
Abstract
Background:
Subspine impingement, or anterior inferior iliac spine (AIIS) impingement, is a type of extra-articular pathology associated with femoroacetabular impingement syndrome and often requires subsequent arthroscopic surgery.
Purpose:
To examine the diagnostic accuracy, prevalence, and clinical outcomes of arthroscopic treatment for AIIS impingement.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 2020 checklist was applied. We searched for studies on the prevalence, diagnostic accuracy, and results of surgical treatment for AIIS impingement. For each included study, data synthesis and statistical analysis were performed to identify pooled prevalence, calculate clinical outcome scores, and estimate adverse events. The QUADAS (a quality assessment tool for diagnostic accuracy studies) was used to assess the quality of the diagnostic accuracy studies, and the Risk of Bias Assessment tool for Nonrandomized Studies was used to assess the quality of the studies on arthroscopic treatment efficacy.
Results:
Out of an initial 791 studies, 23 were included. AIIS impingement was diagnosed by plain radiography with 76% to 86% sensitivity, 3-dimensional computed tomography with 80% to 81.8% sensitivity, magnetic resonance imaging with 80% sensitivity, and ultrasound with 92.5% sensitivity. For patients who underwent hip arthroscopy, the pooled prevalence of AIIS impingement was 18%. Significant improvement between pre- and postoperative clinical outcomes was observed: 25.75 points for the modified Harris hip score (mHHS), 46.88 points for the Hip Outcome Score–Sport subscale, 20.85 points for the Nonarthritic Hip Score, and -2.92 points for the pain visual analog scale. The minimal clinically important difference on the mHHS was exceeded by 94% of patients. The pooled incidence of surgical complications was 1%. Of 6 included studies on diagnostic accuracy, 2 were identified as having a low risk of bias, and 4 included >2 factors with a high risk of bias. All 9 included studies on treatment outcomes had at least 1 factor with a high risk of bias.
Conclusion:
Several imaging modalities assist in the diagnosis of AIIS impingement. The overall prevalence of AIIS impingement in patients that underwent hip arthroscopy was 18%. Clinical outcomes after arthroscopic AIIS decompression were generally favorable, with a relatively low rate of surgical complications.
Keywords
Recent developments in the field of hip arthroscopic surgery have enabled effective surgical treatment of femoroacetabular impingement (FAI) syndrome (FAIS), 29 including other extra-articular pathologies. 19 Subspine impingement, also known as anterior inferior iliac spine (AIIS) impingement, is an important cause of FAI-related hip pain, 7 although it is often overlooked. Although the underlying cause is unclear, AIIS impingement is likely induced by mechanical stress around the subspine region of the AIIS, just adjacent to the acetabulum labrum and capsule; this stress is triggered by particular hip positions such as deep flexion or internal rotation with flexion such as high-kicking dancing. 25 Stress can be induced not only by visible morphologic abnormalities but also by a combination of dynamic factors plus FAI morphology. 7 In particular, existing AIIS impingement is an important risk factor for treatment failure after arthroscopic surgery. 34 Despite accumulating evidence concerning FAIS pathology, many unanswered questions remain, particularly about extra-articular pathology and AIIS impingement.
In the clinical setting, it is important to know how AIIS impingement is diagnosed, its actual prevalence, and likely clinical outcomes after arthroscopic surgery. Although several studies have examined AIIS in the context of these clinical issues, a limited number of systematic reviews or meta-analyses has been performed. 9,36 The purpose of this systematic review and meta-analysis is to clarify the following clinical questions: (1) What are the imaging and diagnostic options for AIIS impingement? (2) What is the prevalence of AIIS impingement? (3) Is arthroscopic decompression a useful and safe treatment for AIIS impingement? It was hypothesized that several imaging modalities are available for AIIS impingement, its prevalence may vary by population, and arthroscopic decompression is a promising surgical option with acceptable clinical outcomes.
