
Abstract
Background:
Lateral meniscus posterior root tears (LMPRTs) almost always occur in association with anterior cruciate ligament (ACL) tears. Their repair is advocated to restore the stabilizing and load-sharing functions of the meniscus.
Purpose:
To study the functional outcomes of combined arthroscopic repair of LMPRTs and ACL reconstruction (ACLR).
Study Design:
Case series; Level of evidence, 4.
Methods:
The authors evaluated patients who underwent simultaneous arthroscopic ACLR and LMPRT repair. All patients had chronic injuries, with a mean time since ACL rupture of 7.9 months. Patient characteristics, Lachman and pivot-shift test results, type of LMPRT, associated injuries, and surgery details were documented. Pre- and postoperative functional status was assessed using the International Knee Documentation Committee (IKDC) score, Knee injury and Osteoarthritis Outcome Score (KOOS), and Lysholm score. An independent single-tunnel transtibial repair using 2 SutureTapes was performed for Forkel type 1 and 3 tear root avulsions, while side-to-side suture repair was performed for type 2 radial/oblique tears. The Wilcoxon signed rank test and minimal clinically important difference (MCID) of the IKDC score were used for statistical analysis.
Results:
Included were 25 patients with a mean age of 29.6 ± 6.5 years. Of these, 22 patients (88%; 95% CI, 73.1%-100%) had a high-grade (grade 2 or 3) preoperative pivot shift. Diagnosis of the LMPRT on magnetic resonance imaging (MRI) scans was possible only in 5 patients (20%). At final evaluation, performed at 37.4 ± 7.1 months postoperatively, all functional scores had improved significantly from preoperatively: IKDC score, from 47.6 ± 9.5 to 81.8 ± 11.5; KOOS, from 45.5 ± 10.9 to 86.5 ± 10.3, and Lysholm score, from 49.0 ± 11.5 to 88.8 ± 7.6 (P < .001 for all). Twenty-four patients (96%) achieved the MCID for the IKDC score. All knees had a negative pivot shift at final analysis, and no patient underwent revision ACLR or LMPRT repair.
Conclusion:
LMPRT repair combined with ACLR led to good short-term clinical outcomes in this study. An LMPRT may frequently go undetected on preoperative MRI scans, but a high-grade pivot shift is present in a large majority of these patients.
Keywords
Meniscal injuries are frequently associated with anterior cruciate ligament (ACL) tears, and the reported incidence at the time of arthroscopy varies widely from almost 31% to 80%. 14,23 The lateral meniscus is more mobile than the medial meniscus and is more frequently injured in association with an acute ACL tear. 26,41 Lateral meniscus posterior root tears (LMPRTs) also occur more commonly in association with ACL tears (5%-10% of ACL tears) than as isolated lesions (<1% of all LMPRTs). 3,6,35 The posterior root attachment of the lateral meniscus is located posteromedial to the lateral tibial eminence apex, anterior to the posterior cruciate ligament (PCL) tibial attachment, and anterolateral to the medial meniscus posterior root attachment 18 (Figure 1). The mechanism of injury as proposed by Forkel and Petersen 8 is an anterior translation and external rotation of the tibia. The resultant traction on the posterolateral meniscus root leads to its rupture in association with the ACL tear.
