
Abstract
Background:
Elbow ulnar collateral ligament (UCL) reconstruction (UCLR) is the gold standard for operative treatment of UCL tears, with renewed interest in UCL repairs.
Purpose:
To (1) assess trends in rates of UCLR and UCL repair and (2) identify predictors of complications by demographic, socioeconomic, or surgical center volume factors.
Study Design:
Descriptive epidemiology study.
Methods:
Patients who underwent UCLR or UCL repair at New York State health care facilities between 2010 and 2019 were retrospectively identified; concomitant ulnar nerve procedures among the cohort were also identified. Surgical center volumes were classified as low (<99th percentile) or high (≥99th percentile). Patient information, neighborhood socioeconomic status quantified using the Area Deprivation Index, and complications within 90 days were recorded. Poisson regression analysis was used to compare trends in UCLR versus UCL repair. Multivariable regression was used to determine whether center volume, demographic, or socioeconomic variables were independent predictors of complications.
Results:
A total of 1448 UCL surgeries were performed, with 388 (26.8%) concomitant ulnar nerve procedures. UCLR (1084 procedures; 74.9%) was performed more commonly than UCL repair (364 procedures; 25.1%), with patients undergoing UCL repair more likely to be older, female, and not privately ensured and having undergone a concomitant ulnar nerve procedure (all P < .001). With each year, there was an increased incidence rate ratio for UCL repair versus UCLR (β = 1.12 [95% CI, 1.02-1.23]; P = .022). The authors identified 2 high-volume centers (720 UCL procedures; 49.7%) and 131 low-volume centers (728 UCL procedures; 50.3%). Patients undergoing UCL procedures at high-volume centers were more likely to be younger and male and receive workers’ compensation (all P < .001). UCL repair and ulnar nerve-related procedures were both more commonly performed at low-volume centers (P < .001). There were no significant differences in 3-month infection, ulnar neuritis, instability, arthrofibrosis, heterotopic ossification, or all-cause complication rates between low- and high-volume centers. The only significant predictor for all-cause complication was Medicaid insurance (OR, 2.91 [95% CI, 1.20-6.33]; P = .011).
Conclusion:
A rising incidence of UCL repair compared with UCLR was found in New York State, especially among female patients, older patients, and nonprivate payers. There were no differences in 3-month complication rates between high- and low-volume centers, and Medicaid insurance status was a predictor for overall complications within 90 days of operation.
Keywords
Medial elbow ulnar collateral ligament (UCL) reconstruction (UCLR) is the gold standard for operative treatment of UCL tears, since Frank Jobe’s first technique on the eponymous Los Angeles Dodgers’ pitcher Tommy John in 1974 to later modifications by Andrews and Yocum and the docking technique.2,17,23,27 Early repair techniques led to less than satisfactory results and inferior return to sports rates compared with reconstruction, leading to a relative abandonment of the technique. However, recent technical and implant innovations have led to a resurgence of UCLrepair popularity,8-10,24,29 including popular media, with a recent in-depth article on the repair technique and newer implant technology reported on a prominent sports website. 28
Increasing numbers of young athletes participating and subspecializing in overhead sports, particularly baseball and year-round pitching, have led to an increasing incidence of UCL-related injuries.14,20 A trifecta of studies in the mid-2010s demonstrated rapid growth of UCLRs over time, primarily in the young male population, with overall volume increases of 193% to 343% over a decade depending on the database queried.12,16,21 With recent advancements in anatomic repair sites, suture anchors, and suture-based augmentation, UCL repair has gained recent favor, with a recent Texas-based study demonstrating a 5.4% increase in annual frequency of UCL repair compared with UCLR over the past decade.4,11,18,29 In addition, these specialized procedures are performed more commonly at academic or high-volume centers, with limited access to these procedures in more rural, low-volume centers, which can be exacerbated in states such as New York with a large discrepancy between urban and rural health care access.6,25,26
Epidemiologic trends in UCL repair compared with UCLR, as well as the complication and readmission rates between low- and high-volume centers, remain unknown in New York State (NYS). The purpose of this study was to (1) assess temporal trends in rates of UCLR and repair in NYS between 2010 and 2019 and (2) identify predictors of complications or readmission by demographic, socioeconomic, or surgical center volume factors.