Methods
A systematic review and meta-analysis were conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 2020 guidelines and was registered on PROSPERO (CRD42021281554).
Literature Search
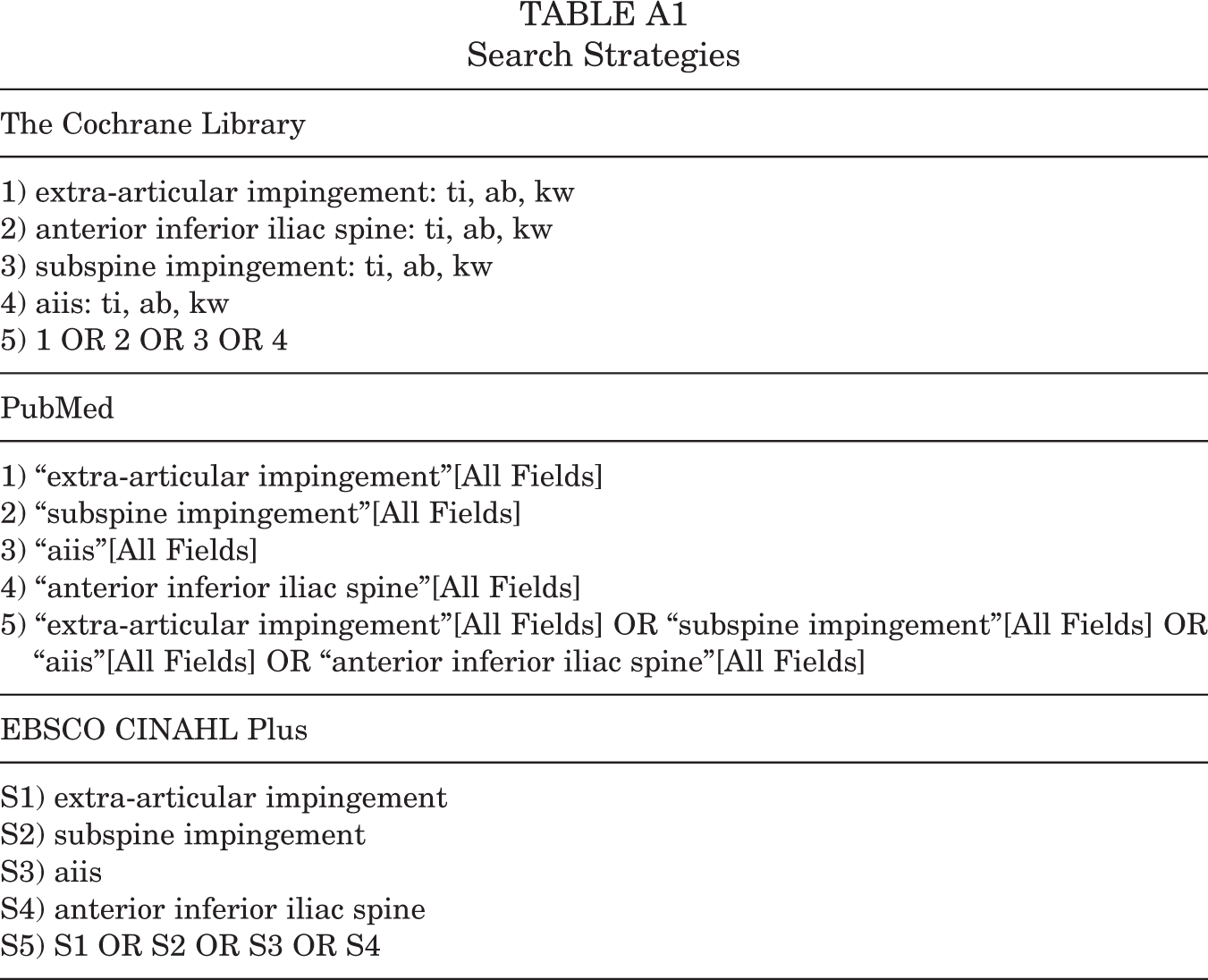
Multiple comprehensive literature searches of the PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL), and Cochrane Library databases were performed on May 6, 2021. Search keywords included (“extra-articular impingement” OR “anterior inferior iliac spine” OR “subspine” OR “aiis”). An additional manual search was performed to identify other relevant articles or bibliographies. Topics covered were (1) the prevalence of AIIS impingement, (2) the accuracy of diagnostic tests for AIIS impingement, and (3) results of treatment for AIIS. The detailed search strategies are listed in Appendix Table A1.