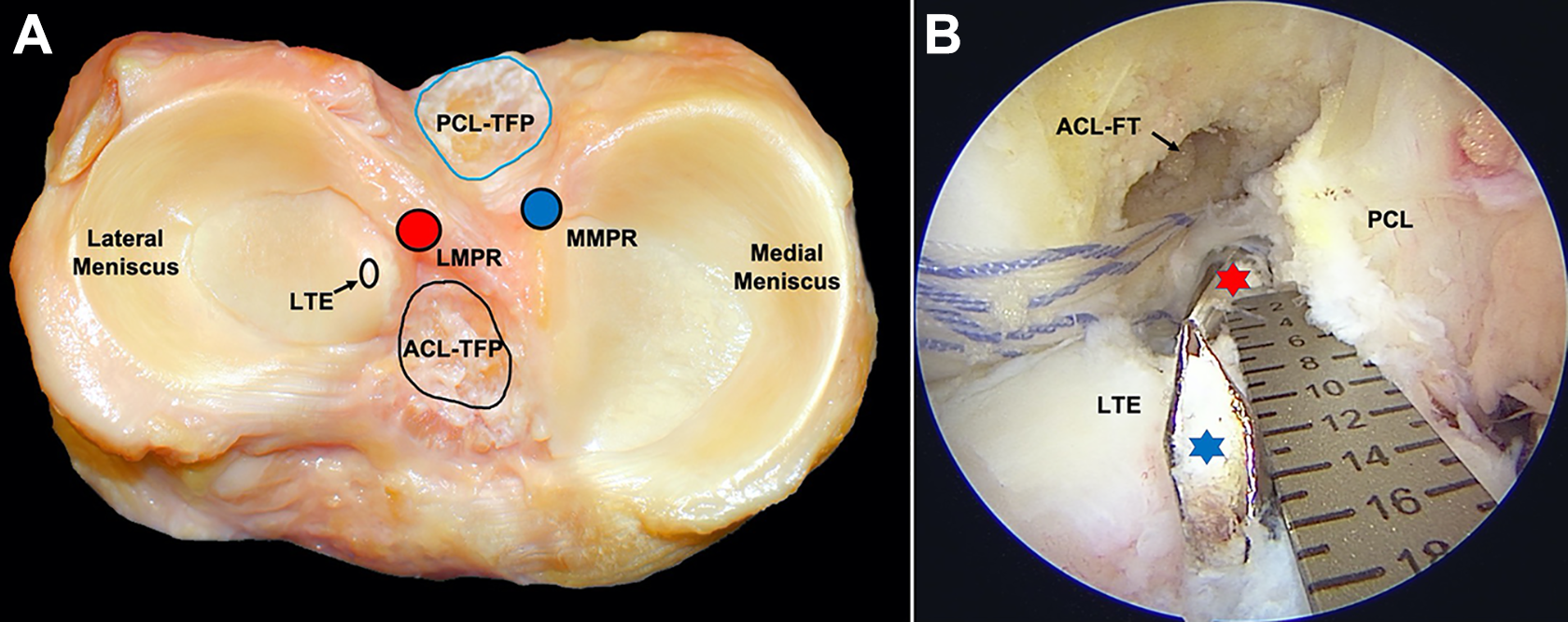
Anatomy of lateral meniscus posterior root (LMPR). (A) Cadaveric axial image. The location of the LMPR (red circle) and medial meniscus posterior root (MMPR) (blue circle) and their relationship with the anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL) tibial footprints (TFPs) are seen. (B) Arthroscopic image, viewing from the anteromedial portal with the knee in 90° of flexion. A drill pin at the center of ACL-TFP (blue star) is about 15 mm anteromedial to the drill bit at the LMPR attachment site (red star). FT, femur tunnel; LTE, lateral tibial eminence. [Figure 1A courtesy of Dr Charles H. Brown Jr, International Knee and Joint Center, Abu Dhabi, UAE.]
The biomechanical consequence of LMPRT in an ACL-deficient knee is a decrease in contact area and increase in mean and peak lateral compartment contact pressures. This effect is more pronounced at higher flexion angles. 2122,29 Additional injury to the meniscofemoral ligaments (MFLs) leads to a further increase in lateral compartment contact pressure. 7 Lateral meniscus extrusion is also seen in association with this injury pattern, especially when there is a complete tear involving both the direct LMPRT attachment and the MFL. 19,35 In addition to load sharing, the integrity of the posterior root of the lateral meniscus is critical for aiding rotational stability.
There is good evidence from cadaveric studies demonstrating the restoration of knee kinematics when the LMPRT is repaired. Transtibial repair of the LMPRT in association with ACL reconstruction (ACLR) can restore tibiofemoral contact mechanics, improving stability on anterior translation and pivot-shift loading at lower flexion as well as internal rotation at higher flexion angles. 7,12,29,33,38 In robotic testing on human cadaveric knees, an untreated posterolateral root tear has been shown to result in increased anterior tibial translation on application of anterior force after an ACLR. 38 Reduction in the sagittal plane lateral meniscus extrusion and subsequent delay of degenerative joint disease has been clinically demonstrated after concomitant ACLR and LMPRT repair. 1,28
The present study was performed to assess the functional outcomes of combined arthroscopic repair of an LMPRT with ACLR in consecutive patients who were evaluated with this injury combination.
