For Lachman and posterior drawer testing, grade 0 was defined as 0 to 1 mm of translation, grade 1 as 2 to 5 mm, grade 2 as 6 to 10 mm, and grade 3 as >10 mm. Graft failure was defined as graft revision, grade 3 anterior or posterior drawer test, or grade 2 anterior or posterior drawer test with symptomatic instability. Additional details not otherwise contained in the registry were obtained via individual review of the electronic medical record. PTS measurements were obtained at the time of data review by an orthopaedic sports medicine fellow and a senior orthopaedic surgery resident (M.T.L and R.T.C.). using the proximal anatomic axis method on perioperative lateral knee radiographs as previously described. 9 Primary outcome measures were PTS in relation to Lysholm and IKDC scores and the presence or absence of a positive Lachman test or posterior drawer test. For IKDC, the patient acceptable symptom state (PASS) was defined as 75.9 based on a previous cohort of patients after primary ACL reconstruction. 28
Linear regression models were created to analyze PTS in relation to Lysholm and IKDC scores. Outcomes were compared for patients with a PTS above and below the mean for the total cohort. Subgroup analyses were performed for patients with an abnormally high PTS (>12°) as well as a low PTS (<5°). These represented PTS values approximately 1 SD above and below the mean. In addition, outcomes were compared for those with a positive or negative Lachman test and those with a positive or negative posterior drawer test. Grade 1 or higher was considered positive for anterior and posterior drawer tests. Continuous variables were compared using Student t test, while categorical variables were compared using chi-square test or Fisher exact test with statistical significance set as P = .05. All analysis was conducted using SAS Version 9.4M6 (SAS Institute Inc).
Results
Demographic and surgical data are shown in Table 1. The mean age at the time of surgery was 33.2 years (range, 18-57 years). The mean time from initial injury to primary multiligamentous reconstruction was 8 months (median, 3 months; interquartile range [IQR], 4.6 months; range, 0-119 months). Ten of the included surgeries were performed as revisions, and the mean time from primary to revision reconstruction was 83 months (median, 47 months; IQR, 141 months; range, 2-208 months). The longest mean clinical follow-up for either an in-person examination or PRO scores was 5.1 years (median, 4.6 years; IQR, 3.1 years; range, 2-16 years). The mean clinical examination follow-up was 2.9 years (median, 2 years; IQR, 3.2 years). The mean PRO follow-up was 4.5 years (median, 3.6 years; IQR, 3 years). The mean PTS for the total cohort was 8.7° (range, 0.4°-16.9°). There were 73 male patients (74.5%). The mean BMI for the cohort was 31 kg/m2. A total of 50 patients (51.0%) had a documented knee dislocation at the time of injury requiring reduction. Six patients (6.1%) underwent combined ACL and PCL reconstruction alone, 38% underwent concomitant MCL reconstruction, 39% had LCL/PLC repair or reconstruction, and 17% had surgical repair or reconstruction of all 4 knee ligaments. For those undergoing LCL/PLC procedures, 7 patients had repair with augmentation, whereas 31 patients had reconstruction. Concomitant meniscal repair was performed in 19 patients (19.4%), whereas partial meniscectomy was performed in 16 patients (16.3%); 2 patients (2.0%) received meniscal allograft reconstructions. A total of 19 patients underwent chondroplasty in a variety of locations in the knee joint, as shown in Table 1. Allograft was used for all PCL reconstructions and all but 2 ACL reconstructions. PCL allografts included 60 Achilles tendon, 21 peroneus longus, and 17 tibialis anterior. ACL allografts included 37 tibialis anterior, 31 patellar tendon, 24 semitendinosus, 3 tibialis posterior, and 1 peroneus longus. ACL autografts included 1 patellar tendon and 1 semitendinosus. Internal bracing was used for both the ACL and PCL grafts in 12 patients. The mean IKDC for patients who underwent concomitant meniscal procedures was 70.6 versus 73.0 for those without (P = .57). The mean IKDC for patients who underwent concomitant cartilage procedures was 71.5 versus 72.3 for those without (P = .88).
