
Abstract
Background:
Lateral meniscal posterior root tears (LMPRTs) affect knee stability and load distribution. LMPRT repair with anterior cruciate ligament reconstruction (ACLR) demonstrated favorable functional outcomes and a high meniscal healing rate. However, most studies have reported only short-term follow-up results.
Purpose:
To evaluate the long-term clinical and radiologic outcomes of LMPRT repairs with ACLR.
Study Design:
Case series; Level of evidence, 4.
Methods:
Inclusion criteria consisted of patients who underwent LMPRT repair and hamstring ACLR from 2005 to 2019. Exclusion criteria were patients without postoperative magnetic resonance imaging (MRI), patients followed for <4 years, and patients who had reinjury. Healing of the repaired LMPRT was evaluated, and extrusion of the midbody of the lateral meniscus was measured by MRI. Joint space width (JSW) of the lateral compartment on the Rosenberg view was measured and compared preoperatively and at follow-up. Lysholm score and Tegner activity scale were compared between preoperative and follow-up periods.
Results:
Thirty-four patients were included, with a mean follow-up period of 96.8 ± 45.9 months (range, 48-200 months). Tear patterns of the LMPRT were classified into oblique (n = 22) and complex (n = 12) types. Follow-up MRI showed complete healing in 27, partial in 4, and none in 3. Follow-up extrusion was not significantly different from preoperative extrusion (1.31 ± 1.35 mm vs 1.46 ± 1.41 mm, P = .646). Preoperative lateral JSW did not show a significant decrease compared to follow-up lateral JSW (6.2 ± 1.1 mm vs 5.9 ± 0.8 mm, P = .18). Preoperative Lysholm score and Tegner activity scale improved significantly at follow-up (P < .001 and P < .001, respectively).
Conclusion:
At a mean 8-year follow-up, LMPRT repair with ACLR led to significant functional improvement and 91.1% complete or partial healing.
The meniscus is an essential structure that facilitates efficient load-bearing capability of the knee. 15 The meniscal root is crucial to maintain the hoop stress of the knee joint. When a meniscal root tear occurs, axial compressive forces are no longer distributed. 2 A previous study reported that meniscal tears are the most common knee lesion, with meniscal root tears accounting for 10% to 21% of all meniscal tears. 5 Demographic characteristics are different according to the side of the meniscal root tears. Young patients are more likely to have lateral meniscal posterior root tears (LMPRTs), commonly in the setting of multiple ligament knee injuries, knee trauma, or concomitant anterior cruciate ligament (ACL) tears.5,12
Lateral meniscus root tears have gained increased attention over the past decade.6,20,25,34 Biomechanical studies have demonstrated that sectioning the lateral meniscal root results in increased knee laxity, reduced contact area, and increased peak contact pressure.23,27,29 Tang et al 29 demonstrated that lateral meniscus root repair improved ACL graft forces closer to those of the native ACL under anterior tibial loading. A recent systematic review reported that patients exhibited favorable functional scores following lateral meniscus root repair with ACL reconstruction (ACLR), and the side-to-side repair for lateral meniscus root tear demonstrated a high meniscal healing rate (>90%). 33 However, most studies in the systematic review reported only a short-term follow-up. 33 Therefore, long-term clinical studies are needed. 14 The purpose of this retrospective study was to investigate the long-term clinical and radiologic outcomes after LMPRT repairs with ACLR. We hypothesized that LMPRT repairs with ACLR would demonstrate significant improvement in functional outcomes and a high healing rate of the repaired LMPRT.
Methods
Patients
Inclusion criteria were patients who underwent LMPRT repair and ACLR using a quadrupled hamstring autograft from May 2005 to March 2019. Exclusion criteria were patients without postoperative magnetic resonance imaging (MRI), patients followed for <4 years, those with varus/valgus malalignment >3°, or those who experienced reinjury. A control group consisted of patients who underwent isolated ACLR without LMPRT. The control group was matched to the study group on age at surgery, sex, body mass index, and postoperative follow-up period. Written consent was obtained from all patients. The study protocol was reviewed and approved by the institutional review board (EMCS 2023-01-017).
