
Abstract
Objective
The objective of this study was to compare the relative stability in lumbar spondylolysis (SP) of a rigid anterior plate (with a novel compression slot) versus traditional posterior pedicle screw (PS) fixation.
Summary of Background Data
Arthrodesis has been a mainstay of treatment for symptomatic isthmic spondylolisthesis in adults. Posterior PS fixation has become a commonly used adjunct. Some have advocated anterior lumbar interbody fixation (ALIF) plate as an alternative. The relative stability afforded by ALIF in SP has not been well characterized, nor has the contribution afforded by a compression screw slot in an ALIF plate.
Methods
Calf spine segments were characterized in the normal state, after sectioning the pars (SP model), then after reconstruction with an interbody spacer and either PS/rods, or an ALIF plate, or both.
Results
ALIF plate conferred stability on the spondylolytic segment only comparable to that of the normal functional spinal unit (FSU). Posterior fixation was more stable than anterior fixation in all testing modes. Addition of an ALIF plate conferred a significant additional stability in those that already had posterior fixation. The utilization of an anterior compression screw conferred additional stability in extension testing only.
Conclusions
ALIF plate reconstruction in the setting of SP may not confer enough segmental stability to predictably encourage fusion beyond that of the uninstrumented intact FSU. The utilization of an integral compression screw in an ALIF plate may not confer clinically significant additional construct stability in SP.
Introduction
Decompression, partial reduction, and stabilization with arthrodesis have been a mainstay of treatment in symptomatic lytic spondylolisthesis in the adult for many decades. 1 , 2 Although arthrodesis has consistently been associated with improved clinical results, 3 the role of internal fixation has been somewhat controversial in the past. Some studies showed no improved outcomes with the inclusion of internal fixation 4 , 5 to a posterolateral fusion (PLF). On the other hand, numerous authors have shown positive results with the inclusion of rigid transpeduncular posterior instrumentation in isthmic spondylolisthesis. 6 , 7 , 8 , 9 , 10 , 11 , 12 More recently, some authors have advocated including an interbody arthrodesis in these patients, citing the difficulty in achieving a reliable robust posterior fusion. 13 , 14 , 15 The addition of interbody fusion to PLF (PLIF) appears to improve one's ability to maintain correction and achieve solid union, 8 , 14 , 15 although this has not been clearly linked to improved patient function. TLIF has been shown to be effective in short-term studies with less morbidity than a combined anterior–posterior spinal fusion or a posterior lumbar inter body fusion. 16 , 17 More recently, with the growing appreciation for anterior lumbar interbody fusion (ALIF) techniques, some surgeons have advocated combined ALIF with posterior instrumentation for these patients. 16 , 18 , 19 , 20 , 21 , 22 , 23 With the advent of newer anterior lumbar plate fixation options, the authors are aware of surgeons who are now advocating instrumented ALIF alone for the treatment of symptomatic adults with isthmic spondylolisthesis, 24 relying on indirect decompression of the L5 foramen by restoring more normal intervertebral spacing.
Biomechanical investigations of instrumentation for adult isthmic spondylolisthesis have tended to focus on posterior methods. Shirado et al evaluated six methods of posterior stabilization of the spine in lumbosacral spondylolisthesis, some with interbody support (tricortical iliac crest) after the method of Cloward. 25 Transpeduncular instrumentation produced the most rigid construct. The addition of their interbody arthrodesis construct did not change the rigidity significantly. A study done by Cunningham et al, tested and endorsed the use of titanium mesh PLIF cages and iliac screws in the operative stabilization of high-grade lumbosacral spondylolisthesis. 26 Minamide et al assessed the biomechanical stiffness of transdiscal fixation with posterior pedicle screws (PSs) against combined interbody/PS fixation in a L5-S1 spondylolisthesis human cadaver model. They showed that transdiscal screw fixation is significantly stiffer than PS fixation alone and comparable to that of combined interbody/PS fixation. 27
Experience with anterior lumbar interbody fusion is growing as newer plate technologies become available. Anterior approaches are promising because they may offer less muscle dissection, more rapid recovery, and less postoperative pain than traditional posterior approaches. The objective of this study was to biomechanically compare the stability of anterior lumbar interbody fixation in spondylolysis (SP) to the already established posterior fixation techniques. The availability of a relatively new anterior lumbar plate allowed us to also assess the biomechanical effect of using an integrated compression screw.
