
Abstract
Background:
Anterolateral knee laxity (ALLx) has been linked to tears of the lateral meniscus (LM) and anterior cruciate ligament (ACL) injury.
Purpose:
To investigate the longitudinal relationship between the signal intensity (SI) of the repaired LM on magnetic resonance imaging (MRI) and residual ALLx after ACL reconstruction (ACLR).
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Included were 87 patients who underwent double-bundle ACLR and lateral meniscal repair (mean age, 23.5 years; body mass index, 23.7 kg/m2; 56 women) at a single institution between 2010 and 2019. Proton density-weighted (PDW) and T2-weighted (T2W) MRI was performed at 3, 6, and 12 months postoperatively, and the SI ratio (SIR) was calculated as (SI of the repaired LM)/(SI of the posterior cruciate ligament). At the 12-month follow-up, ALLx was evaluated using the pivot-shift test; an International Knee Documentation Committee grade ≥1 indicated residual ALLx.
Results:
Overall, 12 patients (13.8%) exhibited ALLx at 12 months postoperatively. At 3 months postoperatively, the SIR on PDW images (SIR-PDW) was significantly higher in patients with ALLx versus those without ALLx (1.98 ± 0.77 vs 1.49 ± 0.52, respectively; P = .007); there was no difference in the SIR on T2W images between the groups. SIR-PDW at 3 months postoperatively was correlated negatively with patient age (r = -0.308, P = .004). When patients were stratified into a younger (≤22 years; n = 53; ALLx = 7 [13.2%]) and an older (>22 years; n = 34; ALLx = 5 [14.7%]) group, the area under the receiver operating characteristic curves (AUCs) for SIR-PDW in the younger group were statistically significant for predicting the prevalence of ALLx at all follow-up times (AUCs, 0.733-0.788) with optimal cutoff values of 2.00 at 3 months, 1.50 at 6 months, and 1.50 at 12 months. Logistic regression analysis revealed that if younger patients consistently had higher SIR-PDW values than the cutoff values, they were more likely to have residual ALLx (odds ratios, 10.24-23.57).
Conclusion:
For younger patients who underwent both ACLR and lateral meniscal repair, higher MRI SI of the repaired LM was associated with a higher prevalence of residual ALLx.
Patients with anterior cruciate ligament (ACL) injury have anterior knee laxity and anterolateral knee laxity (ALLx) due to ACL deficiency. 36 The presence of residual pivot shift among patients who undergo ACL reconstruction (ACLR) indicates poor clinical outcomes such as symptomatic knee instability, 3 inferior patient-reported outcomes,1,26,27 and the development of knee osteoarthritis. 22 Identifying the etiology of residual ALLx after ACLR will lead to better surgical outcomes.
Tear of the lateral meniscus (LM) is a common complication of ACL tear.13,35,41 A concomitant lateral meniscal tear with ACL rupture is more likely to cause ALLx than an isolated ACL tear,11,17,32,40,44 whereas several factors, such as knee hyperlaxity and the derangement of anterolateral structure,19,30,33,38,47 have been reported to be associated with ALLx. In addition, combined ACLR and lateral meniscal repair has been found to improve residual ALLx not only in cadaveric knees but also in the clinical setting.24,42,4 Although combined ACLR and lateral meniscal repair would better prevent residual ALLx than isolated ACLR surgery, previous studies have been limited by their time-zero design, and little is known about the longitudinal relationship between failure of lateral meniscal repair and residual ALLx.
In a previous study, 8 we found that the prevalence of residual pivot shift at 1 year after ACLR was more common among patients who underwent combined ACLR and lateral meniscal repair than among those with an intact LM or a stable lateral meniscal tear (no instability by probing). Based on this previous work, we speculated that the repaired LM in patients with ACLR may fail to heal and restore its function to stabilize the ALLx. Several studies have indicated that the signal intensity (SI) of the repaired LM on magnetic resonance imaging (MRI) is a diagnostic indicator of meniscal healing10,31,43,49; however, at this point, there is little evidence related to how the SI of the repaired LM is associated with residual ALLx after ACLR. In addition, we reported in another study that the SI of the hamstring graft used in ACLR was affected significantly by patient age, 7 wherein younger patients demonstrated higher SI in the intra-articular part of the graft compared with older patients. The younger patients were also found to have a greater risk of residual knee laxity after ACLR. 7 However, the contribution of patient age to the SI of the repaired LM, including the risk of residual ALLx after ACLR, remains largely unclear.
