
Abstract
Background:
The need for capsular closure during arthroscopic hip labral repair is debated.
Purpose:
To compare pain and functional outcomes in patients undergoing arthroscopic hip labral repair with concomitant repair or plication of the capsule versus no closure.
Study Design:
Cohort study.
Methods:
Outcomes were compared between patients undergoing arthroscopic hip labral repair with concomitant repair or plication of the capsule versus no closure at up to 2 years postoperatively and with stratification by age and sex. Patients with lateral center-edge angle <20°, a history of instability, a history of prior arthroscopic surgery in the ipsilateral hip, or a history of labral debridement only were excluded. Subanalysis was performed between patients undergoing no capsular closure who were propensity score matched 1:1 with patients undergoing repair or plication based on age, sex, and preoperative Modified Harris Hip Score (MHHS). We compared patients who underwent T-capsulotomy with concomitant capsular closure matched 1:5 with patients who underwent an interportal capsulotomy with concomitant capsular repair based on age, sex, and preoperative MHHS.
Results:
Patients undergoing capsular closure (n = 1069), compared with the no-closure group (n = 230), were more often female (68.6% vs 53.0%, respectively; P < .001), were younger (36.4 ± 13.3 vs 47.9 ± 14.7 years; P < .001), and had superior MHHS scores at 2 years postoperatively (85.8 ± 14.5 vs 81.8 ± 18.4, respectively; P = .020). In the matched analysis, no difference was found in outcome measures between patients in the capsular closure group (n = 215) and the no-closure group (n = 215) at any follow-up timepoint. No significant difference was seen between the 2 closure techniques at any follow-up timepoint. Patients with closure of the capsule achieved the minimal clinically important difference (MCID) and the patient acceptable symptom state (PASS) for the 1-year MHHS at a similar rate as those without closure (MCID, 50.3% vs 44.9%, P = .288; PASS, 56.8% vs 51.1%, P = .287, respectively). Patients with T-capsulotomy achieved the MCID and the PASS for the 1-year MHHS at a similar rate compared with those with interportal capsulotomy (MCID, 50.1% vs 44.9%, P = .531; PASS, 65.7% vs 61.2%, P = .518, respectively).
Conclusion:
When sex, age, and preoperative MHHS were controlled, capsular closure and no capsular closure after arthroscopic hip labral repair were associated with similar pain and functional outcomes for patients up to 2 years postoperatively.
The past 20 years have seen a significant increase in the popularity of arthroscopic procedures in lieu of open hip surgery to diagnose and treat pathology.9,19,40,59 Of the hip pathologies that are treated with hip arthroscopy, labral tears are most common. 32 During arthroscopic hip labral repair, capsulotomy is often necessary to obtain an adequate visual field; however, the need for closure of the capsule is debated. 5 Although this topic remains controversial, the incidence of surgeons performing closure or plication of the capsule after arthroscopic hip surgery reportedly increased from 7% between 2009 and 2011 to 58% in 2017. 46
Prior authors have described the superiority of capsular closure for dysplasia in cadaveric studies, arguing that capsular ligament repairs ensure that natural hip stability is maintained.1,37,39,45,49 However, repair or plication of the capsule in patients with low risk of postoperative instability may be deleterious to hip range of motion without improving stability.6,14,18,23 Prior clinical studies have reported mixed findings, possibly related in part to limited historical cohort sizes. The largest clinical study to date assessing the influence of capsular closure during a variety of arthroscopic hip procedures found no differences on multiple patient-reported outcomes between groups after adjustment for age, body mass index, sex, preoperative patient-reported outcomes, and degree of chondral damage. 15 In contrast, a recent cohort study suggested that complete capsular repair after hip arthroscopy for femoroacetabular impingement (FAI) significantly improves specific outcome measures, such as the Hip Outcome Score Sport-Specific subscale (HOS-SS), compared with partial capsular repair up to 2.5 years postoperatively. 21 Furthermore, a small cohort study suggested that capsular plication after arthroscopic hip labral repair in patients with dysplasia should be the standard protocol owing to positive reported outcomes over 5 years; however, this study evaluated only 19 patients. 13 This range of contrasting data makes it difficult to determine the superiority of a given capsular management technique after arthroscopic hip labral repair.