Study Screening and Eligibility Assessment
After the first extraction, an initial screen was performed by 2 reviewers (N.K. and E.K.). During this screen, the title and abstract were reviewed, and inappropriate literature was excluded. Disagreements were resolved by discussion. Duplicate articles were removed. Next, an eligibility assessment of full manuscripts was performed by the same 2 reviewers. Exclusion criteria were animal studies, reviews, case reports, technical notes, letters to the editor, and expert opinions. There was no language restriction. The inclusion criteria were as follows: Prevalence: All studies that reported prevalence of AIIS, subspine, or extra-articular impingement. Diagnostic accuracy: Inclusion criteria were articles that reported the sensitivity and specificity of radiographs, computed tomography (CT), magnetic resonance imaging (MRI), ultrasound (US), and physical examination for AIIS impingement. Only studies that mentioned sensitivity and specificity were included. Treatment: Studies that reported (1) a direct comparison between preoperative and postoperative groups following AIIS decompression, in which primary or revision arthroscopy was performed; (2) patient-reported outcomes both preoperatively and postoperatively; and (3) a minimum follow-up period of 6 months.
Data Synthesis and Statistical Analysis
Data from each eligible study were extracted independently by 2 authors (N.K. and E.K.). For studies that did not report standard deviations, the method outlined in the Cochrane handbook was used. 17 If pooling of data was not possible, a narrative approach was used to describe the studies. Pooled prevalence and adverse events estimation for AIIS were calculated using Freeman Tukey double arcsine transformation and Dersimonian-Laird random-effects models, 8,13 respectively. To assess the effects of differences in patient background, a subgroup analysis of high-kicking athletes and nonathletes was performed. For treatment-based studies, the clinical outcome scores were classified. Pooled clinical outcome scores were calculated based on unadjusted mean differences (MDs), with 95% CIs. Pooled MDs of clinical outcome scores were calculated using random-effects models. A P value < .05 was considered statistically significant. The heterogeneity of treatment effects among studies was evaluated by calculating the I 2 value. All statistical analyses were conducted using R (R Core Team, 2020). R package “meta” and “metafor” were used to estimate prevalence and clinical outcome.
Evaluation of Bias Risk
The quality of the studies was assessed independently by 2 reviewers (Y.Y. and E.K.). No specific tool/scoring system was used to assess the quality of studies examining prevalence and morphology. QUADAS (a quality-assessment tool for diagnostic accuracy studies) was graded to assess the quality of diagnosis studies. The Risk of Bias Assessment tool for Nonrandomized studies was graded to assess the quality of treatment studies. Publication bias was evaluated by constructing a funnel plot for each outcome.
Results
Figure 1 shows a flowchart illustrating study screening and eligibility assessment. This process identified 23 studies, of which 6 were imaging diagnosis studies, 2,4,6,18,22,35 9 were prevalence studies, 2,5,21,23 –25,27,32,33 9 reported outcomes after arthroscopic treatment, ∥ and 9 studies ¶ reported on adverse effects after arthroscopic treatment.

Flowchart of the systematic review conducted according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 2020 guidelines. *Titles and abstracts did not meet our inclusion criteria.
