
Abstract
Background:
Ulnar collateral ligament (UCL) reconstruction has been the standard surgical intervention for elite male athletes with UCL insufficiency. Recently, UCL repair and augmentation with an internal brace has been increasingly performed.
Purpose:
To evaluate the clinical and functional outcomes as well as return-to-sport rate after UCL repair in female athletes.
Study Design:
Case series; Level of evidence, 4.
Methods:
Included were 15 female athletes (mean age, 16.5 ± 3.5 years) who underwent UCL repair between 2011 and 2021 at a single institution. Data collected included age, sport played, competition level, symptom onset, previous surgeries, mechanism of injury, surgical intervention, and return to sport. Patients were contacted via phone at minimum 24-month follow-up, and postoperative outcomes were evaluated using the Mayo Elbow Performance Score (MEPS) and the Single Assessment Numeric Evaluation (SANE).
Results:
Of the 15 female athletes, there were 4 cheerleaders, 3 softball players, 2 volleyball players, 2 soccer players, 1 gymnast, 1 tennis player, 1 dancer, and 1 javelin thrower. Ten of the 15 athletes (67%) competed at the high school level, 4 (26%) at the collegiate level, and 1 patient (7%) was a recreational volleyball player. In all patients, there was an acute onset of symptoms after injury. Ten patients underwent UCL repair with an internal brace (67% of athletes), while 5 underwent standard UCL repair. The median MEPS for athletes with and without an internal brace was 100 (range, 80-100). There was no significant difference of MEPS (P = .826) or SANE scores (P = .189) between the patients who received an internal brace and those who did not. Thirteen of the 15 athletes (86.7%) returned to sport.
Conclusion:
The UCL injuries in the female athletes in this study were the result of acute trauma. Primary UCL repair, both with and without internal bracing, was an effective surgical treatment for returning these athletes to sport.
The ulnar collateral ligament (UCL) consists of an anterior, oblique, and posterior bundle, with the anterior bundle providing the primary resistance to valgus force through the elbow. 20 The anterior bundle is particularly susceptible to damage in overhead athletes, with the most research being carried out on baseball pitchers since the late-cocking and early acceleration phase of throwing place tremendous valgus strain across the joint. 18 Overhead athletes who sustain chronic microtrauma to the UCL can develop chronic valgus extension overload syndrome. 20 However, athletes and nonathletes alike can injure the UCL via complex elbow trauma causing rupture. UCL injuries are often initially treated nonoperatively (eg, bracing, physical therapy, and orthobiologics).14,19 Patients who fail nonoperative treatment may warrant surgical intervention (ie, repair or reconstruction augmented by autograft or allograft). 11
UCL reconstruction was first described by Jobe et al 15 in 1986. UCL reconstruction has been highly successful, with Cain et al 4 reporting 83% (610/733) of patients returning to sport after a 2-year follow-up. Mean time to return to sport after UCL reconstruction is 11.6 months in athletes ranging from recreational to major league pitchers, and 17.1 months at the professional level.4,6 UCL repair was first described by Norwood et al 17 in 1981 as an open procedure consisting of the placement of sutures to reinforce the damaged native ligament. Savoie et al 21 modified this in 2008 by using suture anchors, with a high rate of success. The novel UCL repair augmented with an internal brace was first described by Walters 27 in 2016. Supplementation with an internal brace is aimed at enhancing elbow stability while the ligament heals. 28 This technique, made possible by advancements in drilling, anchoring, and biomaterials has made the repair comparable if not superior to reconstruction in specific patient populations.9,16 The decision to proceed with repair over reconstruction is patient dependent, and direct intraoperative visualization to evaluate the ligament is often built into the decision making. 28 Patients with relatively heathy tissue who had an acute traumatic injury may be better candidates for repair, while patients with chronic laxity and thoroughly damaged ligaments may be better suited for reconstruction. Thus, it is important to consider mechanism of injury when deciding between procedures.
