
Abstract
Background:
Differences in the physical characteristics of bilateral and unilateral lumbar bone stress injuries (BSIs) are unknown.
Purpose:
To compare bilateral and unilateral lumbar BSIs in adolescent male soccer players, with a focus on lumbopelvic alignment.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 78 players (age range, 12-15 years) from a local soccer club who had magnetic resonance imaging (MRI) evaluations were included in the study. Lumbopelvic alignment and lumbar BSI were evaluated using short-tau inversion recovery and 3-dimensional LAVA on 3-T MRI; lumbar BSI was defined as the presence of bone marrow edema and/or the complete and incomplete fracture in the pars region on the MRI. Pelvic tilt (PT) and pelvic outflare angles were assessed on the kicking and pivoting sides, and asymmetry for each parameter was calculated by subtracting the kicking side from the pivoting side. In addition, the lumbar lordosis (LL), sacral slope (SS), and SS relative to LL (calculated by subtracting LL from the SS) were assessed. One-way analysis of variance was performed to compare lumbopelvic alignment in players with bilateral BSI, unilateral BSI, or no abnormal findings (controls).
Results:
No significant differences were found regarding lumbopelvic alignment between the players with bilateral versus unilateral lumbar BSI. PT asymmetry was significantly greater in both players with bilateral lumbar BSI and unilateral lumbar BSI compared with controls (P = .018 and P = .016, respectively). In addition, SS relative to LL was significantly greater in players with bilateral lumbar BSI compared with controls (P < .001).
Conclusion:
Although there were no significant lumbopelvic alignment differences between bilateral and unilateral BSI, players with bilateral BSI exhibited increased sacral anterior tilt relative to the LL, and the pelvis was more posterior on the pivoting side than on the kicking side in both players with bilateral BSI and unilateral BSI. Our results suggest that lumbopelvic alignment assessment may contribute to the management strategy for players with lumbar BSI and to the identification of players at high risk of lumbar BSI.
Keywords
Lumbar spondylolysis often occurs in adolescent athletes 22 and has been characterized as bilateral or unilateral bony defects in the pars interarticularis of the lumbar vertebrae due to chronic microtrauma or repetitive loading. 13 Sakai et al 22 reported a 5.9% incidence of lumbar spondylolysis in the Japanese population; however, adolescent athletes had a higher incidence of lumbar bone stress injury (BSI). The incidence of lumbar BSI, which is considered an early stage of lumbar spondylolysis, is approximately 25% in adolescent athletes.9,27 Previous studies also showed that lumbar BSI is a high-risk, time-loss injury in adolescent soccer players.2,29 Therefore, identifying factors that contribute to lumbar spondylolysis and BSI is essential for preventing these injuries during adolescence. Matsuzawa et al 16 demonstrated that the angle of the fracture line of spondylolysis on the horizontal plane (ie, spondylolysis fracture angle) was smaller in bilateral lumbar spondylolysis compared with unilateral lumbar spondylolysis, suggesting that stress is applied differently depending on the pathogenic side. Since unilateral spondylolysis can progress to bilateral onset, 20 the differences in physical characteristics between bilateral and unilateral spondylolysis need to be clarified.
The onset of lumbar spondylolysis has been reported to be associated with factors such as high workload, immaturity of the lumbar vertebrae, and physical characteristics—including lower limb muscle tightness and lumbosacral malalignment.11,27 Among these, there have been several reports that focus on the potential malalignment of the lumbar spine and the pelvis (ie, lumbopelvic malalignment), given that the pathogenesis of lumbar spondylolysis and BSI is influenced by the mechanical load on the lumbar pars. Patients with lumbar spondylolysis have greater lumbar lordosis (LL)3,4,7,30 and greater sacral anterior tilt. 5 In addition, Tsutsui et al 27 showed that increased SS relative to LL is a risk factor for bilateral lumbar BSI. These findings suggest that consistent compression stress to the lower lumbar spine on the sagittal plane may be associated with lumbar spondylolysis and BSI. Sairyo 19 reported that the stress on the pars interarticularis was higher during extension and axial rotation than flexion and bending of the lumbar spine using a 3-dimensional finite element model. In addition, an in vivo study revealed that lumbar spine rotation with pelvic oblique conditions increased lumbar facet load. 18 Based on the mechanism of stress to the lumbar pars interarticularis, physical factors of pelvic alignment other than the sagittal plane potentially increase stress.
