
Abstract
Background:
Borderline developmental dysplasia of the hip (BDDH) accompanied by cam deformity and subspinous impingement has been found to benefit from arthroscopic surgery. However, the research comparing BDDH combined with osseous impingement to femoroacetabular impingement (FAI) without borderline dysplasia remains limited.
Purpose/Hypothesis:
To compare the clinical symptoms, intraoperative findings, and outcomes of hip arthroscopy in patients with BDDH and osseous impingement versus cam-type FAI. It was hypothesized that BDDH with osseous impingement could be classified as a distinct entity between FAI and developmental dysplasia of the hip (DDH).
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Data were collected from patients 18 to 50 years old who underwent primary hip arthroscopy between September 2016 and October 2020. Patients were divided based on preoperative lateral center-edge angle (LCEA) into 2 groups: (1) BDDH group (LCEA 18°-25°; n = 67); and (2) cam-type FAI group without BDDH (FAI group; LCEA 25°-40° and alpha angle >55°; n = 145). Disparities in symptoms, preoperative examination, intraoperative findings and procedures, and patient-reported outcome (PRO) scores were compared.
Results:
Follow-up was available for 61 (91.0%) patients in the BDDH group and 125 (86.2%) patients in the FAI group. The incidence of cam deformity in BDDH patients was 91.8%. The preoperative characteristics and intraoperative findings were similar between the groups; however, preoperative internal and external hip rotation, Tönnis angle, femoroepiphyseal acetabular roof index, labral size, capsule thickness, and percentage of ligamentum teres tear were significantly higher in the BDDH group than the FAI group, and the percentage of pain aggravating factor, cam deformity, and anterior inferior iliac spine types 2 and 3 were also significantly different between groups (P < .05 for all). The percentage of intraoperative minimal acetabuloplasty, subspinous decompression, labral repair, ligamentum teres debridement, and capsular closure was significantly higher in the BDDH group than the FAI group, while the percentage of femoroplasty was higher in the FAI group (P < .05). Pre- to postoperative improvement on PRO scores was seen in both groups.
Conclusion:
Given the differences in etiology and surgical procedures between the 2 conditions, it is suggested that BDDH with osseous impingement be classified as an entity distinct from FAI and DDH (and separate from BDDH without impingement) while excluding joint instability.
Keywords
Borderline developmental dysplasia of the hip (BDDH) has been defined as either a lateral center-edge angle (LCEA) from 18° to 25° or from 20° to 25°.1,2,4,8,10,25 The prevalence of symptomatic BDDH may be as high as 12.8%, and the risk of osteoarthritis in individuals with BDDH is 1.4 to 2.0 times that of the general population. 15 Since Fredensborg 14 described BDDH as being LCEA between 20° and 25° using the Wiberg method in 1976, there has been ongoing controversy surrounding the imaging parameters and range values that define BDDH. Various parameters, such as the anterior center-edge angle, Tönnis angle, Sharp angle, acetabular anterior wall index, posterior wall index, and femoroepiphyseal acetabular roof (FEAR) index, have been utilized in the definition, classification, and evaluation of joint stability in developmental dysplasia of the hip (DDH) or borderline dysplasia of the hip.9,36,37 However, determining the most effective parameters or combinations thereof for assessing acetabular undercoverage and guiding surgical interventions has proven challenging.
Hip instability is generally defined as extraphysiologic hip motion that causes pain with or without symptoms of hip joint unsteadiness.5,20 Hip microinstability is defined as persistent excessive hip motion (insufficient to be classed as dislocation or subluxation) that has become symptomatic, especially with pain, and is associated with hip dysplasia and ligamentous laxity. 22 It remains a challenging diagnosis for clinicians to make.
