
Abstract
Background:
On a questionnaire administered to athletes who had undergone anterior cruciate ligament reconstruction (ACLR), some answered “yes” to a question regarding return to sports (RTS) at the preinjury level despite having lower postoperative subjective athletic performance (PoSAP) intensity compared with preoperative levels.
Purpose:
To investigate the agreement between responses regarding RTS and PoSAP intensity after ACLR.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
A total of 44 individuals, 24.8 ± 18.4 months after ACLR, participated in this study. They completed a questionnaire in which PoSAP was graded as a percentage of preoperative performance level. They also gave dichotomous responses (yes/no) to the question of whether they had been able to RTS at the same level as before their injury (RTS question). Participants were divided into 2 groups according to their PoSAP scores using different cutoff values (100%, 90%, 80%, and 70%), and an exploratory analysis was conducted of the cutoff value for dividing PoSAP scores that provided the greatest agreement with the response to the RTS question.
Results:
The mean PoSAP score was 87.5% ± 14.9%, and 33 participants (75%) answered “yes” to the RTS question. The agreement between the PoSAP score and the RTS question was lowest when the cutoff value was 100% (κ = 0.294) and highest when the cutoff value was 80% (κ = 0.676) and 90% (κ = 0.632).
Conclusion:
More athletes who had undergone ACLR answered “yes” to the RTS question even when their PoSAP score was around 80%. Asking only for dichotomous responses may result in overestimating the level to which these athletes’ performance has recovered after ACLR.
After anterior cruciate ligament (ACL) injury, athletes often undergo ACL reconstruction (ACLR) to enable their return to sports (RTS) at the same level of competition as before injury. 7 However, many athletes who participate in sports after ACLR do not believe that they can RTS at their preinjury level. In a meta-analysis of athletes who had undergone ACLR, only about 44% reported that they returned to sports at the same level of competition as before ACL injury. 5 The inability of athletes to return to their preinjury performance level is a major loss to their team or sporting circle. It is thus important for athletes who have undergone ACLR to evaluate the status of their subjective RTS compared with before they were injured and to confirm this transition.
After receiving permission to take part in sports after ACLR, athletes do not immediately play full games at their preinjury competition level. It is recommended that they first take part in a series of partial games at a comparatively lower performance level, gradually increasing both the level and the duration of the games. 1,6 Questionnaires are generally used to assess subjective RTS in athletes after reconstructive surgery. 9 The most frequently used method is to ask for a dichotomous (yes/no) response to the question “Have you returned to the same level of competition as before your ACL injury?” 3,4,13 –15 A negative response indicates physical and/or psychological problems. 3,4,13 –15
Representative subjective outcome scores for athletes after ACLR are the Lysholm score, International Knee Documentation Committee score, and Single Assessment Numeric Evaluation (SANE) score (Table 1). 11,20,21 These outcomes improve gradually over time, even more than 6 months after athletes have been permitted to RTS. 20,21 Both the SANE and the Lysholm scores use continuous variables, making it easier to assess subjective functional improvement and to conduct statistical analyses after ACLR. 20
Representative Subjective Outcome Scores for Athletes After Anterior Cruciate Ligament Reconstruction a

a IKDC, International Knee Documentation Committee; PoSAP, postoperative subjective athletic performance; RTS, return to sports; SANE, Single Assessment Numeric Evaluation.
In our experience, asking only for dichotomous responses is insufficient to assess whether individuals are achieving athletic performance at the same level of competition as before injury. However, no previous study has addressed the gap between the evaluation of subjective RTS using dichotomous responses and the level of subjective athletic performance. The purpose of this study was therefore to clarify the relationship between the state of subjective RTS and subjective athletic performance in athletes after ACLR. We hypothesized that subjective athletic performance is lower than before injury, even when athletes answer “yes” to the RTS question.
