
Abstract
Background:
While the biomechanical importance of the hip capsule is well described, there remains controversy over the necessity of routine capsular closure after hip arthroscopy.
Purpose:
To perform a meta-analysis of clinical studies to compare pooled outcomes of complete hip capsular closure cohorts against unrepaired hip capsule cohorts.
Study Design:
Systematic review; Level of evidence, 3.
Methods:
The Cochrane Database of Systematic Reviews, Cochrane Register of Controlled Trials, PubMed, MEDLINE, Web of Science, CINAHL/EBSCO, and Scopus were queried in February 2022 for studies that directly compared clinical outcomes for hip arthroscopy patients treated with either complete capsular closure or an unrepaired capsule. Outcomes assessed were incidence of revision hip arthroscopy, incidence of subsequent conversion to total hip arthroplasty (THA), and improvement from baseline in modified Harris Hip Score (mHHS), Hip Outcome Score (HOS) activities of daily living (ADL), HOS sports specific (SS) subscale, Copenhagen Hip and Groin Outcome Score (HAGOS) ADL, and HAGOS SS subscale. A pooled weighted mean difference (WMD) was used to compare changes in mHHS. A pooled standardized mean difference (SMD) was used to compare changes in the ADL and SS outcomes. A pooled risk ratio (RR) was used to compare the probability of revision hip arthroscopy and conversion to THA based on capsular management. For pooled outcomes where heterogeneity was regarded as potentially unimportant, a fixed-effects model was implemented. For pooled outcomes with considerable heterogeneity, a random-effects model was implemented.
Results:
Of the 1896 records identified in our search, 11 studies (1897 patients) were included. A significantly higher improvement in mHHS (WMD, −3.72; 95% CI, −4.95 to −2.50; P < .00001) and ADL outcomes (SMD, −0.30; 95% CI, −0.54 to −0.07; P = .01) were seen after complete capsular closure. There was a significantly lower probability of subsequent revision hip arthroscopy (RR, 1.67; 95% CI, 1.14 to 2.45; P = .008) and conversion to THA (RR, 2.01; 95% CI, 1.06 to 3.79; P = .03) after complete capsular repair. There was no difference in SS outcomes (SMD, −0.02; 95% CI, −0.16 to 0.13; P = .81) between the 2 groups.
Conclusion:
This meta-analysis demonstrated that routine complete capsular closure after hip arthroscopy led to superior clinical outcomes relative to unrepaired hip capsules.
Keywords
Over the past 2 decades, there has been a growing interest in the use of hip arthroscopy to manage nonarthritic hip disorders. 31 Hip arthroscopy has been shown to reliably treat femoroacetabular impingement and labral tears in young, active patient populations. 10 During the procedure, a capsulotomy is performed to gain surgical access to the central and peripheral compartments of the hip joint (Figure 1). Capsulotomy techniques typically include an interportal capsulotomy, which is a transverse incision that usually extends from the modified anterior portal to the anterolateral portal, and a T-capsulotomy, which consists of an orthogonal incision originating at the midportion of the interportal capsulotomy and extending distally toward the intertrochanteric line (Figure 2).11,12 While both techniques allow for adequate access to the femoroacetabular joint and femoral neck, they disrupt the native anatomy and biomechanics of the hip by incising the iliofemoral ligament.20,24,35 This is of clinical importance given that the iliofemoral ligament is the strongest of the 3 ligaments that comprise the hip capsule; disruption of the iliofemoral ligament can lead to pain, dysfunction, and microinstability of the hip joint.4,10

(A) Hip capsular anatomy on cadaveric specimen and as visualized during arthroscopy from both the (B) anterolateral portal and the (C) modified midanterior portal. A, acetabulum; DH, direct head (of rectus femoris); FH, femoral head; GT, greater trochanter; IH, indirect head (of rectus femoris); L, labrum.

Cadaveric representation of an (A) interportal capsulotomy and (B) T-capsulotomy. Retraction of the capsular limbs from the interportal capsulotomy—with added traction of the limb (not represented here)—will provide exposure for acetabular rim trimming and labral repair, while retraction of the capsular limbs from the T-capsulotomy will expose the femoral head-neck junction (FHNJ) for cam resection.