To the best of our knowledge, no prior studies with adequate sample sizes have been conducted to compare pain and functional outcomes of hip arthroscopic labral repair between capsular closure and no-closure groups or to determine whether the type of capsulotomy influences functional outcomes. Therefore, the primary purpose of this study was to compare pain and functional outcomes in patients after undergoing arthroscopic hip labral repair with concomitant repair or plication of the capsule versus no closure. Secondarily, we compared pain and functional outcomes of T-capsulotomy versus interportal capsulotomy in patients after undergoing arthroscopic hip labral repair with capsular closure. We hypothesized that there would be no difference in pain and functional outcomes in patients receiving capsular closure or plication versus no closure.
Methods
Patient Selection
After receiving institutional review board approval for this study, we retrospectively queried the Surgical Outcomes System (Arthrex) global database, which includes patients from approximately 267 centers, for patients who had undergone a primary arthroscopic hip labral repair and concomitant capsular repair or plication versus no closure. Access to the Surgical Outcomes System database was provided by Arthrex (grant No. 01531). We included patients ≥18 years of age who underwent arthroscopic hip labral repair between 2011 and 2022, in order to capture the broad population that receives successful arthroscopic hip labral repairs. 36 Subsequently, we excluded patients with a lateral center-edge angle (LCEA) of <20°, a history of instability, a history of prior arthroscopic surgery in the ipsilateral hip, or a history of labral debridement only. Labral debridement was excluded because labral repair has been shown to be a more effective procedure for labral tears and to maintain procedural homogeneity between capsular management groups. 55 Patients with a previous diagnosis of instability and LCEA <20° were excluded in order to maintain a homogeneous population between capsular management techniques and so that the results would be applicable to patients without comorbidities. Patients were included if they had a minimum of 2 years of follow-up, with scores from at least one of the study outcome measures collected at the 2-year follow-up.
Outcome Measures
Functional outcomes were assessed with the Modified Harris Hip Score (MHHS), the Single Assessment Numeric Evaluation (SANE), a 10-point visual analog scale (VAS) for pain, and the Veterans RAND 12-Item Health Survey (VR-12) and Mental Component Summary. The MHHS comprises assessments of functional activities, pain, and gait in equal parts, with the highest score of 91 indicating proficiency in all parts. 24 All outcome measures were collected preoperatively and postoperatively at the 2-week, 3-month, 6-month, 1-year, and 2-year follow-up points; the VR-12 was not assessed at the 2-week and 3-month follow-up but was evaluated at all other timepoints.
Handling of Missing Data
To avoid the selection bias introduced by complete case analysis 42 and missing functional and pain score data, we used multiple imputation by predictive mean matching to impute data for variables with missing values. Multiple imputation uses existing data to reproduce conclusions that would have been present in a complete dataset and is increasingly used in the shoulder surgery literature.28,50,51 We set the number of imputed datasets (M) to 30 because the rate of missing data in all variables was <30%. 54 Estimates of standard errors among these datasets were calculated using Rubin's rules. 47 Multiple imputation was performed using the mice package in R software (version 4.2.0; R Core Team). 52
Statistical Analysis
We performed a power analysis a priori to determine the minimum sample size necessary to detect a difference equivalent to the minimal clinically important difference (MCID) in the MHHS as reported by Bodendorfer et al 8 using their reported MCID and standard deviation (12.2 and 14.8, respectively) for the MHHS in patients undergoing arthroscopic hip labral repair with minimum 2-year outcomes. We found the necessary sample size to attain 90% power to be 114 with a 1:5 allocation and 64 with a 1:1 allocation. Power analyses were performed in G*Power (version 3.1.9.6) with an α = .05.