Surgical Procedure
LMPRT repair with ACLR was performed at a single center by a single surgeon (
The affected knee was placed in a figure-of-4 position to repair the LMPRT. For side-to-side repair using an absorbable suture, the arthroscope was introduced through the anterolateral portal, and a 45° curved suture hook (ConMed Linvatec) was introduced through the anteromedial portal. The tip of the suture hook penetrated the medial stump of the lateral meniscus from superior to inferior. A leading end of the absorbable suture was advanced through the medial stump. A leading end of another suture was passed through the lateral side of the root tear from superior to inferior. Using the suture shuttle technique, the all-inside suture repair for the LMPRT was performed as described previously. 4 For side-to-side repair using Fast-Fix (Smith & Nephew), the arthroscope was introduced through the anteromedial portal, and the Fast-Fix device was introduced through the low anterolateral portal. One toggle penetrated the medial stump, and another penetrated the lateral side of the root tear. The Fast-Fix device was retrieved, and the suture was tensioned to close the tear gap.
The semitendinosus and gracilis tendons were harvested and prepared for a quadrupled graft. The tibial tunnel was prepared according to the measured diameter of the quadrupled graft. The 25-mm-long femoral tunnel was drilled through the tibial tunnel at the center of the femoral footprint of the ACL. After pulling the hamstring graft through the tibial and femoral tunnels, the graft was fixed using a cortical suspension device at the femoral side. EndoButton (Smith & Nephew), TightRope (Arthrex), and GraftMax (ConMed Linvatec) were used during the study period. After cyclic loading of the graft through the range of motion of the knee, the INTRAFIX tibial sheath and screw (DePuy Mitek) were inserted into the tibial tunnel while the knee was flexed at 20° of flexion. Partial weightbearing using a hinged knee brace was permitted as soon as possible postoperatively. Closed kinetic chain exercises were started as early as possible. Full weightbearing was permitted 6 weeks after surgery. Jogging and leg press began after 12 weeks. Return to sports activity was allowed after 10 months.
Postoperative Evaluation
Clinical outcomes were evaluated using the Lysholm score and Tegner activity scale.17,30 Joint space widths of the lateral compartment on the Rosenberg view were measured preoperatively and at follow-up. 19 Magnetic resonance imaging (MRI) at 6 months after surgery was routinely recommended. Most patients declined an MRI at the end of follow-up because they had no symptoms. Follow-up MRI examination was performed using the following sequences: axial proton-density transverse high bandwidth, sagittal T2 turbo inversion recovery magnitude, sagittal turbo spin-echo, and coronal T2 and proton-density sequences. Slice thickness was usually 3 mm. Healing of the repaired menisci was evaluated on sagittal, coronal, and axial planes. Healing of the repaired root tears was graded according to a modification of the MRI classification by Kim et al 11 as follows: healed (presence of root continuity in all coronal, sagittal, and axial planes), partially healed (presence of partial discontinuity in any 1 plane), and not healed (presence of complete discontinuity) (Figure 1A-C). On the coronal view showing the maximum extrusion of the midbody, extrusion was measured as the distance between the outer edge of the articular cartilage of the tibial plateau and the outer edge of the midbody of the lateral meniscus (Figure 2). 3 Measurements of lateral joint space width and meniscal extrusion were performed by an orthopaedic resident (Y.C.S.) who was blind to the study. All measurements were repeated 3 weeks later to calculate the intraobserver correlation coefficient.