Numerous studies have described outcomes after UCL reconstruction in male overhead athletes; however, there is a paucity of data on the management of UCL injuries in female athletes.2,10,12,24 A 2008 systematic review of 8 studies investigating UCL reconstruction in overhead athletes reported that 4 out of 493 (0.008%) athletes were women. 26 Gardner et al 13 reviewed 15 of the largest UCL outcome studies and found that 79 out of 1902 (0.04%) patients who underwent treatment for a UCL injury were women. Interestingly, these studies most often report UCL reconstructions rather than repairs. The purpose of this study was to evaluate the clinical and functional outcomes as well as rate of return to sport after UCL repair in female athletes.
Methods
After obtaining institutional review board approval for the study protocol, we retrospectively reviewed the medical records of all female patients (n = 18) who underwent surgery for a UCL injury by 2 fellowship-trained shoulder and elbow surgeons (M.J.O., F.H.S.) at a single institution between 2011 and 2021. Nonathletes (n = 3) were excluded from the study, resulting in a final cohort of 15 patients.
After physical examination and imaging, including magnetic resonance arthrogram (MRA), operative intervention was indicated in all patients after acute traumatic rupture of the ligamentous complex. Thus, after diagnosis, patients forwent nonoperative treatment (eg, physical therapy) before surgery. Indications for UCL repair versus UCL reconstruction were determined on an individual basis. Factors to consider when deciding between the 2 procedures included sex, age, severity of the tear, and demand of athletic activity. UCL repair can be considered in younger patients, with partial tears, with relatively healthy tissue. In contrast, UCL reconstruction may be preferred in treating complete tears, chronic injury patterns, and high-demand athletes. All of the patients who suffered acute tears herein underwent UCL repair.
Surgical Technique
In each case, the patient was placed in the prone position for a diagnostic arthroscopy, with a focus on evaluating the capitellum and lateral ligaments in addition to the posterior compartment (Figure 1, A and B). We typically perform arthroscopy in every athlete's elbow (male and female) to look for additional pathology. After elbow arthroscopy in our female athletes, roughly 70% of the time we have found additional pathology; usually a posterior impact osteochondritis dissecans. This is more common in gymnasts who usually have greater hyperextension than the normal elbow. We manage this pathology with microfracture. Other pathology identified via arthroscopy includes pathologic plica (managed with debridement), and laxity of the radial ulnar head ligament (managed with 1-2 plication stitches of Vicryl [Ethicon] roughly 50% of the time).

(A) Anterior arthroscopic view of the medial elbow. (B) An intact lateral capsule with the capitellum pictured superiorly and the radial head inferiorly. After arthroscopy, the shoulder was internally rotated, placing the hand on an arm board in pronation and with the elbow at 70° of flexion. (C) Open view of the medial ulnar collateral ligament demonstrating a proximal tear. (D) A lateral split made in the ligament showing the normal distal half (inferiorly) and the damaged proximal ligament (superiorly). (E) Global view of the torn medial collateral ligament. (F) View of the proximal anchor of the internal brace inserted with the tape retracted superiorly and the suture inferiorly. (G) The repair suture after being passed through the ligament distal to the tear site in preparation of final repair construct. (H) The complete repair with tape in place. Vicryl sutures were placed to completely close the split.
Once the elbow arthroscopy was complete in the study patients, the shoulder was internally rotated, placing the hand on an arm board in pronation and with the elbow in 70° of flexion. The ulnar nerve was carefully palpated and marked, then a small incision was made from the tip of the medial epicondyle distally for 5 to 6 cm. The subcutaneous tissues were carefully dissected, taking care to identify and protect the medial antebrachial cutaneous nerve. At this point, for proximal tears, the flexor pronator muscle was split, as described by Smith et al. 23 For distal tears, the ulnar nerve was identified just distal to the medial epicondyle and carefully protected while the flexor pronator muscle was elevated exposing the UCL. The ligament was carefully inspected for quality and extent of damage (Figure 1, C -E).