To address these knowledge gaps, we conducted the current study with 2 aims in mind: (1) to evaluate the longitudinal relationship between the SI of the repaired LM as measured on MRI scans and the residual ALLx at 1 year after combined ACLR and lateral meniscal repair, and (2) to assess the relationship between the SI of the repaired LM and patient age. Accordingly, we tested 2 hypotheses: (1) patients with a higher SI of the repaired LM would be more likely to demonstrate postoperative residual ALLx and (2) the SI of the repaired LM would be affected by patient age.
Methods
We reviewed the records of 599 patients who underwent anatomic double-bundle ACLR with a hamstring tendon autograft at a single institution between 2010 and 2019. Of these 599 patients, 272 were excluded as having incomplete data, infection, open physis, multiple ligamentous injuries requiring repair or reconstruction, current or previous meniscal resection, revision surgery, ACL reinjury within 1 year postoperatively, severe chondral damage (International Cartilage Repair Society grade 3 or 4), or knee osteoarthritis (Kellgren-Lawrence grade ≥2). Among 327 patients who underwent ACLR, 87 who underwent concomitant lateral meniscal repair were recruited for this study (Figure 1). We obtained patient data, including age, sex, body mass index (BMI), Tegner activity score, and time from injury to surgery, from patient medical records. The ethics committee of our institution approved the study design, and all included patients gave written informed consent before participation.

Flowchart of patient recruitment for this study. ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction.
Surgical Procedure for Anatomic Double-Bundle ACLR
The surgical procedure of double-bundle ACLR in this study was consistent for all patients.9,39 The harvested semitendinosus tendon was split, and the distal and proximal ends of each split tendon were looped to form anteromedial and posteromedial bundles, respectively. Until August 1, 2014, the proximal end of each graft was fixed by the fixed-loop cortical suspensory system (Position Suture Plate; B. Braun Aesculap); thereafter, an adjustable-loop cortical suspensory system (TightRope; Arthrex) was used to retain the graft and provide a longer graft in the femoral tunnel to maximize the graft-bone interface area.5,18 The distal end of each graft was fixed separately by using a suture mini-disc (B. Braun Aesculap), with maximum manual force applied as the initial tension at 15° to 20° of flexion. 39 The postoperative rehabilitation program was consistent with that of a previous study. 39
Arthroscopic Evaluation and Surgical Protocol for Lateral Meniscal Repair
We probed the presence and degree of the lateral meniscal tear during an arthroscopic survey before ACLR. Furthermore, we examined the morphology of the tear (ie, longitudinal, radial, and flap tears) and the lateral meniscal tear lesion (ie, posterior root, posterior horn, and middle body). Meniscal repair was performed if the torn lateral meniscal body was retracted easily by probing and the torn part of the meniscus did not contain any connected tissue (Figure 2, A and B). We repaired the meniscus when the tear occurred in a red-white or red-red zone because these zones are vascularized and have the potential to heal the injured meniscal tissue (Figure 2, C and D).2,4,45 However, if the lateral meniscal tear was connected by the remaining lateral meniscal tissue and the torn lateral meniscal tissue was stable by probing, we did not perform meniscal repair (Figure 2, E and F). Meniscectomy was performed on patients with a deteriorated torn meniscal body or a complex tear pattern (these patients were excluded from the study). Lateral meniscal repair was performed using a Fast-Fix (Smith+Nephew Endoscopy) or Knee Scorpion (Arthrex) system in accordance with the all-inside technique.

Representative arthroscopic images of a patient with repaired and unrepaired lateral menisci in the posterior horn. (A and B) Unstable longitudinal and radial tears were observed and repaired arthroscopically. (C and D) Unstable tears were observed and repaired arthroscopically. (E and F) Longitudinal tears that could not be displaced anteriorly by probing and showed no signs of instability were not repaired.