Methods
Cohort Selection
This study was deemed exempt from institutional review board approval, given that all data used were deidentified within existing public databases. Patients who underwent UCL repairs or reconstructions at NYS health care facilities between 2010 and 2020 (the most recent year available) were retrospectively identified using Current Procedural Terminology (CPT) codes 24345 and 24346 within the New York Statewide Planning and Research Cooperative System (SPARCS) database. Revision procedures were excluded. Concomitant ulnar nerve in situ releases and/or transpositions were identified using CPT code 64718. After the initial evaluation, the year 2020 was excluded from analysis given the effect of COVID-19 on both UCL repairs and reconstructions. The SPARCS database collects variables related to inpatient and outpatient stays (ie, diagnoses, treatments, services, complications, and readmissions) from all registered health care facilities within NYS.
Volume Classification and Data Collection
Surgical center UCL-related procedural volumes were totaled for each surgical center in NYS and subsequently classified into 2 categories: low (<99th percentile) and high (≥99th percentile). These percentiles were chosen to divide the total group of NYS surgical centers into 2groups with comparable total case volumes. Case volume by zipcode area was also plotted on a NYS choropleth map.Patient information (age, sex, race, insurance status, and socioeconomic status [SES]) was collected, with SES estimated by the University of Wisconsin School of Medicine and Public Health US Area Deprivation Index (ADI). 19 The ADI metric ranks neighborhood SES by national and state percentiles based on income, education, employment, and housing quality. Lower ADI percentiles correspond to less disadvantaged neighborhoods. The incidence rates of readmissions and complications (wound complications including cellulitis or postoperative hematoma, heterotopic ossification, continued instability or pain, rerupture, and ulnar neuritis) within 90 days of the index procedure were extracted from the SPARCS database using International Classification of Diseases, ninth and 10th Revision, codes. The SPARCS database also contains data on readmissions, postoperative anemia, deep venous thrombosis (DVT) or pulmonary embolism (PE), acute kidney injury, urinary tract infection, cardiac arrest, cerebrovascular accident, myocardial infarction (MI), pneumonia, respiratory failure, and sepsis; however, these were excluded as there were 0 events in NYS within 90 days.
Statistical Analysis
Poisson regression analysis was used to compare trends in UCLR versus UCL repairs as well as the incidence of ulnar nerve-related procedures. Patient characteristics and 90-day incidence rates of complications and readmissions were compared between surgical center volume categories using the chi-square or Fisher exact test. Multivariable logistic regression analysis was used to determine whether center volume, demographic, or socioeconomic variables were independent predictors of complications. Age and ADI were scaled by a factor of 10 before they were entered into the regression model. All statistical analysis was performed in R (Version 4.1.2; R Foundation for Statistical Computing). Statistical significance was set at a P <.05.
Results
A total of 1448 UCL-related surgeries were performed between the years 2010 and 2019, with 388 (26.8%) concomitant ulnar nerve procedures. UCLR (1084 procedures; 74.9%) was performed more commonly than UCL repair (364 procedures; 25.1%), with patients undergoing UCL repair more likely to be older (P < .001), female (P < .001), non-White (P = .005), and not privately ensured (P< .001) and having undergone a concomitant ulnar nerve procedure (P < .001) (Table 1). There was no significant difference in ADI breakdown between UCL repair and reconstruction (P = .473).