Capsular closure is able to restore native hip anatomy and biomechanics by repairing the iliofemoral ligament (Figure 3). 22 Historically, capsular repair was not routinely performed during hip preservation surgery. 22 This was likely due to a variety of factors including the technical difficulty of capsular repair, the belief that the osseous morphology of the hip gives the joint inherent static stability, and the failure to recognize the hip capsule’s critical role as a stabilizer of the joint.11,18,22,28 More recently, the importance of the hip capsule in preventing microinstability has gained greater clinical acceptance among surgeons. 28 It is increasingly recognized as a key stabilizer of the joint and works in concert with the other primary stabilizers of the joint, including the labrum, ligamentum teres, and static hip stabilizers. 27 As the biomechanical importance of the hip capsule has gained an improved understanding, there has been a paradigm shift among high-volume hip arthroscopists toward performing routine capsular closure.22,31

After femoroplasty, the capsule should be closed completely to minimize instability. With visualization from the modified midanterior portal and instrumentation via the anterolateral portal, the T-capsulotomy is closed first, followed by the horizontal interportal component. (A) Capsular closure is performed with use of a suture passer, deploying the suture through one of the capsular limbs and (B) retrieving it through the opposite limb. (C) Watertight closure is confirmed visually and via probe. (D) This is further represented in a cadaveric model. FHNJ, femoral head-neck junction.
Biomechanical studies have demonstrated that the creation of a capsulotomy disrupts the native strength and function of the iliofemoral ligament and that complete capsular repair fully restores native hip anatomy and biomechanics. 34 While the biomechanical data have supported restoration of native hip anatomy after hip arthroscopy, comparative in vivo clinical studies have been less conclusive. This is highlighted by the fact that several studies have reported the superior clinical outcomes with capsular closure, while other studies have noted no clinical benefit to capsular closure.4,8,10 As a result, routine closure of the hip capsule remains relatively controversial among hip preservation surgeons. 27
Recently, 2 meta-analyses have demonstrated the significant clinical benefit of routine capsular closure.21,22 The first study, by Kunze et al, 21 demonstrated that patients with a repaired hip capsule had a higher probability of reaching the minimal clinically important difference (MCID) for the modified Harris Hip Score (mHHS). While clinically relevant, this study was intrinsically restricted by its study design, as many clinical studies examining hip capsular closure did not report MCID-related outcomes. A subsequent meta-analysis by Looney et al 22 demonstrated a significant clinical benefit to hip capsular closure for the mHHS and the Hip Outcome Score–activities of daily living (HOS-ADL) and–sports specific (HOS-SS) subscales. 22 While impressive, this meta-analysis pooled largely single-arm case series studies, included multiple publications from the same authorship groups, likely had overlapping patient cohorts among several included studies, and did not examine the risk of revision hip arthroscopy or conversion to arthroplasty. Additionally, since the publication of these 2 impactful meta-analyses, there have been 2 additional randomized controlled trials (RCTs) published that directly compare the clinical outcomes between hip capsular closure and unrepaired hip capsules during hip arthroscopy.3,31
The purpose of this study was to systematically review all available comparative clinical outcome studies that compared hip capsular closure to unrepaired hip capsules during hip arthroscopy. By incorporating only comparative clinical outcome studies, a meta-analysis could be conducted to compare patient-reported outcome measures (PROMs), the risk of revision hip arthroscopy, and the risk of subsequent conversion to total hip arthroplasty (THA) between the 2 groups. The authors of this investigation hypothesized that complete hip capsular closure would lead to improved PROMs, a decreased risk of requiring revision hip arthroscopy, and a decreased risk for subsequent conversion to THA relative to the cohort that did undergo complete capsular repair.