SI of Repaired LM
Patients underwent 1.5-T MRI scans (Signa HDxt; GE Healthcare) of their operated knee joint at a mean of 3, 6, and 12 months postoperatively. The knee joint was immobilized, flexed at 10°, and rotated externally to 10° to 15° with a customized frame during the MRI assessment. The following 2 sequences were obtained for the current analysis: (1) sagittal fast spin-echo proton density-weighted (PDW) sequence (repetition time/echo time: 3000/16 ms; slice thickness/intersection gap: 4.0/1.0 mm; field of view [FOV]: 16 cm; number of excitations: 2; echo train length: 14; bandwidth: ±31.25 kHz/FOV) and (2) fast spin-echo T2-weighted (T2W) sequence (repetition time/echo time: 3000/98 ms; slice thickness/intersection gap: 4.0/1.0 mm; FOV: 16 cm; number of excitations: 2; echo train length: 14; bandwidth: ±31.25 kHz/FOV). The oblique sagittal image was reconstructed by identifying the plane that passed through the centers of the femoral and tibial tunnel outlets, as the primary outcome of follow-up MRI was to evaluate the status of the ACL graft.
We selected the specific slices from all sagittal MRI sequences where we could observe the higher SI of the LM corresponding to the meniscal tear site. All higher SIs on multiple MRI slices were assembled and calculated by averaging the regions of interest in the repaired LM. These selected MRI scans were loaded to ImageJ (Version 1.37c; US National Institutes of Health). The lateral meniscal body was traced on the ImageJ screen, and the SI of the repaired LM was measured. The value for each region of interest of the repaired LM was divided by the value of the posterior cruciate ligament to standardize the SI since the SI of intra-articular tissue is affected by the external environment such as synovial fluid accumulation.14,37 The SI ratio (SIR) was calculated as (SI of the repaired LM)/(SI of the posterior cruciate ligament) (Figure 3). If we observed a higher SI of the repaired LM on 3 sagittal MRI slices, we calculated the SIRs of these 3 slices and used the mean value to conduct the statistical analysis.

Representative example of SI measurement on sagittal MRI scans. Shown are images of the LM (top row) and the PCL (bottom row). LM, lateral meniscus; Max, maximum; Min, minimum; MRI, magnetic resonance imaging; PCL, posterior cruciate ligament; SI, signal intensity; SILM, SI of the lateral meniscus; SIPCL, SI of the PCL; SIR, signal intensity ratio.
The SI was measured on ImageJ by a single orthopaedic surgeon with 13 years of experience (D.C.), who was blinded to the clinical information. Each SIR was measured twice with a 1-week gap between measurements. The intrarater reliability of the determination and calculation of SIR values was calculated on the MRI scans of 30 patients; the intraclass correlation coefficient (ICC) for PDW was 0.855 (95% confidence interval [CI], 0.763-0.914), while the ICC for T2W was 0.846 (95% CI, 0.748-0.908), indicating good agreement. For interrater reliability, an orthopaedic resident with 3 years of experience also measured the SIR of 30 patients; the ICC for PDW sequence was 0.740 (95% CI, 0.525-0.855), while the ICC for T2W sequence was 0.699 (95% CI, 0.336-0.859), indicating moderate agreement.
Clinical Assessment at 12-Month Follow-up
All patients were examined at 12 months postoperatively in our outpatient sports medicine clinic. No independent surgeon examined the same patients consistently. Residual sagittal knee laxity applying manual maximum force was evaluated with a KT-1000 arthrometer (MEDmetric Corp), and the detected side-to-side difference was calculated. The pivot-shift test was used to examine residual ALLx according to the International Knee Documentation Committee (IKDC) grade,15,20 and patients who exhibited a pivot shift of IKDC grade ≥1 were considered as having ALLx.
Statistical Analyses
The demographic data were compared between patients with and those without ALLx using the nonpaired t test or Mann-Whitney U test based on the distribution of the continuous variables and the chi-square test for comparison of categorical variables (ie, sex and morphology of lesion and meniscal tear). Repeated-measures analysis of variance was conducted to compare the SIR values among patients at 3, 6, and 12 months postoperatively. The Pearson or Spearman rank correlation coefficient, according to the distribution of data, was used to assess the correlation between patient age and the SIR of the repaired LM.