A summary of the 6 studies 2,4,6,18,22,35 on diagnostic imaging accuracy is shown in Table 1. Plain radiographs, 3-dimensional reconstructed CT (3D-CT), MRI, and US were used for diagnosis of AIIS impingement. For plain radiographs, the sensitivity was 76% to 86% and the specificity was 53% to 64%, for MRI the sensitivity was 80% and specificity was 81%, for US the sensitivity was 92.5% and specificity was 96%, and for 3D-CT the sensitivity was 80% to 81.8% and specificity was 23% to 70.5%.
Summary of Studies on Diagnostic Imaging Accuracy (n = 6) a

a AIIS, anterior inferior iliac spine; FAI, femoroacetabular impingement; 3D-CT, 3-dimensional reconstructed computed tomography; MRI, magnetic resonance imaging.
Table 2 shows a summary of the 9 studies 2,5,21,23 –25,27,32,33 on the prevalence of AIIS impingement. Figure 2 shows the pooled prevalence of AIIS impingement in patients who underwent hip arthroscopy; there were no studies on prevalence in the general population. The random-effects model revealed that the overall prevalence of AIIS impingement in the primary arthroscopy group was 18% (95% CI, 13%-26%). Subgroup analysis of the high-kicking athlete group revealed a high prevalence of impingement (72%) compared with the primary or revision arthroscopy group (23%).
Summary of Studies on AIIS Impingement Prevalence (n = 9) a

a 3D, 3-dimensional; AIIS, anterior inferior iliac spine; CT, computed tomography; FAI, femoroacetabular impingement.

Forest plots showing prevalence of anterior inferior iliac spine impingement in the primary arthroscopy (18%), revision arthroplasty (23%), and high-kicking athlete (72%) populations. Heterogeneity was identified as high for all 3 populations, with I 2 values of 82%, 97%, and 93%, respectively. The funnel plot for prevalence studies revealed a symmetric property regarding publication bias.
The 9 studies on the outcomes of surgical treatment for AIIS impingement are summarized in Table 3. Figure 3 shows a forest plot of the MDs between pre- and postoperative modified Harris Hip Scores (mHHS), the percentage of mHHS that exceeded the minimal clinically important difference (MCID; the previously published MCID of 8.2 was used as a reference), 31 the Hip Outcome Score–Sport subscale (HOS-S), the Nonarthritic Hip Score (NAHS), and pain visual analog scale (VAS). Improvements in each score were observed after arthroscopic decompression of AIIS impingement: 25.75 for mHHS, 94% for mHHS exceeding MCID, 46.88 for HOS-S, 20.85 for NAHS, and -2.92 for VAS.
Summary of Studies on Arthroscopic Treatment Outcomes for AIIS Impingement (n = 9) a

a AIIS, anterior inferior iliac spine; F, female; FAI, femoroacetabular impingement; HOOS, Hip disability and Osteoarthritis Outcome Score; HOS, Hip Outcome Score; HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-S, Hip Outcome Score–Sport subscale; iHOT, International Hip Outcome Tool; M, male; mHHS, modified Harris Hip Score; NA, not available; NAHS, Nonarthritic Hip Score; ROM, range of motion; SF-12, 12-Item Short Form Health Survey; VAS, visual analog scale for pain.
b May include ±SD or (range).