If the tear corresponded to the preoperative MRA findings of either the proximal or the distal end, or the ligament was of good quality, repair was performed. In the early years of this study (2011-2016), this consisted of placing a biocomposite double-loaded anchor (Arthrex). Since 2016, the technique has evolved to utilize the internal brace (Arthrex) as described by Walters et al. 27 For this technique, the same initial approach was made. Once the ligament was exposed, it was split in the middle longitudinally exposing the joint line. The drill holes for both the proximal and the distal anchors were created and tapped and the first anchor was inserted at the site of the tear (Figure 1F). The tear was then repaired using the suture attached to the first anchor. The tape attached to the first anchor was then stretched to the center of the opposite drill hole, and a clamp was placed on the tape. We then measured 16 mm to avoid overtensioning and stress shielding (the depth of the tunnel for the second anchor was 15 mm) and marked the tape. The tape was then placed through the second anchor and was inserted into the drill hole (Figure 1G). Elbow range of motion was evaluated to ensure the tape was not too tight and the ligament was isometric. The anchor was then advanced to complete the repair. Frequently, a few Vicryl sutures were placed to completely close the split (Figure 1H). The ulnar nerve was subsequently re-evaluated to ensure no constriction or subluxation was present.
Postoperatively, elbow range of motion was restricted in a hinged elbow brace between 60° and 90° of flexion. One to 2 weeks postoperatively, patients were allowed elbow movement within the confines of the unlocked hinged brace. Physical therapy began at 2 weeks with the goal of progressively increasing range of motion. At 4 weeks postoperatively, the goal was for patients to be able to fully extend their elbow to 180° within the brace and start full-body conditioning. Strength exercises were incorporated at weeks 6 to 8. Proprioceptive neuromuscular facilitation patterns integrated whole body rehabilitation, and a return-to-hitting program (when appropriate) was initiated at 8 weeks if ultrasound demonstrated satisfactory healing. Gradual return to throwing was started at 12 weeks, followed by complex weightbearing and stretching at 14 to 16 weeks. At 20 weeks postoperatively, patients were allowed to initiate return to competition with proper guidance from the physician and rehabilitation specialists.
Data Collection and Statistical Analysis
The following data were collected for each patient: age, sport played, competition level, symptom onset, previous surgeries, mechanism of injury, surgical intervention, and return to sport. Mechanism of injury was often listed in the patients’ charts. Patients would present to the clinic after having heard a “pop” or feeling their elbow give way acutely, preventing them from continuing their sport. If this information was not found in their chart, they were asked over the phone at 24-month follow-up whether their injury was an acute traumatic injury or whether this was a gradual syndrome of pain and instability that prevented them from playing. There is wide variability in the definition and reporting of return to sport. 8 In our study, return to sport was defined as returning to preinjury level of competition. Return to sport was determined by directly asking patients (yes/no) if they had returned to their sport and whether their elbow prevented them from participating at their desired level of athletic competition.
Each patient was contacted via phone in May 2021, at a minimum of 24 months’ follow-up, to obtain an updated Mayo Elbow Performance Score (MEPS) and Single Assessment Numeric Evaluation (SANE) score.7,25 The MEPS measures elbow function across 4 domains: pain (45 points), stability (10 points), range of motion (20 points), and daily functional tasks (25 points). Scores are categorized as 90 to 100 = excellent, 75 to 89 = good, 60 to 74 = fair, and 0 to 59 = poor. The SANE is a patient's self-rating of one's elbow from 0 to 100. Patients rate their current illness score in relation to their preinjury baseline.
Differences in SANE and MEPS scores in patients who had undergone UCL repair with an internal brace versus without an internal brace were analyzed using the Mann-Whitney U test. All data analysis was conducted with the use of R statistical software (R Foundation for Statistical Computing; Version 4.3.1) with a significance level of .05.
Results
Fifteen female athletes (mean age, 16.5 ± 3.5 years) underwent UCL repair between 2011 and 2021. No patients were lost to follow up. Of the 15 female athletes, there were 4 cheerleaders, 3 softball players, 2 volleyball players, 2 soccer players, 1 gymnast, 1 tennis player, 1 dancer, and 1 javelin thrower. Ten of the 15 athletes (67%) competed at the high school level, 4 (26%) at the collegiate level, and 1 patient (7%) was a recreational volleyball player. The nonthrowing athletes (n = 10; 66.7%) outnumbered the throwing athletes (n = 5; 33.3%) athletes. The throwing athletes consisted of 3 softball players, 1 javelin thrower, and 1 soccer player who also participated in javelin and shot put track events. All throwing athletes injured their dominant arm. However, the soccer player injured her elbow while playing soccer. All patients had an acute onset of symptoms after their injury (Table 1).