To calculate the effect of patient age on residual ALLx, patients were stratified into younger (≤22 years) and older (>22 years) groups. The cutoff age of 22 years was used as it often represents the end of formal education and the beginning of full-time work, with significant changes to activity level and sports participation.6,29 In addition, the cutoff value for the SIR of the repaired LM to predict the occurrence of ALLx was determined using receiver operating characteristic (ROC) curves. Finally, we performed a logistic regression analysis using ALLx prevalence as the independent variable and SIR cutoff as the dependent variable, with adjustments for age, sex, BMI, Tegner score, and time from injury to surgery. All statistical analyses were performed using SPSS (Version 24.0; IBM Corp). Statistical significance was defined as P≤ .05.
Results
Of the 87 included patients, 53 (60.9%) had longitudinal meniscal tears, 22 (25.3%) had radial tears, and 12 (13.8%) had flap tears. Regarding lateral meniscal tear lesions, 72 (82.8%) patients injured their LM on the posterior horn and posterior root; the other 15 (17.2%) were injured on the extended region involving both the posterior horn and the middle body. The morphology and lesion of lateral meniscal tear were unrelated to the prevalence of ALLx and the SIRs of PDW and T2W (Supplemental Table 1). A total of 12 (13.8%) patients demonstrated ALLx at 12 months postoperatively, although no patients with positive pivot shift were observed at 1 month postoperatively. Except for the side-to-side difference in knee laxity, there was no difference in the prevalence of ALLx according to demographic data (Table 1).
Demographic Data of Patients With Versus Without Residual ALLx a
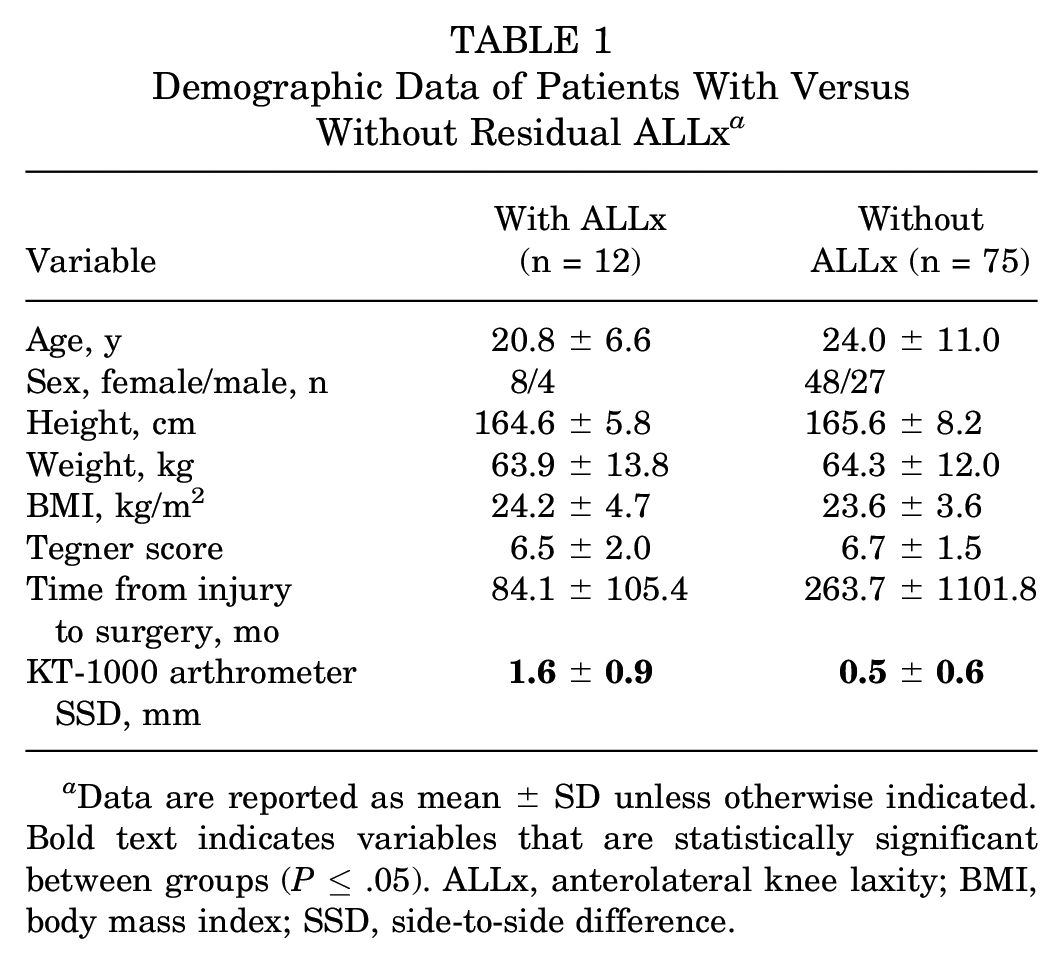
Data are reported as mean ± SD unless otherwise indicated. Bold text indicates variables that are statistically significant between groups (P≤ .05). ALLx, anterolateral knee laxity; BMI, body mass index; SSD, side-to-side difference.