Methods
A prospective study including patients operatively treated for a combined ACLR and LMPRT repair at a single center between March 2016 and August 2018 was undertaken. Institutional review board approval was obtained before commencement of the study (No. ONPH/BHRC/02/16022016). Written informed consent was obtained from all patients who agreed to participate in the study. The inclusion criteria were (1) age >18 years, (2) concomitant ACL tear and LMPRT diagnosed on preoperative magnetic resonance imaging (MRI) scan and/or at arthroscopy, and (3) a contralateral healthy knee. The exclusion criteria included (1) revision ACLR, (2) multiligament knee instability, and (3) coronal plane malalignment sufficient to warrant osteotomy. Patients requiring treatment of any other meniscus or cartilage lesion were not excluded. Thirty-one patients were included, but only 26 who consented for participation were enrolled in the study. One patient was lost to follow-up and excluded from the final analysis.
Data Collection
Preoperative patient data, details about mechanism of injury, and duration since injury were noted. A contact injury was defined as direct trauma to the knee sustained as a result of participation in any sport, sustaining a fall, or a motor vehicle accident. All other patient-reported outcome measures (PROMs) were assessed using the International Knee Documentation Committee (IKDC) score, 15 Knee injury and Osteoarthritis Outcome Score (KOOS), 32 and Lysholm score. 40 Examination under anesthesia was performed, and the Lachman test and pivot-shift laxity were graded using IKDC scores. 17 Intraoperative data including LMPRT type (as classified by Forkel and Petersen 9 ) (Figure 2), technique of LMPRT repair, and associated medial meniscus or articular cartilage surgery performed were collected. The Forkel and Petersen classification was used as it is specific for LMPRT only and takes into consideration the integrity of MFL as well. Postoperatively, all patients were followed up after 3 weeks, 6 weeks, 3 months, and every 6 months thereafter. PROMs were assessed at the end of 1 and 2 years. ACL graft laxity was assessed on clinical examination using Lachman and pivot-shift tests in the clinic by an independent examiner (A.S.). All patients were followed up for a minimum of 24 months postsurgery.

Types of lateral meniscus posterior root (LMPR) tear as described by Forkel and Petersen. 9 (A) Type 1 tear in a left knee, with avulsion of the root from its tibial attachment (red oval) but intact meniscofemoral ligaments (MFLs). (B) Type 2 tear in a left knee, with a complete radial tear within 1 cm from the intact root attachment in the tibia (red oval). (C) Type 3 tear in a right knee, with complete avulsion of the root from its tibial attachment (red oval) with separation of the MFLs from the meniscus. LMPH, lateral meniscus posterior horn; LTE, lateral tibia eminence.