Materials and Methods
Specimen Preparation
Functional spinal units (FSUs) were harvested from fresh-frozen and thawed juvenile bovine cadaver specimens. The highest incidence of isthmic spondylolisthesis in humans is reported at the L5-S1 level; thus our testing methods attempted to recreate the biomechanical environment and loading in the human L5-S1 spinal segment using bovine spine analogs. This was achieved by orienting the superior endplate of the inferior vertebra of the bovine specimen at a 45-degree angle relative to the horizontal, thus approximating the natural physiological angle of S1 in humans, and then rigidly fixing the caudal vertebra to the table of an Instron 8821s servo-hydraulic biaxial test machine (Instron, Norwood, MA, USA) (Fig. 1). Lumbar FSUs were harvested from calf spines, and were used to create a total of eight test samples per test configuration. Specimen preparation included dissection of the surrounding adipose and paraspinal musculature with preservation of the interconnected ligaments (including the supraspinous and interspinous ligaments), intervertebral disk, and osseous structures, including the facet joint capsules.
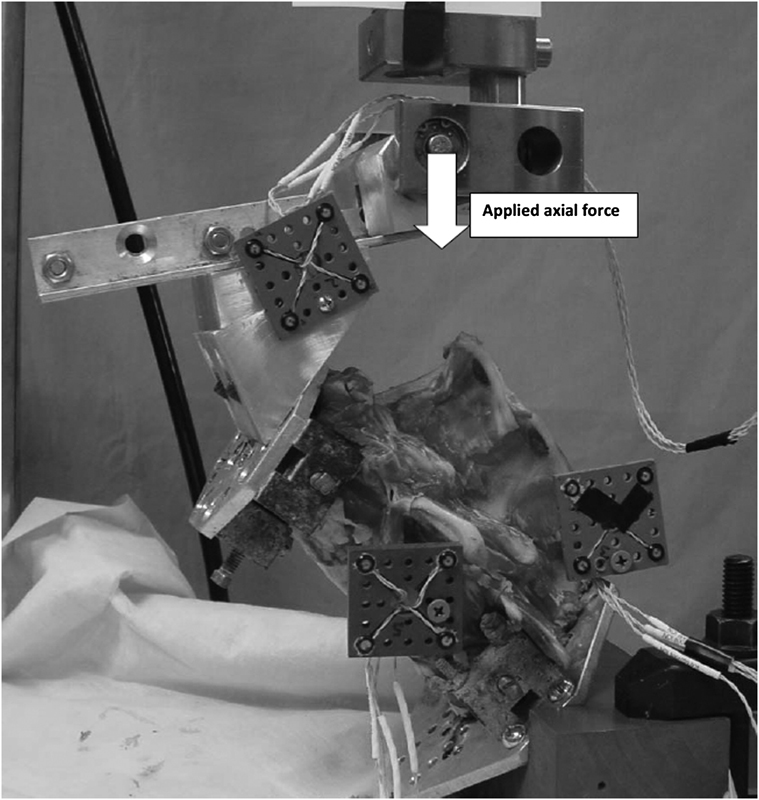
Calf specimen ready for testing in extension.
Testing Configurations
The following spinal testing configurations were performed for each specimen:
Normal intact FSU
Destabilized SP spinal unit
Then, one of the following fixation techniques:
Posterior PS fixation with polyether etherketone (PEEK) interbody cage (PLIF)
Anterior plate fixation with PEEK interbody cage, no compression screw (ALIF-NC)
Anterior plate fixation with PEEK interbody cage, employing integral compression screw (ALIF-C)
Posterior PSs, anterior plate, and PEEK interbody cage (360 fixation).
