
Abstract
Background:
The function of the iliocapsularis (IC) muscle is still unclear. Previous studies have reported that the cross-sectional area of the IC may be useful in identifying borderline developmental dysplasia of the hip (BDDH).
Purpose:
To evaluate the pre- to postoperative changes in IC cross-sectional area in patients with femoroacetabular impingement (FAI) and to determine if there are any associations with clinical outcomes after hip arthroscopy.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
The authors retrospectively evaluated patients who underwent arthroscopic surgery for FAI at a single institution between January 2019 and December 2020. Patients were divided into 3 groups according to lateral center-edge angle: BDDH group (20°-25°), control group (25°-40°), and pincer group (>40°). Supine anteroposterior hip radiographs, 45° Dunn view radiographs, computed tomography scans, and magnetic resonance imaging (MRI) scans were obtained for all patients preoperatively and postoperatively. The cross-sectional areas of the IC and the rectus femoris (RF) were measured on an axial MRI slice at the level of the femoral head center. Preoperative and final follow-up scores on the visual analog scale for pain and the modified Harris Hip Score (mHHS) were compared between groups with the independent-samples t test.
Results:
A total of 141 patients (mean age, 38.5 years; 64 male, 77 female) were included. The preoperative IC-to-RF ratio of the BDDH group was significantly higher than that of the pincer group (P < .05). In the BDDH group, there was significant pre- to postoperative decrease in IC cross-sectional area and the IC-to-RF ratio (P < .05 for both) as well as a significant correlation between the preoperative IC cross-sectional area and the postoperative mHHS (r = 0.434; P = .027).
Conclusion:
Patients with BDDH had a significantly higher preoperative IC-to-RF ratio than patients with pincer morphology. A higher preoperative IC cross-sectional area was associated with better postoperative patient-reported outcomes after arthroscopy for the treatment of FAI combined with BDDH.
Keywords
The iliocapsularis (IC) is a hip muscle overlying the anterior hip capsule that originates at the anteroinferior iliac spine and the anteromedial hip capsule and inserts distal to the lesser trochanter. 17,18 Although the function of the IC is still unclear, it may act as an anterior stabilizer of the hip or play a role in capsular retraction during hip flexion. 2,10,11,13,14,16 In hips with developmental dysplasia of the hip (DDH), this muscle contraction would help stabilize the femoral head in the deficient acetabulum. 2,10 After evaluating the anatomic dimensions of the IC in 85 patients, Babst et al 2 concluded that it was important for stabilizing the femoral head in a deficient acetabulum. Haefeli et al 10 reported that the proportion of the IC to the rectus femoris (RF; IC-to-RF ratio) could be used as an adjunct for clinical decision making in hips with borderline DDH (BDDH) and a concomitant cam-type deformity.
As the characteristics of the IC in patients with BDDH have not been assessed, the purpose of the current study was to evaluate the pre- to postoperative changes in the IC cross-sectional area in patients with femoroacetabular impingement (FAI) and to determine if there are any associations between the cross-sectional area of the IC and clinical outcomes after hip arthroscopy.
Methods
Patients
The study protocol was approved by the ethics committee of our hospital. We retrospectively evaluated patients who attended the sports medicine clinic of our department and who underwent arthroscopic surgery for FAI between January 2019 and December 2020. The inclusion criteria were patients who (1) were diagnosed with FAI through clinical findings, plain radiographs, computed tomography scans, and magnetic resonance imaging (MRI) scans; (2) underwent hip arthroscopy for FAI; (3) underwent postoperative MRI ≥6 months postoperatively; and (4) attended the clinical follow-up ≥12 months postoperatively. Patients with previous hip surgery or those who could not complete the MRI and clinical follow-up were excluded from this study. All participants signed informed consent forms.
Arthroscopic Surgery
All surgeries were performed using a standard supine approach as described by Gao et al. 8 In brief, the interportal capsulotomy technique was used to access the hip joint using the anterolateral and midanterior portals. A detailed inspection of the central compartment was performed to assess the acetabular rim, acetabular labrum, articular cartilage, and ligamentum teres. Labral repair or labral debridement was performed according to the nature of the injury. Femoral osteoplasty or acetabuloplasty was performed according to the intraoperative findings. Capsular closure was routinely done at the end of surgery using a side-to-side suture.