Univariate Analysis of Demographics and Insurance Status of UCL Repair Versus Reconstruction in New York State, 2010-2019 a
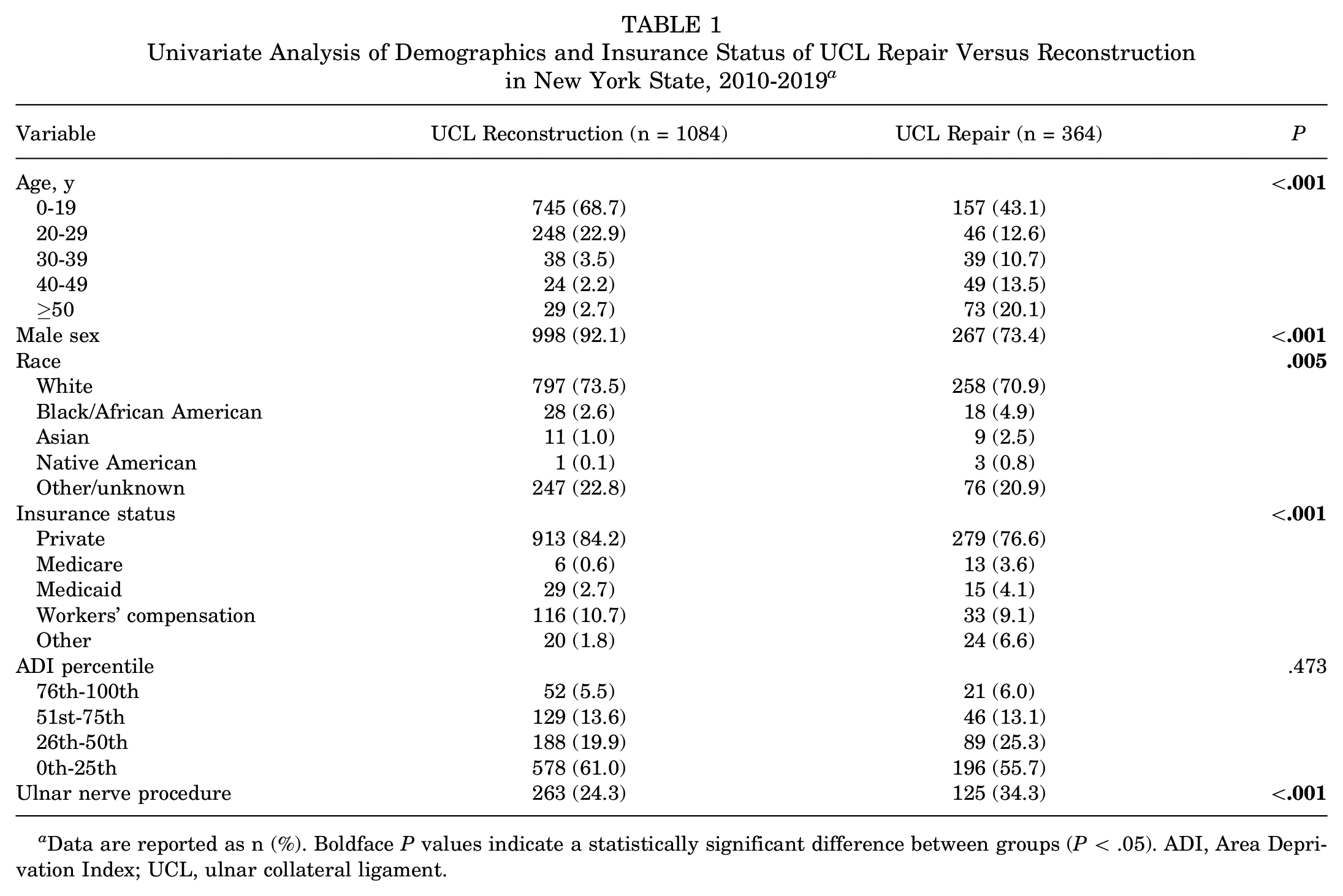
Data are reported as n (%). Boldface P values indicate a statistically significant difference between groups (P < .05). ADI, Area Deprivation Index; UCL, ulnar collateral ligament.
A mean of 108.4 ± 16.9 UCLRs and 36.4 ± 9.5 UCL repairs were performed each year. UCL repairs increased both as a percentage of the total yearly UCL-related procedures, from 21.2% to 30.4%, and as a percentage of total UCL repairs, from 8.0% to 15.4%, across the studied time period. Poisson regression analysis demonstrated that with each progressive year, there was an increased incidence rate ratio for UCL repair versus reconstruction (β= 1.12 [95% CI, 1.02-1.23]; P = .022) (Figure 1).

Temporal trends in ulnar collateral ligament reconstruction and repair in New York State, 2010-2019.
A mean of 38.8 ± 11.9 ulnar nerve-related procedures were performed each year, with no significant difference between repair and reconstruction (P = .738). Poisson regression analysis demonstrated that with each progressive year, there was an increased incidence rate ratio for ulnar nerve-related procedures (β = 1.07 [95% CI, 1.03-1.11]; P < .001) (Figure 2).

Temporal trends in ulnar nerve-related procedures in New York State, 2010-2019.