The objective of hip preservation for BDDH is to improve pathological injury and slow the advancement of osteoarthritis. Long-term studies have shown that periacetabular osteotomy (PAO) is efficacious in improving pain and delaying or preventing hip osteoarthritis in cases with absolute dysplasia. 29 Hip arthroscopy has the advantages of being less invasive, with less morbidity, faster recovery, and no necessity of osteosynthesis. Moreover, mid- and long-term favorable outcomes have been achieved for BDDH with cam deformity or anterior inferior iliac spine (AIIS) morphology type 2 or 3,2,3 in which type 1 morphology has a smooth ilium wall without any bony prominence extending from the caudal area of the AIIS to the acetabular rim, type 2 contains a bony prominence that rests at the level of the acetabular rim, and type 3 has an AIIS that extends distally to the anterosuperior acetabular rim. 13
The purpose of this study was to report the outcomes of hip arthroscopic surgery for patients with BDDH and cam-type FAI without borderline dysplasia and compare the differences between the 2 groups. We hypothesized that (1) patients with BDDH and cam-type FAI would achieve comparable outcomes during a minimum 2-year follow-up period, and (2) it would be possible to categorize BDDH with osseous impingement as a distinct entity between FAI and DDH.
Methods
Patient Characteristics
The ethics review board of our hospital approved the protocol for this study, and all study participants provided written informed consent. Data were retrospectively reviewed for 639 patients who underwent arthroscopic surgery by a senior surgeon (C.L.) between September 2016 and October 2020. BDDH was defined as LCEA between 18° and 25° (Wiberg) as measured on preoperative weightbearing anteroposterior pelvic radiographs,1,2,13,36 and BDDH with osseous impingement was defined as an alpha angle >55° or exhibiting local pincer or prominent AIIS type 2 or 3 on computed tomography (CT) and 3-dimensional (3D) reconstruction. Cam-type FAI without borderline dysplasia was defined as LCEA 25° to 40° and alpha angle >55°. 16
Study inclusion criteria were as follows: (1) age 18 to 50 years; (2) unsuccessful nonoperative treatment for at least 3 months; and (3) symptoms confirmed to be caused by intra-articular pathological changes with an ultrasound-guided local anesthesia injection test.10,26 Exclusion criteria were as follows: (1) any positive outcomes on tests for joint instability 19 ; (2) FEAR index of >5°22,37; (3) previous hip surgery, fracture, avascular necrosis, hyperplastic or immune hip disease; and (4) Tönnis grade ≥2, joint space <2 mm, or articular cartilage exfoliation. Patients were divided into 2 distinct groups: (1) borderline dysplasia (LCEA 18°-25°; BDDH group) and (2) cam-type FAI without borderline dysplasia (LCEA 25°-40° and alpha angle >55°; FAI group).
A total of 67 patients diagnosed with BDDH and 145 patients with cam-type FAI without borderline dysplasia were initially enrolled. In this study cohort, 4 patients with positive joint instability tests and 6 patients with FEAR index >5° were excluded. Ultimately, 61 patients in the BHHD group (91.0% follow-up rate) and 125 patients in the FAI group (86.2% follow-up rate) were included in the study. Figure 1 shows the participant-inclusion process.

Flowchart of patient inclusion in the study.
Clinical Symptoms and Physical Examinations
We examined the location, nature, and severity of preoperative hip pain as well as aggravating factors. The physical examinations encompassed various assessment, such as hip range of motion (specifically flexion/adduction and abduction/internal and external rotation), the flexion/adduction/internal rotation (FADIR) and flexion/abduction/external rotation (FABER) tests, and the hyperflexion rotary compression test of AIIS.13,16,31 Joint instability was evaluated through physical examinations involving anterior apprehension, abduction/extension/external rotation, or prone external rotation tests.19,22
Radiologic Evaluation
The imaging examination included weightbearing anteroposterior pelvic radiographs, CT and 3D reconstruction, and single-hip magnetic resonance imaging (MRI) scans. Anteroposterior pelvic radiographs were employed to evaluate parameters such as LCEA, Tönnis angle, neck stem angle and joint space, and osteoarthritis Tönnis grade. 36 CT and 3D reconstruction were utilized to assess cam deformity, focal pincer, and AIIS morphology.13,17 Single-hip MRI scans were used to analyze the labral size, 21 capsule thickness, 32 soft tissue injury (labral and ligamentum teres), and articular cartilage damage (acetabular and femoral head).