We first compared pain and functional scores at all timepoints between patients undergoing arthroscopic hip labral repair with repair or plication of the capsule versus no closure. This analysis was also stratified by age (<30, 30-45, >45 years) and sex. Pain and functional outcomes were compared using the Welch 2-sided unpaired t test. Count variables were compared using the Fisher exact test. Next, we matched patients undergoing no closure of the capsule 1:1 with patients undergoing repair or plication. Matching was performed based on age (matched pairs within 5 years), sex, and preoperative MHHS (matched pairs within 5 points) using the MatchIt package. 25 Fifteen patients in the no-closure group could not be matched to the repair or plication group because of sex and preoperative MHHS. Toward our secondary aim, we matched patients undergoing arthroscopic hip labral repair with concomitant T-capsulotomy and capsular repair 1:5 with those undergoing interportal capsulotomy and capsular repair based on age (within 5 years), sex, and preoperative MHHS (within 5 points). Pain and functional outcomes were compared between matched cohorts using the Welch 2-sided paired t test. We further assessed clinically important differences between matched cohorts by comparing the proportion of patients who achieved the MCID as well as those who achieved the patient acceptable symptom state (PASS) in the 1-year postoperative MHHS as reported previously for arthroscopic hip surgery for FAI. 10 Count variables were compared using the Fisher exact test. All statistical analyses were performed using R software (version 4.2.0; R Core Team) with an α of .05.
Results
A flowchart of the patient inclusion process is shown in Figure 1. We initially included 3422 patients aged ≥18 years who underwent arthroscopic hip labral repair between 2011 and 2022. Subsequently, we excluded patients for LCEA <20° (n = 13), a history of instability (n = 128), or missing data regarding capsular management (n = 1945). Of the remaining 1336 patients, we excluded patients with a history of prior arthroscopic surgery in the ipsilateral hip (n = 37). We included a total of 1299 patients without prior capsular intervention who underwent repair or plication of the capsule (n = 1069) or no closure (n = 230). We conducted a comparison of pain and functional outcomes in patients undergoing arthroscopic hip labral repair with concomitant T-capsulotomy (n = 48) and repair who were matched 1:5 with patients undergoing interportal capsulotomy (n = 240) and repair based on age, sex, and preoperative MHHS.
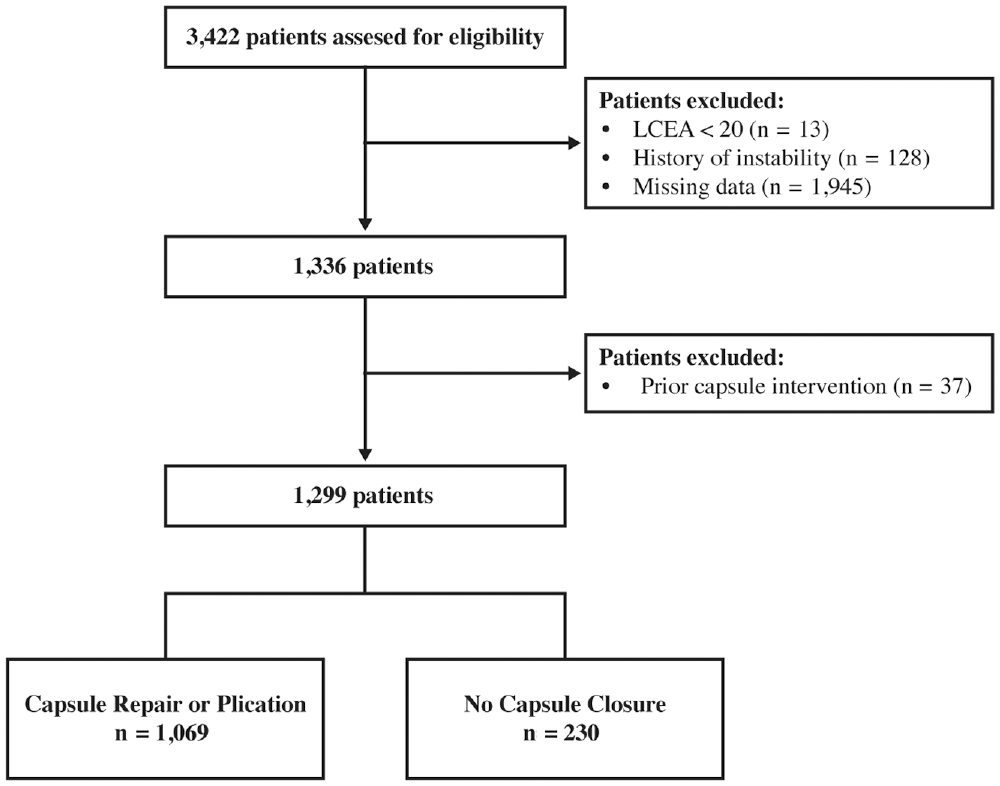
Flowchart of patient inclusion. LCEA, lateral center-edge angle.