Surgical Technique
Examination under anesthesia was followed by diagnostic arthroscopy. Any medial meniscus or cartilage pathology was treated first. The knee was then placed in the figure-of-4 position to effectively view and assess the LMPRT from the anterolateral portal. Probing was performed to check for the status of the MFLs. The choice of ACL graft (bone–patellar tendon–bone [BPTB]) or 5-strand hamstring tendon (HT) graft was determined using tibial footprint measurement and activity type. Patients with an ACL tibial footprint width >10 mm and those engaged in contact sports were selected for a BPTB graft. The ACLR femoral tunnel was drilled at the mid-anteromedial bundle footprint using the transaccessory medial portal technique. The LMPRT was repaired after this according to type. For type 2 radial tears, side-to-side repair using 2 No. 0 FiberWire sutures (Arthrex) was performed using the Knee Scorpion (Arthrex) self-suture retrieving device. The knots were tied on the superior or inferior surface of the meniscus in order to achieve a simple-suture configuration (Figure 3). For types 1 and 3 tears, a bony bed was created at the center of the anatomic root attachment site using a curette and shaver. A meniscus root repair guide (Arthrex) was inserted from the anteromedial portal, and a transtibial tunnel was created using a 4.5-mm drill bit over a 2.4-mm passing pin. A No. 0 FiberWire was passed using a Knee Scorpion device (Arthrex) through the meniscus root. A SutureTape (Arthrex) loop was then shuttled across to achieve a luggage-tag stitch through the root. The step was repeated so as to have 2 tapes passing through the root. The ACL tibial tunnel was then drilled at the center of the ACL footprint. Special care was taken to maintain an adequate bone bridge between the lateral meniscus root repair and ACL tunnels on the tibial cortex. The 4 SutureTape ends were retrieved through the transtibial lateral meniscus root repair tunnel and tied over a 4.5-mm postfixation screw (Biotek) with the knee in 30° of flexion (Figure 4). Finally, the ACL graft was passed and fixed with the knee in 20° to 30° of knee flexion. HT grafts were fixed in the femur using a cortical button (Endobutton CL Ultra; Smith & Nephew) and in the tibia using an interference screw (Biosure HA; Smith & Nephew). BPTB grafts were fixed in the femur and tibia using a titanium interference screw (Softsilk; Smith & Nephew). Lateral extra-articular tenodesis (LET) using a graft of iliotibial band via the modified Lemaire technique 4 was additionally performed for 5 patients who had a high-grade (grade 2 or 3) pivot-shift and were engaged in contact sports or had generalized ligament laxity and >5° of knee hyperextension.

Repair technique for type 2 tears. (A) A type 2 tear of the left knee posterolateral root as seen from the anteromedial portal and probed from the anterolateral portal. (B) A No. 0 FiberWire being passed through the medial portion of the root tissue using a Knee Scorpion device. (C) Sutures passed through the medial and lateral portions of the root. (D) The completed repair using 2 simple-suture configurations. (E) Schematic diagram showing the repair construct. LFC, lateral femoral condyle; MFL, meniscofemoral ligament.

Repair technique for type 1 and 3 tears. (A) The arm of the root repair jig placed at the site of anatomic attachment in the right knee. (B) A suture loop is passed through a tunnel drilled at this site. (C) A No. 0 FiberWire being passed through the root using a Knee Scorpion device. (D) Two loops of SutureTape across the posterolateral meniscus root. (E) The ends of SutureTapes and shuttling suture are retrieved via the anterolateral (AL) portal. The anterior cruciate ligament jig for the tibial tunnel is inserted via the accessory anteromedial (AAM) portal, and care is taken to maintain adequate bone bridge on the tibial cortex. (F) The torn root after repair at its anatomic site. (G) Schematic diagram showing the repair construct of the transtibial technique using a postfixation screw. AM, anteromedial; LTE, lateral tibia eminence.
Rehabilitation
A phased program was initiated postoperatively. 25 All patients wore an extension knee brace and were non-weightbearing for the first 4 weeks after surgery, followed by progression to full weightbearing after 6 weeks. Passive range of motion from 0° to 90° was allowed immediately postoperatively for 4 weeks. Endurance training was begun after 10 weeks, and strength training was begun after 16 weeks. Squatting was limited to 70° in the initial 4 months. Running was allowed after 5 to 6 months, and those engaged in sports activities were allowed to return to play only after 9 to 12 months.
Statistical Analysis
The data analysis was performed using Excel 2010 software (Microsoft Corp) and Stata software Version 15.01 (StataCorp). Qualitative data variables are expressed as frequency and percentage, while quantitative data variables are expressed as mean and standard deviation or median and range (minimum-maximum). The continuous variables were analyzed using nonparametric tests. The Wilcoxon signed rank test was used to analyze differences between pre- and postoperative IKDC score, KOOS, and Lysholm score. P < .05 was considered statistically significant with 95% CI.
An a priori sample size calculation was performed based on the minimal clinically important difference (MCID) of the IKDC score, which has been previously determined as 11.5 by Irrgang et al. 16 A 2-tailed independent t test was used, with α level of .05 and 1 – β = 0.80 (to achieve a power of 80%), using the sample mean and standard deviation of IKDC score from this study. A minimum sample of 22 was determined to detect a clinically meaningful improvement in IKDC scores for all patients, irrespective of additional pathology.