Arthroscopic Findings and Techniques
All patients underwent general anesthesia while lying supine on a traction bed. The joint space was distracted to create an anterolateral portal, a midanterior portal, and a distal anterolateral accessory portal. The extent and severity of labral (Seldes grade), 33 articular cartilage (Outerbridge grade),3,30 and ligamentum teres (Domb grade) 11 injuries were examined. Intraoperative procedures included minimal or moderate acetabuloplasty based on LCEA, decompression of AIIS type 2/3, repair or debridement of the labrum, chondroplasty or microfracture, femoroplasty, and capsular closure. Greater trochanteric bursitis was treated if necessary.
Rehabilitation
The rehabilitation process was broadly divided into 4 stages. Stage 1 was to protect the hip joint as much as possible (1-4 weeks postoperatively). Patients were instructed to use crutches and bear partial weight on their foot while avoiding extension and external rotation to minimize stress on the capsular repair. Additionally, patients were prescribed nonsteroidal anti-inflammatory drugs for 2 to 3 weeks to prevent the occurrence of heterotopic ossification. As patients were weaned from crutches, they progressed through the institutional rehabilitation. 18 Stage 2 consisted of motor neuromuscular retraining (4-6 weeks postoperatively), stage 3 consisted of muscle balance and strength training (6-12 weeks postoperatively), and stage 4 consisted of hip and lower limb function training (12-18 weeks postoperatively) to improve the stability and balance of the hip and lower limbs.
Clinical Evaluation
The patient-reported outcomes (PROs) assessed in this study comprised the modified Harris Hip Score (mHHS), the International Hip Outcome Tool-12 (iHOT-12), and a 10-point visual analog scale (VAS) for pain (10 = worst pain) and for patient satisfaction (10 = most satisfied). The percentage of patients who achieved the minimal clinically important difference (MCID) and patient acceptable symptom state (PASS) was calculated for both the HHS and iHOT-12 scores.2,7,10
Statistical Analyses
All statistical analyses were performed using SPSS for Windows Version 24.0 (IBM). Quantitative variables were reported as mean ± SD. The independent samples t test was employed for data with a normal distribution and homogeneity of variance. In cases where variables did not follow a normal distribution, the Mann-Whitney U test was utilized. The Welch analysis of variance was employed when variance was heterogeneous. Qualitative data were analyzed using either a chi-square or Fisher exact test. The level of statistical significance was set at P < .05.
Results
Patient Characteristics
The mean ages of patients in the BDDH group (n = 61) and those in the FAI group (n = 125) were 30.5 ± 8.5 and 31.0 ± 9.5 years, respectively, and the mean body mass indices were 22.9 ± 3.5 and 23.9 ± 4.2 kg/m2, respectively, with no significant difference between the 2 groups.
Clinical Symptoms and Physical Examinations
Table 1 shows the clinical and physical examination findings according to study group. Patients in the BDDH group had significantly greater hip external rotation (P = .030) and internal rotation (P = .001), and the pain aggravating factors were statistically different from those in the FAI group (P = .027).
Group Comparison of Clinical Presentation and Physical Examination Findings a

Data are reported as n (%) or mean ± SD. Boldface P values indicate statistically significant difference between groups (P < .05). BDDH, borderline developmental dysplasia of the hip; FABER, flexion/abduction/external rotation; FADIR, flexion/adduction/internal rotation; FAI, femoroacetabular impingement.
Radiologic Evaluation
There was a significant difference between the BDDH and FAI groups in the proportion of patients with cam deformity (91.8% vs 100%; P = .003) and AIIS types 2 and 3 (60.7% vs 39.2%; P = .022) (Table 2 and Figure 2). The occurrence of local pincer in the BDDH group was not significantly different from the FAI group (9.8% vs 18.4%; P = .131). The Tönnis angle, FEAR index, labral width, capsule thickness, and percentage of patients with ligamentum teres tear were significantly higher in the BDDH versus the FAI group (P < .05 for all), and the LCEA was significantly higher in the FAI than the BDDH group (P = .001) (Table 2 and Figure 3).