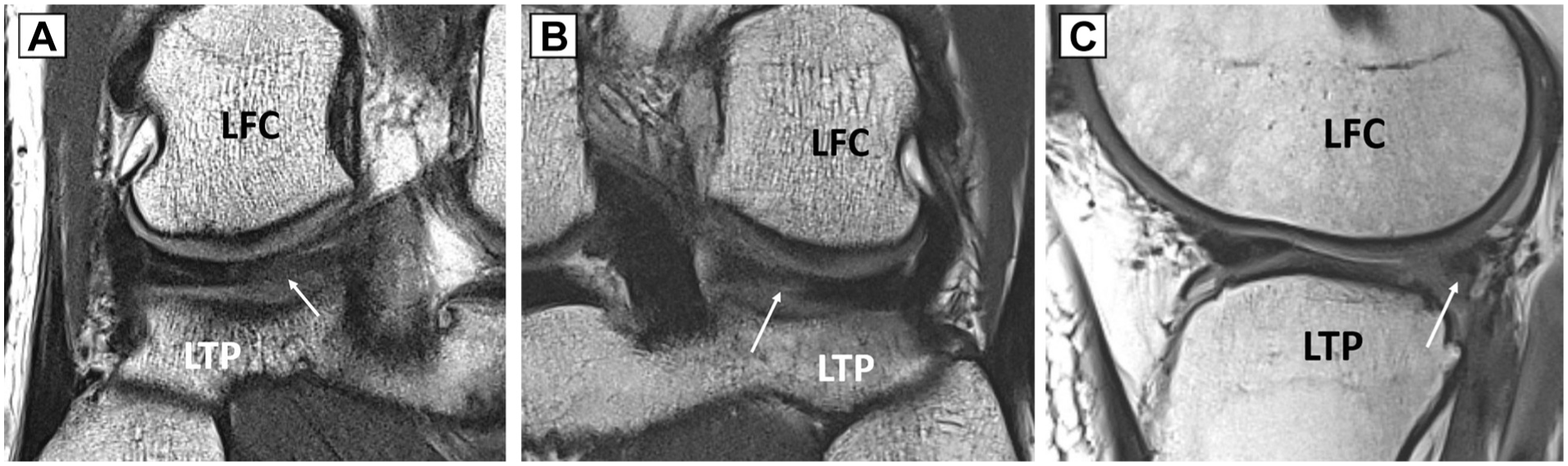
(A) Coronal magnetic resonance imaging (MRI) of the right knee shows a healed lateral meniscal posterior root tear (LMPRT). A white arrow indicates the previous tear site. (B) Coronal MRI of the left knee shows a partially healed LMPRT. A white arrow indicates partial discontinuity of the previous tear site. (C) Sagittal MRI of the right knee shows an unhealed LMPRT. A white arrow indicates an irregular contour of the posterior root of the lateral meniscus. LFC, lateral femoral condyle; LTP, lateral tibial plateau.

Coronal magnetic resonance imaging of the left knee shows measurement of extrusion (*) of the midbody of the lateral meniscus. Extrusion is measured as the distance between the outer edge of the articular cartilage of the tibial plateau and the outer edge of the midbody of the lateral meniscus.
Statistical Analysis
Demographics are expressed using mean and standard deviation. The paired t test was used to compare preoperative and follow-up extrusion, lateral joint space width, Lysholm score, and Tegner activity scale. An independent t test was used to compare the follow-up Lysholm score and Tegner activity scale between the study and control groups. A correlation test was used to investigate any association between the healing of the repaired root, the type of root tear, and the repair method. A correlation test was used to investigate any association between follow-up extrusion and the Lysholm score and the Tegner activity scale. Analysis was performed using SPSS software (SPSS for Windows release 25.0; SPSS), and significance was assumed at .05.
Results
In total, 74 patients were enrolled in the study. Thirty-five patients were followed for <4 years, and follow-up MRI was unavailable for 3 patients. Two patients sustained reinjury during sports. After excluding 40 patients, 34 remained in this study. The patients consisted of 30 men and 4 women, with a mean age of 28.6 ± 10.6 years (range, 13-54 years). The mean follow-up duration was 96.8 ± 45.9 months. Preoperative demographics between the control and study groups did not differ (Table 1).
Preoperative Demographics of the Control and Study Groups a

Values are presented as mean ± SD. BMI, body mass index.