Results
Twenty-five of the 26 recruited patients were available at the last follow-up and included in the final analysis. The characteristics and intraoperative details of the patients are provided in Table 1. The mean interval between injury and surgery was 7.9 ± 6.5 months. The right knee was injured in 13 patients, and the left was injured in 12, with 18 patients (72%) reporting a contact injury mechanism. Using the preoperative MRI, we diagnosed an LMPRT in 5 patients and radial/oblique posterior-third lateral meniscal tear in 8 patients. Thus, in almost half of patients (12/25), the LMPRT could only be diagnosed arthroscopically. A high-grade pivot shift was present in 88% of the patients (95% CI, 73.1%-100%). Nine patients had a concomitant medial meniscal tear. These included a ramp lesion in 2, peripheral longitudinal tear in 6, and horizontal cleavage tear in 1 patient. All these tears were repaired, and no meniscectomies were undertaken. One patient underwent subchondral drilling for a 6 × 8-mm grade 4 lesion of the medial femoral condyle, and another patient underwent chondroplasty for a 4 × 6-mm grade 3 lesion of the lateral tibial plateau. A BPTB graft was used for ACLR in 7 patients, and a 5-strand HT graft was used in 18 patients. An LET using a strip of iliotibial band was performed for 5 patients. Partial coalition of tibial ACLR and LMPRT repair tunnels was seen in 3 patients, while a common tunnel was used in 1 patient because of the near-total coalition.
Patient and Clinical Characteristics (N = 25) a
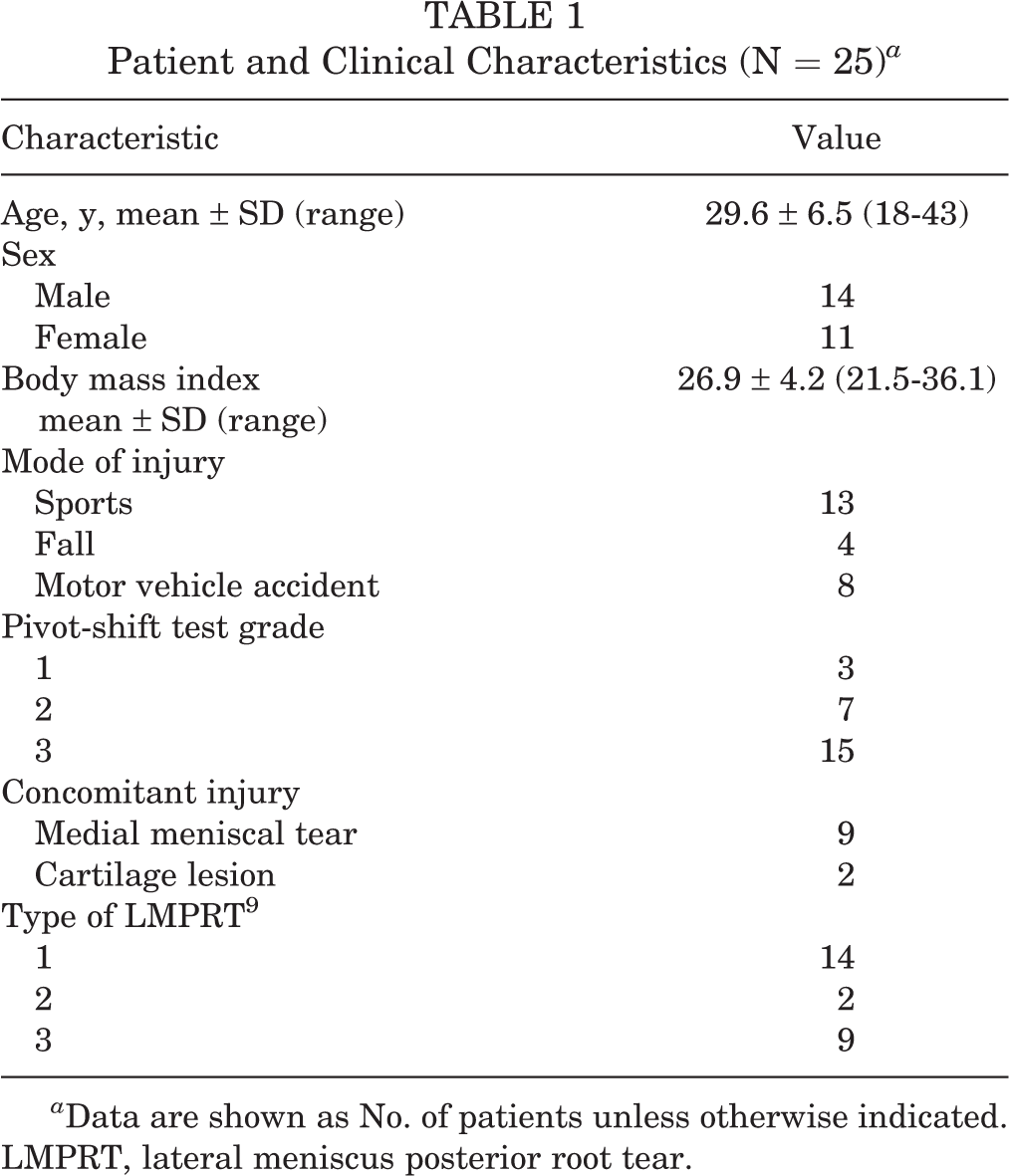
a Data are shown as No. of patients unless otherwise indicated. LMPRT, lateral meniscus posterior root tear.
The 25 patients were followed up for a mean of 37.4 months (SD, 7.12; range, 26-52 months). Negative Lachman and pivot-shift tests were found in all patients at the final follow-up. The change in PROMs is shown in Table 2 and Figure 5. All patients except one had an improvement >11.5 points in IKDC score, which is the threshold for MCID. Preoperatively, 10 patients were grade C (abnormal) and 15 were grade D (severely abnormal) on objective IKDC grading. At the final follow-up, 14 were grade A (normal), 10 were grade B (nearly normal), and 1 was grade C. Preoperatively, 3 patients had fair and 22 had poor scores per the Lysholm grading system. This improved to 11 patients with excellent and 7 each with good and fair scores at the final follow-up. One patient underwent surgery at 14 months to remove a painful postfixation screw. Arthroscopic assessment of this patient revealed a healed repair of the LMPRT.