Group Comparison of Radiologic Evaluation
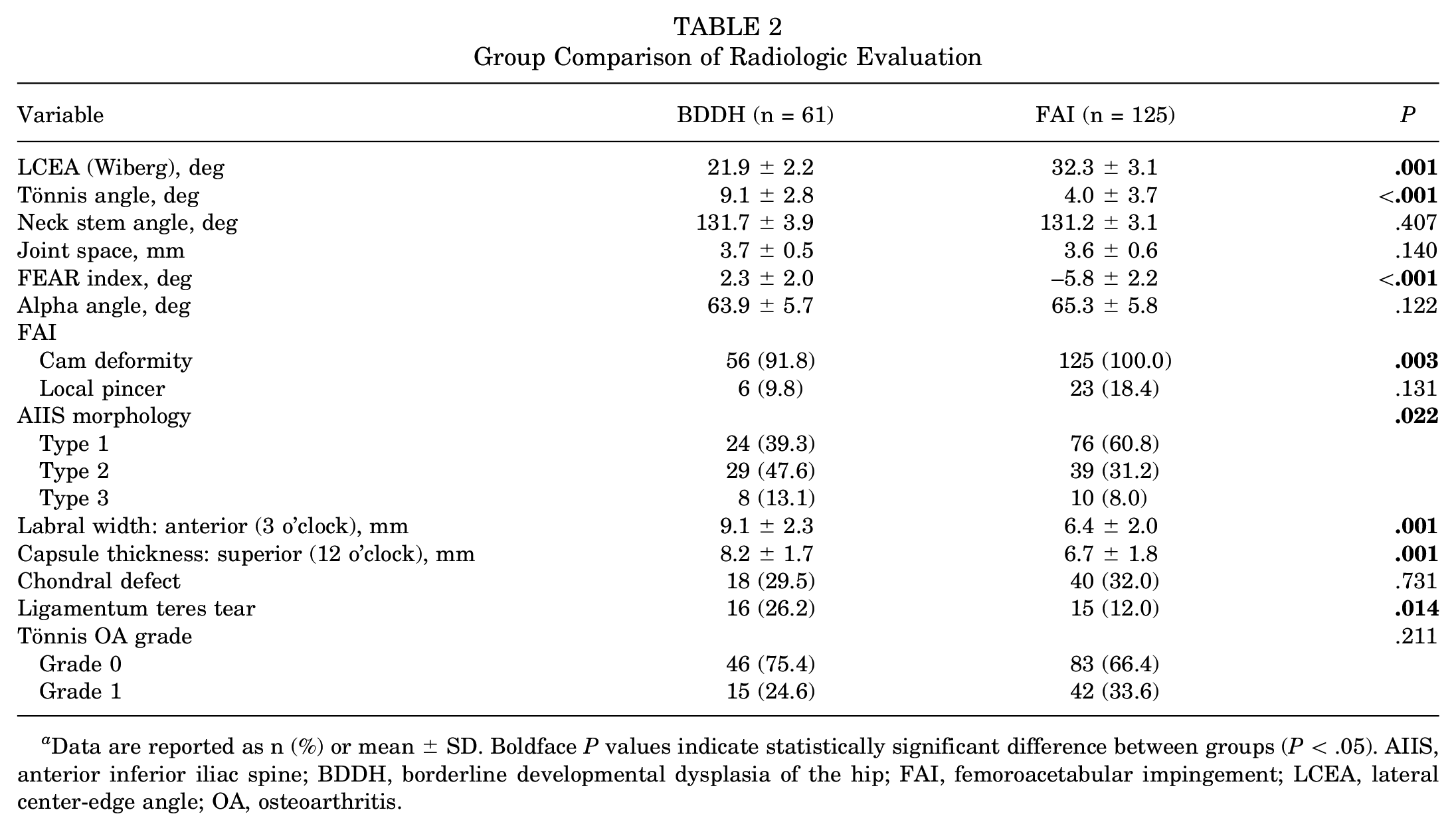
Data are reported as n (%) or mean ± SD. Boldface P values indicate statistically significant difference between groups (P < .05). AIIS, anterior inferior iliac spine; BDDH, borderline developmental dysplasia of the hip; FAI, femoroacetabular impingement; LCEA, lateral center-edge angle; OA, osteoarthritis.

Three-dimensional computed tomography images showing (A) cam deformity and anterior inferior iliac spine. (B) type 1, (C) type 2, and (D) type 3 morphology (black arrows).

(A) Measurement of anterior labral width on a coronal MRI scan (3 o’clock). (B) Measurement of superior capsule thickness on a coronal magnetic resonance imaging (MRI) scan (12 o’clock). (C) Arrow shows thickened, heterogeneously hyperintense ligamentum teres on a coronal MRI scan.
