
Abstract
Background:
Injury of the ulnar collateral ligament (UCL) is common in baseball players. Pitchers are most commonly affected and most likely to have surgery for this injury. The gold standard surgical treatment is UCL reconstruction with autograft; yet, UCL repair with collagen-coated suture tape (ie, internal brace) has shown to be equally effective, and both procedures demonstrate high rates of return to sport and similar postoperative elbow function. However, revision UCL reconstructions have less favorable outcomes regardless of technique.
Purpose:
This pilot case series reports on short-term outcomes of collegiate or professional baseball pitchers whose primary UCL reconstruction failed and who subsequently underwent revision UCL repair with internal brace.
Study Design:
Case series; Level of evidence, 4.
Methods:
A retrospective billing query was performed for patients who had undergone revision UCL repair with internal brace. Patients were eligible for inclusion if they were a pitcher at the collegiate or professional level, were at least 1 year postoperative after revision UCL repair with internal brace, and had a history of ipsilateral primary UCL reconstruction. Clinical and surgical data were collected via electronic medical record review. Outcomes data included return to sport as well as elbow-related function from the American Shoulder and Elbow Surgeons elbow form, Kerlan-Jobe Orthopaedic Clinic score, and Andrews-Carson score.
Results:
A total of 11 pitchers met inclusion criteria (45% professional and 55% collegiate) and had follow-up data collected (mean follow-up time, 2.9 years; range, 1.0-5.0 years). All 11 (100%) were able to return to sport at the preinjury level or higher, and the mean time from surgery to return to competition was 9 months. At follow-up, the mean function score of the American Shoulder and Elbow Surgeons elbow form was 35.8 (out of 36), the mean Kerlan-Jobe Orthopaedic Clinic score was 88.3 (out of 100), and the mean Andrews-Carson score was 95.0 (out of 100).
Conclusion:
This pilot case series shows promising short-term results of using UCL repair with internal brace for high-level pitchers with recurrent UCL injury after UCL reconstruction. Specifically, we found excellent return-to-sport and patient-reported outcomes. Further study is warranted with larger sample sizes and longer follow-up to evaluate outcomes after revision of UCL surgery with UCL repair utilizing internal bracing.
Keywords
The ulnar collateral ligament (UCL) plays a crucial role in maintaining elbow joint stability, especially in overhead throwing activities such as baseball. 24 The biomechanics of the overhead throwing motion places the UCL under supraphysiologic stress and can lead to sprains, tears, and ultimately valgus instability. 17 When nonoperative treatment fails in high-performance overhead athletes, the gold standard surgical treatment has historically been UCL reconstruction with autograft, a procedure known colloquially as “Tommy John surgery.” After primary UCL reconstruction, 80% to 90% of professional baseball players successfully return to sport (RTS) and demonstrate improved elbow-related function. 13 However, despite increasing community outreach and athlete education efforts, UCL injuries are becoming more common, and more baseball players are undergoing primary UCL reconstruction at younger ages.13-15,22 Previous projections have estimated that between 2015 and 2025, the yearly rate of primary UCL reconstruction in patients 15 to 24 years of age would increase by >50%. 22 Given that up to 16% of these primary reconstructions will require revision UCL surgery, there is concern regarding the less favorable outcomes of revision reconstructions.16,23 Current evidence suggests that RTS after revision UCL reconstruction is substantially poorer than primary UCL reconstruction, with studies reporting that 47% to 85% of athletes successfully return. 20 Specifically examining professional pitchers who underwent revision UCL reconstruction, Camp et al 8 reported a mean RTS time of 15 months, with an overall RTS rate of 77% but with only 55% of pitchers returning to the preinjury level of play. Given the increasing rate of primary UCL reconstructions and the likely increase in need for revision procedures, optimization of UCL revision procedures is critical.
Recent advancements in surgical techniques, including augmentation with collagen-coated suture tape (ie, internal brace [IB]), have led to increased interest in UCL repair as an alternative to UCL reconstruction. When possible, repair with IB offers several potential advantages, including preservation of the native ligament, quicker recovery times, and no requirement for a lengthy “ligamentization” process.11,12 Midterm outcomes of UCL repair with IB have been comparable to traditional UCL reconstruction, showing no difference in the proportion of athletes able to RTS at the preinjury level of competition. 10 Despite these results, the decision between primary UCL repair with IB and reconstruction is often dependent on a variety of factors: injury characteristics such as location of tear and severity, an athlete's preinjury activity level, and the timing of injury.2,10-12,29
Outcomes of UCL graft repair with IB as a revision strategy for failed primary UCL reconstructions are not well understood. To our knowledge, in the current literature, there is only 1 small case series presenting outcomes of 6 professional pitchers who underwent UCL graft repair performed by a longitudinal division of the native ligament, then continuous suture to reinforce the ligament. 27 Similar to the spectrum of injuries seen in native UCL ligament, UCL graft failures vary widely, with some graft failures being amenable to repair. The potential benefits of repair include an accelerated postoperative rehabilitation timeline and reduced invasiveness without sacrificing outcomes.5,10,11 This pilot case series aims to investigate the short-term efficacy of UCL repair with IB as a revision procedure for failed primary UCL autograft reconstructions. We hypothesized that UCL repair with IB as a revision procedure would yield similar clinical and RTS success rates as revision UCL reconstructions. This research could help fill a significant gap in the current literature and guide clinicians in selecting the most appropriate operative management of recurrent UCL injuries.