Two high-volume centers were identified in NYS, performing 720 UCL combined procedures (49.7% of total cases), with 131 low-volume centers cumulatively performing 728 UCL procedures (50.3% of total cases). UCL repairs were performed at a significantly higher rate at low-volume centers (40.0% of total cases) compared with high-volume centers (10.1% of total cases) (P < .001). Concomitant ulnar nerve procedures were performed more commonly at low-volume centers (32.8% of total cases) compared with high-volume centers (20.7% of total cases) (P < .001) (Table 2). The 2 high-volume centers performed a mean of 20.3 and 54.5 cases per year, with totals of 203 and 545 cases over the study period. Low-volume centers performed a mean of <1 to 5.4 cases per year, with a range of 1 to 54 cases over the study period. UCL procedures at high-volume centers were more likely to be performed inyounger patients, with 94.7% of patients younger than 30 years, compared with 70.6% at low-volume centers, and 12.5% of patients older than 50 years old at low-volume centers (P < .001). There was a significantly lower proportion of female patients undergoing UCL procedures at high-volume centers (4.6% vs 20.6%; P < .001); a higher proportion of patients receiving workers’ compensation (14.9% vs 5.8%; P < .001), with no difference in private payers; and a higher percentage of patients from less disadvantaged neighborhoods according to the ADI (P < .001) (Table 2). The geographic distribution of low- and high-volume surgical centers is presented in Figure 3. The 2 high-volume centers were located in New York County (the borough of Manhattan in New York City), whereas low-volume centers were dispersed throughout the entire state.
Univariate Analysis of Demographics and Insurance Status of UCL Procedures at High- Versus Low-Volume Centers in New York State, 2010-2019 a
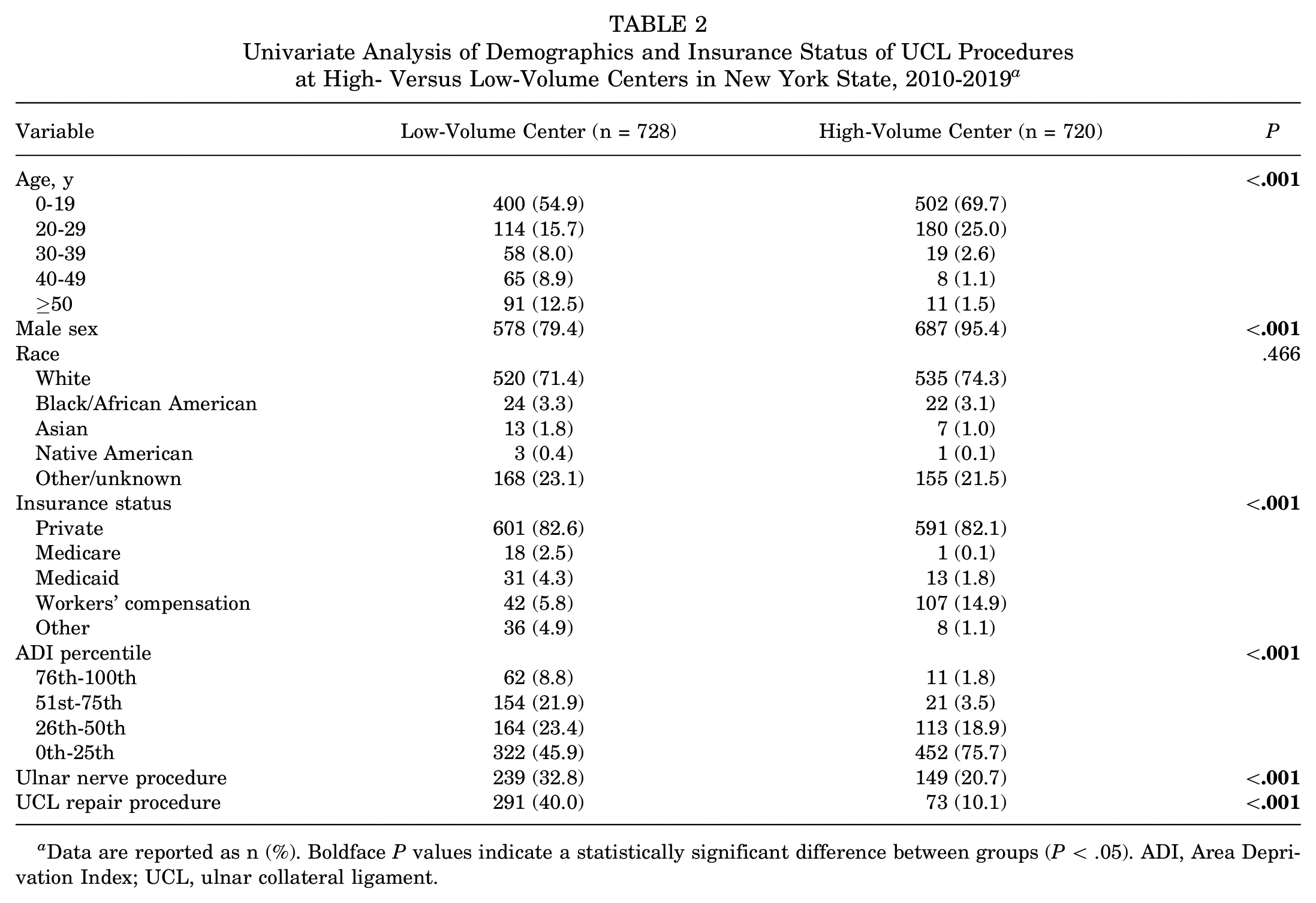
Data are reported as n (%). Boldface P values indicate a statistically significant difference between groups (P < .05). ADI, Area Deprivation Index; UCL, ulnar collateral ligament.