Patients who had concomitant BDDH underwent modified capsular plication. In brief, a double-loaded suture anchor with 4 needles was used for labral repair and capsular plication. One suture limb of the double-loaded suture anchor was passed through the labrum at the chondrolabral junction using a tissue-penetrating device and retrieved about 4 mm from initial penetration through the labral base to complete a repair. The other suture limb was passed through the distal end of the incised capsule, and the distal capsule was pulled to the acetabular rim to increase capsular tension to improve stability.
Postoperative Rehabilitation
Postoperative rehabilitation began with ankle pumps, quadriceps strengthening, and other isometric exercises 1 or 2 days after surgery, as described in a previous study. 9 Hip passive range of motion (ROM) exercise as tolerated began at 3 or 4 days after surgery. Partial weightbearing with crutches began at 3 to 7 days, and passive and active ROM exercises were performed as tolerated after 4 weeks postoperatively. Patients were expected to advance to full weightbearing and regain symmetrical hip ROM by 6 weeks after surgery.
Clinical Evaluation
Patient-reported outcomes (PROs) were recorded preoperatively and at the final follow-up (≥12 months after hip arthroscopy) and included the visual analog scale (VAS) for pain and the modified Harris Hip Score (mHHS). For the mHHS, the minimal clinically important difference (MCID) was defined as 8 points by Kemp et al, 12 and the Patient Acceptable Symptom State (PASS) score was defined as 74 points by Chahal et al. 5 The PROs at the final follow-up were evaluated at the same time as those recorded during the MRI follow-up. In addition, we recorded any complications or revision hip arthroscopy.
Radiographic and MRI Evaluation
Hip MRI was performed with a 3.0-T MR scanner (Magnetom Trio with TIM System; Siemens Healthcare) and a dedicated flexible surface coil around the affected hip joint, as described by Gao et al. 7 The preoperative alpha angle and lateral center-edge angle (LCEA) were measured on the 45° Dunn view and supine anteroposterior hip radiographs, respectively, as described in previous studies. 1,3 The first author (G.G.), who had >5 years of experience in hip MRI and arthroscopy, analyzed all images and was blinded to the clinical and operative findings. Based on the LCEA measurement, the patients were divided into 3 groups: BDDH group (20°-25°), control group (25°-40°), and pincer group (>40°) (Figure 1).
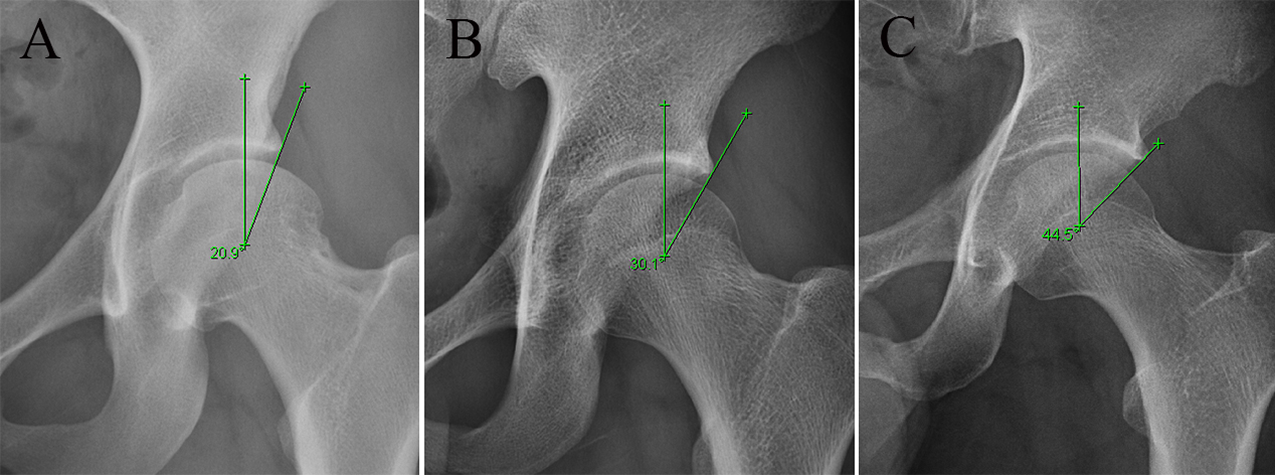
Supine anteroposterior hip radiographs showing representative preoperative lateral center-edge angles (LCEAs) in the 3 study groups: (A) borderline developmental dysplasia group (LCEA, 20°-25°), (B) control group (LCEA, 25°-40°), and (C) pincer group (LCEA, >40°).