Methods
Article Identification and Selection
The study was conducted in accordance with the 2020 PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement. 26 The Cochrane Database of Systematic Reviews, the Cochrane Register of Controlled Trials, PubMed, MEDLINE, Web of Science, CINAHL/EBSCO, and Scopus were queried in February 2022 for clinical literature comparing complete capsular closure against unrepaired capsules during hip arthroscopy. The following search terms were used: “Hip Arthroscopy Capsule” OR “Hip Arthroscopy Capsular.” Inclusion criteria were as follows: comparative clinical study (level of evidence 1, 2, or 3), compared complete capsular closure to unrepaired capsules, patients underwent hip arthroscopy, and the study reported at least 1 PROM. Exclusion criteria were as follows: noncomparative studies (level of evidence 4 or 5), cadaveric/animal/in vitro study, any editorial article, any survey, any letter to the editor, any special topics, and any expert reviews. Additionally, any studies performed by the same authorship group were reviewed to determine if the study included overlapping patient cohorts. For cases in which it was unclear if the patients were unique to each study, only the most recently published study was included to avoid pooling overlapping patient cohorts in this meta-analysis. Two investigators (J.J.C. and L.B.K.) independently screened articles by title, abstract, and full text, when appropriate. For any disagreements, these 2 authors discussed the study with a third author (S.P.D.), and a consensus was reached.
Outcome Measures and Data Extraction
The primary outcome measures evaluated in this meta-analysis were (1) improvement from baseline of mHHS, (2) improvement from baseline of HOS-ADL, (3) improvement from baseline of HOS-SS, (4) improvement from baseline Copenhagen Hip and Groin Outcome Score (HAGOS)–ADL subsection, (5) improvement from baseline HAGOS-SS subsection, (6) incidence of revision hip arthroscopy, and (7) incidence of subsequent conversion to THA. A customized data extraction spreadsheet was created to record all relevant data from the included studies comprising publication information, study design, level of evidence, demographic information (age, sex), time until final follow-up, capsulotomy type, capsular management, and the aforementioned outcome scores. Before inclusion, all data were qualitatively analyzed based on their methods, results, discussion, and conclusion. For studies where the standard deviation for the improvement from baseline was not reported, the value was imputed using the methods described in the Cochrane handbook section 6.5.2.8. 17 An RCT by Sugarman et al 31 was used as a reference for calculating imputations.
Risk-of-Bias Assessment
Two investigators (J.J.C. and L.B.K.) independently assessed risk of bias, with any disagreements resolved by consensus. Nonrandomized comparative studies were assessed using the methodological index for nonrandomized studies (MINORS) criteria, 29 which comprise 12 items each scored as 0 (not reported), 1 (reported but inadequate), and 2 (reported and adequate). For a comparative study, an ideal score would be 24 points. For randomized studies, the Cochrane risk-of-bias tool was implemented. 30 Domains assessed included bias arising from the randomization process, deviations from the intended intervention, missing outcome data, measurement of the outcome, and selection of the reported result; each domain was assessed as being of high concern, some concern, or low concern for bias.
Statistical Analysis
Continuous outcomes (PROMs) were pooled and compared using an inverse variance model. The probability of revision hip arthroscopy or subsequent conversion to THA was assessed by calculating a pooled risk ratio (RR) and compared using a Mantel-Haenszel model. Heterogeneity was assessed with the I2 statistic and regarded as potentially unimportant for cases where the I2 value was <40% and considerable when the I2 value was >75%.14,21 For studies where the heterogeneity was considered potentially unimportant, a fixed-effects model was implemented, which is consistent with previous methodology.5,9,21 For all remaining outcomes, a random-effects model was implemented. The pooled mHHS was compared using a weighted mean difference (WMD) and 95% CI to assess the mean and range of true means. The ADL outcomes were assessed using a standardized mean difference (SMD) with a 95% CI so that both HAGOS and HOS ADL outcomes could be pooled together. The SS outcomes were assessed using a standardized mean difference (SMD) with a 95% CI so that both HAGOS and HOS SS outcomes could be pooled together. The magnitude of the SMD was assessed according to the Cohen d estimate, where <0.5, 0.5-0.8, and >0.8 correspond to small, medium, or large effect sizes, respectively. 6 An alpha <.05 was assigned as significant. Statistical analysis was performed using Review Manager 5 (The Nordic Cochrane Center) and SPSS Statistics for Macintosh (Version 28.0; IBM).
Results
Demographics/Study Characteristics
A total of 11 comparative studies2-4,7,8,10,13,15,16,31,32 (1897 patients) were included in this meta-analysis (Figure 4 and Table 1). Ten studies2-4,7,8,10,13,16,31,32 directly compared complete capsular closure to an unrepaired capsule, and 1 study, by Frank et al, 15 compared complete capsular closure to partial repair for patients with T-capsulotomies. For their partial repair cohort, the authors repaired the T-incision of the capsulotomy, while keeping the interportal incision unrepaired. This study was included in the present meta-analysis, as previous meta-analyses that directly compared capsular closure with unrepaired hip capsules22,25 had included this study and treated the partial repair group as part of the unrepaired cohort in their systematic review and meta-analysis.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart of the study selection criteria. PROM, patient-reported outcome measure.