The tear patterns of LMPRTs were classified as oblique and complex types. A total of 22 (64.7%) patients had an oblique tear, and 12 (35.3%) had a complex tear (Figure 3). Among patients with complex tears, 5 had oblique and longitudinal tears (Figure 4A), and 7 had radial and longitudinal tears (Figure 4B). Fast-Fix all-inside repair was performed in 13 patients, and all-inside or inside-out suture repair was performed in 21 patients (Figure 5). Follow-up MRI demonstrated a healed root in 27 patients, a partially healed root in 4, and an unhealed root in 3. Overall, 91.1% (31 of 34) of patients showed partial or complete healing of the root tear. Healing of the repaired root was not significantly associated with tear type or repair method (P = .893 and P = .869, respectively). Healing of the repaired root was not significantly associated with postoperative Lachman or pivot tests (P = .51 and P = .94). Follow-up extrusion did not differ significantly from preoperative extrusion (1.31 ± 1.35 mm vs 1.46 ± 1.41 mm, P = .646). Mean preoperative lateral joint space width decreased slightly at follow-up, but the difference was not statistically significant (6.2 ± 1.1 mm vs 5.9 ± 0.8 mm, P = .18). Intraobserver correlation coefficients for the intraobserver reliability for the extrusion and the lateral joint space width were 0.99 (95% CI, 0.98-0.99) and 0.97 (95% CI, 0.95-0.98), respectively.

An oblique tear of the lateral meniscus root in the right knee of a 23-year-old male patient.

(A) A complex (oblique + longitudinal) tear of the lateral meniscus root in the right knee of a 28-year-old male patient. (B) A complex (radial + longitudinal) tear of the lateral meniscus root in the left knee of a 17-year-old male patient. An asterisk indicates the radial tear, and 2 white arrows indicate the longitudinal tear.
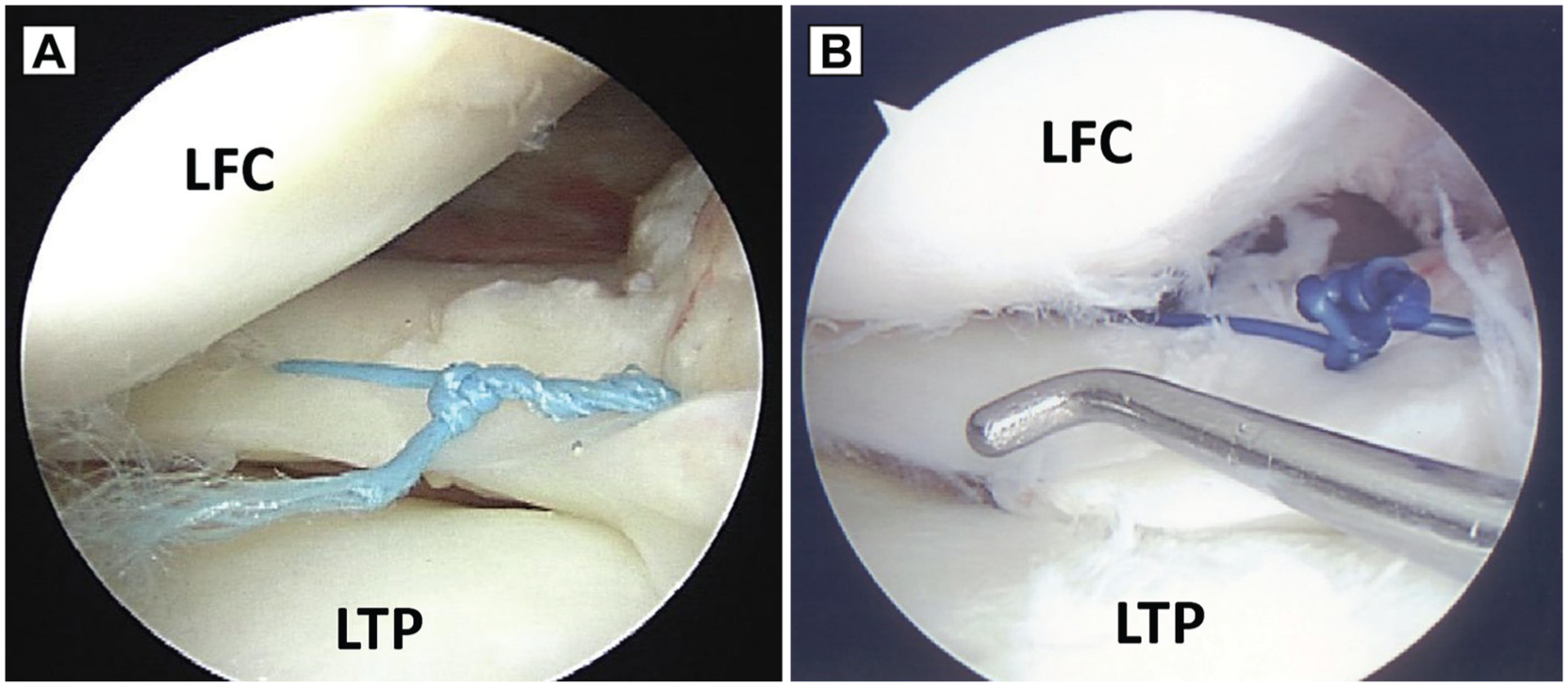
(A) A lateral meniscus root tear in the right knee was repaired using the Fast-Fix (Smith & Nephew) device in a 28-year-old male patient. (B) A lateral meniscus root tear in the right knee was repaired using the all-inside suture technique in a 28-year-old male patient.