Patient Demographic and Surgical Data Based on PTS Slope Greater Than or Less Than the Total Cohort Mean of 8.7° a

Values are given as mean ± SD or n (%). BMI, body mass index; KD, knee dislocation; LFC, lateral femoral condyle; MFC, medial femoral condyle; PTS, posterior tibial slope.
Number of patients. Some patients had >1 chondroplasty, and the subcategories count them all separately.
Table 1 compares the demographic, injury and surgical characteristics in patients with a PTS less than or greater than the mean of 8.7°. The mean PTS for the cohort with an above-average slope was 11.2° compared with 5.9° for the cohort with a below average slope (P < .01). No significant differences were found between these 2 cohorts for age, sex, BMI, knee dislocation, high- versus low-energy injury, vascular or neurologic injury, knee dislocation grade, generalized ligamentous laxity, or concomitant procedures.
No statistically significant correlation was found for PROs including Lysholm or IKDC score in relation to the PTS (Figure 1). There was a weak inverse correlation between both IKDC and Lysholm and PTS (R2 = 0.0074 and 0.0124, respectively). At lower PTS, the IKDC scores were more clustered above the PASS, with more patients falling below the PASS at higher PTS measurements.
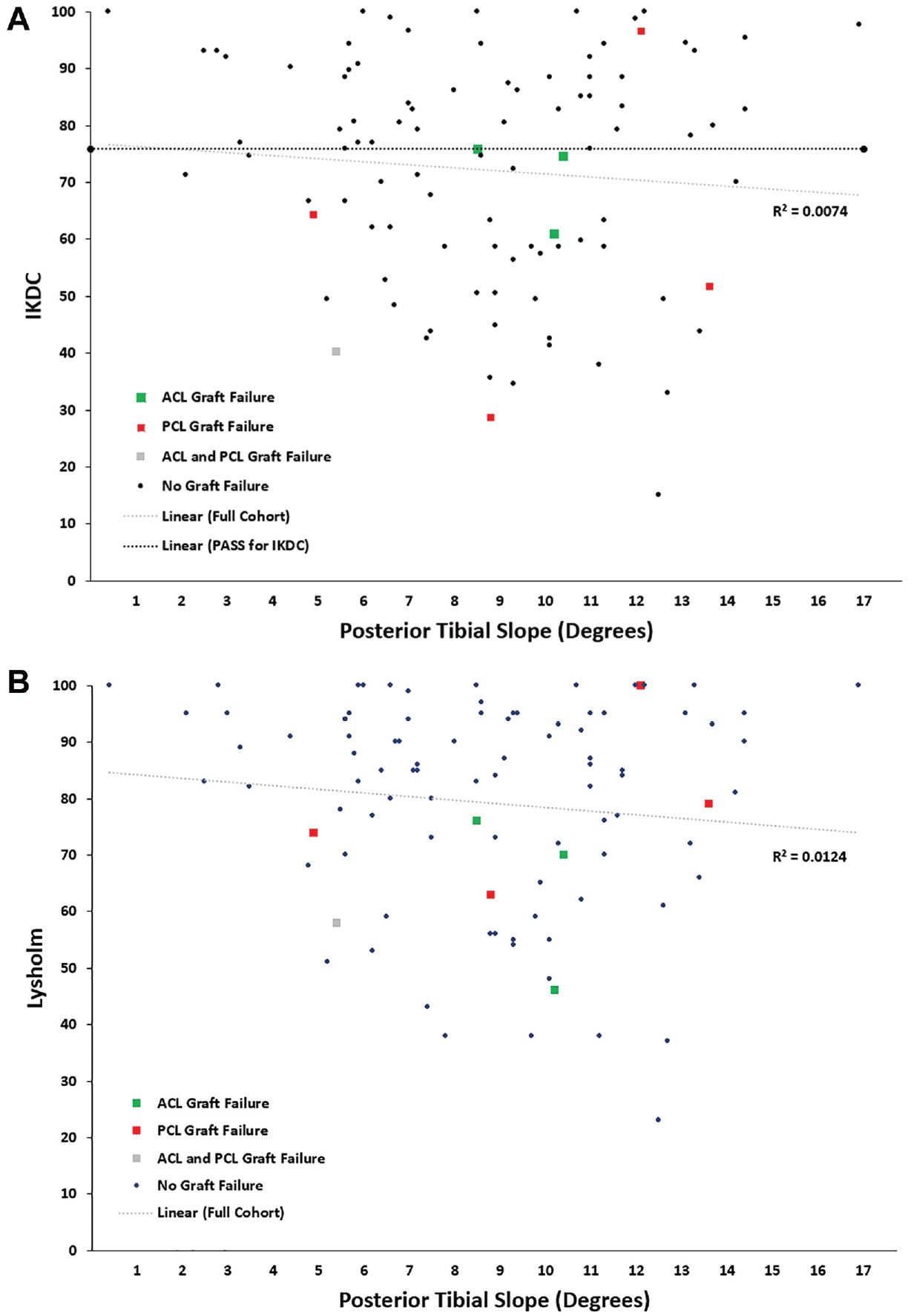
Linear regression model for (A) IKDC score and (B) Lysholm score based on posterior tibial slope. The horizontal black line in (A) represents the PASS for IKDC (there is no validated PASS for the Lysholm). ACL, anterior cruciate ligament; IKDC, International Knee Documentation Committee; PASS, patient acceptable symptom state; PCL, posterior cruciate ligament.