Patient-Reported Outcome Measures a

a Data are reported as mean ± SD (range). IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score.
b All scores were significantly different between preoperative measurement and final follow-up (P < .05, Wilcoxon signed rank test).

Patient-reported outcome measures. A box-and-whisker plot showing the pre- and postoperative patient-reported outcome scores. X represents mean, the middle lines represent median, the boundaries of the box represent inter-quartile range, and the whiskers represent minimum and maximum values, respectively. IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score.
Discussion
The most important outcome of this study was that combined arthroscopic ACLR and repair of an LMPRT resulted in significant improvement of PROMs at an average of 37.4 months (minimum, 2 years) of follow-up in 96% of patients. A definitive MRI diagnosis of an LMPRT preoperatively was possible only in a minority of patients. The preoperative high-grade pivot shift present in 88% of our patients could have been due to the contribution of the tear of the posterolateral meniscus root causing anterolateral rotatory instability in an ACL-deficient knee. This is, to the best of our knowledge, the first report of clinical outcomes of repairing LMPRTs using an independent tunnel drilling technique.
There are several risk factors for an LMPRT along with an ACL tear. Participation in contact sports and the presence of a concomitant medial meniscal tear were identified as independent risk factors in an epidemiological study of 3956 patients by Praz et al. 30 Okoroha et al 27 found an association between LMPRTs and abnormal varus of the tibia, higher posterior tibial slope, and higher body mass index. A majority of the study participants (72%; 18/25) sustained a contact injury, while a concomitant medial meniscal tear was present is 9 patients (36%). The mean body mass index of patients in this series was 26.9 ± 4.2, which is also in the “overweight” category. Most ACL tears occur in noncontact injuries. Della Villa et al 5 found that 88% of ACL tears in a cohort of professional soccer players had a noncontact or indirect contact mechanism. Therefore, since the present study of ACL tears with LMPRTs had 72% of patients with contact injury, which is much higher than the 12% mentioned in the aforementioned study, there may be an association between contact injury, the extra violence involved, and an LMPRT.