Heat map of high- and low-volume centers performing ulnar collateral ligament procedures in New York State.
There were no readmissions or postoperative anemia, DVT/PE, acute kidney injury, urinary tract infection, cardiac arrest, cerebrovascular accident, MI, pneumonia, respiratory failure, and sepsis complications that occurred within 90 days of surgery in NYS. There were no significant differences between low- and high-volume surgical centers in 3-month postoperative wound complications (including cellulitis, dehiscence, and hematoma), ulnar neuritis, instability, arthrofibrosis, heterotopic ossification, or all-cause complication rates (Table 3). The 2 high-volume surgical centers had 21 events (2.9%) of postoperative partial tear or rerupture compared with 7 events (1.0%) in low-volume surgical centers (P = .012). On multivariable regression analysis, the only significant predictor for all-cause complication was Medicaid insurance status (OR, 2.91 [95% CI, 1.20-6.33]; P = .011) (Table 4).
Ninety-Day Readmissions and Complications After UCL Procedures at High- Versus Low-Volume Centers in New York State, 2010-2019 a
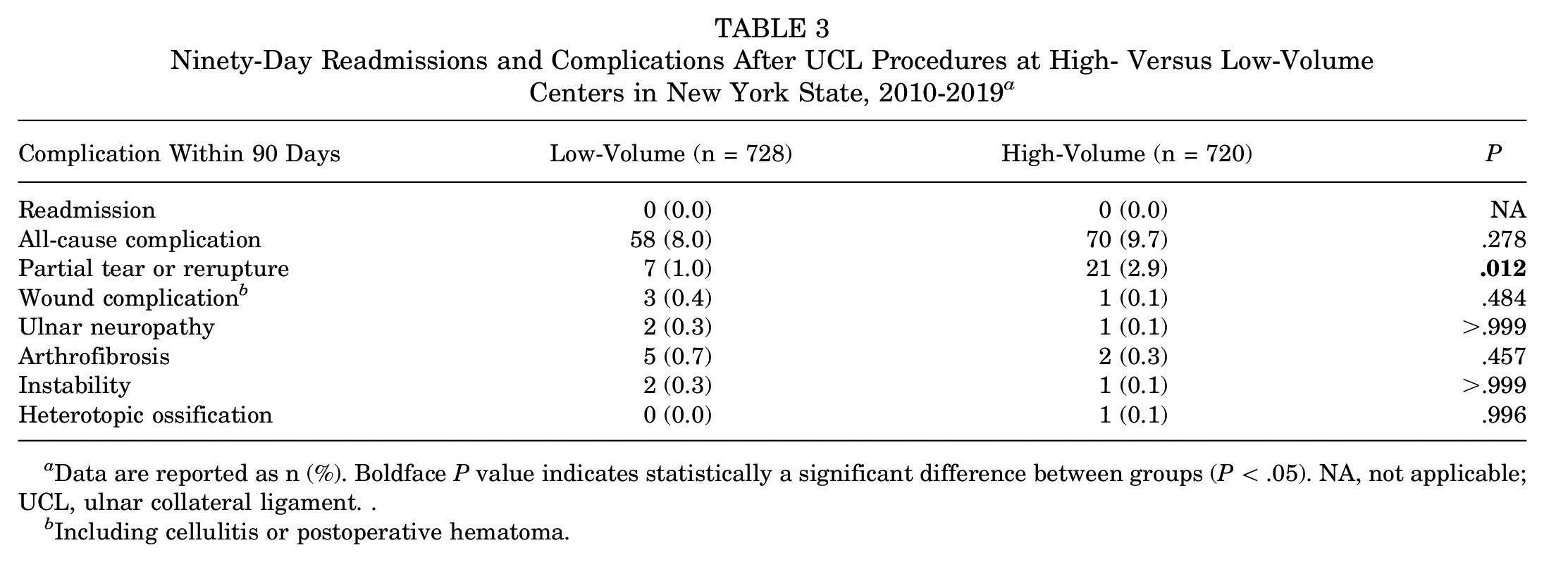
Data are reported as n (%). Boldface P value indicates statistically a significant difference between groups (P < .05). NA, not applicable; UCL, ulnar collateral ligament. .
