
Abstract
Background:
Understanding the factors related to patient-reported outcomes (PROs) after anterior cruciate ligament reconstruction (ACLR) can lead to more effective interventions.
Purpose/Hypothesis:
The purpose of this study was to identify factors associated with PRO scores after ACLR. It was hypothesized that concomitant meniscal treatment and postoperative range of motion (ROM) would be associated with early postoperative PRO scores and that postoperative physical findings would be associated with 2-year postoperative PRO scores.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
We examined the data from the Tokyo Medical and Dental University Multicenter Arthroscopic Knee Surgery (TMDU MAKS) Study for patients who underwent primary ACLR with autologous hamstring tendon grafts; 1252 patients in the TMDU MAKS Study were eligible for inclusion. The International Knee Documentation Committee (IKDC) subjective score, Knee injury and Osteoarthritis Outcome Score (KOOS), and Lysholm score of the patients at 3 months (n = 675), 1 year (n = 660), and 2 years (n = 375) postoperatively were assessed using multiple regression to evaluate the strength of the relationship between PRO scores and the following predictor variables: patient-specific factors, treatment-specific factors, and physical findings.
Results:
Improvement in all PROs significantly exceeded the minimal important change at 1 and 2 years postoperatively. Older age and female sex were predictive of lower PRO scores up to 2 years postoperatively. Concurrent meniscal treatment and limited range of knee motion were predictive of lower PRO scores at 3 months and 1 year postoperatively. A tighter knee (ie, less anterior translation) on the injured side compared with the contralateral knee was predictive of lower KOOS–Quality of Life and IKDC scores at 2 years postoperatively. At all 3 postoperative time points, greater side-to-side difference in knee ROM was predictive of lower PRO scores.
Conclusion:
Inferior PRO scores were associated with concomitant meniscal treatment and limited postoperative ROM until 1 year postoperatively and with older age and female sex up to 2 years postoperatively. PRO scores were associated with knee stability at all assessed time points.
Keywords
Patient-reported outcomes (PROs) after anterior cruciate ligament (ACL) reconstruction (ACLR) vary between patients, indicating that there is much room for improvement.18,20 Understanding the factors, including modifiable procedure-specific factors and nonmodifiable patient-specific factors, that can predict or affect PRO scores after ACLR is important for developing the optimal interventions to maximize clinical outcomes. This will also help physicians in counseling patients who are considering ACLR. 1 Using data from the Multicenter Orthopaedic Outcomes Network (MOON) Group, Spindler et al 24 conducted a multivariate analysis to identify predictors of sports function on PROs after ACLR.
During the past decade, large prospective cohort studies have demonstrated the relationships of older age, 5 female sex, 8 higher body mass index, 25 and concomitant meniscal treatment 4 with poorer results on PROs after ACLR. However, a drawback of previous large cohort studies is that the relationship between PRO scores and postoperative physical findings on knee examinations performed on-site, such as the Lachman test, pivot-shift test, and side-to-side differences in the anterior translation of the tibia, has rarely been examined. Magnussen et al 15 enlisted a 430-patient subgroup (nested cohort) of the MOON Group to return to their respective enrolling centers once between 2 and 3 years after surgery for an evaluation of postoperative physical findings. Patients visited their outpatient clinic at 3 months after surgery (to evaluate the possibility of starting jogging), at 1 year after surgery (to assess and promote their sports performance), and at 2 years after surgery, expanding the surveillance objectives of previous studies by including postoperative physical findings performed on-site at serial time points.
In this study, we aimed to identify the factors associated with PROs at 3 months, 1 year, and 2 years after ACLR, using a multicenter serial prospective cohort (Tokyo Medical and Dental University Multicenter Arthroscopic Knee Surgery [TMDU MAKS] Study). We hypothesized that concomitant meniscal treatment and postoperative range of motion (ROM) would be associated with early postoperative PRO scores and that postoperative physical findings would be associated with PRO scores at 2 years after ACLR.