Methods
Participants
We devised a questionnaire asking athletes taking part in sports after ACLR to rate their present level of athletic performance as a percentage of their preinjury subjective athletic performance. Patients who had undergone primary ACLR between April 2012 and May 2018 and who participated in sports were included in this study if they met the following inclusion criteria: age 16 to 45 years at the time of questionnaire administration; participation in sports with a modified Tegner activity scale 12 score of >5 before injury; and ≥8 months of follow-up after surgery. Participants were excluded if they had not participated in sports for social reasons such as pregnancy or employment; had ACL injury to the contralateral knee or ACL reinjury to the reconstructed knee; had a history of meniscal injury and surgery of the ipsilateral knee and the contralateral knee before ACL injury; had a cartilage injury requiring surgery; had difficulty in follow-up until RTS; or had a complication that would interfere with their RTS after surgery.
Ethical approval was obtained for this study, and all participants provided written informed consent before participation.
Surgical Technique and Postoperative Rehabilitation
All surgeries were performed by orthopaedic surgeons specializing in the knee joint. The autograft sources were bone–patellar tendon–bone or semitendinosus. If semitendinosus was used for the graft source, double-bundle reconstruction was performed in all patients. The gracilis tendon was not used as an autograft source in the present study. The postoperative rehabilitation protocol was the same for all patients. However, patients who underwent repair of the middle-posterior segment of the meniscus were prohibited from deep squatting to bend the knee more than 90° until 3 months after surgery.
Range of motion and muscle contraction exercises were started 3 days after surgery. A straight-position knee-joint immobilizer (Alcare Co) and crutches were used and then removed gradually 4 weeks after surgery. Running movement started from jogging 3 months after surgery, and the running speed was gradually increased. Once 80% of full-speed running was achieved, athletic exercises related to previous sports or desired sports activities were started with detailed instructions. Athletic exercises were specific to each patient, depending on the kinds of previously practiced sports as well as the patient’s athletic level. Sports participation was allowed when the following was achieved: at least 7 months after surgery; stroke test 18 1+ or less; >90% running compared with before injury; >90% limb symmetry index of the single-leg hop distance (anterior, lateral, medial); and sufficient strength recovery (ie, >85% limb symmetry index of extension and flexion), measured with a Biodex System 4 Isokinetic Dynamometer at 60 deg/s and 180 deg/s.
Testing Protocol
This was a cross-sectional study. Participants were tested at a clinical follow-up visit. The mean follow-up period was 24.8 ± 18.4 months. Measurement items consisted of the collection of demographic information and responses to the self-reported questionnaire. Data were recorded on standard forms and entered into an electronic file (Microsoft Excel 2016; Microsoft Corp).
Outcome Measures
We created an index called the postoperative subjective athletic performance (PoSAP) based on the SANE, which we used to assess the patient’s subjective knee condition. The SANE is an index for evaluating the current subjective knee condition with a score from 0 to 100 and is used as an evaluation of the subjective outcome after ACLR. 11,20,21 The PoSAP index ranges from 0% to 100% and reflects the athlete’s performance level relative to his or her subjective athletic performance before ACL injury (Appendix). The status of their RTS was assessed by their dichotomous response to the question “Have you returned to the same level of competition as before your injury?” This question was referred to as the RTS question (Appendix).
Statistical Analysis
Descriptive statistics were generated for all variables. To investigate the agreement between the answers on the RTS question (yes/no) and the PoSAP score, the participants were divided into 2 groups for each of 4 different cutoff values for PoSAP scores: 100%, 90%, 80%, and 70% (cutoff 100 = PoSAP 100% vs <100%; cutoff 90 = PoSAP ≥90% vs <90%; cutoff 80 = PoSAP ≥80% vs <80%; and cutoff 70 = PoSAP ≥70% vs <70%). Kappa coefficients were used to conduct an exploratory analysis of the cutoff value for the PoSAP score that provided the greatest agreement with the response to the RTS question. A kappa coefficient of 0.0-2.0 indicates “none,” 0.21-0.39 indicates “minimal,” 0.40-0.59 indicates “weak,” 0.60-0.79 indicates “moderate,” 0.80-0.90 indicates “strong,” and >0.90 indicates “almost perfect” agreement. 16 Data were analyzed using SPSS Version 21.0 (IBM Corp). The a priori α level was .05.