Characteristics of the Included Studies a
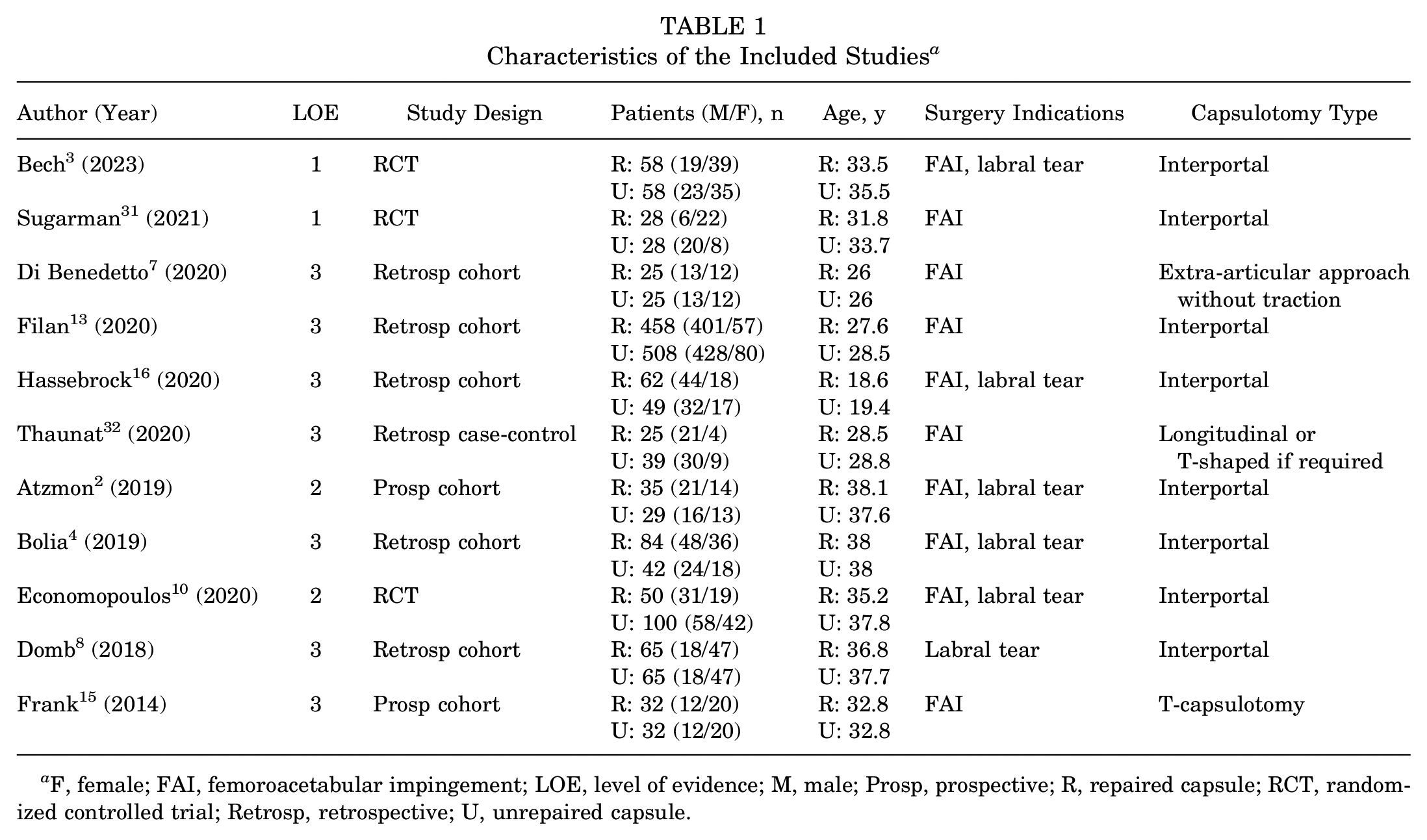
F, female; FAI, femoroacetabular impingement; LOE, level of evidence; M, male; Prosp, prospective; R, repaired capsule; RCT, randomized controlled trial; Retrosp, retrospective; U, unrepaired capsule.