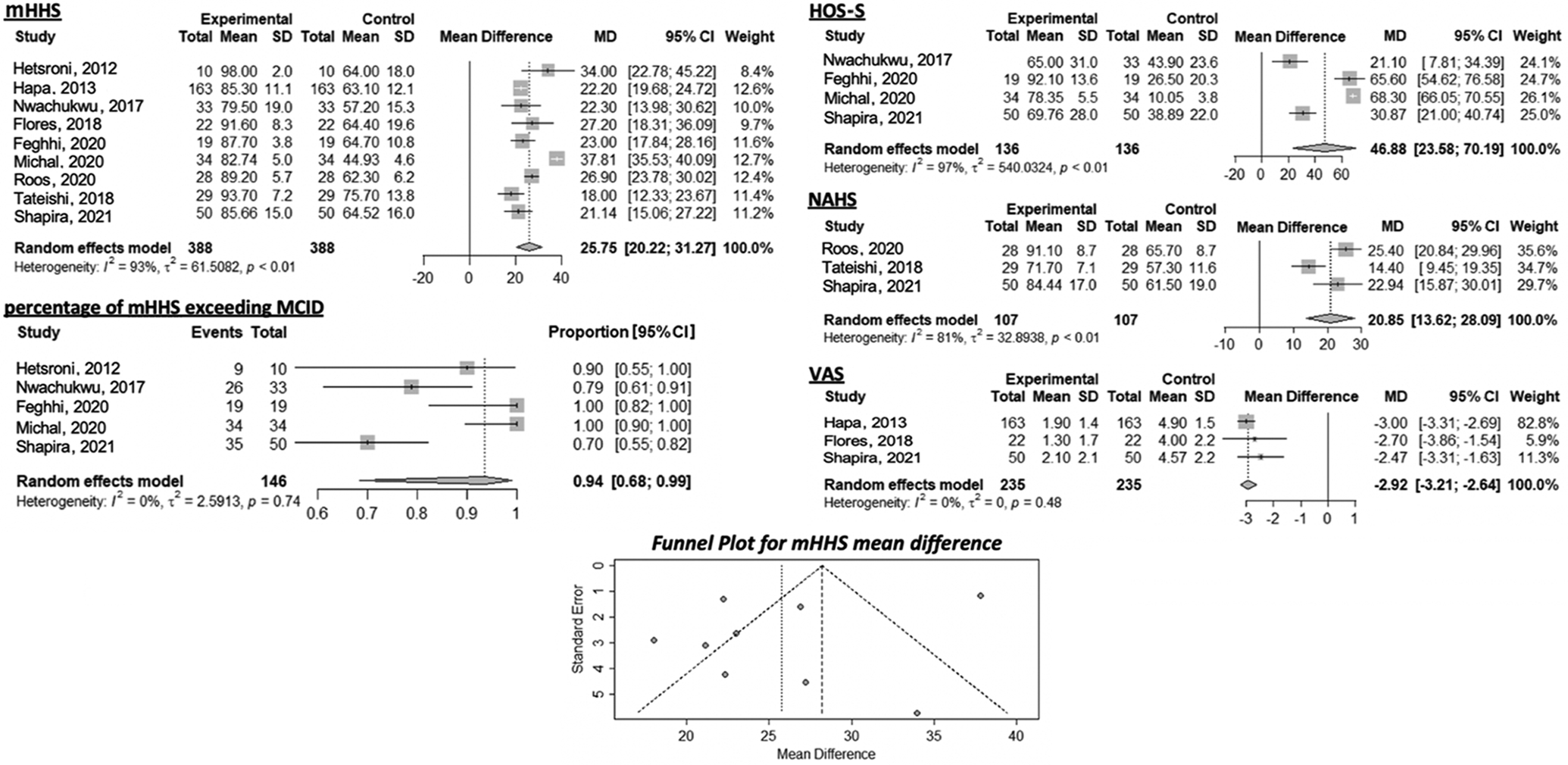
Forest plots of MD between pre- and postoperative improvements in patient-reported outcome scores. The mean differences in mHHS, percentage of mHHS exceeding MCID, HOS-S, NAHS, and VAS were 25.75, 94, 46.88, 20.85, and -2.92, respectively. The I 2 values for heterogeneity were 93%, 0%, 97%, 81%, and 0%, respectively. The funnel plot for patient-reported outcome scores studies revealed an asymmetric property regarding publication bias. HOS-S, Hip Outcome Score–Sport subscale; MCID, minimal clinically important difference; MD, mean difference; mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score; VAS, visual analog scale for pain.
Table 4 summarizes the characteristics of studies on adverse events. The pooled incidences of complications and reoperation were 1% and 2%, respectively (Figure 4).