The SIR on PDW MRI (SIR-PDW) in patients with ALLx (1.98 ± 0.77) was significantly higher than in those without ALLx (1.49 ± 0.52; P = .007) at 3 months postoperatively. However, there were no significant differences in the SIR-PDW between patients with and without ALLx at 6 and 12 months postoperatively. SIR-PDW measured at 3 months postoperatively in patients with ALLx was significantly lower than that measured at 12 months postoperatively (Figure 4A). In addition, the SIR on T2W MRI (SIR-T2W) did not differ between those with versus without ALLx on any follow-up MRIs (Figure 4B).
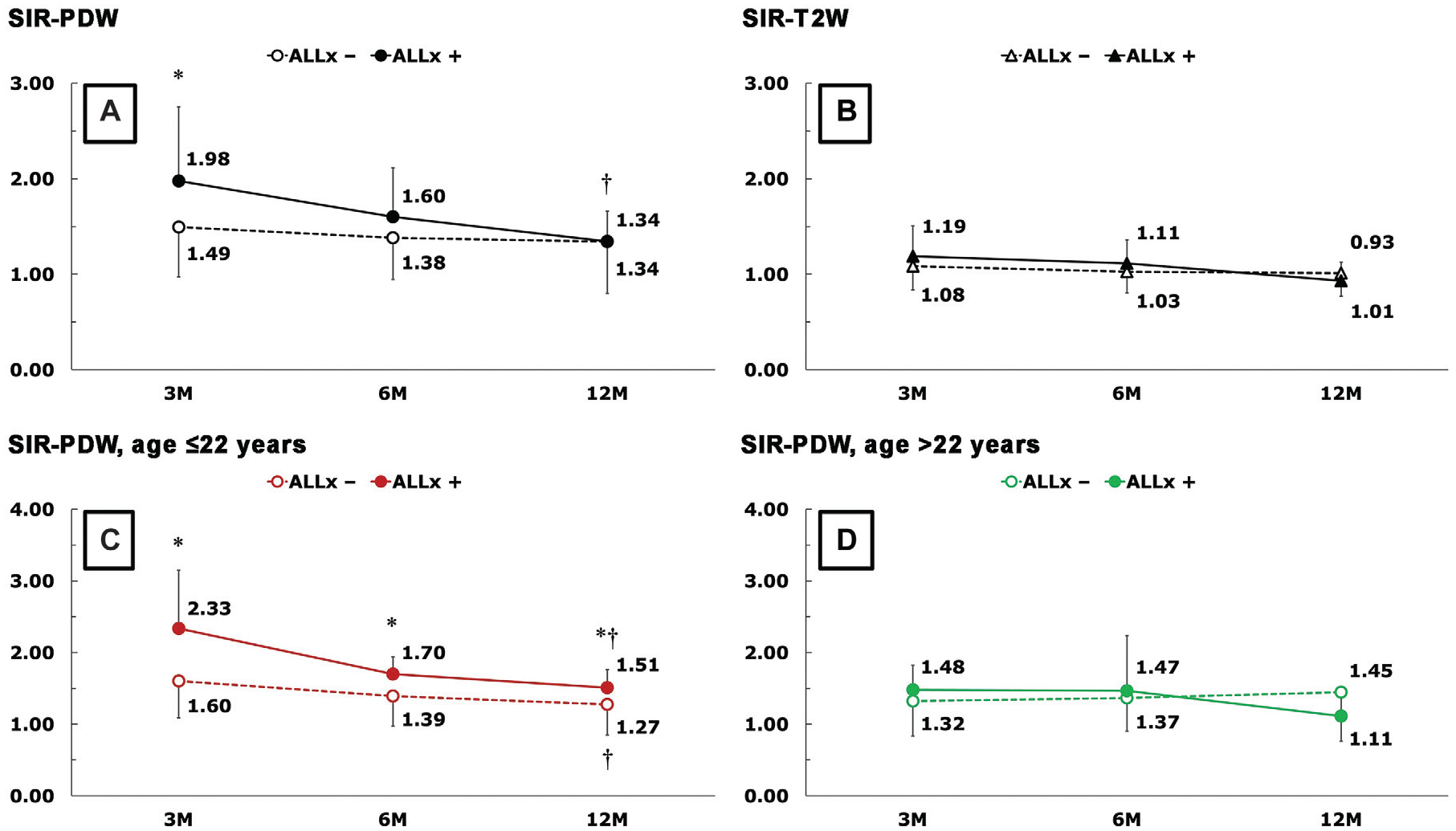
Postoperative SI of repaired LM on PDW and T2W MRI. *Statistically significant difference between groups without (ALLx-) and with (ALLx+) ALLx (P ≤ .05); †statistically significant difference between 3- and 12-month SIR. ALLx , anterolateral knee laxity; LM, lateral meniscus; M, months; MRI, magnetic resonance imaging; PDW, proton density-weighted; SI, signal intensity; SIR, signal intensity ratio; T2W, T2-weighted.