Pedicle screws (Stryker Spine, Allendale, NJ, USA) were used (6.5 × 45 mm), affixed to 5.5 mm rods. An anterior lumbar plate (Stryker) (Fig. 2) was used for the ALIF constructs (denoted in figures as ALIF-NC). This includes an integral compression screw slot (Fig. 2) that may be used to apply additional compression (denoted in figures as ALIF-C) to the spacer and interbody bone graft. PEEK interbody spacers (Stryker) (12 mm) were used in all constructs.

The anterior lumbar plate used for this study. This is fixed to the vertebral bodies through the four variables—angle holes and the integral locking rings are rotated to prevent screw back-out. The superior (fifth) hole is for optional additional compression of the intervertebral graft before placement of the two locking screws into the cranial vertebra.
Testing Protocol
Three consecutive tests were run on each individual spinal unit: (1) intact spine, (2) unstable SP spinal unit, and (3) one of the four fixation methods. A biaxial load frame was used to apply flexion, extension, lateral bending, and axial rotation moments on the vertebral segment. The superior vertebra was fixed to a gripping plate attached to the Instron ram through an unconstrained pushrod designed to apply either pure axial load or pure torsion (Fig. 1).
An Optotrak Certus (NDI, Waterloo, Ontario, Canada) optical three-dimensional rigid body tracking system with a resolution of 0.01 mm was used to detect displacements and rotations of L5 and S1 during each test. Rigid body markers were attached to the L5 and S1 vertebrae, as well as the loading pushrod so that application of load and relative displacements and rotations could be tracked in real time during all tests. Optotrak data were collected at a rate of 100 Hz throughout the test.
The pars interarticularis was bilaterally sectioned using an oscillating saw to create a SP model 28 , 29 without disturbing the supporting ligaments.
Flexion and Extension
A flexion or extension moment load was applied via a moment arm attached to the superior vertebra (Fig. 1). A neutral load position was determined before testing. This neutral position was defined as the point at which an axial load of 25 N did not induce either flexion or extension motion of the vertebral segment, which occurs when the force vector passes through the initial center of rotation for the segment. Subsequently, a moment in the direction of interest (i.e., flexion or extension) was applied by adjusting the moment arm length, 10 mm anterior (for flexion) and 10 mm posterior (for extension), measured from the determined neutral load position. The application of load 10 mm from the initial center of rotation induced a combined axial compressive force on the segment and a moment at the segment similar to the expected combined loading applied in vivo to the lower lumbar spine in humans. Load was applied at a rate of 0.25 mm/s up to 4 Nm, which was below the measured physiologic limits of the segment. Tests were stopped before failure to preserve all components for subsequent testing. Load deformation curves were recorded for three consecutive loading cycles. Stiffness was determined from the slope of the linear range of the third load deflection curve.
Lateral Bending
A load was applied to induce right or left lateral bending via a similar method as above using a moment arm attached to the superior vertebra. Again, a neutral position was determined before testing, and then the force vector was moved 10 mm left or right of the determined neutral position to apply a combined compression and lateral moment load. Load deformation curves are recorded for three consecutive cycles. Lateral loading was applied at a rate of 0.25 mm/s below the physiologic limits of the segment. The unconstrained axial loading pushrod allowed for normal kinematics of the specimen during testing in all directions.
Axial Torsion
A moment was applied to the superior vertebra to produce a transverse-plane torque on the segment. As with the previous loading, the neutral position was determined before testing. A pure moment was applied with an axial preload to simulate physiologic torsion on the segment. Three consecutive load deformation curves were recorded.