Methods
TMDU MAKS Study
The current study used data from the TMDU MAKS Study, a prospective longitudinal multicenter cohort study that was designed to identify factors predicting the outcomes of knee ligament and meniscal surgeries.9,27 The TMDU MAKS Study was a collaborative effort involving 30 sports medicine surgeons across 12 medical centers. Patient enrollment began in August 2013. A single principal university hospital was responsible for entering the baseline and follow-up data of all participants and functioned as the data coordinating center. The selection of the surgical technique in each case was left to the discretion of the treating surgeon; however, all participating surgeons were board-certified orthopaedists and had completed a subspecialty training program in knee arthroscopy, including physical examinations of the knee joint and knee joint arthroscopic procedures at the principal university hospital. All patients used the same surgical records and physical examination forms. The study protocol received institutional review board approval, and all participating medical centers obtained local institutional review board approval or delegated their approval to the institutional review board of the university hospital. All patients scheduled for knee ligament and meniscal surgery at the medical centers were invited to participate in the TMDU MAKS Study. All patients provided full written informed consent for participation in this clinical research before their inclusion in the TMDU MAKS Study.
Study Participants
In total, 2874 patients were enrolled in the TMDU MAKS Study. Of these, 1485 had an ACL injury. The inclusion criterion for the current study was patients in the TMDU MAKS Study who underwent primary ACLR using an autologous hamstring tendon graft between August 2013 and November 2021. A total of 1300 patients met the inclusion criteria. The exclusion criteria were as follows: (1) patients who experienced concomitant ligament injuries requiring surgery, (2) patients who underwent combined high tibial osteotomy for osteoarthritis or additional procedures for osteochondral defects, (3) patients who had prior surgeries in the involved knee, and (4) patients who had revision surgery for reinjury, meniscal revision surgery for meniscal reinjury, or joint mobilization for joint contracture within 2 years after the index surgery. After excluding 48 patients based on the exclusion criteria, 1252 patients were eligible for the current study (Figure 1). Of these, 675, 660, and 375 patients visited the outpatient clinic at 3 months, 1 year, and 2 years postoperatively, respectively, and were included in the analyses for these time points.

Flowchart of patient inclusion in the study. ACLR, anterior cruciate ligament reconstruction.
Clinical Evaluations
Knee joint extension and flexion ROM, side-to-side difference in extension ROM, side-to-side difference in flexion ROM, Lachman test (International Knee Documentation Committee [IKDC] grades 0-3), anterior drawer test (IKDC grades 0-3), pivot-shift test (IKDC criteria: grade 0 = negative; 1 = glide; 2 = clunk; 3 = gross), anterior knee translation in the injured knee, and side-to-side difference in anterior translation (at 30° of flexion with manual maximum drawer using a KT-1000 arthrometer [MEDmetric]) were recorded preoperatively with the patient under anesthesia in the operating room as well as at 3 months, 1 year, and 2 years postoperatively in the outpatient clinic. After ACLR, each attending surgeon completed the surgical record form to record the surgical technique (single bundle [Figure 2A] or double bundle [Figure 2B]) and any concomitant medial and lateral meniscus treatment (repair or partial meniscectomy).

Representative images of (A) single-bundle and (B) double-bundle anterior cruciate ligament reconstruction. The radiographic images (top row) show the bone tunnel (black arrowheads), and the sagittal and coronal T2-weighted fat-suppressed proton density–weighted magnetic resonance imaging scans (bottom row) show the single-bundle or double-bundle graft (white arrows).
Patients completed the IKDC subjective questionnaire 10 and the Knee injury and Osteoarthritis Outcome Score 21 (KOOS; including the Pain, Symptoms, Activities of Daily Living [ADL], Sports and Recreation [Sports/Rec], and Quality of Life [QOL] subscales) preoperatively and at 3 months, 1 year, and 2 years postoperatively at the outpatient clinic. In addition, the Lysholm score 14 was recorded by each participating attending surgeon preoperatively and at 3 months, 1 year, and 2 years postoperatively. If >50% of the KOOS subscale items were omitted, the response was considered invalid and no subscale score was calculated, as per the 2012 KOOS user guide. The IKDC subjective score was calculated when at least 90% of the items were answered. According to the original scoring instructions for the IKDC Subjective Knee Form, missing values were supplied using the mean score of answered items.