Results
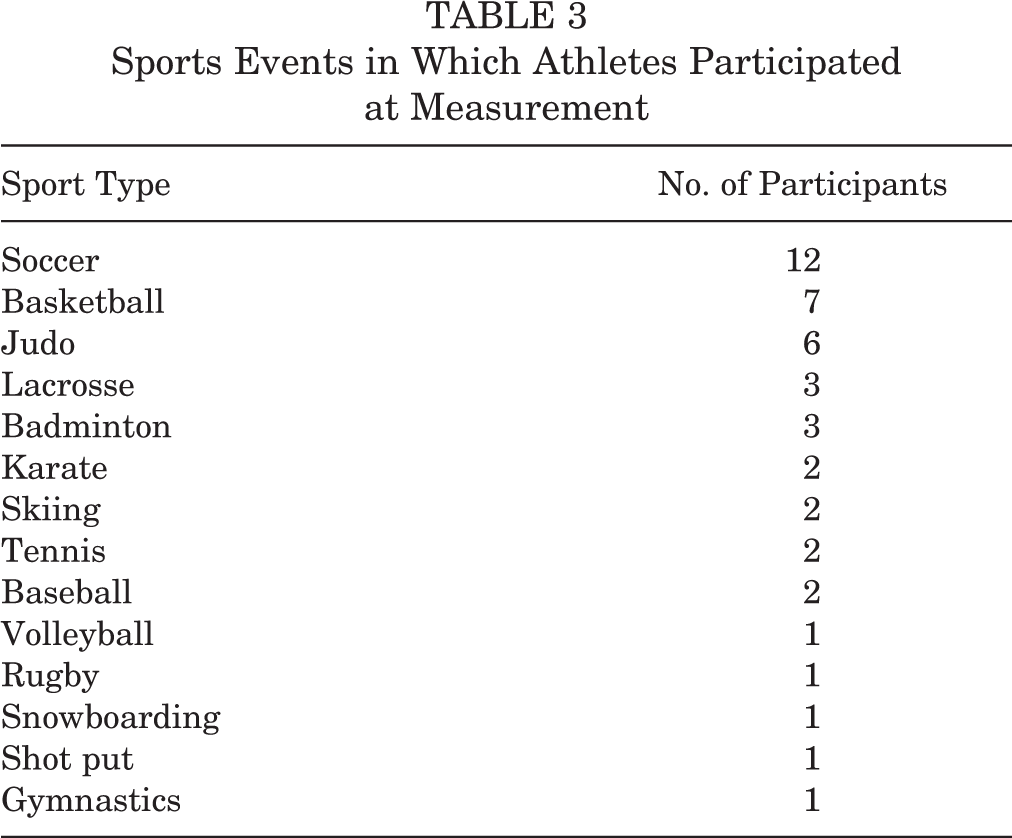
Our study inclusion criteria were met by 48 participants; of these, 4 refused to participate, leaving 44 who were included in this study (Figure 1, Tables 2 and 3). The mean PoSAP score was 87.5% ± 14.9% (Figure 2). A total of 15 respondents (34%), the largest number, had a PoSAP score of 100%, followed by 13 (30%) who had scores between 90% and 99%. Further, 33 (75%) answered “yes” to the RTS question. The kappa coefficients for agreement between the RTS question (yes/no) and the PoSAP score were κ = 0.294 (P = .006, minimal agreement) for cutoff 100%, κ = 0.632 (P < .001, moderate agreement) for cutoff 90%, κ = 0.676 (P < .001, moderate agreement) for cutoff 80%, and κ = 0.533 (P < .001, weak agreement) for cutoff 70% (Table 4). Of the 33 respondents who answered “yes” to the RTS question, 18 (55%) had PoSAP scores less than 100%, and 6 (18%) had PoSAP scores less than 90%. Among them, the reason why the PoSAP score was less than 70% was “The performance is not the same as before injury because of knee pain.” Conversely, of the 11 respondents who answered “no” to the RTS question, 1 respondent (9%) had a PoSAP score above 90%, and investigation of the reason for the negative response elicited the answer “I’m afraid of re-injury, meaning that I can’t say that I’ve returned to sports at the same level as before my injury.”