This study aimed to identify the difference in lumbopelvic alignment between bilateral and unilateral lumbar BSI in adolescent male soccer players. We hypothesized that lumbopelvic side-to-side asymmetry would contribute to differences between unilateral and bilateral BSI.
Methods
Participants
Japanese adolescent male soccer players at a single soccer club in Tokyo, Japan, were recruited for this study. A total of 80 male soccer players were initially enrolled in the study in October 2022, and data from 78 players who were able to undergo magnetic resonance imaging (MRI) evaluations were analyzed (mean ± SD age, 13.7 ± 0.9 years; range, 12-15 years). The soccer club was part of a local recreational league, and the participants attended regular soccer training for about 2 hours a day 5 times a week after school and on weekends. The characteristics of the participants are summarized in Table 1. All players were verified through a questionnaire and a direct interview with an orthopaedic surgeon (S.To.) to be free from injuries or illnesses that may affect physical growth or physical activity. In addition, we evaluated the age at peak height velocity, an established indicator of the pubertal growth spurt, using the AUXAL3.1 program (Scientific Software International), based on height records from 6 years of age to the time of height measurement in this study. Parents were asked to provide annual data on their children’s heights, which nurses or elementary school teachers measured. All measurements were performed at Waseda University. Our ethics committee approved the study protocol, and the participants and their parents provided signed informed consent before participation.
Participant Characteristics

MRI and Image Acquisition
Lumbopelvic alignment and lumbar BSI were determined using 2 imaging modes, short-tau inversion recovery (STIR) and 3-dimensional (3D) LAVA, with a 3-T MRI scanner (SIGNA Premier; GE Healthcare). STIR scanning parameters were as follows: repetition time/echo time = 1800/minimum (60) ms; slice thickness = 2 mm; field of view = 24 cm; matrix = 320 × 224 pixels; TI = 150 ms. The lumbar spine, including the lumbosacral vertebrae, was scanned using 3D LAVA with the following parameters: repetition time/echo time = 4.5/2.1 ms; slice thickness = 0.80 mm; field of view = 24 cm; matrix = 384 × 384 pixels. The participant was in the supine position during scanning, with the ankle at 90° of dorsiflexion and the knee in extension using a fixture.
Lumbopelvic Alignment Evaluation
Lumbopelvic alignment was analyzed using an MRI taken in the 3D LAVA mode. First, the LL angle (between the superior endplate of L1 and the inferior endplate of L5) and the sacral slope (SS) angle (between the superior endplate of S1 and the horizontal line) were calculated. 27 The axis on the coronal plane was set to pass through both points, centered at the intersection of the diagonals of L1 and L5 (Figure 1A). Next, the pelvic tilt (PT) and pelvic outflare (POF) angles were evaluated. The PT angle between the line connecting the anterior superior iliac spine (ASIS) and the posterior superior iliac spine (PSIS), the horizontal line on the sagittal image (Figure 1B), the POF angle between the line connecting the ASIS and PSIS, and the line between a white line of the rectus abdominis and the sacral median ridge on the axial image (Figure 1C) were calculated. The ASIS and PSIS were defined as the most anterior and posterior points of the pelvis on the coronal plane (Figure 1, B and C). In addition, the PT and POF angles were evaluated based on players’ shooting legs when playing soccer and categorized on the kicking and pivoting sides, respectively. This classification was based on the participants’ answers to a questionnaire regarding their dominant kicking side for shooting during regular play. To clarify the asymmetry of lumbopelvic alignment, the asymmetry was calculated for the PT and POF angles by subtracting the values from the pivoting and kicking sides, respectively.17,24 To assess the balance of the lumbar curve, SS relative to LL was calculated by subtracting the LL from the SS, as described in a previous study. 27 All analyses were performed by a single examiner (T.T.) using image-processing software (Osirix MD; Pixmeo), and the intraclass correlation coefficient (1,1) measured 3 times each for 5 participants was 0.88 (95% CI, 0.85-0.92) and 0.94 (95% CI, 0.90-0.97) for the PT and POF, respectively.