Statistical Analysis
All statistical analyses were performed using SPSS Version 25.0 (IBM Corp). Patient characteristics, postoperative physical findings, and PRO scores were compared at the 3 postoperative time points (3 months, 1 year, and 2 years) using the Kruskal-Wallis test, followed by the Steel-Dwass test as the post hoc test and the Fisher exact test. We evaluated whether patients exceeded the minimal important change in the KOOS subscale scores (0-18.3 points), IKDC subjective score (10.9 points), and Lysholm score (10.3 points) as determined with reference to the Panther Symposium ACL Injury Clinical Outcomes Consensus Group 26 and Nwachukwu et al. 19
Multiple regression analyses were used to assess the strength of the relationship between postoperative PRO scores at the 3 time points and patient-specific factors, treatment-specific factors, and physical findings as predictor variables. The independent variables were the following 14 factors, grouped as patient characteristics (age at surgery and sex), surgical factors (concomitant medial meniscus excision and repair, concomitant lateral meniscus excision and repair, and graft type), and postoperative physical findings (side-to-side difference in knee extension ROM, side-to-side difference in knee flexion ROM, Lachman test grade, anterior drawer test grade, pivot-shift test grade, and anterior knee translation [on injured side and side-to-side difference]). Univariate regression analysis was used to assess the correlation of side-to-side difference in anterior translation with 2-year postoperative IKDC score. Statistical significance for all tests was set at P < .05.
The minimum required sample size for multiple regression was calculated with an α of .05, a β of 0.8, a standardized effect size (f 2) of 0.09, and a number of independent variables (n = 14), resulting in 216 samples indicated for each of the 3 groups. All 3 groups in the current study met the minimum sample size requirement.
Results
There were no significant differences in preoperative patient characteristics among the 3 outcome groups except for preoperative anterior knee translation and surgical technique (Table 1). Extension and flexion ROM decreased from preoperatively to 3 months postoperatively (Table 2). Accordingly, the side-to-side difference in knee extension ROM was greater at 3 months compared with 1 and 2 years postoperatively. The KOOS, IKDC, and Lysholm scores at 3 months postoperatively were comparable to the preoperative scores (Table 3). The scores for all 3 PROs significantly increased from preoperatively to 1 and 2 years postoperatively, exceeding the minimal important change at 1 and 2 years after surgery.