Summary of Studies on Adverse Events (n = 9) a

a AIIS, anterior inferior iliac spine; FAI, femoroacetabular impingement; NA, not available; SSI subspine impingement; THA, total hip arthroplasty.

Incidence of complications and reoperations after arthroscopic surgery for AIIS impingement. Incidence of complication was 1% and incidence of reoperation was 2%. The I 2 value was 0% for both complications and reoperations, suggesting low heterogeneity. The funnel plots for complications and reoperations revealed asymmetric properties regarding publication bias.
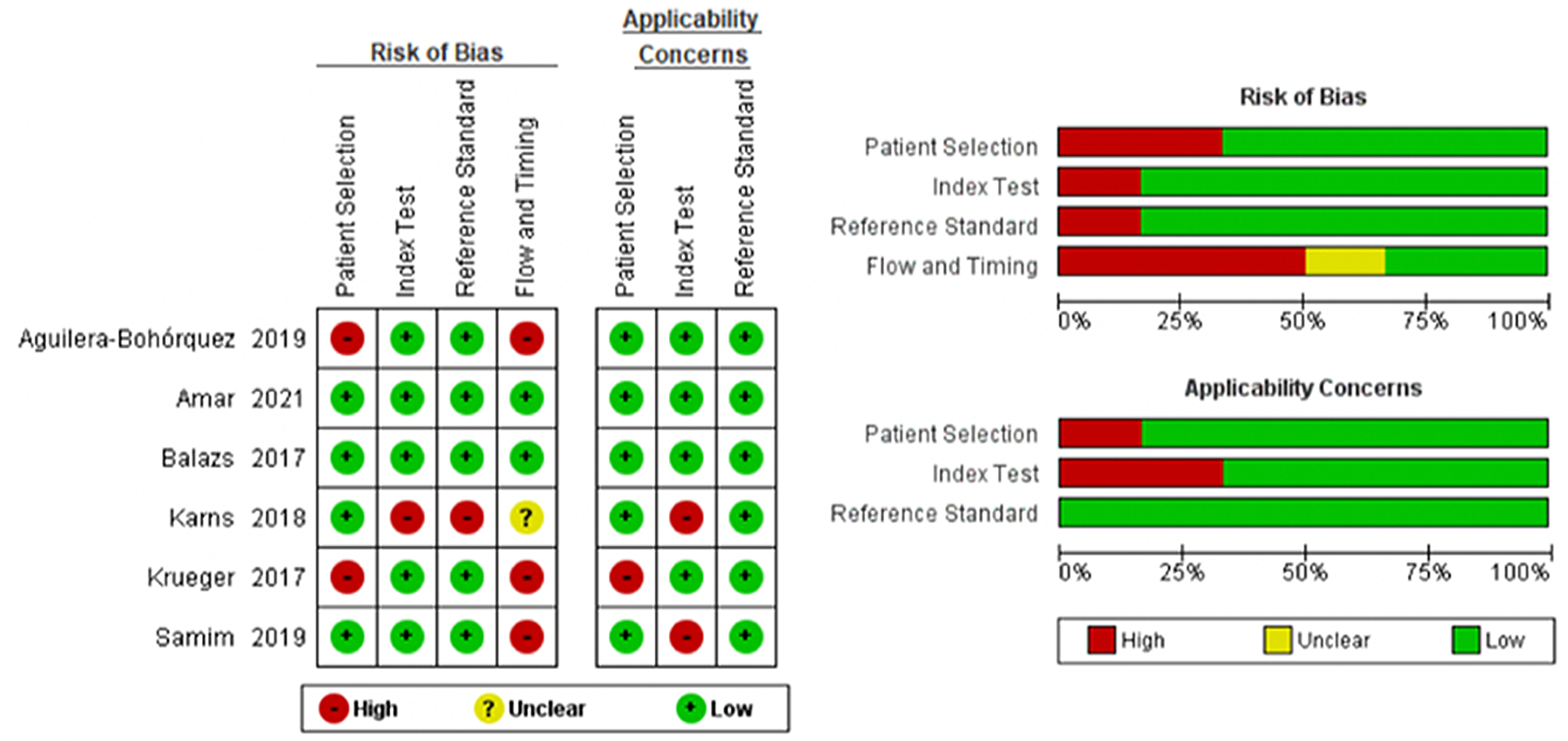
The heterogeneity of the studies depended on the type of assessment. The I 2 value for prevalence showed high heterogeneity; the value for improvement in clinical scores varied from 0% to 97% (no heterogeneity to high heterogeneity), and the I 2 value for complications and reoperation was 0% (no heterogeneity). Figures 5 and 6 show the risk of bias for the studies on diagnostic accuracy and arthroscopic treatment outcomes, respectively. Two of the studies on diagnostic accuracy were identified as having a low risk of bias, while the remaining 4 studies had >2 factors with a high risk of bias (Figure 5). All studies on arthroscopic treatment outcomes had at least 1 factor with a high risk of bias with respect to selection of participants and blinding of outcome assessments (Figure 6).