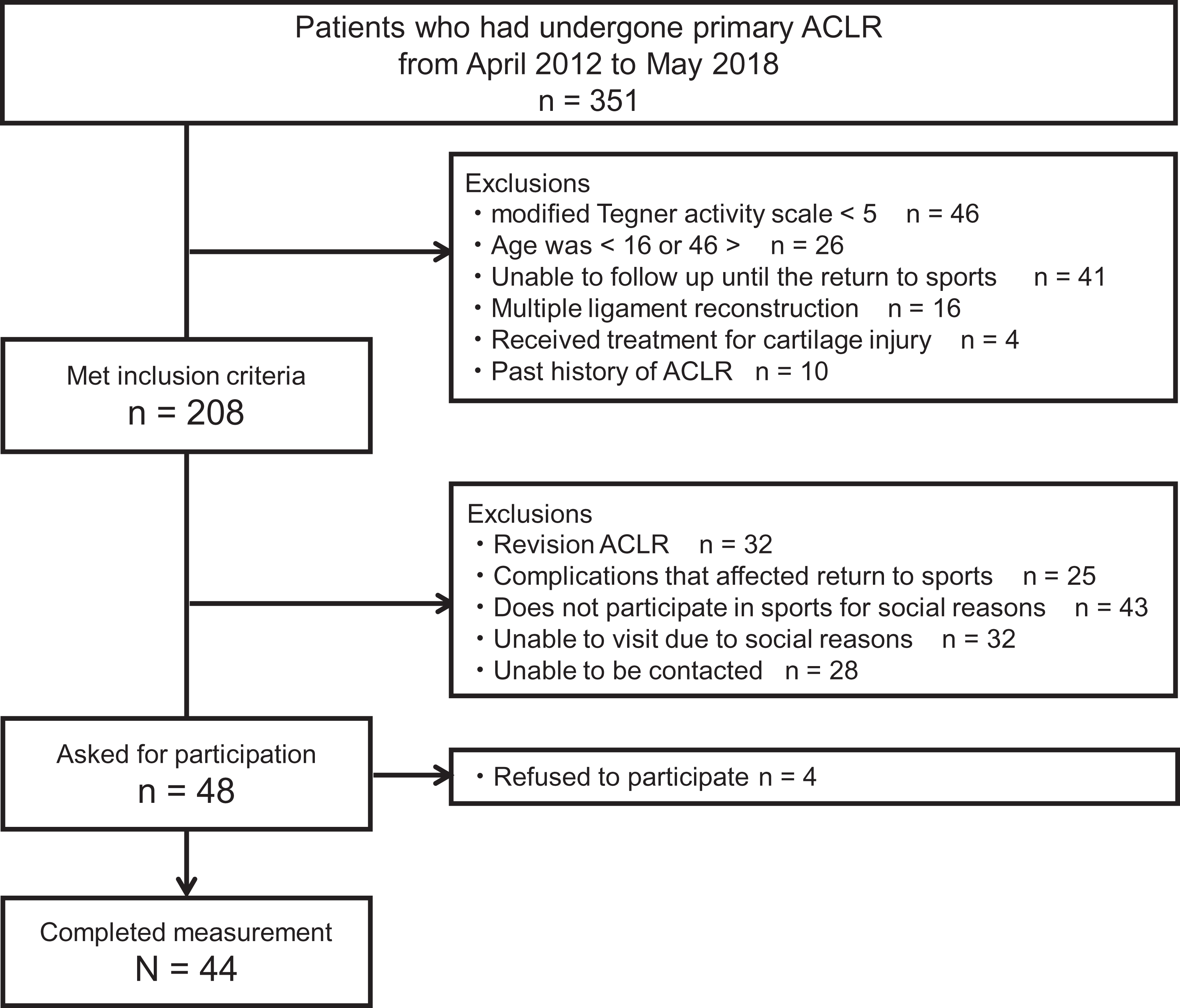
Participant flow chart. ACLR, anterior cruciate ligament reconstruction.