Participant Characteristics According to Outcome Assessment a
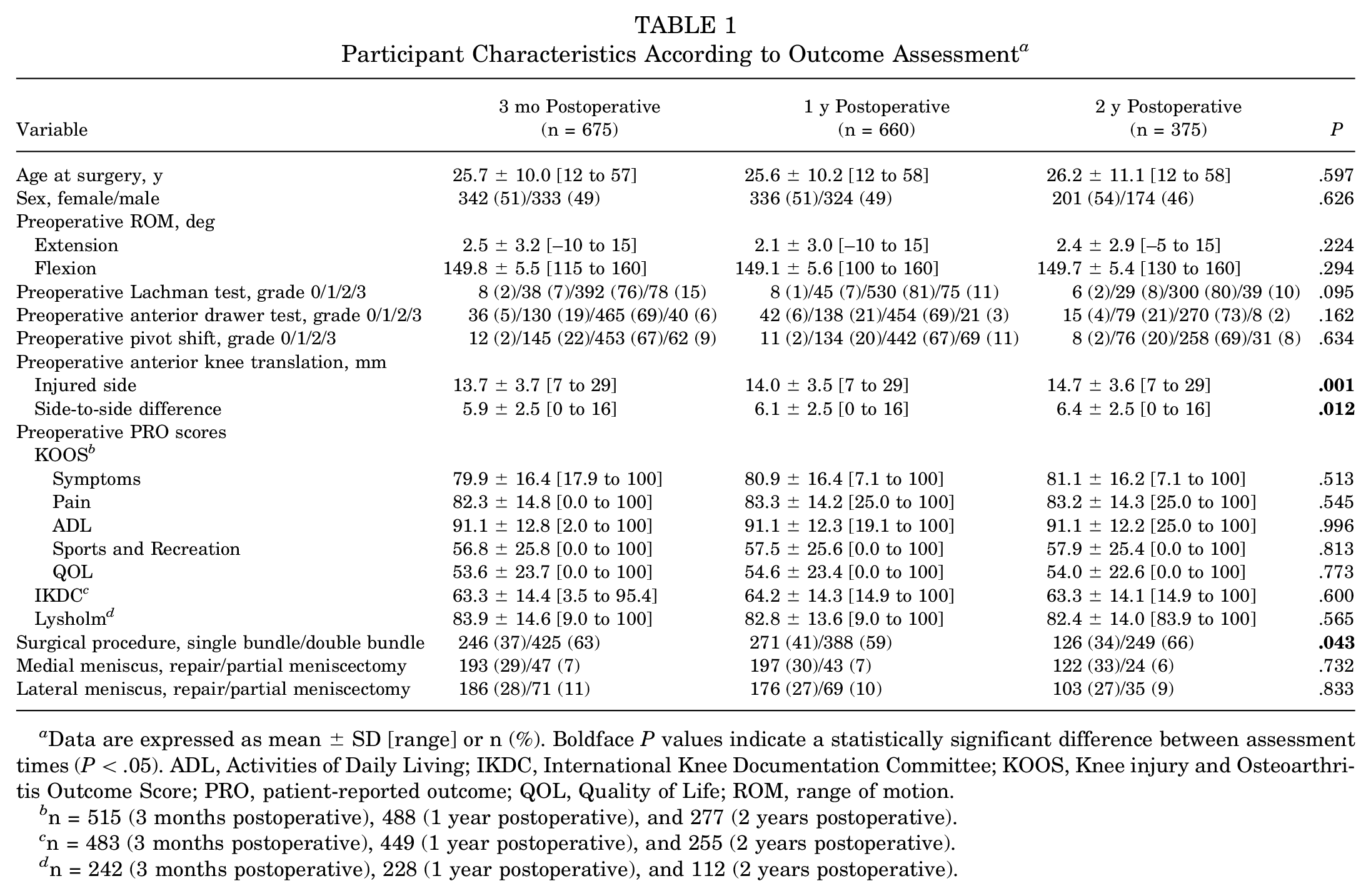
Data are expressed as mean ± SD [range] or n (%). Boldface P values indicate a statistically significant difference between assessment times (P < .05). ADL, Activities of Daily Living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; PRO, patient-reported outcome; QOL, Quality of Life; ROM, range of motion.
n = 515 (3 months postoperative), 488 (1 year postoperative), and 277 (2 years postoperative).
n = 483 (3 months postoperative), 449 (1 year postoperative), and 255 (2 years postoperative).
n = 242 (3 months postoperative), 228 (1 year postoperative), and 112 (2 years postoperative).
Postoperative Physical Findings a

Data are expressed as mean ± SD [range] or n (%). ROM, range of motion; SSD, side-to-side difference.
Pre- and Postoperative PRO Scores a

Data are expressed as mean ± SD [range]. ADL, Activities of Daily Living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; PRO, patient-reported outcome; QoL, Quality of Life.
n = 932 (preoperative), 539 (3 months postoperative), 556 (1 year postoperative), and 303 (2 years postoperative).
n = 808 (preoperative), 509 (3 months postoperative), 528 (1 year postoperative), and 313 (2 years postoperative).
n = 542 (preoperative), 667 (3 months postoperative), 634 (1 year postoperative), and 361 (2 years postoperative).
Factors Associated With PRO Scores at 3 Months After ACLR
Older age was predictive of lower scores on all PROs at 3 months after surgery (Table 4). Male sex was predictive of better KOOS-ADL and Lysholm scores. Among the surgical factors, medial meniscus repair was predictive of worse IKDC scores and all KOOS subscale scores except for KOOS-Symptoms. Compared with double-bundle reconstruction, single-bundle reconstruction was predictive of better KOOS-Pain, KOOS-QOL, and Lysholm scores. Greater side-to-side differences in knee ROM were predictive of lower scores on all PROs. Higher postoperative Lachman test grades were predictive of lower KOOS-Sports and Recreation scores, and higher postoperative anterior drawer test grades were predictive of lower Lysholm scores.