Rotational stiffness was defined as the amount of torque required to rotate one vertebra relative to another by 1 degree about the axis of interest. Shear stiffness was defined as the amount of force per mm required to displace one vertebra relative to another in the transverse plane of the disk space. To account for interspecimen size, the data were normalized by the intact behavior of each FSU.
Statistical Analysis
Measured stiffness values were standardized to those of normal intact FSUs. The change scores of these standardized values (from the normal intact) were used as dependent and independent variables, respectively. Since there were six different loading modes in the testing protocol, all possible pairwise comparisons were conducted. In view of these multiple tests, the false discovery rate (FDR) was used to control the rate of false discoveries. Thus, for these multiple tests, FDR adjusted p values less than 0.05 were considered significant. Considering a small sample size per group, the Mann–Whitney U test and the Wilcoxon signed-rank test were used for the pairwise comparisons among five loading modes (SP, noncompression plate [NCP], compression plate [CP], PS, and 360) and comparison with the intact mode (In), respectively. The analysis was done in SAS version 9.2 software (SAS Institute, Cary, NC, USA).
Results
The instantaneous load-deformation data for 4 Nm moments applied in all three planes and for all constructs is shown in Table 1. Although these data were generated continuously in real time during loading, this “snapshot” look offers an opportunity to make comparisons in relative stiffness for each of the constructs. In general, the rotational stiffness data are represented for comparison in Fig. 3 and the shear stiffness data in Fig. 4. The observed trends included the following: (1) the SP model was measurably less stiff than the intact FSU, as noted by the larger measured rotations for the same applied moment, particularly in axial rotation and sagittal plane bending, (2) ALIF constructs were less stiff than either model with posterior support, (3) circumferential fixation created the stiffest construct, and (4) all cycles demonstrated hysteresis between loading and unloading (Fig. 5).
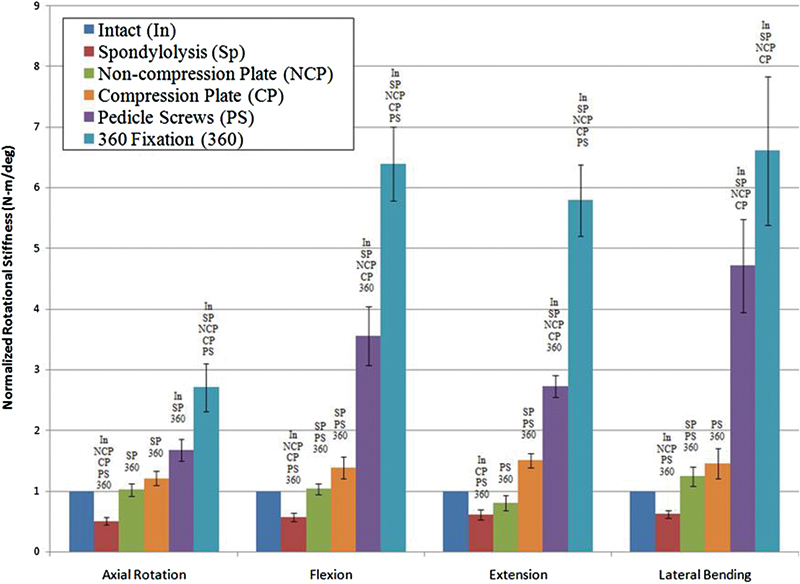
Normalized rotational stiffness of tested calf spines with concomitant spondylolysis (n = 8) and various reconstructions. Note: symbols above bars indicate groups that are significantly different from intact FSU, p < 0.05.