Patients who underwent repair or plication were younger than patients who had no capsular closure (36.4 ± 13.3 vs 47.9 ± 14.7 years, respectively; P < .001) and were more likely to be female (68.6% vs 53.0%; P < .001) (Table 1). Patients who underwent repair or plication had a higher preoperative MHHS than patients without capsular closure (64.0 ± 16.5 vs 58.6 ± 17.7, respectively; P < .001) and higher VR-12 Physical score (36.0 ± 9.1 vs 33.4 ± 9.2; P = .002). Closure or plication of the hip capsule, compared with no closure, was associated with superior MHHS functional outcomes at 3 months (80.6 ± 15.5 vs 77.4 ± 17.1, respectively; P = .025), 6 months (83.7 ± 15.3 vs 78.3 ± 17.8; P < .001), 1 year (83.1 ± 15.3 vs 78.4 ± 17.9; P = .001), and 2 years (85.8 ± 14.5 vs 81.8 ± 18.4; P = .020). The VR-12 Physical scores followed the same trend, but no reported VR-12 Physical scores were available at month 3 (Table 1). There were no group differences in VAS pain scores at any follow-up timepoint.
Comparison of Pain and Functional Outcomes in Patients Undergoing Arthroscopic Hip Labral Repair With Concomitant Repair or Plication of the Capsule Versus No Closure a
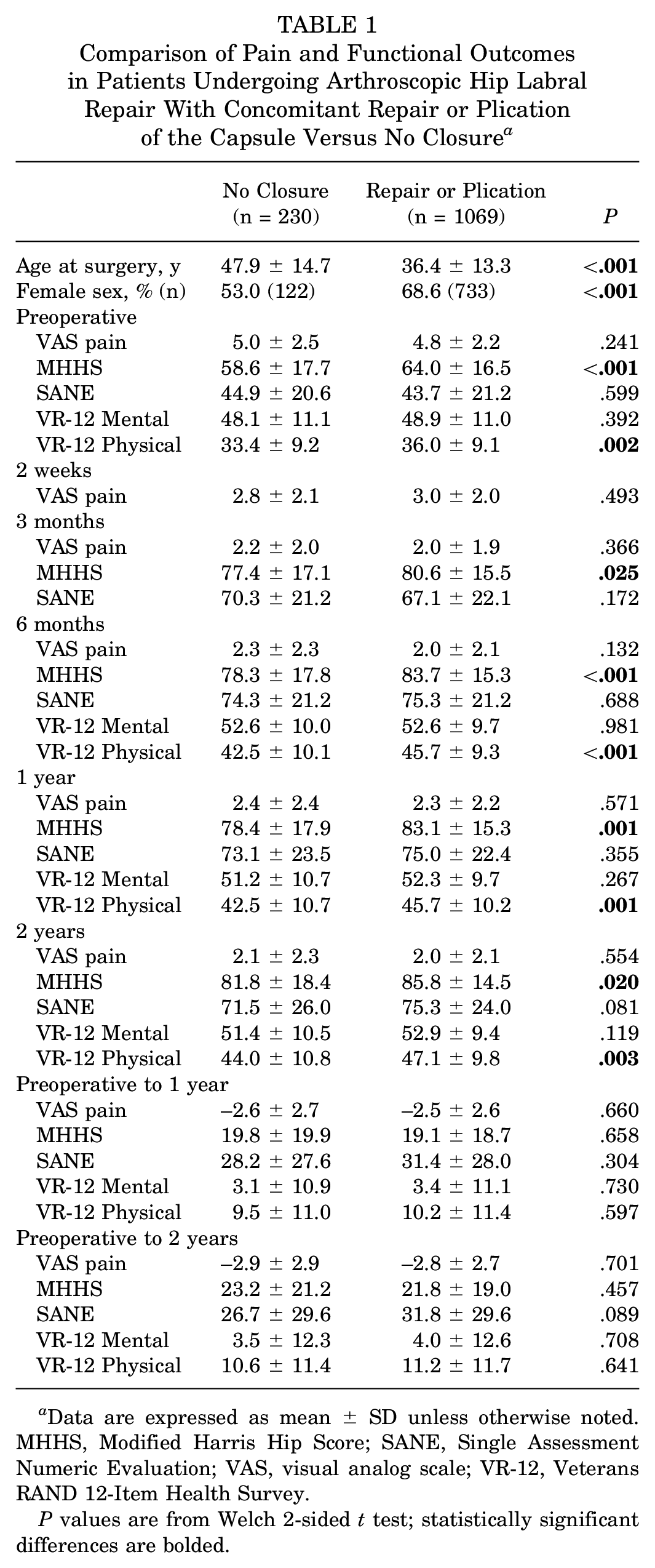
Data are expressed as mean ± SD unless otherwise noted. MHHS, Modified Harris Hip Score; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale; VR-12, Veterans RAND 12-Item Health Survey.