The lower PTS cohort trended toward higher IKDC (76.2 vs 68.8, P = .08) and Lysholm (83.3 vs 76.0, P = .06) scores compared with the cohort with higher PTS (Table 2), although this did not reach statistical significance. The 2 cohorts had similar range of motion at their last clinical follow-up visit. A positive Lachman test was seen in 15% of patients with a below-average PTS (grade 1, n = 5; grade 2, n = 1; and grade 3, n = 1) compared with 25% of patients with an above-average PTS (grade 1, n = 9; grade 2, n = 4; and grade 3, n = 0) (P = .32). A positive posterior drawer was seen in 34.8% of patients with a below-average PTS (grade 1, n = 12; grade 2, n = 2, and grade 3, n = 2) compared with 32.7% of patients was an above-average PTS (grade 1, n = 13; grade 2, n = 2; and grade 3, n = 2) (P = .83). There were no differences between the 2 cohorts for complications, reoperations, or revisions. A detailed list of complications is seen in Table 2. ACL graft failure occurred in 4 patients (4.1%) at a mean of 5.8 years postoperatively. Only 1 of these underwent revision ACL reconstruction (1.0%). Of the other 3, 1 patient elected for nonoperative management with a brace, 1 patient underwent total knee arthroplasty, and 1 patient was lost to follow-up in the setting of significant psychiatric comorbidities. No difference in PTS was demonstrated for patients with ACL graft failure compared with those without (8.6° vs 8.7°, P = .97). Five patients experienced PCL graft failure (5.1%) at a mean of 2.9 years postoperatively. One patient underwent revision PCL reconstruction (1.0%). The mean PTS in patients with ACL graft failure was 8.6° compared to 8.9° in patients with PCL graft failure (P = .88).
Comparison of Outcomes Based on PTS Greater Than or Less Than the Total Cohort Mean of 8.7° a

Values are given as mean ± SD or n (%). ACL, anterior cruciate ligament; IKDC, International Knee Documentation Committee; LCL, lateral collateral ligament; MCL, medial collateral ligament; PCL, posterior cruciate ligament; PTS, posterior tibial slope.
Number of patients. Some patients had >1 nonrevision reoperation.