In the unrepaired cohort, there were a total of 975 patients (674 male/301 female) who had surgery at a mean age of 30.9 years (range, 19.4-38.0 years) and had a mean final follow-up of 29.3 months (range, 7.3-75.7 months). In the complete capsular closure cohort, there were a total of 922 patients (634 male/288 female) who had surgery at a mean age of 30.0 years (range, 18.6-38.1 years) and had a mean final follow-up of 28.3 months (range, 6.4-64.8 months). When examining surgical technique, a total of 8 studies examined interportal capsulotomies,2-4,8,10,13,16,31 1 study examined T-shaped capsulotomies, 15 1 study examined longitudinal or T-shaped capsulotomies, 32 and 1 study examined an extra-articular approach without traction. 7
Risk-of-Bias Assessment
Eight nonrandomized comparative studies2,4,7,8,13,15,16,32 were assessed with the MINORS criteria; the mean MINORS score was 19.9 (range, 18-22) (Figure 5A). Of 3 randomized clinical studies3,10,31 assessed using the Cochrane risk-of-bias tool, 2 studies3,31 had a low risk of bias (Figure 5B). In the third study, 10 there was some concern of bias during the randomization process, resulting in a moderate risk of bias.
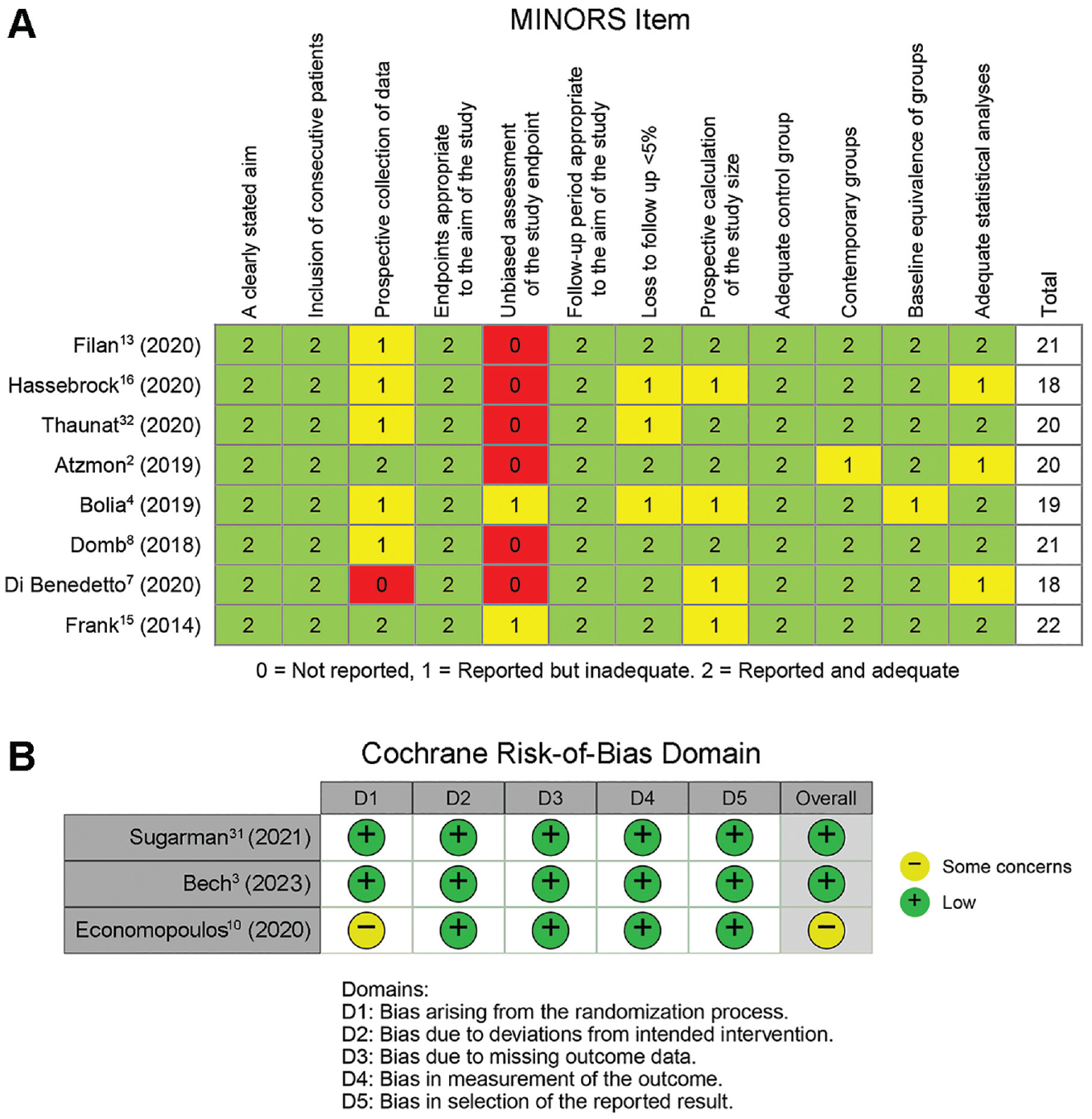
Bias assessment using the (A) methodological index for nonrandomized studies (MINORS) and the (B) Cochrane risk-of-bias 2.0 tool for randomized clinical studies.
Primary Clinical Outcomes
Nine studies4,7,8,10,13,15,16,31,32 assessed postoperative mHHS improvements in patients undergoing hip arthroscopy. For this mHHS-based analysis, there were 834 patients who had an unrepaired hip capsule and 792 patients who had a completely repaired hip capsule. The improvement from baseline in mHHS was assessed with a pooled WMD and a 95% CI (Figure 6). There was a significantly greater pooled improvement from baseline in mHHS for patients who underwent complete capsular closure relative to unrepaired capsule groups (WMD, −3.72; 95% CI, −4.95 to −2.50; P < .00001).

Forest plot demonstrating the weighted mean difference for improvement in modified Harris Hip Score in hip arthroscopy patients treated with complete capsular closure or hip arthroscopy patients with unrepaired hip capsules. This includes a summary estimate (center of the diamond) and a 95% CI (width of the diamond) for the true mean difference. The size of each square represents the relative weight given to each respective study. For this outcome, a random-effects inverse variance (IV) model was implemented.