Risk of bias for the studies on arthroscopic treatment outcomes.
Discussion
This systematic review and meta-analysis revealed that imaging modalities such as plain radiographs, 3D-CT, MRI, and US are useful for diagnosis. The prevalence of AIIS impingement in those that have undergone primary hip arthroscopy is around 18%, and overall clinical outcomes after arthroscopic AIIS decompression are acceptable with improvement of 25.75 for mHHS, 94% for mHHS exceeding MCID, 46.88 for HOS-S, 20.85 for NAHS, and -2.92 for pain VAS, and with an overall complication rate of about 1%.
AIIS impingement is an extra-articular pathology that is occasionally latent under FAI conditions. While clinical recognition of AIIS impingement has increased gradually, 7 evidence in the literature is still limited. Regarding image-based diagnosis of AIIS impingement, we found no single gold standard imaging modality. Plain radiographic imaging is a basic tool for identifying AIIS. 22 Although morphological classification of AIIS based on CT images is established, 16 actual impingement between the AIIS and the femur during motion cannot be visualized on a static image. Therefore, Hetsroni et al 16 conducted computer simulation analyses to show that range of motion (ROM) was limited significantly in cases with prominent AIIS morphology (type 2 or 3). Thus, kinematic computer simulation analysis is a powerful tool for evaluating ROM and identifying the location of AIIS impingement. 2,21 MRI also has potential for diagnosing AIIS impingement. Indeed, Samim et al 35 showed that soft tissue injuries and osseous findings, such as distal cam, on MRI scans that were not morphologic features of the AIIS are associated with subspine impingement. Finally, US is useful for evaluating AIIS morphology. 4 The overall accuracy of US compared with the false-profile view is 92.3%. 4 Thus, imaging diagnosis of AIIS impingement basically relies on morphological evaluation of plain radiographs and CT, with MRI and US as additional diagnostic modalities.
The prevalence of AIIS impingement is an important clinical issue. It is difficult to discuss prevalence because there are no standardized diagnostic criteria for AIIS impingement. In addition, a high percentage of patients with an AIIS morphology associated with subspine impingement are asymptomatic. 6 To make a reliable estimate of prevalence, large-scale epidemiological surveys are required. Based on the limited evidence available, we found that the overall incidence of AIIS impingement in patients who underwent primary hip arthroscopy was approximately 18%; also, subanalyses revealed a difference in incidence between high-kicking athletes and nonathletes. For instance, the prevalence was higher in activities involving high-kicking, such as dancing and soccer. 25,27 Thus, special attention needs to be given to the possibility of AIIS impingement in individuals undertaking such sporting activities. In addition, we found a higher prevalence of AIIS impingement in revised hip arthroscopy cases than in primary hip arthroscopy cases. This suggests (indirectly) the potential persistence of AIIS impingement after primary arthroscopy. Cam or pincer resection may improve ROM 11 ; however, subsequent AIIS impingement may ensue. 21 Nevertheless, it should be noted that all results reported here are valid only for patients undergoing hip arthroscopy, not for the general population. Recent anatomic data based on 1797 cadaveric specimens reported that AIIS dysmorphism was present in 6.4%. 20 This is lower than the current rate for patients undergoing hip arthroscopy.