A total of 22 patients had a PTS <5°. When comparing these patients with a low slope with the rest of the cohort, there were no statistically significant differences for IKDC, Lysholm, Lachman test, posterior drawer test, graft failures, or revisions (Table 3).
Comparison of Outcomes Based on PTS < or >5° a

Values are given as mean ± SD or n (%). ACL, anterior cruciate ligament; IKDC, International Knee Documentation Committee; PCL, posterior cruciate ligament; PTS, posterior tibial slope.
Similarly, 16 patients were considered to have abnormally high PTS (>12°). There were no statistically significant differences between patients with an abnormally high slope and those with a normal slope for IKDC, Lysholm, Lachman test, posterior drawer test, graft failures, or revisions (Table 4).
Comparison of Outcomes Based on PTS > or <12° a

Values are given as mean ± SD or n (%). ACL, anterior cruciate ligament; IKDC, International Knee Documentation Committee; PCL, posterior cruciate ligament; PTS, posterior tibial slope.
A subgroup analysis was performed for patients with a positive Lachman test (n = 20) versus those with a negative Lachman test (n = 78) at final clinical follow-up as shown in Table 5. A total of 14 patients had a grade 1 Lachman test, 5 patients had a grade 2, and 1 patient had a grade 3. Those with a positive Lachman test had lower IKDC and Lysholm scores (both, P = .04) compared with those with a negative Lachman test. There was no difference in PTS between the 2 cohorts (P = .15). Patients with a positive Lachman test had higher rates of vascular and neurologic injury at the time of presentation (both, P = .01). The cohort with a positive Lachman test also had higher rates of generalized ligamentous laxity as documented by the senior surgeon at the preoperative visit (P = .04).