Analysis of lumbopelvic alignment: (A) the lumbar lordosis and sacral slope, (B) the pelvic tilt, and (C) the pelvic outflare. ASIS, anterior superior iliac spine; PSIS, posterior superior iliac spine.
Lumbar BSI
Lumbar BSI was diagnosed based on the MRI findings. An orthopaedic surgeon (Su.T.) with >40 years of experience assessed the lumbar MRI using STIR and 3D LAVA modes in the axial and sagittal plane views according to the pars. In particular, the STIR image was evaluated for the presence of bone marrow edema (BME) in the pars region (Figure 2C) in accordance with previous studies.6,10,21,24 The 3D LAVA mode was used to determine the complete (Figure 2A) and incomplete (Figure 2B) fracture based on the discontinuities of the lumbar pars interarticularis, which are difficult to detect with STIR mode. Lumbar BSI was defined as positive if the participant had either BME on STIR images or a complete or incomplete fracture in the 3D LAVA mode.1,26 The BSI side from L1 to L5 was recorded (bilateral or unilateral). In addition, the unilateral lumbar BSI was classified according to the kicking and pivoting sides based on the main leg used during soccer shooting. A third party determined lumbar BSI in an anonymized setting to ensure that the results were blinded.
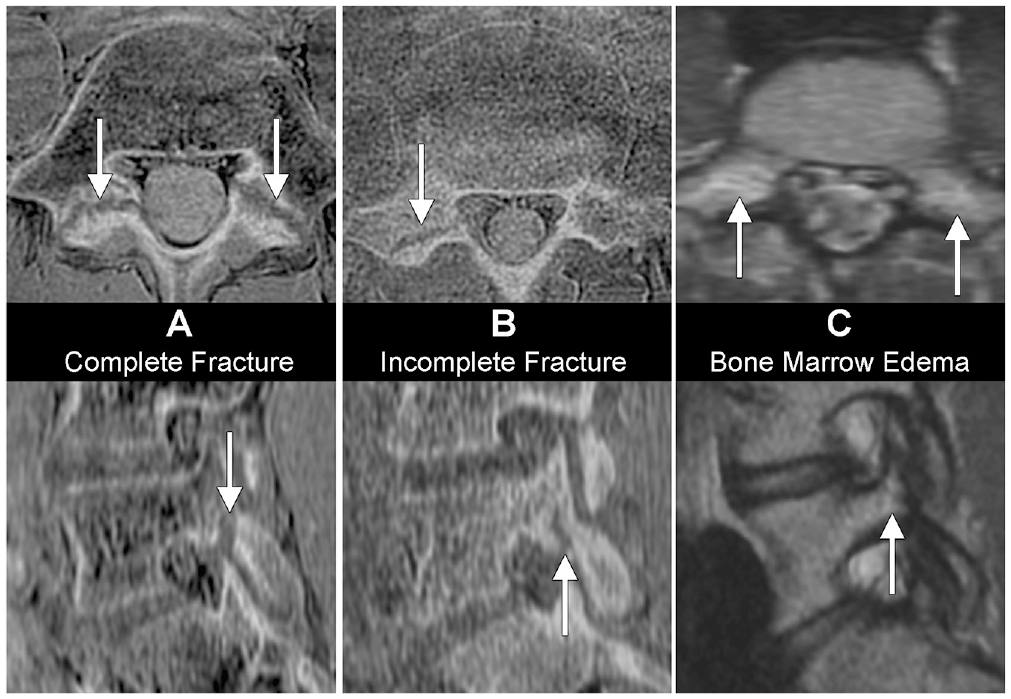
Types of lumbar BSI. The images in the top row show the horizontal plane, and images in the bottom row show the sagittal plane. The arrows in the images indicate positive signs. (A) In a complete fracture, the lumbar pars interarticularis has a full discontinuity. (B) In an incomplete fracture, the lumbar pars interarticularis has a partial discontinuity. (C) With bone marrow edema, the lumbar pars interarticularis shows stress reactions. BSI, bone stress injury.