Arthroscopic Findings and Procedures
The only significant difference in intraoperative findings observed between groups was the percentage of ligamentum teres tear (P = .005) (Table 3). In the BDDH group, minimal acetabuloplasty was performed, except for 6 patients with local pincer, and all patients underwent labral repair and fixation as well as capsular closure. Arthroscopic procedures are shown in Figure 4 and compared between groups in Table 4. Intraoperative subspinous decompression was performed in 60.7% of patients in the BDDH group and 39.2% of patients in the FAI group (P = .001), and femoroplasty was performed in 91.8% of patients in the BDDH group and 100% of patients in the FAI group (P = .006). Within the FAI group, 12 (9.6%) patients underwent minimal acetabuloplasty (LCEA of 25°-28°), 28 (22.4%) patients underwent labral selective debridement due to poor labrum quality, and 33 (26.4%) patients did not undergo capsular closure due to the location of cam deformity near the head and neck junction and only a “transverse” incision of the joint capsule.
Group Comparison of Intraoperative Findings a

Data are reported as n (%). Boldface P value indicates statistically significant difference between groups (P < .05). BDDH, borderline developmental dysplasia of the hip; FAI, femoroacetabular impingement.

Arthroscopic procedures: (A) subspinous decompression, (B) labral repair, (C) ligamentum teres debridement, (D) femoroplasty, and (E) capsular closure.
Group Comparison of Arthroscopic Procedures a
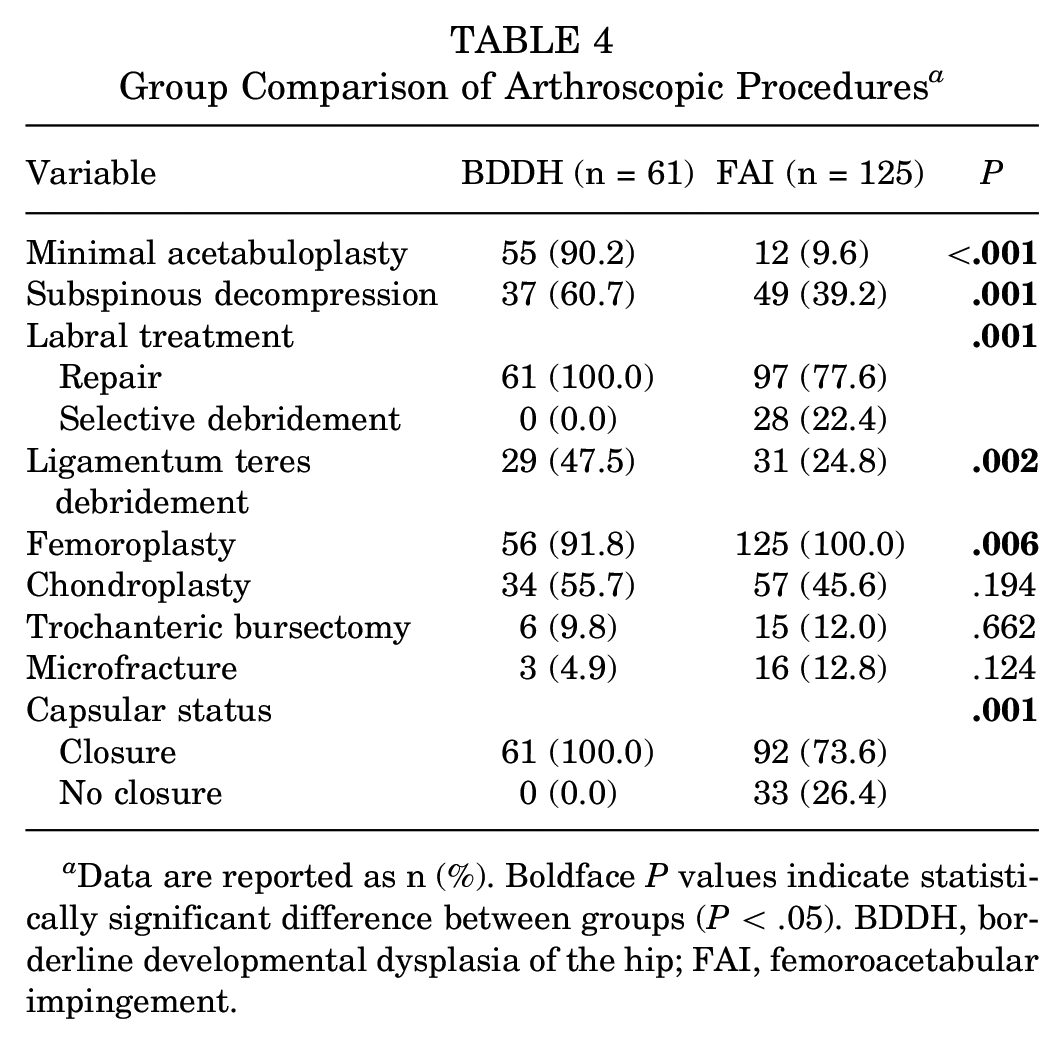
Data are reported as n (%). Boldface P values indicate statistically significant difference between groups (P < .05). BDDH, borderline developmental dysplasia of the hip; FAI, femoroacetabular impingement.