Comparison of Patient Factors and Outcomes Based on Presence or Absence of a Lachman Sign at Last Clinical Follow-up a
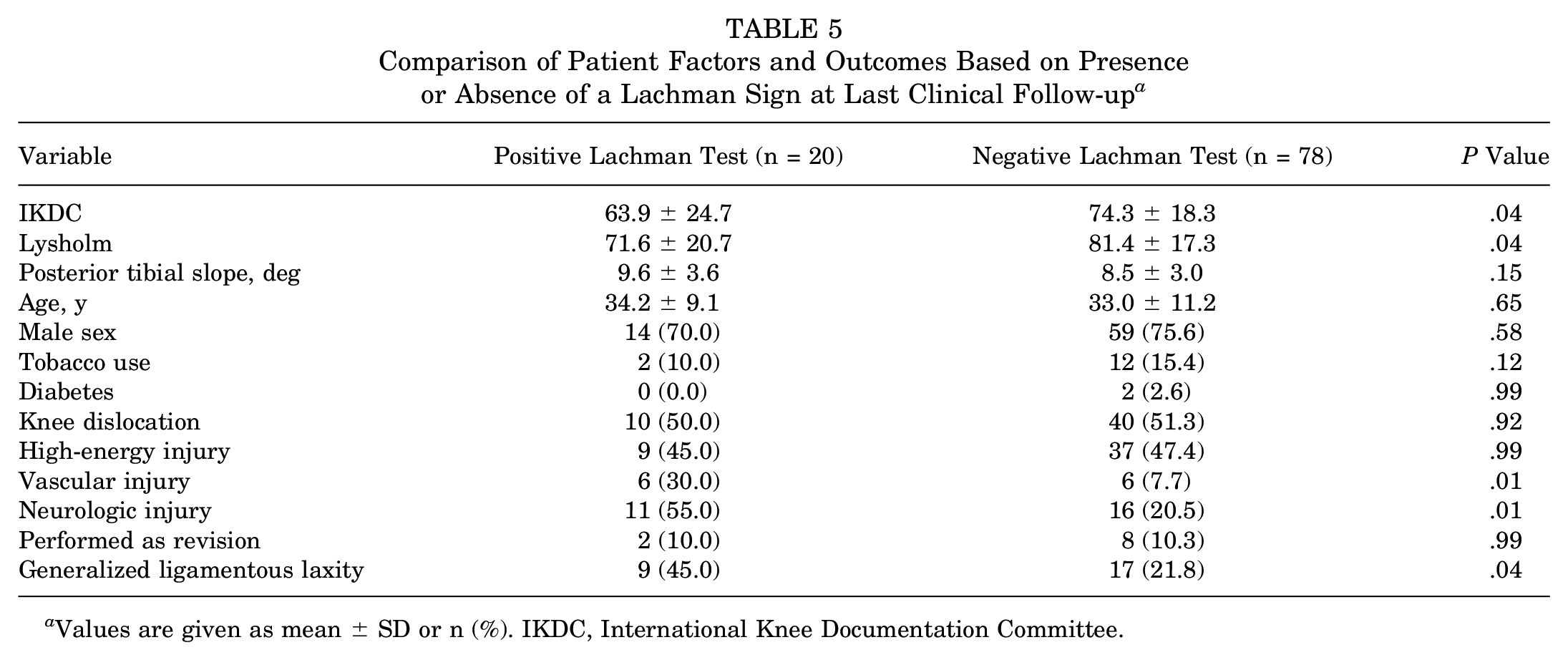
Values are given as mean ± SD or n (%). IKDC, International Knee Documentation Committee.
Similarly, a subgroup analysis was performed to compare patients with a positive posterior drawer test and those with a negative posterior drawer test (Table 6). A total of 25 patients had a grade 1 posterior drawer test, 4 patients had a grade 2, and 4 patients had a grade 3. No difference was found for IKDC, Lysholm, PTS, knee dislocation, or generalized ligamentous laxity.
Comparison of Patient Factors and Outcomes Based on Presence or Absence of a Posterior Drawer Test at Last Clinical Follow-up a
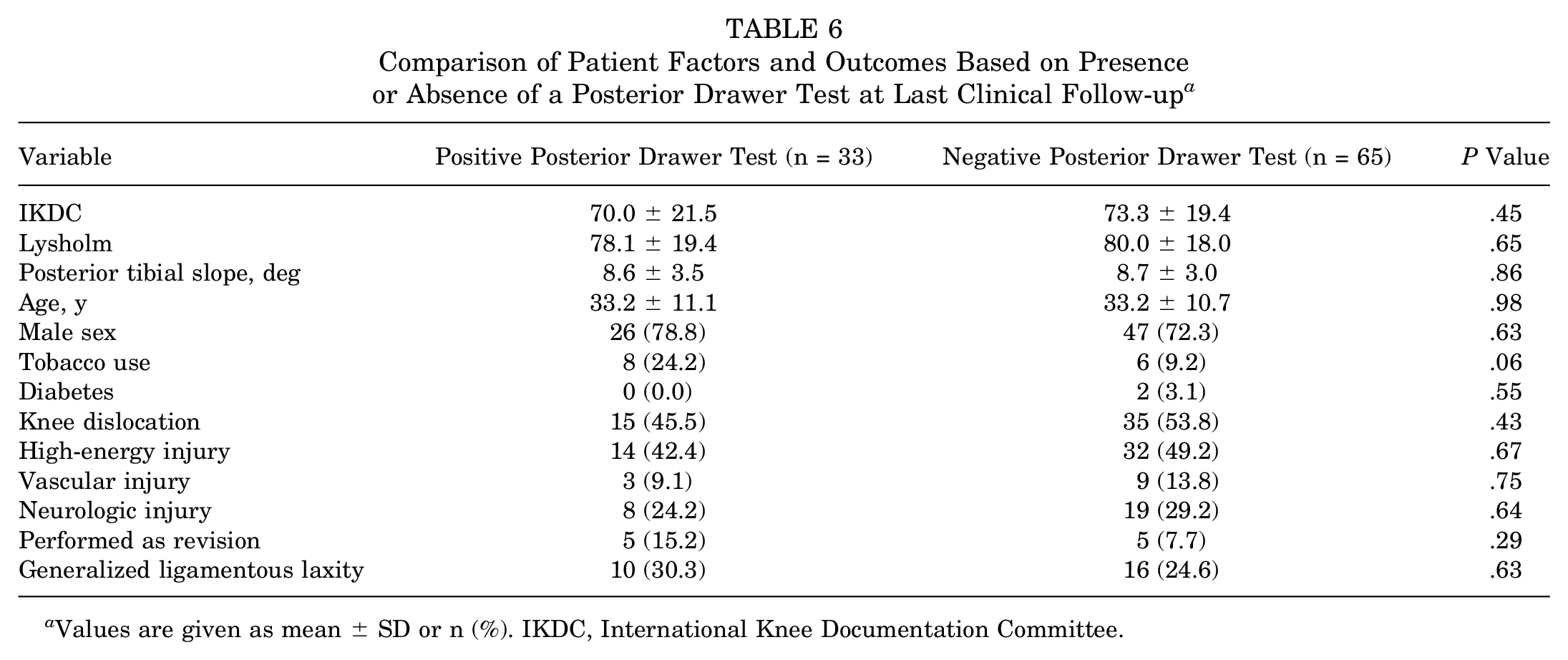
Values are given as mean ± SD or n (%). IKDC, International Knee Documentation Committee.
In the present cohort, patients with a knee dislocation had a slightly lower arc of motion compared with those without a knee dislocation, but this did not reach statistical significance (118° vs 125°; P = .10). Patients with a vascular injury had a mean IKDC score of 69.6, compared with 72.5 for those without a vascular injury (P = .66), and a mean Lysholm score of 75.2 versus 79.8 (P = .44). Similarly, patients with a peroneal nerve injury had a mean IKDC score of 69.3, compared with 73.2 for those without (P = .41), and a mean Lysholm score of 75.3 versus 80.7 (P = .19). One patient with a vascular injury went on to arthrodesis, whereas another had ACL graft failure with subsequent revision. Two patients with a peroneal nerve injury went on to ACL graft failure. In patients