Participants’ Descriptive Data a

a BPTB, bone–patellar tendon–bone; PoSAP, postoperative subjective athletic performance; RTS, return to sports; ST, semitendinosus.
Sports Events in Which Athletes Participated at Measurement

Distribution of postoperative subjective athletic performance scores.
Agreement Between PoSAP and Response to the RTS Question a
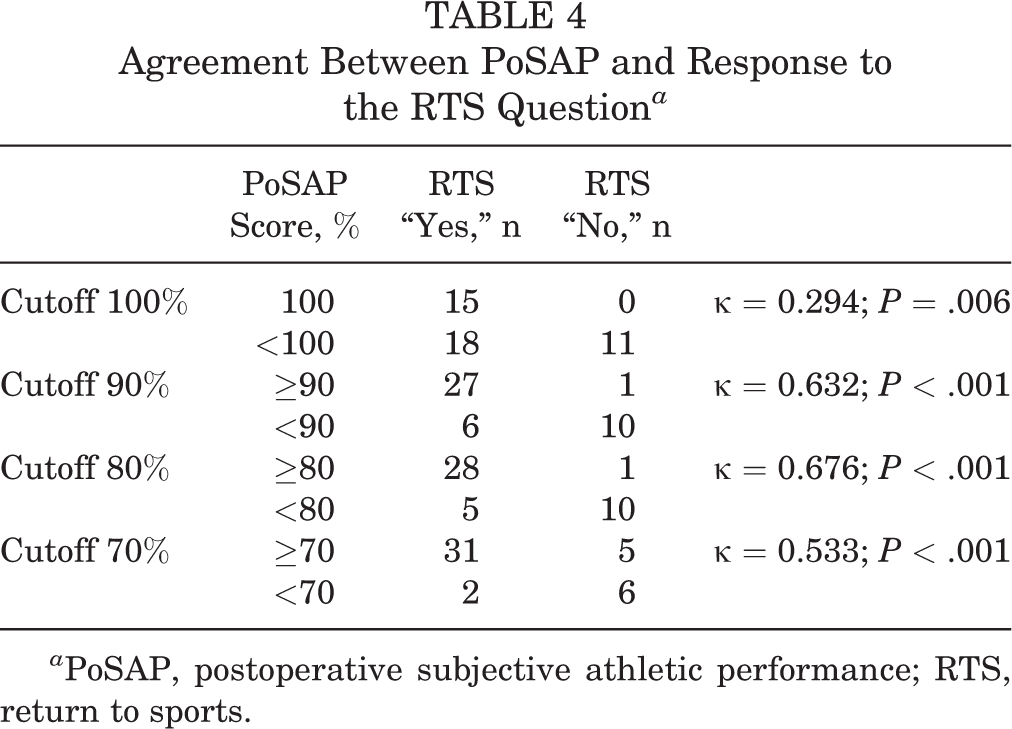
a PoSAP, postoperative subjective athletic performance; RTS, return to sports.
Discussion
In this study of athletes participating in sports after primary unilateral ACLR, the level of agreement between their response regarding RTS and their PoSAP score was investigated. In some cases, athletes who responded “yes” to the RTS question had lower PoSAP scores than before their injury, demonstrating the existence of a gap between these 2 self-reported outcomes. The results of this study supported our hypothesis.