The same orthopaedic surgeon also detected and recorded the presence/absence of low back pain using the lumbar stress test—including extension and bilateral Kemp test.21,24,27 The Kemp test involves lateral flexion and extension of the trunk while standing upright on both legs to confirm low back pain in this maneuver.
Statistical Analysis
A statistical power analysis was conducted for sample size estimation. According to a previous study, 27 the estimated intragroup standard deviation of the SS relative to the LL was 3°, and the calculated difference between the lumbar BSI and the control group was >3°. This study required >8 players with lumbar BSI to achieve a power of 80% and an alpha of .05.
All data were analyzed using SPSS Statistics Version 28 (IBM). Age, height, weight, LL, SS, PT, and POF were expressed as means and standard deviations for bilateral and unilateral lumbar BSI and controls, and normal distributions were confirmed. One-way analysis of variance was performed to compare parameters for bilateral BSI, unilateral BSI, and controls. Post hoc tests were performed using the Tukey method. The significance level was set at P < .05.
Results
Of the 78 participants, 18 had bilateral lumbar BSI at L5, 8 had unilateral lumbar BSI at L5 on the pivoting side, and 52 players had no abnormal imaging findings and were categorized into the control group. In addition, 12 (66.7%) players with bilateral lumbar BSI, 5 (62.5%) with unilateral lumbar BSI, and 9 (17.3%) controls had lumbar extension pain. No participants had a unilateral lumbar BSI at L5 on the kicking side. Two participants had bilateral lumbar BSI at L4 and L5 (Figure 3).
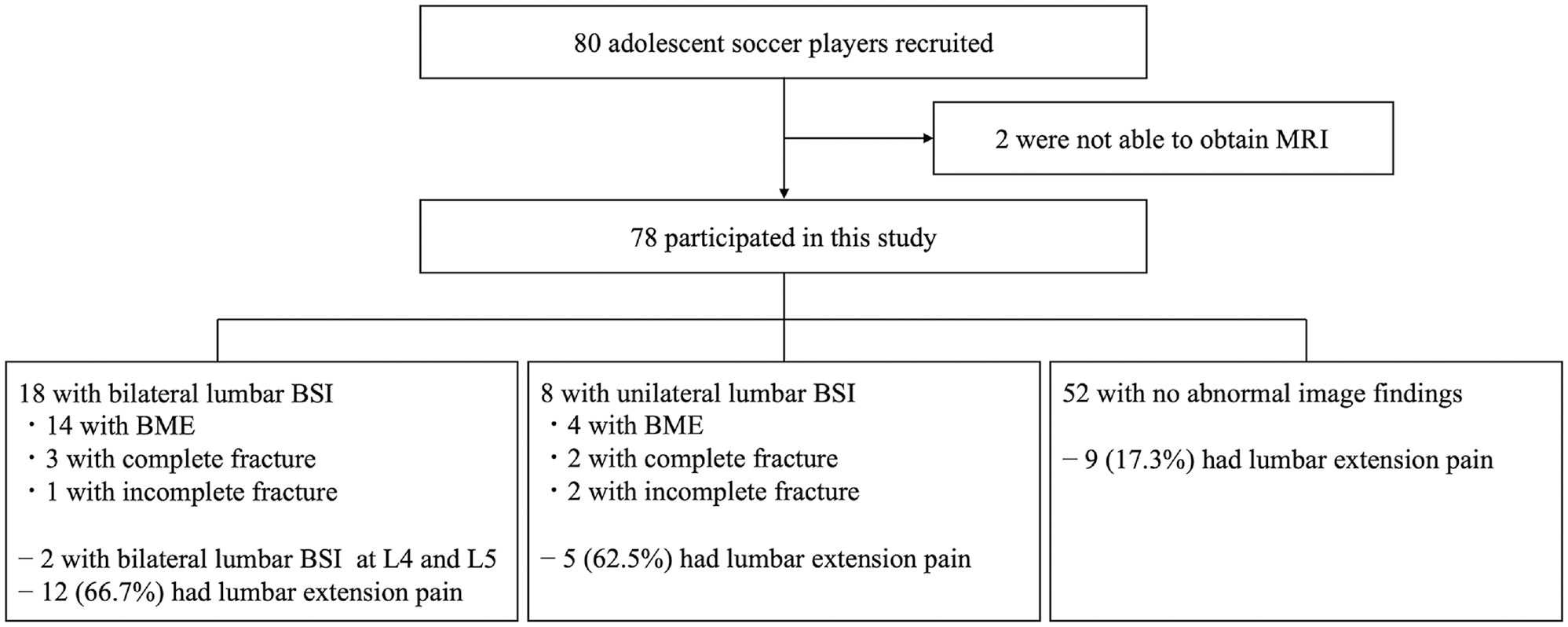
A flowchart of bilateral and unilateral BSI and the control group classification. BME, bone marrow edema; BSI, bone stress injury; MRI, magnetic resonance imaging.