Evaluation of Functional Outcomes
At the final postoperative follow-up, the VAS pain, mHHS, and iHOT-12 scores exhibited a significant improvement compared to the preoperative scores, with no significant differences between the groups. Furthermore, there were no significant difference between the groups in terms of patient satisfaction or the percentage of patients who achieved the MCID and PASS for both mHHS and IHOT-12 (Table5).
Group Comparison of Patient-Reported Outcome Scores and Achievement of MCID and PASS a
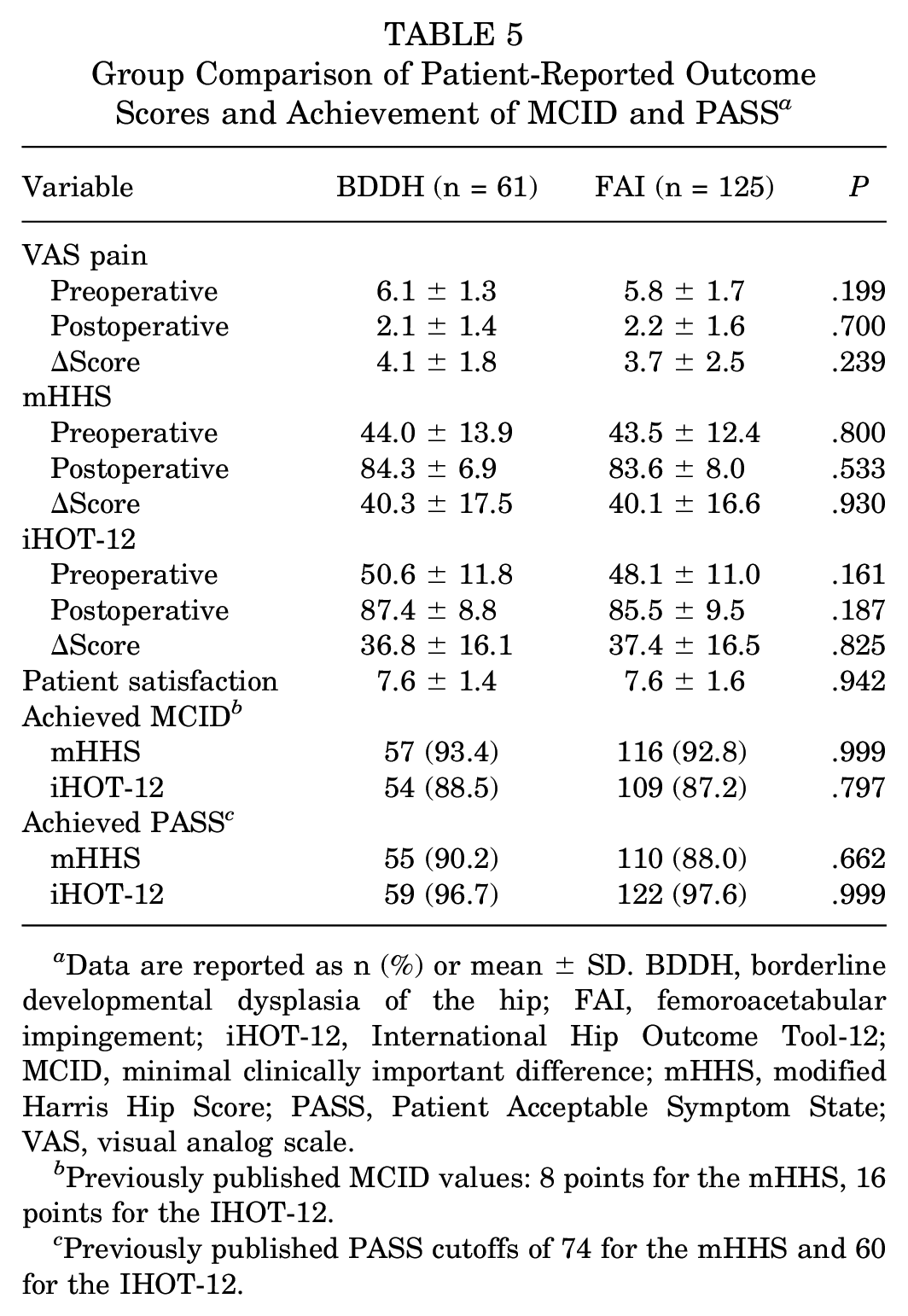
Data are reported as n (%) or mean ± SD. BDDH, borderline developmental dysplasia of the hip; FAI, femoroacetabular impingement; iHOT-12, International Hip Outcome Tool-12; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; PASS, Patient Acceptable Symptom State; VAS, visual analog scale.
Previously published MCID values: 8 points for the mHHS, 16 points for the IHOT-12.
Previously published PASS cutoffs of 74 for the mHHS and 60 for the IHOT-12.
Complications
Within 1 week after surgery, 7 patients experienced numbness in the perineum and the area innervated by the lateral femoral cutaneous nerve (3 patients in the BDDH group and 4 patients in the FAI group). Additionally, 8 patients developed iliopsoas muscle snaps within 1 to 2 months postoperatively and received symptomatic and physical therapy (4 patients in the BDDH group and 4 patients in the FAI group). These symptoms resolved after the outpatient visit 5 months postoperatively. Importantly, none of the patients required conversion to PAO or total hip arthroplasty.
Discussion
The findings of the current study demonstrated that patients with BDDH had a high incidence of bony impingement, specifically cam deformity (91.8%) and AIIS types 2 and 3 (60.7%). Preoperatively, some symptoms and signs in patients with BDDH resembled those of individuals with cam-type FAI, and arthroscopic surgery for BDDH both with and without with osseous impingement and cam-type FAI yielded satisfactory and comparable clinical outcomes, assuming joint instability was excluded.