In this study, PoSAP scores were operationally divided into 2 groups using 4 different cutoff values, and an exploratory analysis of the agreement with the answers to the RTS question was conducted. Significant agreement between the 2 outcomes was observed for all cutoff values. However, the agreement between the PoSAP score and the answer to the RTS question was lowest when the cutoff value was 100% (κ = 0.294) and highest when the cutoff value was 80% (κ = 0.676) and 90% (κ = 0.632). For athletes who underwent ACLR with the purpose of returning to sports at their preinjury competition level, the RTS question (yes/no) may have resulted in an overestimation of the recovery level. Next to 80%, the highest level of agreement was when the cutoff value was 90%, with 1 patient accounting for the difference. We consider it important that the PoSAP score was less than 100% even if athletes participating in sports after ACLR answered “yes” to the RTS question. There has been no previous report of a gap between dichotomous responses to the RTS question and self-reported postoperative athletic performance level, and this study has provided new data.
As for the reason for the gap between the 2 outcomes, there may be problems with the measurement scales. Although a nominal scale is widely used to examine the relationships between 2 variables, problems may arise when variables associated with intensity are categorized on a nominal scale. 17 For example, different people will have different understandings of what a “yes” response means, and the interpretation of the question risks giving rise to confusion between participants. 10 “Yes” may well encompass a range of intensities (from “absolutely yes” to “mildly yes”). However, because the use of a nominal scale means that all of these are included, the fewer possible responses to the question, the easier it is for measurement error to occur. 10 For these reasons, it is unreasonable to use dichotomous responses to assess the status of athletes’ subjective RTS, since it may improve over time. This may also have given rise to the gap between answering “yes” to RTP and having a low PoSAP score.
Because the RTS involves not only physical factors but also psychosocial factors, the RTS question can be described as a comprehensive evaluation of these factors. 2,8 However, the PoSAP score used in the present study evaluated only performance in competition. The analysis of these 2 outcomes showed that none of the athletes who rated their PoSAP score as 100% responded “no” to the RTS question. Only 1 patient who rated the PoSAP level as 90% gave this response. Few athletes with high PoSAP scores responded “no” to the RTS question, suggesting that the PoSAP score can be used for the evaluation of the status of their RTS.
As evaluating patients’ self-reported outcomes requires both clinician and patient time and resources, a simple method is desirable to reduce the workload. 20 Because the SANE score, which was used as a reference when creating the PoSAP score, is assessed using a simple question, it has the advantage of ease of use in clinical settings. The SANE has also been used for longitudinal studies because it can be sensitive to changes in knee function levels. 19 –21 If physical and psychosocial factors related to PoSAP levels were to be clarified in the future, it would provide useful information to support RTS after ACLR.
Limitations
This study has several limitations. Because data from all athletes who had returned to sports after ACLR were not measured, inherent selection bias cannot be excluded. However, all athletes in a particular period were enrolled according to the inclusion and exclusion criteria described above to minimize bias as much as possible. The PoSAP score is only an outcome assessed in relation to an athlete’s own preinjury score. Thus, it may vary according to the category and level of sport in which the athlete takes part. This issue should be addressed in future studies. The PoSAP can simply assess performance intensity, but it alone cannot accurately assess the level of competition. The RTS question and the PoSAP may complement each other. For example, there is a method to evaluate RTS by combining the RTS question and the PoSAP, which will be our future research topic. Although the PoSAP was created based on the SANE, whose validity as a measure of functional recovery after ACLR has already been confirmed, 11,20,21 the validity of the PoSAP itself has not been confirmed with another scale. The SANE and the PoSAP are both simple, since they ask 1 question requiring an answer on a scale from 0 to 100, and this does not appear to be a problem that affected this study. Last, no upper limit was set on the time elapsed since surgery. The subjective outcomes for athletes after ACLR show gradual improvement over 2 years after surgery. Therefore, the outcome used in this study may also change over time after surgery. Studies at set periods may also be required in the future.
Conclusion
This study showed a gap in agreement between dichotomous responses regarding RTS and subjective athletic performance intensity after ACLR. It is not sufficient in terms of the characteristics of the scale to evaluate RTS from dichotomous response. The method of asking athletes to rate their present subjective performance level as a percentage of their preinjury performance may be an effective method of evaluating RTS after ACLR.
Footnotes
Final revision submitted March 18, 2020; accepted April 3, 2020.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Tokyo Medical and Dental University (ID No. M2016-197).