P values are from Welch 2-sided t test; statistically significant differences are bolded.
When pain and functional outcomes were stratified by age and sex, no differences were seen at any follow-up timepoint for men in any age grouping (Supplemental Table S1, available separately) and for women <30 years and 30 to 45 years of age (Supplemental Table S2). Women between 30 and 45 years who received capsular repair or plication had significantly higher preoperative MHHS compared with those in the no-closure group (63.1 ± 15.9 vs 56.6 ± 14.8, respectively; P = .022). Women between 30 and 45 years who received capsular repair or plication reported no difference in pain and functional scores compared with the no-closure group at any follow-up time. A similar preoperative trend for significantly higher MHHS and VR-12 Physical score was reported for women >45 years with capsular repair compared with those who did not undergo capsular closure (MHHS, 60.5 ± 16.3 vs 53.5 ± 17.1, P = .009; VR-12 Physical, 34.2 ± 8.7 vs 29.9 ± 8.2, P < .002, respectively). The reported MHHS for women aged >45 years with capsular repair, compared with women of the same age without capsular repair, was significantly improved at 3 months (76.9 ± 16.9 vs 70.8 ± 18.4, respectively; P = .034), 6 months (80.0 ± 16.5 vs 71.5 ± 18.7; P = .004), and 1 year (80.7 ± 15.9 vs 72.4 ± 18.5; P = .005). No group difference in MHHS was seen for women >45 years at the 2-year follow-up, and no difference in VAS pain scores was seen between groups for women in any age group.
When comparing capsular closure versus no closure matched by patient age, sex, and preoperative MHHS, we found no difference in pain and functional scores at any follow-up timepoint (Table 2). Patients with closure of the capsule achieved the MCID in the 1-year MHHS at a similar rate as those without closure (50.3% vs 44.9%, respectively; P = .288). Likewise, patients with closure of the capsule achieved the PASS in the 1-year MHHS at a similar rate as those without closure (56.8% vs 51.1%, respectively; P = .287).
Comparison of Pain and Functional Outcomes in Patients Undergoing Arthroscopic Hip Labral Repair With Concomitant Repair or Plication of the Capsule Matched 1:1 With No Closure a

Data are expressed as mean ± SD unless otherwise noted. Matching was based on age (within 5 years), sex, and preoperative MHHS (within 5 points). MHHS, Modified Harris Hip Score; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale; VR-12, Veterans RAND 12-Item Health Survey.
P values are from Welch 2-sided unpaired t test; no statistically significant differences were found.
When comparing patients who underwent interportal capsulotomy with capsular closure versus T-capsulotomy and capsular closure matched according to age, sex, and preoperative MHHS, we found no differences in pain and functional outcomes at any follow-up timepoint (Table 3). Patients with T-capsulotomy achieved the MCID in the 1-year MHHS at a similar rate as those with interportal capsulotomy (50.1% vs 44.9%, respectively; P = .531). Likewise, patients with T-capsulotomy achieved the PASS in the 1-year MHHS at a similar rate as those with interportal capsulotomy (65.7% vs 61.2%, respectively; P = .518).
Comparison of Pain and Functional Outcomes in Patients Undergoing Arthroscopic Hip Labral Repair With Concomitant T-Capsulotomy and Repair Matched 1:5 With Interportal Capsulotomy and Repair a

Data are expressed as mean ± SD unless otherwise noted. Matching was based on age (within 5 years), sex, and preoperative MHHS (within 5 points). MHHS, Modified Harris Hip Score; SANE, Single Assessment Numeric Evaluation; VAS, Visual Analog Scale; VR-12, Veterans RAND 12-Item Health Survey.