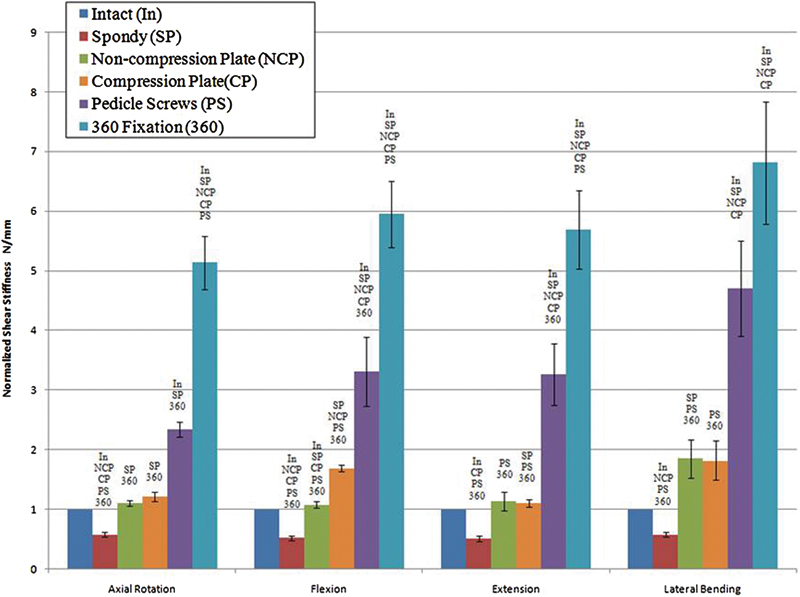
Normalized shear stiffness of tested calf spines with concomitant spondylolysis (n = 8). Note: symbols above bars indicate groups that are significantly different from intact FSU, p < 0.05.
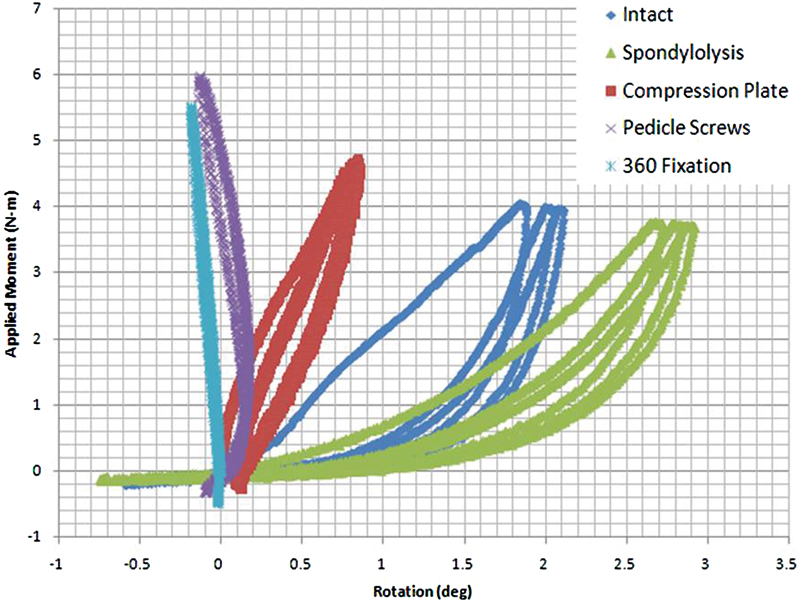
Load versus rotation hysteresis plots for flexion loading of one specimen.