Diagnosis of hip microinstability remains a challenge. Wyatt et al 37 proposed the FEAR index to predict the joint stability of BDDH. A systematic review demonstrated that the FEAR index has a high agreement and consistent application, making it a useful diagnostic tool in hip-preservation surgery, particularly in patients with BDDH. 9 A positive result from any joint instability test (abduction-hyperextension-external rotation, the prone instability, and the hyperextension-external rotation tests) predicts hip microinstability in 86.3% to 90.9% of patients. 19 Expert consensus suggests that diagnostic criteria should be subcategorized into patient history, examination, and imaging, such as hip pain, positive anterior apprehension or hyperextension external rotation tests, and FEAR index of >5°. 22
Both PAO and hip arthroscopy with capsular placation have been shown to provide patients with BDDH with clinically significant improvements and low revision rates at a minimum of 5 years postoperatively. 1 However, the optimal approach treatment for symptomatic BDDH remains to be debated. BDDH combined with hip instability is more likely to fail an arthroscopic-only approach. 23 PAO is efficacious in improving pain and delaying or preventing hip osteoarthritis in cases with true dysplasia 29 and in treating patients with hip instability that does not improve after single or multiple hip arthroscopic procedures. 5
The clinical manifestations of BDDH are similar to FAI in certain cases. The incidence of BDDH combined with cam deformity is in the range of 40% to 93%, with overlapping clinical manifestations and impingement symptoms. 10 DDH is more serious than BDDH in terms of acetabular undercoverage; thus, cam deformity in DDH may not lead to early mechanical impingement. 27 Although a prominent AIIS does not typically cause symptoms in individuals without hip abnormalities, cam deformity in the presence of hip dysplasia and/or hip flexion in patients with FAI is prone to impingement with AIIS, and subspinous decompression under arthroscopy is a safe and effective method to prevent this. 13 Thus, the symptoms of BDDH caused by impingement are similar to those of patients with cam-type FAI.