Five studies4,10,15,16,31 assessed postoperative improvements in HOS-ADL in patients undergoing hip arthroscopy. One study 3 assessed the improvement from baseline in the HAGOS-ADL subsection in patients undergoing hip arthroscopy. Thus, the ADL outcome was assessed using a pooled SMD with a 95% CI (Figure 7). For this outcome, there were 274 patients with an unrepaired hip capsule and 292 patients with a completely repaired hip capsule. There was a significantly greater improvement in ADL outcomes for hip arthroscopy patients with a completely closed capsule relative to hip arthroscopy patients with an unrepaired hip capsule (SMD, −0.30; 95% CI, −0.54 to −0.07; P = .01).

Forest plot demonstrating the standardized (std) mean difference for improvement in activities of daily outcomes in hip arthroscopy patients treated with complete capsular closure or hip arthroscopy patients with unrepaired hip capsules. This includes a summary estimate (center of the diamond) and a 95% CI (width of the diamond) for the true mean difference. The size of each square represents the relative weight given to each respective study. For this outcome, a random-effects inverse variance (IV) model was implemented.
Seven studies4,7,8,10,15,16,31 assessed the postoperative improvement from baseline of the HOS-SS after hip arthroscopy. One study 3 assessed the improvement from baseline in the HAGOS-SS subsection in patients who underwent hip arthroscopy. Thus, the SS outcome was assessed using a pooled SMD with a 95% CI (Figure 8). For this outcome, there were 364 patients with an unrepaired hip capsule and 382 patients with a completely repaired hip capsule. There was no significant difference between the 2 groups for SS outcomes (SMD, −0.02; 95% CI, −0.16 to 0.13; P = .81).

Forest plot demonstrating the standardized (std) mean difference for improvement in SS outcomes in hip arthroscopy patients treated with complete capsular closure or hip arthroscopy patients with unrepaired hip capsules. This includes a summary estimate (center of the diamond) and a 95% CI (width of the diamond) for the true mean difference. The size of each square represents the relative weight given to each respective study. For this outcome, a fixed-effects inverse variance (IV) model was implemented.