Including cellulitis or postoperative hematoma.
Multivariable Logistic Regression Analysis of Predictors of 90-Day Complications After UCL Procedures a

Boldface P value indicates statistical significance (P < .05). ADI, Area Deprivation Index; UCL, ulnar collateral ligament.
Discussion
While UCLRs continue to be the overall more common procedure performed for UCL ruptures in NYS, UCL repairs were increasing in usage at a more rapid rate between 2010 and 2019. Ulnar nerve-related procedures have also significantly increased over this study period, with a higher proportion performed concomitantly with UCL repairs than reconstructions. Both UCL repairs and ulnar nerve-related procedures were more commonly performed at low-volume centers than high-volume centers. UCL-related procedures remain extremely safe, with no readmissions or major medical complications within 90 days in NYS. Two centers perform nearly half of the UCL-related procedures in NYS, with the remaining procedures performed by 131 surgical centers, with no significant differences in complication profile except for a higher rate of postoperative pain, partial tear, or rerupture in high-volume centers.
While causality cannot be inferred from our study, the rise in UCL repair frequency is likely because of a variety of factors. As with many cycles in orthopaedics, what is old becomes new again (such as the 1970s anterior cruciate ligament repair of Feagin and Curl 13 ), and UCL repair is no different, with relatively poor return-to-play results reported in early landmark studies by Conway et al 8 and Azar et al 3 leading to repair surpassed by reconstruction techniques. With recent success and biomechanical support reported by Savoie et al 24 and Dugas et al,9,10 UCL repair has returned as a viable option, substantiated by recent literature. Modern techniques using more advanced suture anchor and biological suture augmentation technology have made repair a more appealing procedure, reducing operative time and surgical morbidity compared with reconstructions, as the surgical exposure required is reduced and the need for autograft harvest is obviated. 22 A secondary benefit of UCL repair over UCLR is the shortened time to return to sports, as many players return around 6 to 7 months after a repair compared with 12 to 18 months after UCLR.1,9
We were surprised by our finding of high rates of ulnar nerve-related procedures with UCL repair compared with reconstruction techniques, as the more proximal exposure required around the medial epicondyle for the majority of reconstruction techniques lends itself to identifying, releasing, and/or transposing the ulnar nerve. Procedure popularity also often follows research popularity/productivity, or vice versa, with a recent study by Willenbring et al 29 demonstrating a parallel rise in UCL repair procedures in Texas with recent publications related to UCL repair.
We found that patients undergoing UCL repair in NYS were overall older than those undergoing reconstruction, with >20% older than 50 years old and only 55.7% younger than 30 years old, compared with 91.6% younger than 30 years old undergoing UCLR and only 2.7% older than 50 years old. In addition, a higher proportion of female patients underwent UCL repair (26.6% vs 7.9%) as well as a significant but marginally lower rate of White patients (29.1% vs 26.5%). The younger age of patients undergoing UCLR corroborates prior studies by Erickson et al, 12 Mahure et al, 21 and Cain et al. 5 We hypothesize that the higher proportion of older patients undergoing UCL repair is linked to the decreased morbidity of the procedure and the viewpoint that older patients are likely to place lower demands on their operative elbow, and thus possibly not require the current gold-standard graft reconstruction, similar to many surgeons’ viewpoints on anterior cruciate ligament repair.7,15 The differences between repair and reconstruction in our study contrasted with those in the study by Willenbring et al, 29 in which they found no demographic differences, and likely represents state-to-state differences between Texas and New York.