with a previous cruciate ligament reconstruction with failure requiring revision, the mean IKDC score was 66.7 versus 72.7 for patients undergoing primary cruciate ligament reconstruction (P = .39), and the mean Lysholm was 78.8 versus 79.3 (P = .94). Of the 10 revision multiligamentous reconstructions included in the study, the mean PTS was 9.5°. No patients underwent concomitant or previous slope-correcting osteotomies. The mean IKDC was 70.0 and Lysholm was 80.9. One PCL graft failure was seen in this cohort with subsequent PCL graft revision. No ACL graft failures were observed in this cohort. No statistically significant differences were observed for the revision cohort compared with the rest of the cohort for IKDC, Lysholm, Lachman test, posterior drawer test, graft failures, or revisions.
Discussion
At a mean follow-up of 5.1 years, the present study found no differences in graft failure, complications, reoperations, or revisions based on PTS. A recent study by Winkler et al 43 similarly did not demonstrate a statistically significant correlation between PROs and PTS for patients undergoing isolated and combined PCL reconstruction. In their cohort, patients with PCL graft failure were found to have a significantly lower PTS compared with patients without PCL graft failure. In our cohort, no difference in PTS was demonstrated between the 5 patients with PCL graft failure and patients without PCL graft failure (8.9° vs 8.6°; P = .88). Furthermore, no difference was found for PTS in patients with or without a positive posterior drawer test. Therefore, there did not appear to be any significant correlation between PTS and PCL graft laxity in our cohort of combined bicruciate multiligamentous knee reconstructions.