When stratified by age, 53 patients were in the younger group (≤22 years; 7 [13.2%] with ALLx), and 34 patients were in the older group (>22 years; 5 [14.7%] with ALLx). Table 2 provides the demographic data stratified by age-group. SIR-PDW at 3 months postoperatively was correlated negatively with patient age (r = -0.308, P = .004) (Table 3). In the younger group, the SIR-PDW in those with ALLx was significantly higher than in those without ALLx at every follow-up (Figure 4C). However, in the older group, there were no significant differences in SIR-PDW or SIR-T2W between patients with versus without ALLx at any follow-up (Figure 4D).
Demographic Data of Patients According to Age-Group a

Data are reported as mean ± SD unless otherwise indicated. Bold text indicates values that are statistically significant between groups (P≤ .05). ALLx, anterolateral knee laxity; PDW, proton density-weighted imaging; SIR, signal intensity ratio; SSD, side-to-side difference; T2W, T2-weighted imaging.
Correlation Between Signal Intensity of the Repaired LM and Patient Age a

Bold P value indicates statistical significance (P≤ .05). LM, lateral meniscus; SIR-PDW, signal intensity ratio on proton density-weighted imaging; SIR-T2W, signal intensity ratio on T2-weighted imaging.
Spearman correlation coefficient.
The ROC curves for SIR-PDW in the younger and older groups are shown in Figure 5. The area under the curve (AUC) for the younger group significantly predicted the occurrence of ALLx at all follow-up time points (3 months: 0.780 [95% CI, 0.613-0.946]; 6 months: 0.758 [95% CI, 0.616-0.899]; 12 months: 0.733 [95% CI, 0.569-0.897]). In contrast, the AUC in the older group could not predict the prevalence of ALLx. Based on the ROC curves of SIR-PDW in the younger group, the SIR cutoff values were 2.00 at 3 months, 1.50 at 6 months, and 1.50 at 12 months postoperatively (Figure 5A).

ROC curves for the SI of repaired LM on PDW MRI scans to predict the occurrence of residual ALLx in (A) patients ≤22 years old and (B) patients >22 years old. ALLx, anterolateral knee laxity; AUC, area under the curve; LM, lateral meniscus; M, months; MRI, magnetic resonance imaging; PDW, proton density-weighted; ROC, receiver operating characteristic; SI, signal intensity; SIR, signal intensity ratio.
The results of the multiple logistic regression analysis revealed that younger patients who consistently had higher SIR-PDW values than the cutoff were more likely to have residual ALLx (odds ratios, 10.24-23.57) (Table 4). During the 12-month follow-up, 8 of 87 patients consistently had SIR-PDW levels that were higher than the cutoff values. Of these 8 patients, 3 (37.5%) had residual ALLx; however, of the other 79 patients, 9 (11.4%) had residual ALLx at the 12-month follow-up (odds ratio, 4.67; Pearson χ2 = 4.164; P = .041) Moreover, in the younger group, 5 of 53 patients demonstrated consistently higher SIR-PDW values than the cutoff values at 12-month follow-up. Of these 5 patients, 3 (60.0%) had residual ALLx; however, of the remaining 48 patients, 4 (8.3%) had residual ALLx at 12 months postoperatively (odds ratio, 16.50; Pearson χ2 = 10.545; P = .001).