Multiple Regression Analyses of Factors Associated With PRO Scores at 3 Months Postoperatively a

Data are expressed as regression coefficient ± SD; standardized partial regression coefficient (P value). Dashes indicate nonsignificant associations. ACLR, anterior cruciate ligament reconstruction; ADL, Activities of Daily Living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; PRO, patient-reported outcome; QoL, Quality of Life; ROM, range of motion; SSD, side-to-side difference.
Factors Associated With PRO Scores at 1 Year After ACLR
Older age was predictive of lower scores on all PROs 1 year after surgery (Table 5). Male sex was predictive of better KOOS-Symptoms and KOOS-Pain scores. Among the surgical procedures, medial meniscus repair was predictive of lower KOOS-Symptoms and KOOS-Pain scores. Regarding physical findings, greater side-to-side differences in knee ROM were predictive of lower scores on all PROs, and higher postoperative anterior drawer test scores were predictive of lower Lysholm scores.
Multiple Regression Analyses of Factors Associated With PRO Scores at 1 Year Postoperatively a

Data are expressed as regression coefficient ± SD; standardized partial regression coefficient (P value). Dashes indicate nonsignificant associations. ADL, Activities of Daily Living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; PRO, patient-reported outcome; QoL, Quality of Life; ROM, range of motion; SSD, side-to-side difference.
Factors Associated With PRO Scores at 2 Years After ACLR
Two years after surgery, older age was predictive of lower scores on all PROs, and female sex was predictive of lower KOOS-Symptoms scores (Table 6). None of the surgical factors were associated with PRO scores at 2 years postoperatively. Regarding postoperative physical findings, greater side-to-side differences in knee flexion ROM were predictive of lower KOOS-Symptoms scores, and positive Lachman tests were predictive of lower KOOS-QoL scores. Positive Lachman test, anterior drawer test, and anterior knee translation on the injured knee were predictive of lower Lysholm scores. A tighter knee (ie, less anterior translation on the injured side compared with the contralateral knee) as indicated by side-to-side difference in anterior knee translation was predictive of lower KOOS-QoL and IKDC scores. While the absolute value and side-to-side difference in anterior knee translation showed mixed results, scatterplots comparing anterior knee translation side-to-side differences with KOOS-QoL and IKDC scores produced quadratic regression curves with apices at 2.2 and 2.0 mm of anterior knee translation, respectively (Figure 3).
Multiple Regression Analyses of Factors Associated With PRO Scores at 2 Years Postoperatively a

Data are expressed as regression coefficient ± SD; standardized partial regression coefficient (P value). Dashes indicate nonsignificant associations. ADL, Activities of Daily Living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; PRO, patient-reported outcome; QoL, Quality of Life; ROM, range of motion; SSD, side-to-side difference.

Scatterplots showing the postoperative side-to-side difference in anterior knee translation and (A) 2-year postoperative Knee injury and Osteoarthritis Outcome Score Quality of Life (KOOS-QoL) subscore, with the apex of the quadratic regression curve occurring when the side-to-side difference was at 2.2 mm, and (B) 2-year postoperative International Knee Documentation Committee (IKDC) score, with the apex of the quadratic regression curve occurring when the side-to-side difference was at 2.0 mm.
Discussion
The main findings of the present study were that after ACLR with hamstring tendon autograft, lower PRO scores were associated with factors including older age, female sex, concurrent meniscal treatment, limited knee ROM, and both looseness and tightness in knee laxity and that these factors differed over time up to 2 years postoperatively.
In the current cohort, older age was predictive of lower PRO scores for up to 2 years after surgery. A prior single-institution cohort study for single-bundle ACLR found that IKDC subjective scores at 1 year after surgery decreased with older age, with the greatest difference being between the youngest (age, <15 years) and oldest (age, >45 years) patient groups. 28 In a study of data from the Danish Knee Ligament Reconstruction Registry, younger patients (age, ≤12, 13-15, and 15-19 years) had higher scores on the combined KOOS Symptoms, Pain, Sports and Recreation, and QoL subscales compared with adults (age, ≥20 years). 5 The current study extends these findings to include results from multiple regression analyses using multicenter cohort data.