Comparative Rotational Compliance Data for Each Construct (n = 8) in All Three Planes
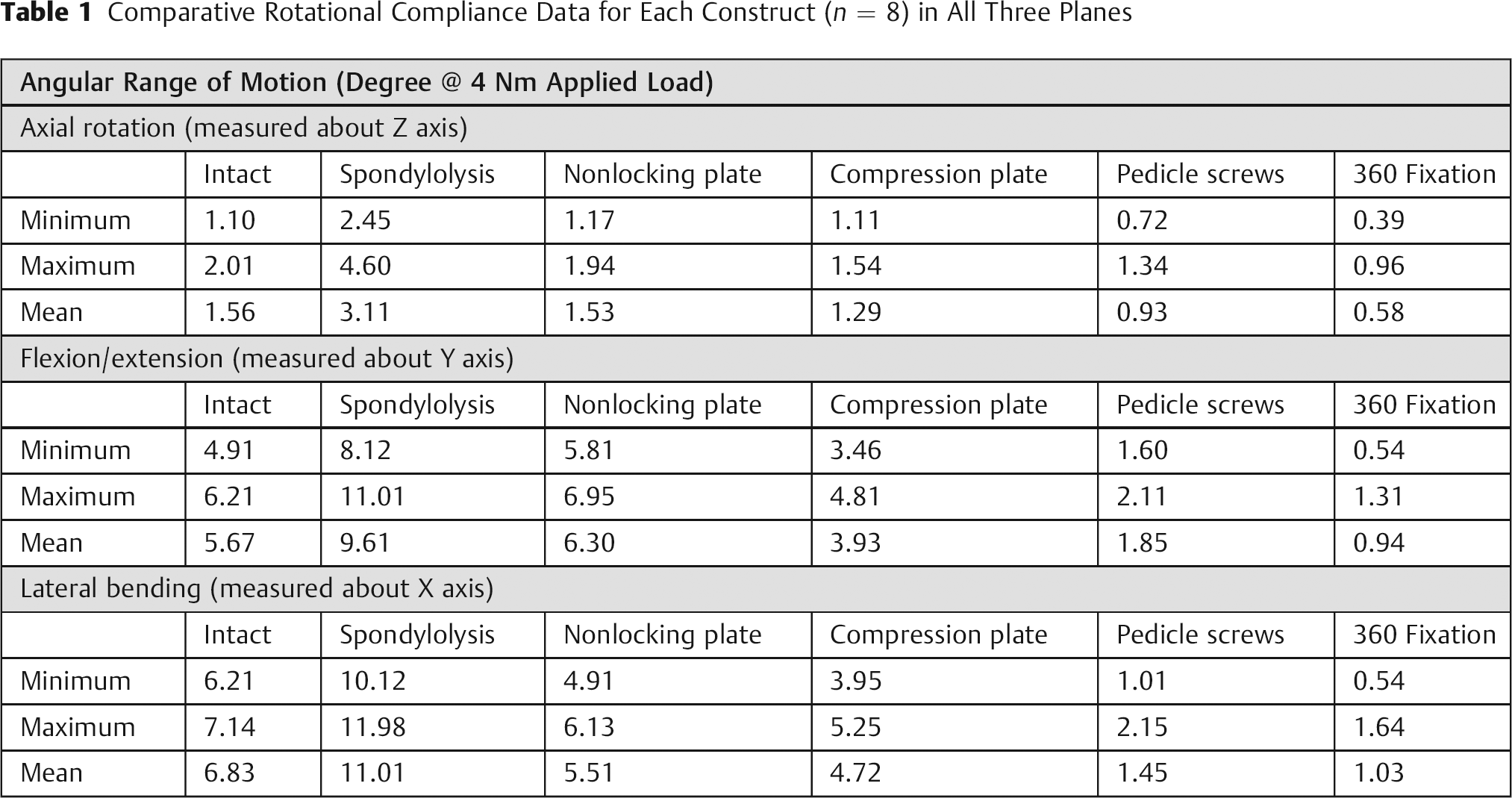
Fig. 3 presents the normalized rotational stiffness for the various configurations tested including: In, SP, NCP, CP, PSs, and 360 fixation (360). It was seen that, when a spondylolytic defect was present, neither ALIF construct (with or without compression screw) demonstrated a significant increase in the segmental stiffness over the normally intact FSU except for the CP in extension. There was a trend toward the CP conferring a slightly stiffer construct than did the NCP; however, the difference was not statistically significant. PS fixation resulted in significantly stiffer constructs in all modes of motion and loading. The addition of NCP to PS fixation (360) resulted in significantly stiffer constructs compared with PS alone in all modes except lateral bending.