The present study similarly did not demonstrate a correlation between PTS and ACL graft laxity. No difference in PTS was demonstrated for patients with ACL graft failure compared with those without (8.6° vs 8.7°, P = .97). Patients with a positive Lachman test were found to have a slightly higher PTS (9.6° versus 8.5°, P = .15) although this did not reach statistical significance. This trend was expected, as an elevated PTS will place increased stress on ACL grafts. 6 More recently, proximal tibial osteotomies have been indicated in patients with a PTS >12° to decrease the risk of ACL graft failure, especially in the revision setting.3,11,12,37,40,41 In our study of patients who underwent combined ACL and PCL reconstruction, no differences were seen for PROs, Lachman test, ACL graft failure, or ACL revision in patients with a PTS >12°.
A potential reason for the lack of a difference in ACL graft failure based on PTS in our cohort is the fact that these patients also had PCL reconstruction. Although numerous studies have evaluated the effect of PTS on ACL reconstruction and PCL reconstruction independently, less information is available analyzing the effect of PTS on patients undergoing combined ACL and PCL reconstruction.6-8,29,31,34,45 In combined ACL and PCL reconstruction, an important consideration during PCL graft tensioning is to accurately set the tibial station to avoid anterior overreduction of the tibiofemoral joint. The inverse is true for the ACL graft. Therefore, it is possible that these competing interests decrease the PTS effect in the combined ACL- and PCL-reconstructed knee. Although Winkler et al 43 demonstrated an increased risk of PCL graft failure in patients with a decreased PTS, only 48% of their cohort had combined ACL and PCL reconstruction. It is unclear if the significant effect of PTS was present for the patients who underwent combined ACL and PCL reconstruction. Another consideration is the difference in rehabilitation protocols for bicruciate versus single cruciate reconstruction. It is possible that the slower and more restrictive recovery protocols after bicruciate ligament reconstruction may be protective against the increased graft failure risk demonstrated in the isolated cruciate reconstruction literature.
Our data did not demonstrate a significant correlation between PTS and IKDC or Lysholm scores. Linear regression models did show a weak inverse correlation, with higher PTS being correlated with lower PRO scores. This trend was further suggested by the comparison of cohorts with a below-average slope with those with an above-average slope. Patients with an above-average slope trended toward lower IKDC and Lysholm scores, although neither reached statistical significance (P = .08 and .06, respectively). Very little data are available in the literature evaluating the effect of PTS on PROs in patients undergoing combined ACL and PCL reconstruction. Winkler et al 43 did not show a significant correlation between PTS and PROs in their study, which included 48% combined ACL and PCL reconstruction. PRO scores were not reported for the combined ACL and PCL reconstruction subset of patients specifically. Hatch et al 18 reported Multiligament Quality of Life scores for a cohort of 33 patients with knee dislocations. Even though IKDC and Lysholm scores were mentioned for this cohort, specific values were not provided. No mention was made of PTS in the study. Our study contributes to the current paucity of PRO data in the multiligamentous reconstruction literature, especially with respect to PTS.
In our cohort, both vascular and neurologic injuries were statistically significantly correlated with a positive Lachman test at final clinical follow-up. Previous studies have reported the effects of peroneal nerve and vascular injuries on outcomes after ligament reconstruction.21,35 Sanders et al 35 evaluated the effect of vascular injuries on a cohort of patients with MLKI matched to a control group without vascular injury. There was no difference in the presence or absence of a Lachman or posterior drawer test between the matched cohorts. Patients with popliteal artery injuries requiring bypass grafting had significantly lower functional scores. In our study, no difference was seen for IKDC or Lysholm scores for patients with or without a vascular injury (P = .66 and .44, respectively). Krych et al 21 showed that patients with peroneal nerve injuries after a knee dislocation had no difference in Lysholm or IKDC scores compared with those without. Similarly, no difference was seen in our cohort for IKDC or Lysholm scores for patients with a peroneal nerve injury (P = .41 and .19, respectively).