P values are from Welch 2-sided unpaired t test; no statistically significant differences were found.
Discussion
The current study compared pain and functional outcomes between patients who underwent arthroscopic hip labral repair with concomitant capsular repair or plication versus no closure. This study is the largest retrospective study to date, reviewing a total of 1299 patients. Before matching, we found that patients undergoing capsular repair or plication had superior preoperative and postoperative MHHS and VR-12 Physical scores, with no differences between groups when pre- to postoperative improvements were compared (Table 1). However, capsular repair or plication was performed more frequently in younger and female patients. After accounting for age, sex, and preoperative MHHS, we found no difference in any pain and functional outcomes at any timepoint when comparing capsular repair or plication versus no closure (Table 2) or when comparing patients with capsular closure performed after T-capsulotomy versus interportal capsulotomy (Table 3). Additionally, patients with capsular closure achieved the MCID and the PASS for the 1-year MHHS at a similar rate compared with those without closure.
Biomechanical studies support the correlation between hip capsular management and stability of the hip joint postoperatively and suggest closure of the capsule to preserve stability.3,4,6,29,39 Some studies demonstrated that preservation of the iliofemoral ligament was critical to maintain native external rotation and anterior translation of the head of the femur, an important mechanism in protecting the hip from dislocating.3,30,31,39 Other studies that evaluated the kinematics and torsional load of the hip joint concluded that the capsule should be routinely repaired in any hip procedure for patients with a predisposition to hip microinstability.11,27,30,56 Additionally, cadaveric studies investigating all chondral and ligamentous elements of the hip joint have determined that the iliofemoral ligament is not the only structure maintaining hip capsular placement; the labrum of the hip contributes to maintaining the external rotation and anterior translation of the femur, and the zona orbicularis provides stability to the head of the femur.26,39
Clinical studies have produced conflicting results. Domb et al 15 conducted a study investigating the difference in capsular repair versus no repair in patients who underwent hip arthroscopic procedures at a single institution for an array of indications including labral tears, FAI, and chondral damage. When adjusting for age, sex, body mass index, and preoperative patient-reported outcomes, the authors found no significant differences in patient-reported outcomes for capsular repair versus no closure. Additionally, a prospective cohort study conducted by Filan et al 20 found no difference in pain and functional outcomes and revision rate at 2 years postoperatively between capsular repair (n = 458) and no repair (n = 508) after arthroscopic hip surgery for FAI. Their study included only patients <45 years of age and did not control for differences in preoperative patient-reported outcomes or sex match between the 2 groups, potentially missing a large patient population. Lin et al 34 conducted a systematic review of studies comparing capsular closure and no repair after hip arthroscopy surgery and reported no significant difference in MHHS, HOS-SS, and Hip Outcome Score–Activities of Daily Living subscale (HOS-ADL) between arthroscopic hip surgery with capsular repair versus no closure. This study also reported no significant difference in risk ratio of revision rate for the 2 groups (risk ratio, 0.66; P = .21). In a systematic review, Harris et al 23 reported that the disadvantages of capsular repair included increased surgical time, postoperative stiffness, and capsular adhesions, possibly leading to poorer range of motion and overall patient satisfaction. Our study supports these findings and the notion that whether the capsule is repaired does not influence clinical outcomes of arthroscopic hip labral repair. Furthermore, our study demonstrates that the lack of a difference between repair and no closure of the capsule reported by prior studies is less likely due to underpowering.