Among the 11 studies included in this meta-analysis, 7 studies3,4,8,10,13,15,16 reported the number of patients who underwent subsequent revision hip arthroscopy. Of the 916 patients with unrepaired hip capsules at final follow-up, 65 patients required a subsequent revision hip arthroscopy procedure. Of the 883 patients with completely closed hip capsules at final follow-up, 36 patients underwent a subsequent revision hip arthroscopy procedure. The probability of requiring a subsequent revision hip arthroscopy procedure was assessed using the RR and 95% CI (Figure 9). There was a significantly lower probability of requiring a subsequent revision hip arthroscopy procedure in patients with completely closed hip capsules relative to the unrepaired hip capsule cohort (RR, 1.67; 95% CI, 1.14-2.45; P = .008). This indicates that hip arthroscopy patients with unrepaired hip capsules were 67% more likely to require a subsequent revision hip arthroscopy procedure than the complete capsular closure patient cohort.

Forest plot demonstrating the risk ratio (RR) for subsequent revision hip arthroscopy procedures in hip arthroscopy patients treated with complete capsular closure or hip arthroscopy patients with unrepaired hip capsules. This includes a summary estimate (center of the diamond) and a 95% CI (width of the diamond) for the true mean difference. The size of each square represents the relative weight given to each respective study. For this outcome, a fixed-effects Mantel-Haenszel (M-H) model was implemented.
Four studies4,8,10,13 reported the number of patients who underwent a subsequent conversion to THA. Of the 916 patients with unrepaired hip capsules at final follow-up, 22 patients were converted to THA. Of the 883 patients with completely closed hip capsules at final follow-up, 12 patients were converted to THA. The probability of subsequent conversion to THA was assessed using the RR and 95% CI (Figure 10). There was a significantly lower probability of subsequent conversion to THA in patients with completely closed hip capsules relative to the unrepaired hip capsule cohort (RR, 2.01; 95% CI, 1.06-3.79; P = .03). This data set indicates that hip arthroscopy patients with unrepaired hip capsules were 101% more likely to subsequently convert to THA than the complete capsular closure patient cohort.

Forest plot demonstrating the risk ratio for subsequent conversion to total hip arthroplasty in hip arthroscopy patients treated with complete capsular closure or hip arthroscopy patients with unrepaired hip capsules. This includes a summary estimate (center of the diamond) and a 95% CI (width of the diamond) for the true mean difference. The size of each square represents the relative weight given to each respective study. For this outcome, a fixed-effects Mantel-Haenszel (M-H) model was implemented.
Discussion
The major findings of this systematic review and meta-analysis were that complete capsular closure leads to (1) a significantly higher improvement in mHHS from baseline relative to unrepaired hip capsules (WMD, −3.72; 95% CI, −4.95 to −2.50; P < .00001); (2) significantly higher improvement from baseline in ADL outcome scores relative to unrepaired hip capsules (SMD, −0.30; 95% CI, −0.54 to −0.07; P = .01); (3) significantly lower probability of subsequent revision hip arthroscopy (RR, 1.67; 95% CI, 1.14 to 2.45; P = .008); and (4) significantly lower probability of subsequent conversion to THA (RR, 2.01; 95% CI, 1.06 to 3.79; P = .03). Of note, there was no significant or clinically important difference observed regarding SS outcomes between the capsular repair and unrepaired cohorts (SMD, −0.02; 95% CI, −0.16 to 0.13; P = .81).