In a study of data from the Swedish National Knee Ligament Registry, Barenius et al 3 observed that medial meniscus treatment was a significant predictor of treatment failure as defined by a prespecified KOOS cutoff score. In a multicenter prospective cohort study that evaluated 1512 individuals for 6 years, Cox et al 4 revealed that lateral meniscus repairs were not associated with inferior results but that medial meniscus repairs predicted worse IKDC subjective and KOOS values at 6 years after ACLR. Those authors referred to a previous suggestion by Shelbourne and Gray 23 that medial meniscal tears differ from lateral meniscal tears on the load distribution function in the ACL-injured population. Similarly, in the current study cohort, concurrent medial but not lateral meniscus repair was found to be predictive of lower PRO scores at 3 months (KOOS-Pain, KOOS-ADL, KOOS-Sports and Recreation, KOOS-QoL, and IKDC) and 1 year (KOOS-Symptoms and KOOS-Pain) postoperatively. On the other hand, medial meniscus repair was not predictive of lower scores at 2 years after surgery. However, since these data are from a cohort study and not a randomized controlled study, they do not necessarily mean that meniscal repair would result in worse outcomes than those in cases in which the injured meniscus had been left unrepaired.
The relevance of clinical measures of residual knee laxity to PRO scores remains inconclusive, and more evidence is needed.6,12 Patients exhibiting a side-to-side difference in residual anterior laxity exceeding 6 mm were noted to have significantly decreased PRO scores 6 years after ACLR in a cohort of 433 patients studied by the MOON Group. 16 Magnussen et al 15 found that the presence of an increased anterior tibial translation side-to-side difference of up to 6 mm was not associated with decreases in PRO scores 2 years after ACLR. Their scatterplot of anterior knee translation and IKDC subjective scores indicated a quadratic regression curve with the apex a bit on the loose side. In the current cohort, looseness on postoperative Lachman test, anterior drawer test, and anterior knee translation in the affected knee, as well as tightness in anterior knee translation side-to-side difference, correlated with lower PRO scores at 2 years postoperatively. Based on these results, surgeons should control knee stability by referencing the contralateral side to ensure the patient's satisfaction.
Restored knee ROM correlated with higher PRO scores at early time points in the current study. Both side-to-side differences in knee ROM and the strength of the associations between side-to-side differences in knee ROM and PRO scores decreased by 2 years postoperatively. Restoration of knee ROM is considered critical for the recovery of postoperative sports activities. Greater postoperative knee extension deficit contributes to quadriceps atrophy at 4 weeks after ACLR. 7 On the other hand, in a review of the effect of physical findings on PROs after ACLR, high-level evidence supporting the association of improvement in postoperative knee ROM with long-term PRO scores was not found. 17
In the present study, factors for lower PRO scores after ACLR varied at different time points. Previous research has shown that older age and female sex contribute to definite poor recovery in muscle strength11,28 and differences in biomechanics 2 over 1 year. Moreover, psychological responses to recovery after ACLR have been shown to vary depending on patient sex and age. 13 Female patients and older patients have a more negative outlook for recovery after ACLR, which can affect PROs in the longer term. 29 Patients undergoing concomitant meniscal treatment may have greater irritation after surgery compared with patients undergoing isolated ACLR. The recovery time after meniscal treatment is shorter than that after ACLR. Mean return-to-sports time after isolated meniscal treatment has been reported to be 5 months. 22 The mechanisms of each factor on outcome vary, and different factors have effects at different time points. Considering these timing differences may improve interventions, however, future studies are needed to reveal the specific mechanisms of each factor on poor outcomes.
The clinical relevance of the current study lies in clarifying the prognostic value of patient-specific factors, including age and sex, for counseling patients undergoing ACLR. Surgeons can share this negative evidence regarding PROs in older or female patients, offer them alternative nonoperative treatments, and support them in reaching a satisfactory decision. With regard to postoperative ROM, the current results support the widely accepted theory that rehabilitative interventions to avoid limited range of residual knee motion are valuable. Finally, both looseness and tightness correlated with the lower knee laxity PRO scores. However, further evidence is needed to obtain robust definitions of the adequate range of knee laxity after ACLR.