Association Between SIR Cutoff Values and Prevalence of Anterolateral Knee Laxity in Patients Aged ≤22 Years a

3M, 3 months; 6M, 6 months; 12M, 12 months; β, regression coefficient; BMI, body mass index; OR, odds ratio; SIR, signal intensity ratio; SIR-PDW, signal intensity ratio on proton density-weighted imaging.
Adjusted for age, sex, BMI, Tegner score, and time from injury to surgery.
Discussion
The main finding of this study was that a higher SI of the repaired LM as seen on postoperative PDW MRI scans indicated an increased risk of residual ALLx among patients who underwent combined ACLR and lateral meniscal repair. A consistently higher SI of the repaired LM at 3, 6, and 12 months postoperatively demonstrated increased odds of residual ALLx (odds ratios, 10.24-23.57). This finding was statistically significant, especially in patients aged ≤22 years (Figure 4C and Table 4). Therefore, patient age affected the etiology of a higher SI of the repaired LM on PDW MRI sequences.
In this study, the SI of the repaired LM on the T2W MRI sequences demonstrated no significant differences between those with and without residual ALLx, although the SI of the repaired LM on the PDW MRIs did demonstrate differences between these groups. Furthermore, as the follow-up period progressed, the SI of repaired LM on PDW imaging was reduced longitudinally. Similarly, PDW MRIs may have detected the healing process of the repaired LM in patients who underwent anatomic ACLR. Because previous MRI reports included patients who underwent isolated meniscus repair,10,31,43 these studies imply that T2W sequences would be preferable for detecting insufficient healing of the isolated meniscal repair. However, the current study was related to the concomitant lateral meniscal tear with ACL tear: the diagnostic performance to detect incomplete healing of focal LM posterior horn tear concomitant with an ACL tear may be superior on PDW compared with T2W sequences. Moreover, the lower interrater reliability we obtained for calculation of SIR on the T2W MRIs (ICC: 0.699 vs 0.740 for SIR-PDW) may explain the superiority of SIR-PDW for detecting incomplete healing of the repaired LM.
The ALLx after primary ACLR did not improve in some patients in the current study who underwent concomitant repair for a lateral meniscal tear, which contradicted previous time-zero studies in which the simultaneous lateral meniscal repair surgery regulated the ALLx of patients undergoing anatomic ACLR.24,42,46 Regarding the most important finding of this study, the prevalence of residual ALLx increased according to the consistently higher SI of the repaired LM across the 3 timepoints during the initial 1 year after combined anatomic ACLR and lateral meniscal repair. Previous data indicated that the increased signal density of repaired LM on MRI scans corresponded to the incomplete healing of meniscal tissue confirmed by second-look arthroscopy.10,31,43,49 Based on current data, the increased SI of repaired LM has the potential to explain why the repaired meniscal tissue failed to heal and restore its function to stabilize the ALLx after lateral meniscal repair. At the same time, the current data could not exclude the possibility of the other direction: the residual ALLx provokes the nonhealing or delayed healing of the repaired LM. Future longer follow-up study would be needed to clarify the detailed mechanism among the higher SI of repaired LM, the incomplete healing of repaired LM, and the residual ALLx after combined ACLR and lateral meniscal repair.
Another significant finding of this study was that the SI of the repaired LM on PDW MRI was correlated negatively with patient age in the early (ie, 3-month) postoperative stage (r = -0.308, P = .004). The higher SI of the repaired LM, especially in younger patients, showed a significantly higher risk of residual ALLx after anatomic ACLR. However, in the older population, the predictive performance of the repaired LM SI was not significant at 12 months postoperatively. Accordingly, younger age has been associated with a higher risk of residual knee laxity after ACLR.23,48 In line with these previous studies, the results of current study shed light on a novel etiology of the unhealed lateral meniscal tear that causes lateral meniscal dysfunction to stabilize the ALLx after ACLR, especially in younger patients, who are more likely to engage in vigorous physical activity.