The cross-sectional areas of the IC and the RF were measured preoperatively and postoperatively on a single MRI axial slice at the level of the femoral head center as described by Haefeli et al 10 (Figure 2). The measurements were performed by 2 evaluators (G.G. and Y.X.). The outlines of both the IC and RF were determined manually, and the cross-sectional area of each was calculated using Digimizer Image Analysis software (Version 4.5.2; MedCalc Software Ltd). The IC-to-RF ratio was calculated by dividing the IC cross-sectional area by the RF cross-sectional area. We randomly selected 30 scans to evaluate interrater reliability.

The iliocapsularis (IC) and rectus femoris (RF) were outlined manually at the level of the femoral head center on an axial magnetic resonance imaging scan.
Statistical Analysis
Differences in continuous variables with a normal distribution in the baseline data between the 3 study groups were examined using the independent-samples t test. The 2-tailed paired t test was used to evaluate significance between preoperative and postoperative data. Differences in categorical variables were compared using the chi-square test. The Pearson correlation coefficient (r) was used to test for the association between the imaging parameters (IC cross-sectional area, RF cross-sectional area, and IC-to-RF ratio) and postoperative PRO scores. Interrater reliability of the MRI measurements was evaluated using a 2-way, mixed, absolute-agreement, single-measures intraclass correlation coefficient. P values <.05 were considered statistically significant. A Bonferroni correction was used to control for the remaining multiple comparisons, with statistical significance defined as P ≤ .001. All statistical analyses were performed using SPSS Statistics (Version 22; IBM Corp).
Results
As shown in Table 1, 141 patients (mean age, 38.5 years; age range, 20-67 years; 64 male, 77 female) were included in this study. There were 54 left sides and 87 right sides. The mean alpha angle of all patients was 56.0° ± 6.4°, and the mean LCEA was 33.9° ± 9.5°. The mean follow-up time was 26.1 months (range, 12-36 months).
Patient Characteristics (N = 141) a
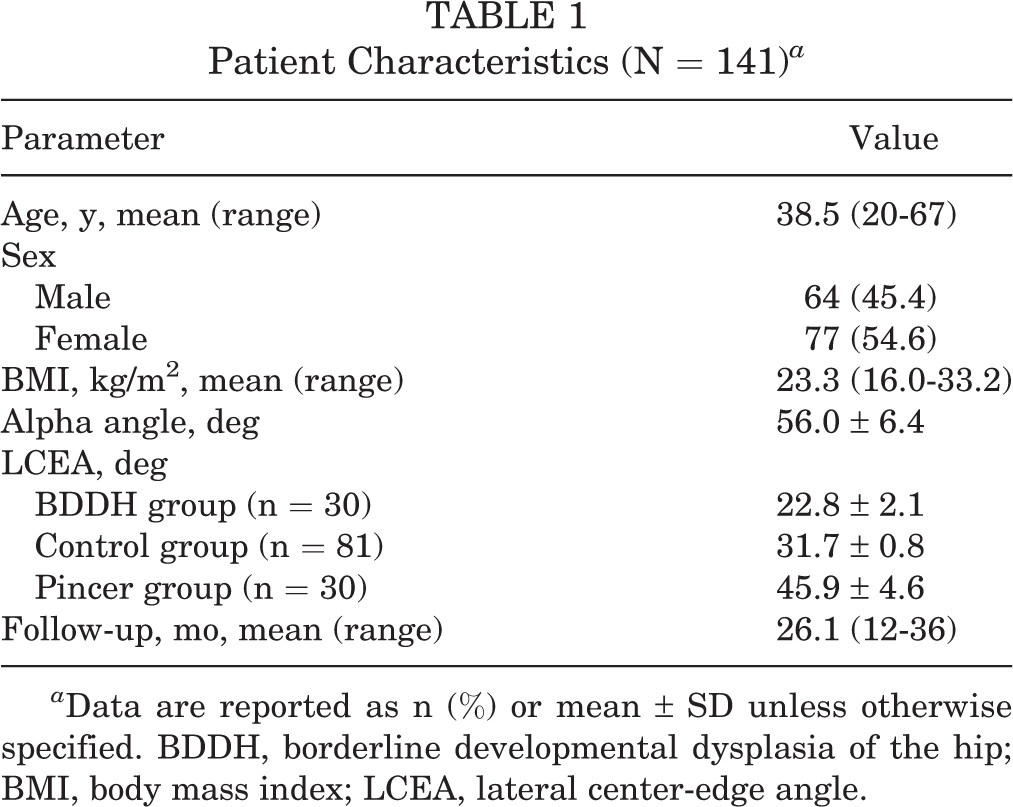
a Data are reported as n (%) or mean ± SD unless otherwise specified. BDDH, borderline developmental dysplasia of the hip; BMI, body mass index; LCEA, lateral center-edge angle.