Biomechanical evaluation of the hip capsule has consistently demonstrated its critical role in preventing microinstability by acting as a key stabilizer of the joint. For example, a novel biomechanical study by Johannsen et al 19 demonstrated the importance of the hip capsule in controlling femoral head motion and minimizing hip microinstability, while a separate study by Myers et al 23 concluded that repair of the labrum and iliofemoral ligament should be performed to restore native hip rotation and translation. While clinical studies have reported increased rates of anterior dislocation and microinstability in cases where hip capsular closure was not performed, there still remains controversy regarding routine capsular closure. 27 Opponents of capsular closure have historically stated that complete capsular closure may lead to overconstraint of the joint, limitations in hip range of motion, and increased surgical time. 27 A 2017 study by Philippon et al 27 demonstrated that both interportal and T-capsulotomies lead to increased femoral rotation, but subsequent repair of the capsulotomies improved stability at the hip joint without overconstraining the joint. A similar study by Wach et al 33 at demonstrated that capsulotomies reduced the resistive torques at the hip joint, but repair of T-type and interportal capsulotomies restored resistive torque to a level comparable with the intact state. A separate biomechanical study evaluating hip laxity also demonstrated that capsular repair restores hip joint stability back to the native, intact state. 1 Thus, it is evident that the biomechanical literature strongly advocates for routine capsular closure and restoration of native anatomy when performing minimally invasive, hip arthroscopic procedures. As a result, when placing the results of this present meta-analysis in the context of the current biomechanical literature examining hip capsular repair, it is not surprising that the capsular repair group largely demonstrated superior pooled clinical outcomes relative to the unrepaired capsule group.
Due to the conflicting clinical literature regarding hip capsular management during hip arthroscopy, previous meta-analyses have attempted to pool the clinical literature to guide practice. Well-designed studies by Kunze et al 21 and Looney et al 22 have demonstrated an overwhelming benefit to capsular closure when pooling clinical outcomes. Similar to the study by Kunze et al, the present meta-analysis only included comparative studies but was not restricted by evaluation of MCID. In addition to mHHS-centric analysis, the present study also demonstrated an increased benefit in ADL outcomes when only including comparative studies. The broader study by Looney et al reported a significant benefit in SS outcomes by including noncomparative literature; however, this benefit was not noted in this present meta-analysis of comparative studies. Novel to both previous meta-analyses, the present study examined the probability of revision hip arthroscopy and subsequent conversion to THA based on capsular management. Hip capsular closure demonstrated a significantly lower risk of subsequent revision hip arthroscopy and conversion to THA. This indicates there is a substantial benefit to complete capsular closure after hip arthroscopy that extends beyond PROMs. Thus, in the context of the current clinical literature, the present study provides significant support and expands on the conclusions drawn by the previous meta-analyses.
Limitations
This study is not without limitations. First, as a meta-analysis, it is inherently limited by the study design of the included publications. The majority of the included studies did not report outcomes as a change from baseline. Thus, the mean difference and standard deviation of improvement from baseline were imputed using methods described in the Cochrane handbook. 17 While valid, this represents a relative approximation of absolute real-world values. Additionally, for each primary clinical outcome, the majority of individual study confidence intervals suggested a nonsignificant clinical benefit of complete capsular closure; however, a statistically significant pooled benefit was noted, suggesting underpowered cohorts. This emphasizes the need for a future, adequately powered RCT, which may be better able to elucidate the true clinical benefit of complete capsular closure in the context of hip arthroscopy. The present meta-analysis was also limited by the number of studies that examined T-capsulotomies, and future comparative literature addressing capsular management outcomes in the setting of T-capsulotomies should be pursued for patients being arthroscopically treated for femoroacetabular impingement with large cam lesions. This meta-analysis was also limited by variability in postoperative rehabilitation protocols, and a future, adequately powered investigation with uniform postoperative rehabilitation across both cohorts would be better designed to assess the true benefit of complete capsular closure in hip arthroscopy patients. Finally, we were limited by the relatively short final follow-up of the included studies. Studies with longer follow-up would be better designed to examine terminal outcomes such as conversion to THA.
Conclusion
The findings of this systematic review and meta-analysis demonstrated that routine complete capsular closure after hip arthroscopy led to superior clinical outcomes relative to unrepaired cohorts.
Footnotes
Final revision submitted March 8, 2023; accepted April 26, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: L.S. has received education payments from Medwest, Rock Medical, and Smith & Nephew. M.H. has received education payments from Medwest and Smith & Nephew, consulting fees from Moximed, and hospitality payments from Medical Device Business Services. J.C. has received grant support from Arthrex; education payments from Arthrex and Smith & Nephew; consulting fees from Arthrex, DePuy, Linvatec, Ossur, Smith & Nephew, and Vericel; nonconsulting fees from Linvatec and Smith & Nephew; and hospitality payments from Styker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.