Methods
Patient Population
Following institutional review board approval, we performed a retrospective search via Current Procedural Terminology code 24345 at the Andrews Sports Medicine and Orthopaedic Center in Birmingham, Alabama, to identify patients who underwent UCL repair with a collagen-coated suture tape (IB) between June 1, 2013, and October 1, 2024. Each electronic medical record was reviewed to verify that the potential participant had previously undergone primary UCL reconstruction, subsequently underwent a revision procedure employing the IB repair technique, and was a competitive pitcher at the collegiate or professional level. Our specific inclusion criteria were as follows: (1) a documented UCL repair with IB at our institution after a failed UCL reconstruction within the specified period, (2) status as a competitive collegiate or professional baseball pitcher at the time of revision surgery, (3) at least 1 year of postoperative follow-up, and (4) the ability and willingness to provide informed consent. Athletes competing at the collegiate or professional level were selected for inclusion based on the assumption that their primary UCL surgery was most likely to have been performed by an experienced surgeon at a high-volume institution, which increased the likelihood of appropriate graft preparation and tunnel placement, thus decreasing the likelihood that the primary surgery would negatively affect the secondary repair. All participants were contacted by telephone to obtain their informed consent.
Demographic Information and Patient Evaluation
For eligible athletes, demographic information and injury characteristics were collected via electronic medical record review. Data collected included the date of injury, hand dominance, sport, position, level of athletic competition, and body mass index of each participant at or just before the time of surgery. Tear location, type of graft tear (insufficiency, partial, or complete), and ossicle and osteophyte locations, as well as information regarding any concurrent procedures such as ulnar nerve transposition, were collected from detailed operative reports. If graft tear location and tear type could not be confirmed intraoperatively, preoperative magnetic resonance imaging interpretations were used for classification (Figure 1).

Pre- and postoperative UCL MRI. (A) Preoperative MRI arthrogram: coronal T2 sequences demonstrating a proximal UCL graft tear (arrow). (B) Postoperative MRI arthrogram: coronal T2 sequences demonstrating postoperative healing after UCL graft repair with internal brace augmentation (arrow). MRI, magnetic resonance imaging; UCL, ulnar collateral ligament.
Patient-Reported Outcomes
Eligible athletes were contacted via telephone and asked to complete a series of patient-reported outcome (PRO) measures. The American Shoulder and Elbow Surgeons elbow form (ASES-E) score, Kerlan-Jobe Orthopaedic Clinic (KJOC) score, and Andrews-Carson score were evaluated postoperatively to evaluate pain, elbow function, and satisfaction with the surgical outcome.1,3,9,25 Current ulnar and medial antebrachial cutaneous neuropathy symptoms experienced by the athlete were measured via the sensorimotor subscore of the Patient-Rated Ulnar Nerve Evaluation (PRUNE) questionnaire. 21 Finally, athletes were asked a series of questions evaluating their ability to return to preinjury sport and preinjury level of sport, including time to return to practice and competition, as well as any complications or need for subsequent ipsilateral procedures at outside institutions. PROs could be completed via telephone or electronically, via a REDCap survey, which allowed for secure survey distribution.18,19 All study-related data were collected, combined, and managed by REDCap electronic data capture tools hosted at the American Sports Medicine Institute.18,19
Operative Techniques
All surgical procedures were conducted by a single fellowship-trained sports medicine surgeon (J.R.D.) at the Andrews Sports Medicine and Orthopaedic Center. The operative technique for UCL repair involved the use of a collagen-coated IB, as previously described.10,11,29 The indication for UCL revision via repair with IB augmentation for each patient in this report included the following: (1) high-grade or complete tear of the previous UCL reconstruction from either the origin on the medial epicondyle or the insertion on the ulna and (2) adequate tissue for repair to bone. In each case, the previous incision was utilized and enlarged to allow for our standard approach to the UCL. In cases where the ulnar nerve was previously transposed, the nerve was identified and protected throughout the case. In cases where the nerve had not been transposed at the initial UCL reconstruction, the nerve