A similar pattern was seen in the shear stiffness data shown in Fig. 4. ALIF constructs returned segmental stiffness only to that of the intact FSU. Again, PS fixation conferred significantly greater stiffness in all modes, and 360 fixation significantly greater than that, in all modes but lateral bending. Even though mean shear stiffness was similar between NCP and In as shown in Fig. 1, a statistical significance was found in the distribution of changes from In to NCP based on the rank-based nonparametric test (Wilcoxon signed-rank test).
Discussion
Our SP model significantly reduced segmental stability (p < 0.05), particularly in axial rotation (Figs. 34–5). This is in agreement with previous studies. 30 , 31 , 32 , 33 , 34 , 35 However, our model was not able to reproduce the laxity that develops in the disk and supporting ligaments in the setting of chronic SP. The addition of an interbody spacer and an anterior plate increased the segmental stability of the SP model only to stiffness range of a normal FSU. Had we been able to include chronic laxity in the disk and ligaments, it is likely that the ALIF construct would have performed even more poorly in conferring segmental stability. If one were to accept the proposition that stiffer segmental constructs lead to more predictable spinal fusion, 36 , 37 then such an anterior-only construct may not likely be an acceptable option in isthmic spondylolisthesis. Yet, there are clinical reports of quite good fusion rates at 2 years using such an anterior-only strategy. 24
This points out that there are still several incompletely answered questions when one wishes to optimize outcomes of arthrodesis for isthmic spondylolisthesis. First, there may be variations in the preparation of fusion beds that can affect success rates. Second, there are variations in postoperative treatment protocols with respect to bracing that may affect clinical outcomes. Neither of these is taken into account in most laboratory biomechanical cadaveric models. Third, the optimal robustness of the fusion mass at the lumbosacral junction is currently unknown. Fourth, there is still difficulty in accurately determining successful fusion radiographically. Criteria that were commonly used before computed tomography (visual presence of bridging trabecular bone on plain films) may over-call successful interbody fusion 38 and this may serve as a confounder when attempting to compare historical fusion rates of different surgical techniques.
The addition of posterior PS-rod fixation significantly increased the segmental stiffness as compared with the In and the SP models (p < 0.05). This is in agreement with that of previous studies, 25 and has been associated with good clinical results in numerous studies. 10 , 12 , 39 Posterior PS fixation was also significantly more stable than ALIF constructs. We chose to use the same interbody spacer for our anterior and posterior fixation constructs. While there are certainly a myriad of interbody spacer options available, we felt that there would not likely be large variations in their contributions to construct stability 40 and wished to eliminate this variable in our study.
A surprising finding of this study was that even in the face of rigid posterior PS fixation and interbody spacer, the addition of an anterior plate conferred significant additional rigidity to the construct. This has not been previously reported, nor has such a construct been reported with clinical results. It may be that there is a threshold effect in the linkage of construct rigidity and spinal arthrodesis such that the addition of an anterior plate to a posterior PS construct will not result in significant clinical improvement. This will remain to be investigated in live models.
Finally, there has not been a biomechanical evaluation of the addition of an intrinsic compression screw to an ALIF plate, as has been tested here. Based on our data, this seems to confer no additional significant stability to the construct in our spondylolisthesis model.
Summary and Conclusions
This cadaveric study indicates that an anterior plate alone may not be sufficient to confer the segmental stability necessary to achieve predictable fusion in isthmic spondylolisthesis. Posterior PS fixation does confer significant stability in such a model. There is a significant additional stiffening effect of anterior plate fixation superimposed on posterior PS fixation in such a setting. It is unclear what the clinical significance of this additional effect may be. There is no significant additional stability imparted in this model by the inclusion of an intrinsic compression screw within the ALIF plate.
Research Support
The authors wish to thank Stryker Spine for in-kind support (implants) for use during this investigation.
Disclosures
Theodore Choma, None
Ferris Pfeiffer, None
Santaram Vallurupalli, None
Irene Mannering, None
Youngju Pak, None