Advantages of repair of the hip capsule after arthroscopic hip surgery include greater stability and prevention of an iatrogenic dysplasia-like configuration with potential subluxation and further chondral damage.14,23,39 Clinical benefits have been demonstrated by some. Frank et al 21 conducted a retrospective cohort study that evaluated the differences in outcomes after partial closure (n = 32) versus complete closure (n = 32) of the capsule after primary hip arthroscopy for FAI. At 2.5-year follow-up, Frank et al noted significantly improved HOS-SS scores after complete capsular repair after hip arthroscopy for FAI compared with partial capsular repair (87.3 ± 8.3 vs 83.6 ± 9.6, respectively; P = .001). Economopoulos et al 17 conducted a prospective, randomized controlled trial comparing interportal capsulotomy without closure (n = 45), T-capsulotomy without closure (n = 40), and interportal capsulotomy with closure (n = 46). At 2 years postoperatively, the MHHS was significantly greater after interportal capsulotomy with complete closure (86.2 ± 14.5) compared with interportal capsulotomy without closure (81.7 ± 17.8) or open T-capsulotomy without closure (76.0 ± 20.1) (P < .001 for all). 17 However, the rates of revision surgery and conversion to total hip arthroplasty were similar between groups. That study included much stricter inclusion criteria than we used in the present study and was conducted at a single institution, which suggests that a different patient population was sampled and therefore could explain the difference in outcomes compared with our study. After conducting a systematic review and meta-analysis of 36 studies, Looney et al 35 reported significantly superior improvements in MHHS (coefficient, 2.011 ± 1.457; P = .007), HOS-ADL (coefficient, 3.635 ± 1.712; SE = 0.873; P < .001), and HOS-SS (coefficient, 4.137 ± 2.362; P < .001) postoperatively in patients who underwent arthroscopic hip surgery with concomitant capsular repair compared with patients who did not have capsular repair. The analysis, however, included a majority of studies that indicated hip arthroscopic surgery for FAI, dysplasia, or borderline dysplasia and did not control for patients with multiple comorbidities or inclusion criteria of primary hip arthroscopy.
Case reports of hip dislocation after arthroscopic hip labral repair and FAI correction with or without capsular plication or repair have been published. 43 Hip instability was shown to occur in patients with LCEA <20° and generalized ligament laxity who received a labral repair with an unrepaired capsulotomy.2,7,38 We believe that outcomes in those cases represent a small percentage of the actual outcomes of patients undergoing hip arthroscopy, and it is difficult to draw conclusions based on the small cohort being reported. Gupta et al 22 reported that most high-volume hip arthroscopy surgeons (78%) consider radiographic findings, instability risk factors, and a patient's social history when determining whether to repair the capsule. Although the association between capsular repair and the risk of dislocation would ideally be evaluated in a randomized controlled trial, the low incidence of this outcome may be prohibitive; a rigorously designed case-control study of a large cohort may be adequate to address this question.
Numerous studies have evaluated clinical, radiographic, and arthroscopic findings that should be indications for capsular repair during arthroscopic hip surgery. 14 Evidence suggests that capsular repair is indicated for revision hip arthroscopy for acetabular dysplasia in patients with symptomatic instability after primary hip arthroscopy surgery.41,57 Additionally, patients with borderline dysplasia who have undergone hip arthroscopy for FAI or labral preservation with concomitant capsular repair have reported minimal revision rates and improved stability.16,33 Saadat et al 48 reported a higher percentage of female patients (93%) with a high ligamentous laxity (Beighton score ≥4) in patients undergoing hip arthroscopy compared to patients with a low ligamentous laxity (Beighton score 0-3) who underwent hip arthroscopy (59% female), which is consistent with previous findings that female patients without preoperative stiffness were more likely to undergo capsular repair or plication. 14 Although our exclusion criterion of LCEA <20° minimized the variability of hip instability among patients in our study, the incidence of ligamentous laxity among women and improved outcomes with capsular closure support our findings that women >45 years of age had improved pain and functional scores at 1-year postoperative follow-up with capsular closure (Supplemental Table S2). Additionally, women aged 30 to 45 years had higher preoperative MHHS in the capsular repair or plication group than in the no-closure group, which may suggest a bias. This difference was mitigated when controlled for age. The change from preoperative to 1- and 2-year outcomes was not significantly different, which may suggest that change is similar among age groups despite the higher preoperative MHHS overall. Additional studies are needed to assess the risk of instability in women and younger patients who undergo hip arthroscopy without capsular repair or plication.