was identified and freed from its soft tissue restraints to allow for later transposition. The flexor fascia was split in line with the ulnar nerve to expose the underlying sublime tubercle. The flexor mass was elevated from the previously reconstructed UCL to expose the entire ligament reconstruction from origin to insertion. The ligament tissue was split from the apex of the sublime tubercle, in the midsubstance of the ligament, up to the medial epicondyle origin. The tear was identified, and a high-speed bur was used to create a bleeding surface on the bone to improve healing. On the humeral side, a 4.75-mm corkscrew anchor (Arthrex SwiveLock) was used, and a 4.0-mm pilot hole was drilled in the medial epicondyle at the native origin of the ligament. The larger corkscrew anchor was utilized to ensure good purchase in the epicondylar bone in the event of previous tunnel widening. The anchor was placed with collagen-coated FiberTape and 2 No. 0 FiberWire sutures through the islet. Once inserted, the previous reconstruction tissue was repaired to bone using the No. 0 FiberWire sutures. The ulnar anchor hole was drilled at the apex of the sublime tubercle, with careful attention to avoid the articular surface of the ulna. The ulnar anchor was a 3.5-mm corkscrew anchor (Arthrex SwiveLock). The longitudinal split in the reconstruction tissue was closed side-to-side using interrupted No. 0 permanent sutures. The FiberTape (Arthrex) was tensioned with the elbow in 60° to 70° of flexion, and the ulnar anchor driver was inserted into the ulnar pilot hole to assess the isometricity of the IB construct before advancing the ulnar corkscrew anchor, completing the IB. Three interrupted permanent No. 0 sutures were used to sew the IB to the underlying reconstruction mass. Ulnar nerve transposition was then performed if it had not been done at the index procedure before closure.
Postoperative Rehabilitation
Postoperative care was standardized across all patients. The postoperative course for revision UCL repair with IB was slower than that for primary UCL repair with IB, with the primary difference being a 6- to 8-week slower return to throwing. Patients were placed in a hinged elbow brace locked at 70° of flexion and neutral forearm rotation for the first week after surgery. Patients were instructed to begin passive range of motion exercises within their brace at 1 week after the operation, with the goal of achieving full elbow extension by the end of weeks 3 to 4. After 6 weeks, patients were permitted to remove their brace and engage in active range of motion exercises and subsequently progress to plyometric and resistance training with the Throwers Ten program. 30 An interval throwing program was initiated at 4.5 to 5 months, depending on the patients’ progress, level of play, and concomitant pathologies.
Statistical Analyses
All statistical analyses were performed in SPSS 29.0 (IBM). We calculated summary statistics (means and standard deviations or counts and proportions) for baseline descriptive data (sex, age at surgery, dominant side, sport, position, level of competition), injury data (UCL tear location and characteristics), and surgical data (concomitant procedures). To evaluate outcomes, we reported summary statistics for PRO data evaluated at follow-up (ASES-E, KJOC, Andrews-Carlson scores). Additionally, we provided the frequency and severity of ulnar nerve symptoms using items from the PRUNE sensory/motor symptoms subscale. Last, we presented the proportions of athletes who were able to successfully return to preinjury sport at the preinjury level or higher, the timing of their return, and, if applicable, factors contributing to the inability to return.
Results
Demographics and Injury Characteristics
We identified 13 collegiate or professional pitchers who had undergone primary UCL reconstruction with autograft followed by revision UCL repair of the autograft with IB at our institution and were at least 1 year postoperative. From this initial group of 13 eligible athletes, we collected outcomes data from 11 (85%). All 11 athletes were male and had revision UCL repair with IB performed on the throwing arm. The mean ± SD time from the initial primary UCL reconstruction to revision UCL repair with IB was 3.4 ± 2.3 years (range, 1.1-8.4). The mean length of time from revision UCL repair with IB to follow-up was 2.9 ± 1.3 years (range, 1.0-5.0).
In terms of tear characteristics, 4 athletes (36%) had complete UCL graft tears, while 7 (64%) had partial graft tears causing pain and inability to compete. Regarding tear location, 9 athletes (82%) had tear locations at the proximal ligament origin, 1 (9%) had a tear location at the distal insertion, and 1 (9%) had tears at the origin and midsubstance of the ligament.