Characteristics of the Study Patients (N = 15) a
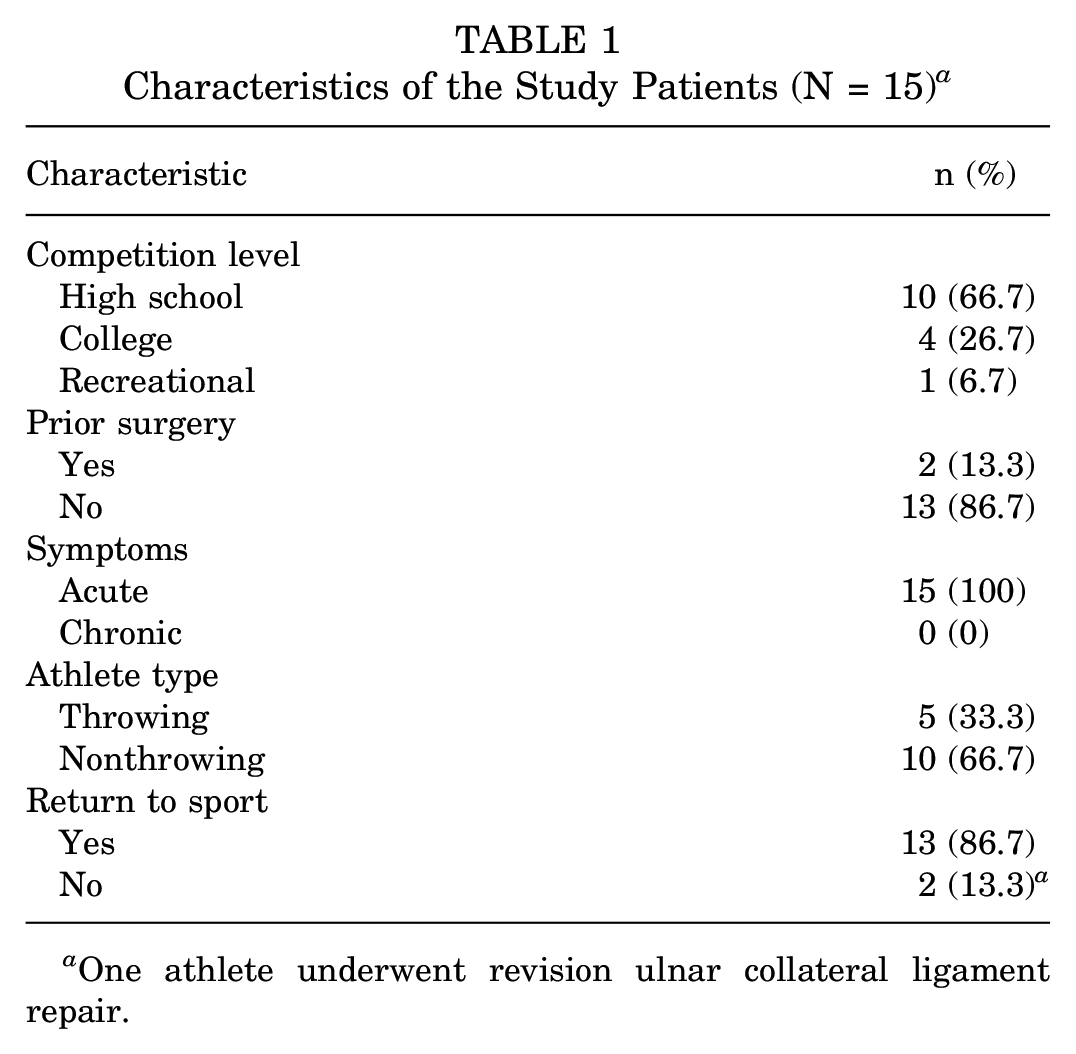
One athlete underwent revision ulnar collateral ligament repair.
Two patients had prior elbow surgery: a softball player who had an ulnar nerve transposition and a dancer who had UCL repair performed by a physician from an outside facility. Thirteen athletes (86.7%) returned to sport after UCL repair. Of the 2 athletes that did not return to sport (13.3%), one was the patient who had previously undergone a UCL repair at an outside institution. This patient had loose bodies identified and subsequently removed from her joint space on arthroscopic examination (Table 1).