Of the 141 patients, there were 30 (21.3%) in the BDDH group, 81 (57.4%) in the control group, and 30 (21.3%) in the pincer group. There was no significant difference in age, sex, body mass index, or alpha angle among the 3 groups. There was a significant difference in LCEA among the 3 groups (P < .05). Arthroscopic procedures performed by group are shown in Table 2.
Arthroscopic Procedures Performed in 3 Groups a

a BDDH, borderline developmental dysplasia of the hip.
PRO Scores
The preoperative mHHSs of the BDDH, control, and pincer groups were 47.4 ± 13.3, 49.4 ± 12.3, and 48.1 ± 10.1, respectively, and the postoperative mHHSs were 75.4 ± 13.8, 76.2 ± 18.3, and 74.6 ± 17.7, respectively. The preoperative VAS scores of the BDDH, control, and pincer groups were 4.7 ± 1.9, 4.6 ± 1.8, and 4.9 ± 1.8, respectively, and the postoperative VAS scores were 1.0 ± 1.1, 1.1 ± 0.9, and 0.9 ± 1.3, respectively. Patients in all 3 groups saw significant pre- to postoperative improvement in both PROs (P < .05 for all), with no significant difference in preoperative or postoperative PRO scores among the groups (P > .05). The percentages of patients who achieved the PASS for the mHHS were 93.3%, 93.3%, and 96.7% for the BDDH, control, and pincer groups, respectively (P > .05), and the percentages of patients who surpassed the MCID were 83.3%, 80.0%, and 83.3%, respectively (P > .05).
Imaging Outcomes
The intraclass correlation coefficient values for the preoperative IC and RF cross-sectional areas were 0.82 and 0.93, respectively, and the values for the postoperative cross-sectional areas were 0.81 and 0.91, respectively, indicating excellent interrater reliability.
The comparison of imaging parameters between groups and between preoperative and postoperative measurements is shown in Table 3. Compared with preoperative values, there was a significant decrease in the postoperative IC cross-sectional area and the postoperative IC-to-RF ratio in the BDDH group (P < .008 for both). There was no significant pre- to postoperative difference in the IC cross-sectional area between the control and pincer groups, and there was no significant pre- to postoperative difference in the RF cross-sectional area in any of the groups. The preoperative IC-to-RF ratio of the BDDH group was significantly higher than that of the pincer group (P < .008).
Comparison of the Imaging Parameters Between the Study Groups a

a Data are reported as mean ± SD. Boldface P values indicate statistically significant differences between the groups compared (P < .05). BDDH, borderline developmental dysplasia of the hip; CSA, cross-sectional area; IC, iliocapsularis; Postop, postoperative; Preop, preoperative; RF, rectus femoris.