Operative Management
All patients who did not have ulnar nerve transposition at the time of primary UCL reconstruction underwent transposition at the time of revision UCL repair with IB. Thus, 7 athletes (64%) underwent ulnar nerve transposition, while 4 (36%) had decompression of a previously transposed nerve. Additionally, 2 athletes (18%) had posteromedial olecranon osteophyte excision at the time of revision repair.
PROs, Complications, Revisions, and RTS
Table 1 demonstrates mean PRO data for the athletes at follow-up. The mean ASES-E satisfaction score was 9.7 (out of 10; 10 being totally satisfied), the mean ASES-E function score was 35.8 (out of 36; 36 being highest function), and the mean ASES-E pain score was 1 (out of 50; 0 being no pain) (Table 2). Additionally, the mean KJOC score was 88.3 (out of 100) and the mean Andrews-Carson score was 95.0 (out of 100). Results of the PRUNE survey at follow-up revealed that no athletes reported numbness, paresthesia, or cramping of the little finger. One athlete (9%) cited weakness in the hand that did not limit his ability to throw. Four athletes (36%) indicated numbness around the incision/medial aspect of the elbow at a level ≤5 of 10.
Patient-Reported Outcomes Data a
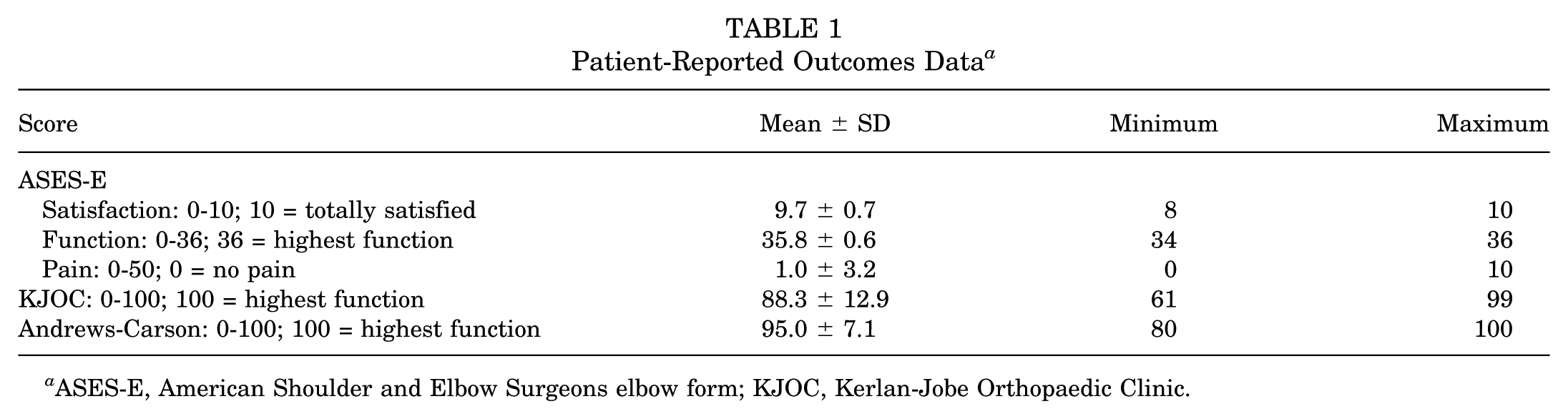
ASES-E, American Shoulder and Elbow Surgeons elbow form; KJOC, Kerlan-Jobe Orthopaedic Clinic.
Return-to-Play Data

All 11 athletes returned to their same level of play or higher.
During the 90-day postoperative period, no patients required reoperation. Minor complications included only peri-incisional numbness. One athlete developed postoperative intrinsic hand weakness, which did not affect his return to play. No patients have required revision surgery to date.
Regarding RTS, all 11 athletes were collegiate or professional pitchers. Six (55%) played at the collegiate level and 5 (45%) at the professional level. All 11 athletes (100%) returned to their preinjury sport and to the same level of play or higher. Regarding their perceived performance before and after revision UCL repair with IB, athletes were asked to compare their current performance against their preinjury performance and rate it on a scale from “much worse” to “much better.” Four pitchers (36%) reported that their performance was a little better, 3 (27%) a little worse, and 4 (36%) about the same. One pitcher indicated changing positions from a starter to a reliever after surgery. The overall mean time from surgery to return to competition was 9.0 ± 2.1 months (Table 2).