For patients with BDDH with osseous impingement, the surgical strategy varies from that for cam-type FAI due to the coexistence of acetabular undercoverage and impingement. Previous studies have shown that satisfactory clinical outcomes can be achieved for BDDH through labral repair and fixation with minimal acetabuloplasty.1,28 Our findings indicate that patients with BDDH have significantly greater labral size, capsule thickness, and percentage of ligamentum teres tear compared to patients with FAI. The reason may be related to the compensatory reaction of soft tissue with acetabulum undercoverage.
Of the patients with BDDH in this study, labral repair and fixation was performed based on minimal acetabuloplasty, except for 6 patients with local pincer, and all patients underwent capsular closure. Bryan et al 6 reported that acetabular rim resection exceeding 3 mm posed a risk for unfavorable postoperative outcomes in patients with hip dysplasia. Similarly, Chandrasekaran et al 8 proposed that a threshold of 2 mm for acetabular rim resection should be observed to prevent hip instability. In recent years, the significance of the labrum in maintaining joint stability has gained increasing recognition among experts and scholars. 38 The expert consensus on the classification system and treatment strategy for arthroscopy in cases of labral injury recommends that repair, fixation, or reconstruction of a damaged labrum should be carried out as far as possible for patients with hip dysplasia to avoid excessive cleaning. 24 The capsule is an important part of hip joint function and stability. A literature review suggests that suture of the joint capsule should be performed after capsule incision in patients with BDDH to avoid iatrogenic joint instability. 12
We suggest that BDDH with osseous impingement should be classified as a distinct entity between FAI and DDH (and separate from BDDH without impingement), while excluding joint instability. First, it should be noted that the utilization of LCEA has certain limitations in accurately classifying hip dysplasia and formulating appropriate surgical strategies. Relying solely on LCEA measurements to determine the extent of undercoverage may result in mischaracterizing the morphology and insufficiently informing treatment decision. 35 Second, BDDH frequently coexists with osseous impingement, which is becoming recognized as a problem in its own right, requiring dedicated treatment. 2 Third, the identification of the underlying causes of symptoms holds substantial significance in the development of surgical protocols. The current study highlighted the importance of classifying patients into impingement or instability categories and tailoring treatment appropriately with arthroscopic surgery or PAO, respectively. 34 Beck et al 4 recognized that not all patients with acetabular dysplasia had hip instability, and a significant number of these patients had cam deformity, and these patients did not have instability but impingement. Simultaneously, the reason for the revision hip arthroscopy may be related to the secondary injury caused by residual cam deformity and prominent AIIS. 6
Limitations
There are several limitations to our study. First, the minimum follow-up time was 25 months, and it remains uncertain as to whether the observed improvement will be sustained over a longer duration. A more extensive study involving a longer-term follow-up is currently being conducted at our institution to address this concern. Second, we did not assess the presence of generalized ligamentous laxity in our patients. Additional research is needed to determine whether generalized ligamentous laxity affects the clinical outcomes of hip arthroscopy for the treatment of BDDH. Third, the surgical strategy in this study is more suitable for patients with BDDH combined with bony impingement.
Conclusion
Arthroscopy performed on patients with BDDH and osseous impingement and those with cam-type FAI yielded comparable results. BDDH often presented with a significant incidence of osseous impingement, and certain symptoms and signs exhibited similarities with cam-type FAI. Given the differences in etiology and surgical procedure between the 2 conditions, it is suggested that BDDH with osseous impingement should be classified as a distinct entity between FAI and DDH (and separate from BDDH without impingement), while excluding joint instability.
Footnotes
Final revision submitted October 12, 2023; accepted October 24, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding was received from the National Natural Science Foundation of China (grant 82072517). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Chinese PLA General Hospital (ref No. S2021-018-01).