We found no difference in functional outcomes between capsular dissection techniques with repair (interportal capsulotomy vs T-capsulotomy). Although functional outcomes may not differ between the 2 techniques, 3 studies have claimed that preferences in type of capsular dissection are due to the differences in hip joint visualization.3,12 To our knowledge, only 1 study has compared interportal versus T-type capsulotomy with capsular repair in patients undergoing FAI repair, and the authors found no difference at 2-year follow-up. 44 Corroborating these findings, patients in our study with T-capsulotomy achieved the MCID and the PASS in 1-year MHHS at a similar rate compared with those who underwent interportal capsulotomy (MCID, 50.1% vs 44.9%, P = .531; PASS, 65.7% vs 61.2%, P = .518, respectively).
Limitations
Although we used a well-powered case-control design, the current study is not without limitations. The use of large, multicenter databases allowed for larger patient cohorts with many operating surgeons, and thus conclusions are more generalizable; however, large databases are intrinsically limited. We could not control for capsular exposure technique when comparing pain and functional outcomes between patients who underwent arthroscopic hip labral repair with concomitant capsular repair and patients without capsular closure. Objective imaging data (ultrasonography or magnetic resonance imaging) on capsular integrity at follow-up were not available; therefore, we were unable to assess the incidence of capsular repair failure. The available surgical data also limited assessment of labral repair technique, osteoplasty, and capsular repair technique. Coding bias may have occurred when we accessed the Surgical Outcomes System database. 58 Additionally, our database was limited by variable surgeon experience and by postoperative protocols that vary by institution and surgeon.
Although pain and functional outcomes may be equivocal, we were unable to evaluate whether patients undergoing capsular closure or plication had a lower risk of revision surgery, dislocation, or instability events.20,57 Although these outcomes may be indirectly evaluated by the included pain and functional scores, low rates of dislocation and instability may have been obscured by predominant similarities in pain and daily function. Given the multifactorial nature of patient selection when a surgeon is deciding whether to repair the capsule, the potential effect of selection bias must be considered despite our attempts to reduce bias by excluding patients with obvious indications for capsular repair (eg, history of instability and LCEA <20°), because we also did not control for preoperative Beighton scores. Also, we were unable to match some patients between the repair or plication group and the no-closure group, which could have contributed to selection bias. Additionally, our study specifically assessed patient outcomes after primary hip arthroscopy labral repair and excluded patients with previous capsular intervention or closure, and we were unable to match for body mass index between our cohorts. Although we found no differences in pain and functional outcomes between groups, capsular closure may be more influential of patient outcomes when performed in the setting of revision hip arthroscopy or in athletes desiring an expedited return to sport.41,53
Conclusion
Controlling for patient sex, age, and preoperative MHHS, we demonstrated similar pain and functional outcomes in patients undergoing hip arthroscopic labral repair with concomitant capsular repair compared with no capsular closure, with improvement in outcomes in both groups. Similarly, whether a T-capsulotomy or interportal capsulotomy was performed before capsular closure did not influence pain and functional outcomes. Future studies are needed to ascertain long-term outcomes and the rate of revision surgery and conversion to arthroplasty.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671241243303 – Supplemental material for Comparison of Pain Scores and Functional Outcomes of Patients Undergoing Arthroscopic Hip Labral Repair and Concomitant Capsular Repair or Plication Versus No Closure
Supplemental material, sj-pdf-1-ojs-10.1177_23259671241243303 for Comparison of Pain Scores and Functional Outcomes of Patients Undergoing Arthroscopic Hip Labral Repair and Concomitant Capsular Repair or Plication Versus No Closure by Victoria E. Bindi, Kevin A. Hao, David A. Freeman, Bankole O. Olowofela, Michael W. Moser, Kevin W. Farmer, Marissa Pazik and Ryan P. Roach in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted September 24, 2023; accepted October 11, 2023.
One or more of the authors declared the following potential conflict of interest or source of funding: M.W.M. has received education payments from CGG Medical and Fortis Surgical LLC. K.W.F. has received nonconsulting fees from Arthrex, Arthrosurface Inc, Baudax Bio, and CGG Medical; education payments from CGG Medical and Arthrex; consulting fees from Exactech, Arthrex, and Flexion Therapeutics; and honoraria from Baudax Bio. R.P.R. has received education payments from CGG Medical, Arthrex, and Smith & Nephew and grant payments from Arthrex. K.H. has received consulting fees from LinkBio Corp. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto
Ethical approval for this study was obtained from the University of Florida (reference No. 16614).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.