Discussion
The incidence of UCL injuries continues to increase while the mean age at the time of surgery (repair or reconstruction) is decreasing, with a growing number of young athletes requiring revision, despite its less favorable results, highlighting the need for innovative solutions to treat injuries in this population.13-15,22 To our knowledge, the present pilot case series is the first to examine outcomes of UCL repair with IB in restoring medial elbow stability in the revision setting after failed primary UCL reconstruction. In a population of high-level baseball pitchers (collegiate and professional), we demonstrate that all athletes were able to successfully RTS at the preinjury level, with no postoperative complications or additional elbow-related surgery reported. These findings provide preliminary evidence that UCL repair with IB may serve as an effective approach to treat failed UCL reconstruction in elite athletes.
In a similar case series evaluating UCL repair in the setting of proximal avulsion of the graft after primary reconstruction, Steffes et al 27 found a mean KJOC score of 87.9 ± 14.6 at follow-up, similar to the findings of the current study. Of the 6 pitchers included, 4 successfully returned to professional baseball, and 3 had a Conway score indicative of full return to their previous level of competition. 27 Notably, the UCL repair technique described in this study does not incorporate the use of internal bracing. In our study, in which internal bracing was utilized in UCL repair, all 11 athletes returned to competition as pitchers at the same level of play or higher. Incorporation of internal bracing offers biologic and mechanical support to the graft, providing a scaffold for healing as well as a valgus backstop, augmenting the native ligament to create a more robust construct. 26
Multiple previous studies have evaluated outcomes of revision UCL reconstructions. Andrews et al 4 reported on their outcomes of revision UCL reconstructions, demonstrating that 80% of patients cited good or excellent outcomes. Despite this, only 50% of athletes and 47% of pitchers were able to RTS at their preinjury level of competition at a mean 12.8 months postoperatively. Other studies report similar outcomes, with recurrent medial elbow pain, prolonged length of postoperative rehabilitation, and recurrent neuropathy barring athletes from returning to sport.7,20 In Major League Baseball pitchers, a recent systematic review found that while 77% to 85% of athletes are able to return to some level of sport after revision UCL reconstruction, only 55% to 78% return at the preinjury level of play. 28 A multitude of factors may contribute to the poorer outcomes observed after revision UCL reconstruction, including limited graft options, need for larger tunnels in revision procedures, and overall damage to the soft tissues and capsule from previous procedures.4,6 In our cohort, collegiate and professional pitchers had comparable outcomes after revision UCL repair with IB, and all athletes were able to return to the preinjury or higher level of competition, with a shorter mean return-to-competition time frame of 9.3 months as compared with revision UCL reconstruction. Importantly, all professional pitchers in our study were still active in their sport at the time of follow-up.
Limitations
This study has several limitations. First, it is a pilot case series, with a small number of participants and no control or comparison group. Furthermore, this case series focuses on collegiate and professional athletes only, which limits the applicability of its findings to other patient populations and pitchers, including younger athletes. Second, and important, there is some selection bias inherent in selecting patients whose UCL injuries were amenable to repair. At the time of preoperative counseling, revision UCL reconstruction with autograft and revision UCL repair with IB were discussed with each athlete. Selection of a revision technique was dependent on intraoperative evaluation of ligament quality. Intraoperative ligament insufficiency would prevent effective repair; therefore, patients would typically undergo revision reconstruction. Third, this study is limited by its lack of objective measures of performance at follow-up, as well as lack of baseline PRO scores, with potential for future studies to incorporate these data points, as this was a preliminary case series. Furthermore, this case series is limited in the data that could be reliably collected for each patient, including details regarding previous UCL grafts and changes in position or level of competition. Additionally, overall follow-up is relatively short, with a minimum time of 1 year postoperative. However, UCL repair is a new surgical technique, and the present case series represents a “first look” at feasibility and preliminary outcomes. Conclusions regarding longitudinal durability or reinjury of UCL repair with IB after failed UCL reconstruction should not be drawn from this study. Last, this study could be subject to surgeon performance bias. The primary surgeon has an extensive history of performing UCL procedures, including UCL repair with IB, and making the intraoperative decision to proceed with repair versus reconstruction. These results may not be translatable depending on surgeon experience.
Conclusion
This pilot case series demonstrates preliminary feasibility and outcomes of revision UCL repair with IB in collegiate and professional baseball pitchers. These results demonstrate that there may be advantages to performing revision UCL repair with IB in athletes whose injury and failed UCL reconstruction are appropriate for repair. We found a high rate of return to preinjury sport at the same level or higher and excellent elbow-related function in the short to midterm. Future studies are needed with longer follow-up, larger sample sizes, and comparison UCL treatment groups.
Footnotes
Final revision submitted January 4, 2026; accepted January 8, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.R.D. has received consulting fees from Arthrex, Bioventus, DJO, Royal Biologics, and Smith & Nephew; nonconsulting fees from Arthrex; and royalties from Arthrex and In2Bones. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Sterling IRB (project 9503).