Table 2 compares the patient characteristics of players with bilateral and unilateral lumbar BSI versus the control group. Figure 4 shows the relationships between SS relative to LL and the PT and POF. There were no significant differences between the bilateral and unilateral lumbar BSI in any of the variables. Meanwhile, PT asymmetry was significantly greater in the bilateral and unilateral injuries compared with PT in the control group (P = .018 and P = .016). In addition, SS relative to LL was significantly greater in players with bilateral lumbar BSI compared with the control group (P < .001).
Comparison of Basic Characteristics and Lumbopelvic Alignment in the Bilateral and Unilateral BSI Groups Versus Controls a

Values are expressed as mean ± SD. APHV, age at peak height velocity; BSI, bone stress injury; LL, lumbar lordosis; SS, sacral slope.
Significant differences compared with the control group (P < .05).

Relationship between SS relative to LL and (A) asymmetric PT and (B) POF. LL, lumbar lordosis; POF, pelvic outflare; PT, pelvic tilt; SS, sacral slope.
Discussion
This study was conducted to elucidate the differences in lumbopelvic alignment between bilateral and unilateral lumbar BSI in adolescent male soccer players. We found no difference in lumbopelvic alignment between players with bilateral BSI and unilateral BSI. However, when compared with the control group, the players with bilateral BSI exhibited sacral anterior tilt relative to the LL and the pelvis, and both the bilateral and unilateral BSI players had a more posterior tilt of the pelvis on the kicking side compared with the pivoting side. Based on our findings, it may be useful for clinicians to include lumbopelvic alignment assessment as part of their routine evaluation of adolescent players, particularly those with BSI and a high risk for lumbar BSI.
Side of Lumbar BSI Prevalence
Few studies have attempted to detect lumbar spondylolysis and/or lumbar BSI using MRI in a cohort of athletes. We identified 26 adolescent soccer players (33.3%) with lumbar BSI. Previous studies9,27 have shown that the incidence of lumbar BSI in adolescent athletes was approximately 25%. In the present study, we used 3-T MRI to detect both BME and the complete and incomplete fracture in the pars region using 3D BONE LAVA mode. 1 The higher prevalence of lumbar BSI in our study may be due to the ability to identify the BSI pathologies of the pars interarticularis in the lumbar vertebrae, which includes BME and stress fracture, 28 as well as our targeting of athletes within a single club. In addition, lumbar BSIs are usually bilateral, 27 and unilateral spondylolysis is more likely to occur on the nondominant side. 19 Bilateral lumbar BSIs occurred in 18 (69.2%) players in our study, and unilateral lumbar BSIs only occurred on the contralateral side of the kicking leg. Thus, the specific repetitive rotational direction—including the soccer kicking motion—may cause side-to-side differences in mechanical stress on the lumbar pars regions.
Group Differences in Lumbopelvic Alignment
Our results showed that the SS relative to LL value was greater in the bilateral lumbar BSI group compared with the control group. Previous studies focusing on the relationship between lumbosacral alignment and lumbar spondylolysis and BSI found that greater LL9-12 and SS 13 values were associated with these conditions. Prospective cohort studies also showed that the odds ratio for the incidence of lumbar BSI increased approximately 4 times for an SS ≥5° relative to the LL. 3 This finding suggests an increase in consistent compressive stress between L5 and S1. Both the bilateral and unilateral lumbar BSI groups in the present study had an SS relative to the LL >5°, suggesting that this measurement may be an indicator of increased stress in the sagittal plane, independent of the side of prevalence. Therefore, checking the balance of the sacral anteversion against the LL would be important to potentially minimize stress on the pars, which is the pathogenic mechanism of lumbar spondylolysis and BSI, and it would also contribute to prevention strategies for players at high risk of lumbar BSI and to treatment management and recurrence prevention for players with lumbar BSI.