Limitations
The most significant limitation of this study was the differences between successive groups caused by the progressive loss to follow-up. The consecutive dropouts may have resulted in some degree of selection bias. Second, several factors that have been shown to affect PRO scores after ACLR in previous studies, such as body mass index, were outside the scope of this study. Third, this study was limited to 2 years of follow-up. Our short-term outcome data did not capture the factors associated with the development of degenerative changes in the knee joints. Fourth, because of the squared terms involved in the quadratic regression, outliers can exert a stronger influence on the fitted curve. To avoid this problem, we examined the outliers in the data set carefully. Fifth, this study only included measurements at 3 months, 1 year, and 2 years after ACLR and did not provide any information for other time points. Finally, prospective cohort studies have an inherent technical limitation in that the nonrandomized design precludes inferences about causality; therefore, care should be taken when interpreting the results.
Conclusion
The nature of the factors associated with lower PRO scores after ACLR with autologous hamstring tendon differed over time. Inferior PRO outcomes were associated with concomitant meniscal treatment and limited postoperative ROM until 1 year after surgery and with older age and female sex up to 2 years after surgery. Knee stability was associated with PRO scores at all assessed time points.
Footnotes
Acknowledgements
The authors thank Atsushi Okawa, MD, PhD, for continuous support; all collaborators for data collection; and Aiko Yamada, Haruno Kroda, Kahaer Abula, Yuki Omura, Masayo Tsukamoto, and Miyoko Ojima for data registration. The authors also thank Editage and Vern Fischer for English language editing.
The authors also acknowledge the following study collaborators: From Kawaguchikogyo General Hospital: Akiho Hoshino, MD, PhD; Takashi Ogiuchi, MD, PhD; Toru Takahashi, MD, PhD; Hiroko Ueki, MD, PhD; Kenta Katagiri, MD, PhD; Kazumasa Kawata, MD, PhD; and Masaaki Isono, MD, PhD. From Doai Memorial Hospital: Tomohiko Tateishi, MD, PhD; Etsuko Matsumura, MD, PhD; So Suzuki, MD, PhD; and Kiyotaka Horiuchi, MD, PhD. From Yokohama Minato Red Cross Hospital: Koji Asano, MD, PhD, and Kaori Nakamura, MD, PhD. From Tama-Hokubu Medical Center, Jyu Neishin, MD, PhD; Mio Udo, MD, PhD; and Kei Inomata, MD, PhD. From Nitobe Memorial Nakano General Hospital: Arata Yuki, MD, PhD. From Suwa Central Hospital: Shinichi Shirasawa, MD, PhD. From Nissan Tamagawa Hospital: Katsuaki Yanagisawa, MD, PhD. From Tsuchiura Kyodo General Hospital: Daisuke Hatsushika, MD, PhD. From Soka City Hospital: Shinpei Kondo, MD, PhD. From Tokyo Bay Urayasu Ichikawa Medical Center: Enichi Nakatsuru, MD. From Tokyo Medical and Dental University Hospital: Masaki Amemiya, MD; Jae-Sung An, MD; Mai Katakura, MD, PhD; Takashi Hoshino, MD, PhD; and Nobutake Ozeki, MD, PhD. From Nerima General Hospital: Masayuki Shimaya, MD, PhD; and Mari Uomizu, MD, PhD. From Kyoundo Hospital: Masafumi Horie, MD, PhD, and Mika Yamaga, MD, PhD. From Dokkyo Medical University Saitama Medical Center: Toshifumi Watanabe, MD, PhD; Ryusuke Saito, MD, PhD; and Mikio Shioda, MD, PhD. From Tokyo-Kita Medical Center: Tomoyuki Mochizuki, MD, PhD, and Kanehiro Hiyama, MD, PhD.
Final revision submitted October 31, 2023; accepted November 15, 2023.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Tokyo Medical and Dental University (ref No. M2000-1547-01).