Regarding clinical significance, monitoring the SI of the repaired LM on PDW MRI in the younger population may be helpful for predicting the likelihood of residual ALLx after combined ACLR and lateral meniscal repair. Consequently, in some cases in which lateral meniscal function cannot be restored, revision meniscal repair surgery may be required,21,25 or possibly another additional surgery such as anterolateral augmentation or meniscus centralization may need to be performed to prevent residual ALLx after ACLR.12,34
Limitations
The limitations of this study include the following: first, no second-look arthroscopy was performed. Therefore, we could not confirm whether the higher SI of repaired LM grossly demonstrated the unhealed meniscal condition. Second, the follow-up duration was limited to 1 year; thus, the specific mechanism of a higher SI in the repaired LM acting on the residual ALLx for patients with ACLR at ≥2-year follow-up remains unknown. Third, the ACLR graft was an autologous hamstring graft alone. Therefore, we were unable to demonstrate consistent results among patients who received ACLR using a bone-tendon-bone graft. Fourth, patient-reported outcomes were not included. We could not evaluate how the higher SI of repaired LM affects the knee symptoms after combined ACLR and lateral meniscal repair. Fifth, the current MRI scan alignment was built originally to evaluate the status of the ACL graft. Therefore, the MRI slices were created in accordance with the oblique alignment of the ACL graft; the current MRI could not completely trace the alignment of LM. Finally, the ALLx was evaluated only by the IKDC grade of the pivot-shift test. Quantitative evaluations of the pivot-shift phenomenon were introduced recently that demonstrate the mechanism of ALLx before and after ACLR in greater detail.16,28
Despite these limitations, these recent MRI data for patients after combined ACLR and lateral meniscal repair shed light on the new radiological mechanism of the residual ALLx after surgery as well as the clinical relevance of monitoring MRI to predict residual ALLx in the early postoperative phase. Future studies are required to clarify the detailed mechanism behind the SI of the repaired LM on PDW MRI.
Conclusion
In this study, a higher SI of the repaired LM observed on PDW MRI indicated a significantly higher prevalence of residual ALLx after combined anatomic ACLR and lateral meniscal repair in patients aged ≤22 years old. These findings suggest that if younger patients demonstrate a consistently higher SI of the repaired LM during the first postoperative year, they will be at higher risk of residual ALLx at the 12-month follow-up.
Supplemental Material
sj-pptx-1-ojs-10.1177_23259671241241821 – Supplemental material for Association Between MRI Signal Intensity of the Repaired Lateral Meniscus and Residual Anterolateral Knee Laxity After ACL Reconstruction
Supplemental material, sj-pptx-1-ojs-10.1177_23259671241241821 for Association Between MRI Signal Intensity of the Repaired Lateral Meniscus and Residual Anterolateral Knee Laxity After ACL Reconstruction by Daisuke Chiba, Yuji Yamamoto, Yuka Kimura, Eiji Sasaki, Shizuka Sasaki, Eiichi Tsuda and Yasuyuki Ishibashi in Orthopaedic Journal of Sports Medicine
Footnotes
Appendix
Prevalence of residual anterolateral knee laxity and signal intensity of repaired lateral meniscus by meniscal tear morphology a

| Longitudinal tear | Radial tear | Flap tear | ||
|---|---|---|---|---|
| (n = 53) | (n = 22) | (n = 12) | ||
| Prevalence of ALLx | 7 / 53 (13.2%) | 3 / 22 (13.6%) | 2 / 12 (16.7%) | |
| 3 months | PDW | 1.6 ± 0.53 | 1.56 ± 0.74 | 1.4 ± 0.46 |
| T2W | 1.11 ± 0.23 | 1.09 ± 0.29 | 1.08 ± 0.33 | |
| 6 months | PDW | 1.47 ± 0.47 | 1.31 ± 0.33 | 1.32 ± 0.56 |
| T2W | 1.05 ± 0.22 | 1.05 ± 0.21 | 0.95 ± 0.26 | |
| 12 months | PDW | 1.41 ± 0.59 | 1.25 ± 0.35 | 1.22 ± 0.38 |
| T2W | 1 ± 0.27 | 1.01 ± 0.19 | 0.98 ± 0.12 |
The statistical analysis was performed using the chi-squared test and one-way analysis of variance. ALLx, anterolateral knee laxity; PDW proton density–weighted; T2W, T2-weighted image
Final revision submitted September 16, 2023; accepted September 24, 2023.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Hirosaki University Graduate School of Medicine (ref No. 2012-250).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.