There was a stark contrast found in UCL procedural volume among surgical centers in NYS, with 2 centers in Manhattan performing a near-equivalent amount to the remaining 131 centers combined. Overall, UCL repair and reconstruction procedures were found to be extremely safe at low- and high-volume surgical centers, with no readmissions or major medical complications such as DVT/PE or MI, and no differences were demonstrated in elbow-related complication rates between low- and high-volume surgical centers. While there was a higher rate of postoperative pain, partial tear, or rerupture in high-volume centers compared with low-volume centers (2.9% vs 1.0%), the overall rate remains low with likely a high fragility of this statistically significant finding, with possible underreporting or underdiagnosis of complications within the SPARCS database from low-volume centers. Recent literature on hip arthroscopy, another relatively subspecialized procedure by Shankar et al, 26 demonstrated contrary results, with higher rates of readmissions, all-cause complications, acute kidney injury, urinary tract infection, DVT/PE, MI, sepsis, fracture, and wound complications at low-volume centers compared with high-volume centers. This may represent a steeper learning curve or technical demand of hip arthroscopy, or a magnified effect of surgical volume given the more central anatomic location of the hip joint compared with the elbow.
UCL procedures performed at high-volume centers were more likely to be in younger and male patients, with 94.7% of patients younger than 30 years old and 4.6% female patients, compared with 70.6% and 20.6%, respectively, at low-volume centers. This was similar to the findings of Shankar et al, 26 with hip arthroscopy in older patients more likely to be performed at low-volume centers. This likely represents a younger, more athletic-minded population seeking out higher-volume surgeons for their procedures, thus concentrating age groups of <20 years old and 20 to 30 years old within high-volume centers. Within our study, there were no differences in private insurance, Medicare, or Medicaid payer status; however, there was a significantly higher proportion of workers’ compensation patients at high-volume surgical centers compared with low-volume centers, which likely represents the higher proportions of professional athletes seeking care at high-volume surgical centers. These results cannot be compared with those of prior epidemiologic studies on UCLR by Erickson et al, 12 as they utilized databases composed completely of privately insured patients; however, a study by Hodgins et al 16 utilizing the same SPARCS database investigating only UCLR (and not UCL repairs) demonstrated that individuals with private insurance were 25 times more likely to undergo UCLR than those with Medicaid, which is consistent with our findings. Using ADI percentiles, in which lower percentiles correspond with less disadvantaged neighborhoods, we found that UCL procedures at high-volume centers were significantly more likely to be performed in those from less disadvantaged neighborhoods than the procedures performed at low-volume centers.
Limitations
There are several limitations of this study. First, as with most database studies, the results are limited to the quality and generalizability of the SPARCS database. As it is primarily a claims database, there are limited demographic and operative variables available for analysis, preventing a more thorough review of procedure information such as intraoperative complications, procedure time, or number of surgeons per surgical center or number of cases performed per surgeon. As it is a single state record, other states or regions may exhibit different practice patterns than those of NYS, limiting the external validity of these findings to the entire US population and UCL procedural trends. The SPARCS database also does not report mechanism of injury; thus, we were unable to investigate whether UCL repairs were more commonly performed in acute traumatic ruptures compared with more chronic overuse injuries with possibly irreparable tissue. Second, with regard to surgical center volume analysis, we were limited by database information from obtaining other determinants of center volume, including surgeons per center and individual surgeon case volume. Third, the time frame of the analysis may not be the most representative of current epidemiology trends, as we were limited on the front end by the implementation of the CPT code for UCL repair (24345), and on the back end by the SPARCS database, which lags a few years and currently reports public data only until 2020, which was excluded because of the onset of the COVID-19 pandemic. The SPARCS database also only reports complications within 90 days of the index procedure, which, while acceptable for some complications, is likely inadequate to accurately represent several complications after UCL surgery.
Conclusion
Within NYS, there is a rising incidence of UCL repair compared with UCLR, especially among female patients, older patients, and nonprivate payers. There were no differences in 3-month complication rates between high- and low-volume centers, with Medicaid insurance status found to be an independent predictor for overall 90-day complications.
Footnotes
Final revision submitted September 23, 2023; accepted October 29, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.S.R. has received education payments from Gotham Surgical and hospitality payments from Arthrex. L.M.J. has received education payments from Arthrex, consulting fees from Flexion Therapeutics, and hospitality payments from Horizon Therapeutics. B.J.E. has received grant support from Arthrex; education payments from Arthrex and Smith + Nephew; consulting fees from Arthrex, DePuy Synthes, and Pinnacle; nonconsulting fees from Arthrex; and hospitality payments from Linvatec and Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.