Regarding clinical outcomes of arthroscopic surgery for AIIS impingement, we extracted 9 studies with standardized clinical assessment protocols. These studies reported favorable improvements with limited complications, including 2 cases with heterotopic ossification, 1 case with insertion tendinopathy of direct head of rectus femoris, 1 case with a small vaginal skin lesion, 1 case with irritation of the hip flexor. However, most of these had a short follow-up period of 1 to 2 years. A case series by Hetsroni et al 15 was the first to report arthroscopic decompression for AIIS impingement. A recent study that compared AIIS impingement with borderline hip dysplasia and nondysplastic FAIS revealed that arthroscopic AIIS decompression is a safe and effective treatment. 10 A clinical issue is the decision regarding the area of decompression within the AIIS lesion. In this regard, an important cadaveric study was conducted by Hapa et al. 14 They showed that the direct head of the rectus tendon has a broad insertion on the AIIS; however, the area devoid of tendon provides a “safe zone” for subspine decompression in cases of symptomatic AIIS impingement. This is important to ensure safe AIIS decompression, particularly in terms of retaining muscle strength after surgery. Indeed, Tateishi et al 38 reported that AIIS decompression did not compromise knee extensor or hip flexor strength postoperatively. In addition, the pooled incidence of surgical complications was 1%, which is almost the same as the overall complication rate after hip arthroscopy for FAIS in adolescents, 29 and slightly lower than the pooled rate of all complications (4%) in adults. 1
Limitations
There are several limitations to this study. The heterogeneity in the assessment of prevalence (see Figure 2) was very high in all subgroups. We identified a relatively high risk of bias, particularly with respect to selection of participants and blinding of assessments of arthroscopic treatment outcomes. In addition, there was a relatively high risk of bias regarding the flow and timing of diagnosis. Furthermore, we must note the possibility of publication bias because there was asymmetry in funnel plot for each outcome. Particularly adverse events may be underestimated or unreported. Thus, further studies with a lower risk of bias are needed to better assess clinical outcomes and diagnostic accuracy.
Conclusion
Study findings indicated that several imaging modalities assist diagnosis of AIIS impingement. The overall prevalence of AIIS impingement in the primary hip arthroscopy population is approximately 18%, with higher prevalence in those participating in high-kicking sports activities. Clinical outcomes after arthroscopic AIIS decompression are generally favorable with a relatively low rate of surgical complications.
Footnotes
Notes
Final revision submitted June 9, 2022; accepted August 7, 2022.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
APPENDIX
Search Strategies
| The Cochrane Library |
|---|
| 1) extra-articular impingement: ti, ab, kw |
| 2) anterior inferior iliac spine: ti, ab, kw |
| 3) subspine impingement: ti, ab, kw |
| 4) aiis: ti, ab, kw |
| 5) 1 OR 2 OR 3 OR 4 |
| PubMed |
| 1) “extra-articular impingement”[All Fields] |
| 2) “subspine impingement”[All Fields] |
| 3) “aiis”[All Fields] |
| 4) “anterior inferior iliac spine”[All Fields] |
| 5) “extra-articular impingement”[All Fields] OR “subspine impingement”[All Fields] OR “aiis”[All Fields] OR “anterior inferior iliac spine”[All Fields] |
| EBSCO CINAHL Plus |
| S1) extra-articular impingement |
| S2) subspine impingement |
| S3) aiis |
| S4) anterior inferior iliac spine |
| S5) S1 OR S2 OR S3 OR S4 |