PT asymmetry was greater in players with bilateral and unilateral lumbar BSI compared with asymmetry in players with no BSI. Interestingly, in players with bilateral and unilateral BSI, the pelvis tilted more posteriorly on the pivoting side than on the kicking side. Since the pelvis on the pivoting side tilts backward during ball contact in soccer kicking, 14 the repetition of the kicking motion may cause PT asymmetry. A positive correlation has been reported between the anterior PT and the hip extension range of motion during running. 23 The increased posterior tilt of the pelvis on the prevalent side may lead to limited mobility of anterior PT and hip extension, resulting in excessive load on the lumbar pars in the direction of the lumbar extension during running and soccer kicking motions. Given that hamstring tightness, which contributes to lumbar spondylolysis and BSI,12,27 causes the pelvis to tilt backward, the clinician should check and improve both hamstring tightness and PT asymmetry. In addition, Sairyo et al 20 reported that unilateral spondylolysis may lead to bilateral spondylolysis. Tatsumura et al 25 also speculated that unilateral lumbar spondylolysis may increase stress on the contralateral pars. Thus, clinical evaluation for unilateral BSI, which exhibits the most PT asymmetry, may be valuable in preventing the transition from unilateral to bilateral lumbar spondylolysis and/or BSI.
We did not detect any differences in POF between the groups. Surprisingly, the POF on the kicking side was greater in the controls, despite being only 2°. We speculate that this difference may be related to repetitive motions, such as inside kicks, that externally rotate the pelvis and hip joints. If a high POF on the kicking side is normal for soccer players, the POF on the kicking side of the prevalence group may be relatively smaller. Further investigations focusing on injuries other than lumbar injuries are needed.
Limitations
Our study has several limitations. First, this was a cross-sectional study. Thus, we could not determine a causal relationship between lumbopelvic alignment and lumbar spondylolysis and/or BSI incidence. However, according to the current findings, it is considered that pelvic alignment asymmetry could serve as a potential risk factor for lumbar BSI. Therefore, more attention would need to be directed toward assessing muscle tightness and strength, as these factors could mediate the pelvic alignment asymmetry. Second, an MRI was performed in the supine position, which differed from the actual sports activity. Although we eliminated the influence of lower limb joint angles as much as possible by fixing the ankle and knee during MRI, it was considered that lumbopelvic alignment may be altered depending on the posture. Previous studies have shown that lumbar lordosis and sacral tilt were increased when assessed in the standing rather than supine position,8,15 while the PT was decreased. 8 Thus, clinicians could utilize our findings, taking into account the characteristics of lumbopelvic alignment caused by different postures. Finally, this study did not examine each player’s practice or game workload. A higher percentage of days in training and a shorter break have been reported to be associated with lumbar BSI. 11 This is probably a limitation of this study, although it is assumed that there are few differences between players because the players in this study belonged to the same club.
Conclusion
The study findings indicated no differences in lumbopelvic alignment between adolescent male soccer players with bilateral and unilateral BSI. Nevertheless, compared with controls, players with bilateral BSI exhibited anterior sacral tilt relative to the LL. In addition, in both players with bilateral BSI and unilateral BSI, the pelvis was more posterior on the pivoting side than on the kicking side. Our results suggest that lumbopelvic alignment assessment may contribute to the management strategy for players with lumbar BSI as well as the identification of players at high risk of lumbar BSI.
Footnotes
Acknowledgements
The authors sincerely thank the players who participated in this study. We also thank Nao Shinoda, the head coach of the junior soccer team in Tokyo and Kyoji Ohta, the technical support in MR measurements.
Final revision submitted September 1, 2023; accepted September 6, 2023.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Waseda University (ref No. 2021-218).