The median MEPS and SANE scores overall and according to repair type and prior surgery groups are summarized in Table 2. The median MEPS across all patients was 100 (range, 75-100). There was significant difference in MEPS scores between patients who had undergone prior surgery compared with those who had not (83 vs 100, respectively; P = .033). There was no significant difference in MEPS scores between patients who had received an internal brace versus those who had not (P = .826). The median SANE score for all patients was 85 (range, 60-100). The median SANE score was 77.5 for patients who had undergone prior elbow surgery, while it was 85 for patients with no prior surgery (P = .488). There was no significant difference in the SANE scores between those who received an internal brace compared with those who did not (P = .189) (Table 2).
Postoperative MEPS and SANE Scores a
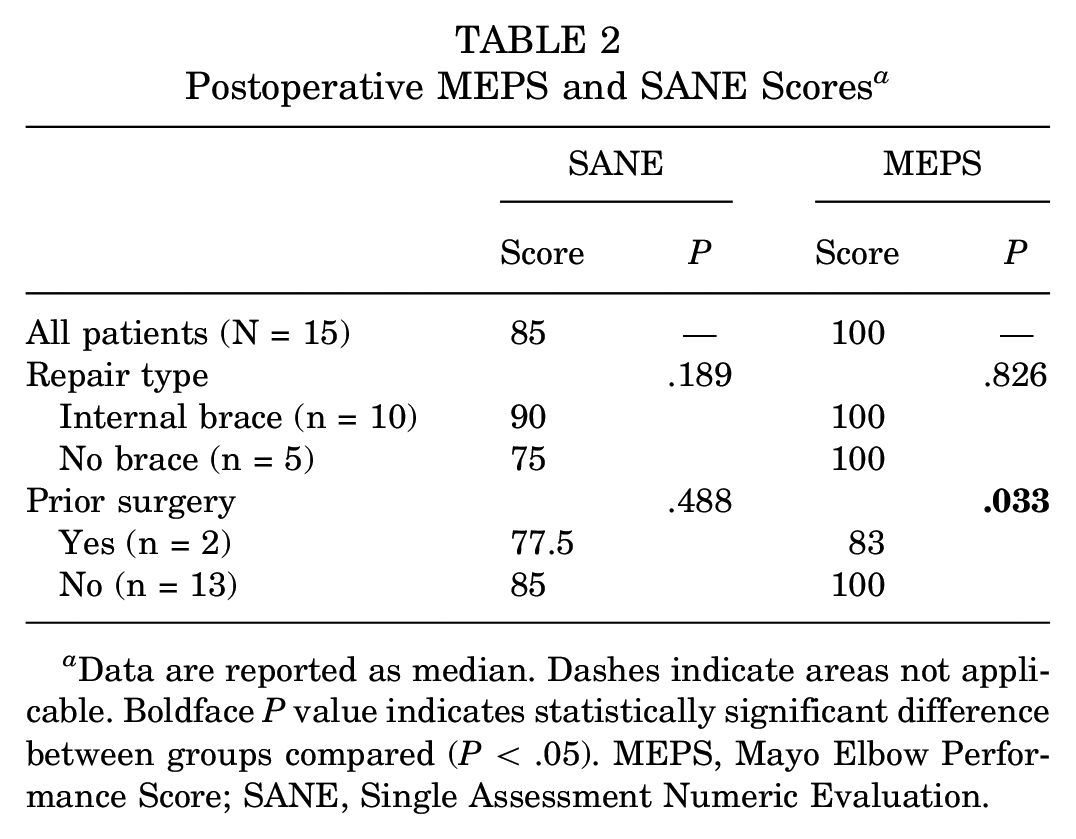
Data are reported as median. Dashes indicate areas not applicable. Boldface P value indicates statistically significant difference between groups compared (P < .05). MEPS, Mayo Elbow Performance Score; SANE, Single Assessment Numeric Evaluation.