In a cadaveric experiment using infrared camera motion analysis, Shybut et al 36 demonstrated that the mean anterior tibial translation of the lateral tibial condyle significantly increased on pivot-shift loading when the lateral meniscus posterior root was avulsed compared with an isolated ACL-deficient state. Forkel et al 11 additionally demonstrated that while an isolated root tear increased internal rotation laxity at 60° and 90° of knee flexion alone, additional injury to the MFLs increased this instability at all flexion angles. Clinical studies have also demonstrated that a complete LMPRT in the presence of an ACL tear is an independent risk factor for the prevalence of high-grade (grades 2 and 3) anterolateral rotatory instability, especially in injuries >12 weeks. 24,37 Although there is evidence from cadaveric studies 11,22,29,36 on the detrimental biomechanical effects of an LMPRT in an ACL-deficient knee and the benefit of repairing that lesion, clinical data on the management and outcomes of this injury complex are sparse.
Ahn et al 1 reported a series of 25 patients who underwent all-inside side-to-side suture repair of LMPRT along with transtibial ACLR. There was significant improvement in the IKDC and Lysholm scores of all patients at a mean of 18 months postsurgery. A second-look arthroscopy was performed in 9 patients, 8 of whom had complete healing of the root repair 1 of whom had an incompletely healed but stable meniscus. MRI scans revealed statistically significant reduction of meniscus extrusion in the sagittal plane but not in the coronal plane. 1 Anderson et al 2 performed transtibial repair of LMPRTs in 16 patients using the ACL tibial tunnel for the LMPRT fixation sutures. They reported a mean Lysholm score of 86.1 ± 13.3 and mean IKDC score of 84.3 ± 17 after a mean 53.6 months of follow-up. There were 2 repair failures, one of which was due to a reinjury. These subjective outcome scores are similar to those attained in the present study, where all patients but one had significant improvement in knee function that was clinically meaningful per the psychometric analysis of the IKDC system. Thus, it is evident that repair of LMPRT in association with ACLR is associated with significant improvement in knee function, although variables such a medial meniscus repair or performance of an extra-articular tenodesis need to be considered where appropriate.
In a retrospective comparative study of 31 LMPRTs that underwent transtibial repair versus matched 31 tears that were treated nonsurgically, Pan et al 28 reported higher IKDC and Lysholm scores in the repair group. Although this difference was not statistically significant, a higher rate of radiographic arthritis (6 mild, 8 moderate, and 2 severe) after a minimum 2-year follow-up was seen in those whose LMPRTs were not repaired. The relative contribution to improved knee function reported in the present study from the ACLR and repair of LMPRT is, however, impossible to assess. A level 4 systematic review of 9 nonrandomized studies with 215 patients reported favorable functional outcome after combined ACLR and LMPRT repair with a meniscus healing rate >90%. 42 However, in a long-term study, Shelbourne et al 34 reported that subjective outcomes were not significantly different in patients whose LMPRT was left untreated compared with a matched control group with intact menisci. The mean IKDC score after 10 years was 84.6 ± 14 in the LMPRT group. These scores are slightly higher than those from our study. A significantly greater reduction in radiographic lateral joint space was found in patients whose LMPRTs were unrepaired in that study, which could reflect secondary lateral chondral overload and failure over a long duration. 34
The MFLs play an important biomechanical role in the presence of an LMPRT. 13 It is for this reason that we prefer the classification system proposed by Forkel and Petersen 9 for devising a treatment plan, as other systems do not account for the MFLs. 1 Fifty-six percent (14/25) of patients in this study had a type 1 tear, while 36% (9/25) had a type 3 tear. This contrasts against an incidence of 43.8% (14/32) of type 1 and 15.6% (5/32) of type 3 tears reported by Forkel and Petersen. 9 Transtibial pull-out repair is recommended for these tear types. 7,22 Forkel and colleagues 9,10 have advocated the use of the ACL tibial tunnel or, in the double-bundle ACLR technique, the posterolateral bundle tibial tunnel for passing the fixation sutures through the tibia. They also demonstrated in a cadaveric experiment that an independent tibial tunnel for the posterior root is not necessary. 7 Although a biomechanically sound option, such a technique does not restore the anatomic attachment of the lateral meniscus posterior root. LaPrade et al 22 have demonstrated that nonanatomic medial meniscus root repairs do not restore contact area or pressure in the medial compartment. Therefore, the surgeon (S.T.) whose patients were included in the present study prefers to drill an independent tunnel for type 1 and 3 tear repairs rather than simply using the ACL tibial tunnel. Drilling of 2 tunnels in proximity is difficult, and some degree of coalition was seen in 20% (5/25) of patients in the present series. Type 2 tears are technically challenging to repair because of a small medial remnant (root attachment). A transtibial repair is not ideal for this tear type since it would require a nonanatomic repair, with fixation at the medial limit of the larger lateral meniscus remnant. Side-to-side repair of the meniscus in this scenario has been shown to have good outcomes by Ahn et al. 1 However, these repairs may be vulnerable to a higher failure rate since the construct concerned is more vulnerable with loading.