In the BDDH group, there was a significant correlation between the preoperative IC cross-sectional area and the postoperative mHHS (r = 0.434; P = .027). There was no correlation between preoperative RF cross-sectional area and postoperative PRO scores, and no correlation between postoperative cross-sectional areas (IC or RF) and postoperative PRO scores.
Discussion
The literature suggests that the IC is a tightener of the hip capsule, 18 thus stabilizing the anterior part of the hip joint. 2,6,10,15 Walters et al 17 thought that the IC formed the largest muscular contribution to the capsule of the hip joint and hypothesized that the IC together with the gluteus minimis, the reflected head of the RF, and the horizontal and vertical limbs of the iliofemoral ligament form a “stability arc” that prevents anterior subluxation or dislocation of the femoral head. 11 The IC is an important landmark in direct anterior approaches to the hip joint for total hip arthroplasty, periacetabular osteotomies, and arthroscopic T-capsulotomy. 4,6,11
In this study, the preoperative IC-to-RF ratio of the BDDH group was significantly higher than that of the pincer group (P < .008). This result was similar to the studies of Haefeli et al 10 and Babst et al. 2 They reported that IC was observed to be hypertrophied in patients with hip dysplasia, while on the other hand it was atrophied in those with excessive acetabular coverage. Babst et al thought the reason was that extra stabilization was provided by the abnormal excessive bone and fibrocartilage of the acetabulum in patients with excessive coverage, whereas IC may act to support the femoral head in the acetabulum in patients with dysplasia. A similar finding could also be observed in patients with BDDH according to our study. We postulate that this was because patients with BDDH had similar instability to those with DDH.
Postoperative muscle atrophy is common after hip arthroscopy, 19 so the IC-to-RF ratio was also calculated. We found that the IC cross-sectional area and IC-to-RF ratio in the BDDH group decreased after hip arthroscopy, and there was no significant difference between the preoperative and postoperative RF cross-sectional areas in all 3 groups. IC may be damaged during arthroscopic capsulotomy. However, there was no significant difference between preoperative and postoperative IC cross-sectional areas in the control and pincer groups. We postulate that capsular plication increased the tension of the capsule and provided extra stabilization, so the function of the IC in capsular retraction decreased and atrophied because there was no need to compensate for the instability of BDDH. This indirectly explained the function of the IC as an anterior stabilizer of the hip or a tightener of the hip capsule.
In the current study, there was a significant correlation between the preoperative IC cross-sectional area and the postoperative mHHS in the BDDH group (r = 0.434; P = .027). A higher preoperative cross-sectional area may predict better clinical outcomes for arthroscopic treatment of FAI combined with BDDH. We thought that preoperative compensatory hyperplasia of the IC could play a role in stabilization of the hip and improve functional scores after operation. Patients with strong muscle compensation may have better postoperative outcomes. The IC cross-sectional area would decrease after capsular plication in patients with BDDH, as the capsule provided extra stabilization. The decrease in cross-sectional area may indirectly indicate that the preoperative compensatory function of the IC decreased after capsular plication provided extra stabilization. Further study is needed to identify the reasons for these changes.
Limitations
This study has several limitations. First, the IC and RF cross-sectional areas were measured only on a single MRI axial slice at the level of the femoral head center. MRI in this study did not include their entire course. However, this measurement method has been proven useful by previous studies. 2,10 Second, we were unable to exclude all potential causes for muscle hypertrophy and atrophy in this retrospective study. However, all patients underwent the same postoperative rehabilitation process in our hospital, which minimized the influence of postoperative rehabilitation on the muscles. Third, the time points of follow-up varied from 12 to 36 months, and the IC and RF cross-sectional areas may be different at different time points. Further study is needed to find the changes in IC and RF cross-sectional areas over time.
Conclusion
Patients with BDDH had a significantly higher preoperative IC-to-RF ratio than patients with pincer morphology. A higher preoperative IC cross-sectional area was associated with better postoperative PRO scores after hip arthroscopy for the treatment of FAI combined with BDDH.
Footnotes
Final revision submitted October 18, 2022; accepted October 26, 2022.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Peking University Third Hospital.