Discussion
In the current study, 13 of 15 (86.7%) athletes were able to return to preinjury level of competition after UCL repair, regardless of whether they had internal bracing. Argo et al 1 published the largest detailed study of female athletes with UCL injuries and elbow instability in 2006. These authors evaluated 19 female patients who failed nonoperative treatment and underwent surgical intervention for UCL tears. Eighteen of the 19 patients (95%) underwent repair with a majority (16; 84%) having excellent results, while the remaining 3 patients (16%) had good results. Argo et al found that 17 of 18 athletes (94%) were able to return to competition at a mean of 2.5 months postoperatively, which is less time compared with the reconstruction.2,15,24 Both the 2006 study and our current data show that most patients were able to return to sport after UCL repair.
In our study, 100% of the female athletes experienced acute UCL injury and thus were treated with repair. Interestingly, what is typically seen in the male athlete is a chronic syndrome of ligamentous laxity caused by repeated microtrauma. 20 This results in pain, instability, and chiefly, lack of velocity and control in baseball pitching. We report here that 100% of our patients had an acute onset of symptoms, which is in direct contrast to the chronic syndrome typically seen in male athletes. This dimorphic injury pattern between the sexes warrants further investigation.
The clinical presentation in which female athletes injure their UCL is likely different from that of male athletes for many reasons. Biomechanical studies categorizing baseball and softball pitching have isolated the overall range of motion into 4 phases; windup, stride, delivery, and follow-through. Throughout the progression of throwing, a softball pitch has less force through the elbow compared with a baseball pitch. 3 Moreover, studies have compared elite male baseball pitchers and elite female baseball pitchers directly, to isolate the variable of sport. These reports found women produce fewer proximal forces at the shoulder and elbow with the maximum elbow torque being approximately 75% of male values. 5 Sex-specific differences in ligamentous composition at the elbow may also play a role in the clinical presentation of UCL injuries.
We chose to uniformly evaluate postsurgical outcomes via the MEPS and SANE scores. The MEPS has been shown to be an accurate and reliable tool in assessing patients in orthopaedic sports medicine. 7 Research has shown that when comparing the MEPS and SANE scores in patients with elbow pathology, the strongest correlation was found in female patients. 22 While the SANE score is more subjective (85 across all patients), it closely mirrored our MEPS (100 across all patients) data throughout. It is noteworthy that athletes self-rated their elbow lower than what the MEPS rated their elbow.
Limitations
There are several limitations to this study. First, the sample size was relatively small. Although our cohort of 15 athletes is the second largest cohort of patients examined in this fashion, it still represents only a small fraction of all female athletes. No statistical significance was reached when comparing SANE scores of patients with prior surgery versus surgery-naïve patients, and no statistical significance was reached between outcome scores of repair with versus without an internal brace, which is most likely due to the small patient population. Another limitation is the time frame in which we followed up with our patients. Given that this was a retrospective study, all patients were contacted after their surgery and rehabilitation. We did not track when exactly the athletes returned to sport within the minimum 2-year follow-up. In the future, determining the patient's length of recovery, rehabilitation, and ultimate return to sport would be useful to improve patient care.
Conclusion
The UCL injuries in the female athletes in this study were the result of acute trauma. Primary UCL repair, both with and without internal bracing was an effective surgical treatment for returning these female athletes to sport.
Footnotes
Acknowledgements
Statistical analysis was performed by the Tulane University Translational Science Institute (TUTSI).
Final revision submitted August 27, 2023; accepted September 6, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by the Tulane University School of Medicine ASPIRE summer research fellowship and the Tulane University School of Medicine DeBakey Scholar Program. M.J.O. has received research support from Smith & Nephew, Depuy, and Mitek and consulting fees from Smith & Nephew, DePuy, Mitek, and Stryker. M.K.M. has received education payments from Alon Medical Technology, consulting fees from Arthrex, and nonconsulting fees from Arthrex. F.H.S. has received consulting fees from Exactech, Medical Device Business Services, Smith & Nephew, Zimmer Biomet Holdings, Mitek, and Linvatec; nonconsulting fees from Smith & Nephew and Linvatec; royalties from Exactech, Linvatec, and Zimmer Biomet Holdings; and acquisitions from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Tulane University (ref No. 2020-965).