In the present study, generalized ligamentous laxity, as defined by a Beighton score of ≥4 at the preoperative visit, was associated with a positive Lachman test. Ziegler et al 45 demonstrated an increased risk of ACL graft failure in patients with an elevated Beighton score. Similarly, Larson et al 22 showed higher graft failure rates and lower PRO scores for patients with hypermobility undergoing ACL reconstruction. The presence of hyperlaxity as demonstrated by an elevated Beighton score should be considered by the surgeon for the purpose of planning graft choice, optimal graft tensioning, and appropriate postoperative management in these patients.
Mechanism of injury was not correlated with PRO scores, graft failure, Lachman test, or posterior drawer test in our cohort. Similarly, patients with a documented knee dislocation requiring reduction had no significant difference in rates of a positive Lachman test or posterior drawer test at follow-up. Previous studies have reported better range of motion after operative treatment of knee dislocations compared with nonoperative treatment.10,25 In the present cohort, patients with a knee dislocation had a slightly lower arc of motion compared with those without a knee dislocation, but this did not reach statistical significance (118° vs 125°; P = .10).
Our study does have limitations. First, it has the limitations inherent to retrospective studies. These include heterogeneity of surgical techniques and rehabilitation protocols, although these differences are minimal for the surgeons in the current study as standardized rehabilitation protocols have been implemented for >15 years. Second, our study has a wide range of PRO follow-up times. The mean length of PRO follow-up was 5.1 years, ranging from 2 to 16 years. It is possible the PRO values used in our analysis would yield different results if they were obtained at different times in each patient's recovery. An additional limitation includes the fact that laxity was based only on physical examination findings obtained by the treating surgeon, which exposes the data to potential bias. However, the long study period and retrospective nature of the study made obtaining kneeling stress radiographs or KT-1000 arthrometer measurements on each patient impossible. Another potential limitation is the exclusion of coronal plane evaluation, as it was beyond the scope of the current study. However, varus malalignment is implicated in patients with medial compartment knee osteoarthritis, which would confound the results of our PRO outcomes. Finally, our sample size of 98 patients could have been a limiting factor for the observance of statistically significant outcomes. No pre hoc power analysis was performed due to the retrospective nature of the study. In addition, it is difficult to assess the effect of PTS in this heterogeneous patient group with a wide range of injury patterns. However, the cohort in this study is relatively large compared with combined ACL and PCL reconstruction cohorts in other published studies. We also report PRO data in relation to PTS, which was not previously available in the literature.
Conclusion
In this series of bicruciate multiligamentous knee reconstructions (knee dislocation grade 2, knee dislocation grade 3, and knee dislocation grade 4) at midterm follow-up, no differences in graft failures, complications, reoperations, revisions, or PRO scores based on PTS were identified, including for patient with a PTS >12°. Patients with a positive Lachman test were found to have a slightly higher PTS, although this did not reach statistical significance. Further clinical and biomechanical data are necessary to further evaluate a potential relationship.
Footnotes
Final revision submitted October 31, 2023; accepted November 16, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding. A.J.K. has received nonconsulting fees from Arthrex; royalties or licensing fees from Arthrex; consulting fees from Arthrex, the Joint Restoration Foundation, and Responsive Arthroscopy; grants from DJO; and honoraria from Musculoskeletal Transplant Foundation. M.H. has received education payments from Arthrex, Foundation Medical, Medwest Associates, and Smith+Nephew; honoraria from Encore Medical; hospitality payments from Orthalign, Stryker, and Medical Device Business Services; and consulting fees from Vericel. K.R.O. has received education payments from Foundation Medical, Gemini Medical, Arthrex, Endo Pharmaceuticals, Pinnacle, Smith+Nephew, and Medwest Associates; nonconsulting fees from Smith+Nephew, Arthrex, and Medical Device Business Services; hospitality payments from Stryker, Arthrex, and Zimmer Biomet; consulting fees from Endo Pharmaceuticals; grants from Arthrex; and gifts from Wright Medical Technology. M.J.S. has received royalties or licensing fees from Arthrex; consulting fees from Arthrex; nonconsulting fees from Arthrex; and hospitality payments from Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Mayo Clinic (reference No. R07-004018-16).