Of the patients, 88.4% showed stability, while 11.6% showed grade 1 laxity on the Lachman test. In addition, 92.4% showed stability, while 3.8% showed grade 1 and 3.8% showed grade 2 laxity on the pivot-shift test. Follow-up Lysholm scores significantly improved from preoperative scores (94.6 ± 5.8 vs 60.8 ± 16.7, P < .001), as did the Tegner activity scale (6.3 ± 1.1 vs 2.1 ± 1.0, P < .001). Of the patients, 94% achieved the minimal clinically important difference for the Lysholm score above 8.9 points, and 100% achieved the minimal clinically important difference for the Tegner activity scale above 1 point, respectively. 32 Follow-up extrusion did not correlate with either the Lysholm score or the Tegner activity scale (P = .378 and P = .977, respectively). There was no significant difference in follow-up Lysholm scores or Tegner activity scales between the study and control groups (P = .676 and P = .070, respectively).
Discussion
The most important finding of this study was a significant improvement of patient-reported outcomes (PROs) following LMPRT repairs with ACLR at a mean 8-year follow-up. Of the patients, 91.1% showed a partially or completely healed root tear. Healing of the repaired root was not associated with either tear type or repair method. Extrusion of the midbody did not increase and lateral joint width did not decrease significantly at follow-up. Our hypothesis was affirmed.
LMPRTs are clinically important because the meniscus serves as a shock absorber and stabilizer for the knee. 13 In the cadaveric knees, LMPRT increases anterior instability, tibial internal rotation, and meniscal extrusion.7,8,27,28 Forkel et al 7 demonstrated that transection of the LMPRT increased internal rotational instability compared with the ACL-insufficient state. Tibial fixation of the lateral meniscus root reduced the internal tibial rotation in all flexion angles. Geeslin et al 8 reported that isolated lateral meniscus root avulsion did not change contact pressure or area. However, lateral meniscus root avulsion, combined with meniscofemoral ligament deficiency, resulted in a significantly decreased lateral compartment contact area and increased pressure compared with the intact state. Smith et al 28 demonstrated that the addition of a lateral meniscus oblique radial tear increased meniscal extrusion and anterior laxity for both the anterior drawer and the pivot-shift tests compared with an isolated ACL tear.
Outcomes for repairs in LMPRTs are biomechanically superior to leave-alone treatment. 27 However, repairs for radial tears at the posterior horn need to be performed with caution. The inside-out or all-inside repair technique at the posterior horn has a high risk for vascular injury.18,24 Given the potential risk of popliteal artery injury, nonoperative treatment may be an alternative to repair for the LMPRT. Nonoperative treatment for LMPRTs at the time of ACLR is rarely reported in the literature. Two studies reported an overall range in mean change of Lysholm score of 25 to 40 in patients undergoing nonoperative treatment of the LMPRTs.10,22 Keyhani et al 10 reported a similar International Knee Documentation Committee (IKDC) subjective score and Lysholm knee score after 2 years between the 2 groups: ACLR with nonoperative treatment for LMPRTs and ACLR with LMPRT repair. IKDC and Lysholm scores of patients who underwent ACLR with nonoperative treatment for LMPRTs became significantly worse at mid-term follow-up. Pan et al 22 reported an IKDC score of 86.9 ± 11.5 and a Lysholm score of 87.8 ± 12.0 at 3.2 years after ACLR with nonoperative treatment for the LMPRTs. Shelbourne et al 26 compared long-term clinical and radiologic outcomes between patients who underwent ACLR with nonoperative treatment of LMPRTs and those who had isolated ACLR. A 45° flexed posteroanterior radiograph showed a mean 1.0-mm lateral joint space narrowing in the ACLR with the LMPRT patient group compared with a mean of 0 mm in the isolated ACLR group. Mean IKDC subjective scores at a mean of 10.6 years were 84.6 ± 14.0 in the ACLR with LMPRT group and 90.5 ± 13.3 in the isolated ACLR group (P = .09). Shelbourne et al 26 suggested that patients do well with LMPRTs left in situ, at least at the 10-year follow-up. However, they did not evaluate the healing status of LMPRTs using MRI or second-look arthroscopy.