The lateral meniscus is a known secondary restraint to anterolateral tibial motion in the pivot-shift phenomenon. 24,36,37 A high-grade pivot shift seen in 88% of patients in the current series also affirmed this phenomenon. Medial meniscus ramp lesions, high tibial slope, and damage to the anterolateral soft tissues also contribute to the magnitude of pivot shift, and the mere presence of a high-grade pivot shift is not specifically related to LMPRTs. However, since using preoperative MRI for diagnosing LMPRTs is still challenging owing to its low sensitivity, whenever a high-grade pivot shift is found, the surgeon should consider the possibility of LMPRT. Qian et al 31 reported MRI scans could detect only 33% of LMPRTs in a series of 45 arthroscopically confirmed tears. 20 Lateral meniscus extrusion >1.1 mm may be an indirect predictor of an LMPRT, if the tear is not clearly visualized. This is, however, not a sensitive indicator in case of a partial tear or when the MFL is intact. 19 In the present series, only 13 patients (52%) had a preoperative MRI report of a tear in the posterior lateral meniscus, 5 of which were diagnosed as definitive root tears and 8 of which were diagnosed as a posterior horn tear. Therefore, failure to examine the posterolateral root adequately via probing during arthroscopy may result in a missed diagnosis of an LMPRT in almost half of patients. A missed LMPRT is a known factor in the ACLR graft failure. 39
This study has several limitations. First, while the outcomes presented are encouraging, the follow-up is short-term, and sustained improvement in functional outcomes and future chondral deterioration needs to be assessed on longer follow-up. Second, no instrumented laxity measurements pre- and postoperatively were available to assess the effect of the LMPRT and its repair on laxity. However, none of the patients reported instability or had excess ACL laxity on clinical examination at the final follow-up. Third, the long interval between injury and surgery makes it difficult to pinpoint if the lateral meniscus root tore at the time of index trauma or during subsequent episodes of instability. Fourth, different types of repairs were used for various tear patterns, thus making the cohort less homogeneous, but this reflects the spectrum of LMPRTs. Fifth, no MRI scan or second-look arthroscopy was performed to evaluate the healing of LMPRT repairs. Finally, there was no control group with which to objectively compare the outcomes of surgery. However, this was because the authors believe that a tear of the lateral meniscus root should always be repaired, in view of existing evidence of its role in knee stability and function.
Conclusion
Arthroscopic repair of an LMPRT combined with ACLR led to good clinical outcomes in the short term. An LMPRT may frequently go undetected on preoperative MRI scans, but a high-grade pivot shift is present in the majority of these patients.
Footnotes
Acknowledgment
Final revision submitted November 18, 2021; accepted December 8, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.T. has received grants from Zimmer Biomet and personal fees from Arthrex, ConMed, Smith & Nephew, Stryker, and Zimmer Biomet. A.W. has received grants and personal fees from Smith & Nephew and has shares in Innovate Orthopaedics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Biomedical and Health Research Committee for Sahyadri Hospitals.