Recently, repair for LMPRT during ACLR has been reported.1,12,21,31,35 Krych et al 12 reported that the mean IKDC score, Tegner activity scale, and Lysholm score at 41 months following pullout repair for the 30 LMPRTs were 89.5, 6.5, and 93.9, respectively. Okazaki et al 21 reported IKDC scores and mean meniscus extrusion at 6 months after LMPRT repairs with double-bundle ACLR in 17 patients. Transtibial pullout repairs (T group) for the LMPRTs were performed for 9 patients, and inside-out repairs (I group) were performed for 8 patients. Mean IKDC scores of both T and I groups were 73.0 ± 17.7 and 70.7 ± 16.8, respectively. No significant differences in pre- or postoperative extrusion were found between the 2 groups. Tsujii et al 31 reported that second-look arthroscopy demonstrated complete healing in 18 (60%) patients, partial healing in 9 (30%), and nonhealing in 3 (10%) at 3.4 years after side-to-side repair for the LMPRTs with ACLR in 41 patients. However, they did not report IKDC score or Lysholm scores. Zhuo et al 35 reported that the mean IKDC score, Tegner activity scale, and Lysholm score at 26 months following side-to-side repair for LMPRTs in 29 patients were 91.4, 5.4, and 95.1, respectively. Of the patients, 26 of 29 underwent ACLR concomitantly. Follow-up MRI showed that 28 (96.6%) patients had complete healing, and 1 patient demonstrated an unhealed meniscus. Aga et al 1 reported that the mean Lysholm score and Tegner activity scale were 79.2 and 4.3, respectively, at 26 months after transtibial pullout repair in 18 patients with LMPRTs. Follow-up MRI demonstrated complete healing in 11, partial healing in 5, and no healing in 2 patients. Preoperative Kellgren-Lawrence grade decreased by 0.1 grade at follow-up. 9
Most studies reported clinical outcomes at short-term follow-up after the LMPRT repair, except the study by Krych et al. 12 LaPrade et al 14 stated that the biomechanical evidence supports repair of the LMPRT, but long-term clinical studies are needed. The patients of this study were followed for a mean of 8 years after the LMPRT repair. Long-term PROs were excellent and did not differ from PROs of the isolated ACLR group. Moreover, the lateral joint space did not decrease significantly. Therefore, this study may support the biomechanical superiority of the LMPRT over nonoperative treatment at long-term follow-up.
Several limitations of this study need to be acknowledged. First, there was no control group of patients who underwent nonoperative treatment or partial meniscectomy for the LMPRT. Although a systematic review reported that root repair has superior radiologic and clinical outcomes compared with nonoperative treatment for meniscal root tears, most patients in that review underwent medial meniscus posterior root tear (MMPRT). Thus, to our knowledge, no study comparing repair versus partial meniscectomy for the LMPRT at the time of ACLR has been published. 16 Second, 40 of 74 patients were excluded because they were followed <4 years, their MRIs were unavailable, or they were reinjured during the follow-up period. A high exclusion rate, a possible transfer bias, and a small sample size were limitations of this study. Additionally, it is unknown how much improvement in PROs is due to the ACL reconstruction versus LMPRT repair.
Conclusion
Patients demonstrated significant improvement of PROs following LMPRT repairs with ACL reconstructions at a mean 8-year follow-up. Of the patients, 91.1% showed a partially or completely healed root tear.
Footnotes
Final revision submitted October 28, 2025; accepted November 10, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from Nowon Eulji Medical Center, Eulji University (EMCS 2023-01-017).