
Abstract
Background:
Increased posterior tibial slope angle (PTSA) has been shown to be an important risk factor for anterior cruciate ligament (ACL) injury. PTSA modulation is not utilized routinely to reduce risk of primary rupture or graft failure. Displaced tibial tubercle (TT) fractures in the skeletally immature are associated with potential growth arrest and may be used as a model to study PTSA changes in this setting.
Purpose/Hypothesis:
To quantify the change in PTSA (ΔPTSA) after operative treatment of displaced TT fractures in skeletally immature patients. It was hypothesized that there would be a progressive decrease in PTSA after TT injury and that rate of ΔPTSA would be highest during peak growth velocity.
Study Design:
Case series; Level of evidence, 4.
Methods:
Included were 22 patients (n = 23 knees; mean chronological and bone age at injury, 14 years; 86% male) who underwent surgery for displaced TT fracture. PTSA was measured on lateral radiographs at time of surgery and subsequent follow-up, and bone age at the time of injury was determined using radiographic standards. The rate of ΔPTSA for individual patient, total cohort, and sex-based subgroup trends were determined via linear regression (degrees per month; positive value indicates relatively anterior). Individual patient regression coefficients were averaged into bone age cohorts.
Results:
Average follow-up was 17 months (range, 6-52 months). The mean PTSA was -12°± 2.4° at the time of injury, and the mean ΔPTSA for the cohort was 0.30°± 0.31° per month (range, -0.27° to 0.97° per month). Linear regression demonstrated a significant relationship between months postfixation and PTSA, demonstrating a ΔPTSA of 0.31° per month (95% confidence interval [CI], 0.24° to 0.38°; P < .001). The highest ΔPTSA was seen at bone age 14 years (mean, 0.58°± 0.44° per month). The mean absolute change in PTSA from injury to final follow-up was 4.1° (range, -3.4° to 21°).
Conclusion:
Our data suggested that PTSA becomes more anterior after operatively treated pediatric TT fractures and that ΔPTSA may be influenced by bone age. This concept may be useful in considering surgical modulation of excessive PTSA in the pediatric ACL-deficient knee.
Anterior cruciate ligament (ACL) injuries are among the most common sports injuries in pediatric patients, 28 with the incidence rising over the past several decades due to an increased emphasis on athletic competition and specialization. 4 The current standard of care for pediatric ACL tears is ACL reconstruction (ACLR) to restore stability and limit further meniscal and chondral injury. 20 Although there have been significant improvements in pediatric ACLR over recent decades, including optimal graft choice, graft and tunnel preparation, and rehabilitation parameters, 7 pediatric patients continue to have a greater risk of graft failure after ACLR when compared with adult populations. 29 Therefore, there has been an impetus to identify and mitigate risk factors for ACL graft failure. Increased posterior tibial slope angle (PTSA) has been identified as a risk factor for both primary ACL injury and graft failure.9,10 Increased PTSA leads to anterior translation of the tibia, which increases the load on the ACL as the primary anterior stabilizer of the knee and subsequently increases its risk of injury. 2 There are no interventions described in the literature to modulate PTSA in skeletally immature patients at the time of ACLR to mitigate the risk of graft failure. Whereas anterior tibial epiphysiodesis in a skeletally immature person could theoretically reduce PTSA, there are no data to inform the optimal timing or effects of such an intervention.
Tibial tubercle (TT) fractures are a relatively rare injury among pediatric patients, with an incidence between 0.4% and 2.7%, 12 which may offer a model for anterior tibial epiphysiodesis. The TT is the secondary ossification center, or apophysis, of the proximal tibia. When a person approaches skeletal maturity, the physeal fibrocartilage becomes replaced with columnar cartilage, which is weak when newly formed. The proximal tibial physis fuses at around 15 years for females and 17 years for males. 8 This predisposes adolescents to TT avulsion fractures caused by an abrupt contraction of the quadriceps muscle. 11 The Ogden (modified Watson-Jones) classification is used to characterize these fractures based on fracture displacement and involvement of the apophysis and proximal tibial epiphysis. 23 Treatment of displaced TT fractures is open reduction internal fixation (ORIF) via screw, Kirschner-wire (K-wire), or suture anchor fixation. Nonoperative treatment with closed reduction and casting is often reserved for minimally displaced (Ogden type 1) injuries. Displaced TT fracture and subsequent operative fixation can halt growth of the anterior proximal tibial physis, leading to relative overgrowth of the posterior physis and subsequent loss of posterior tibial slope. 6 In severe cases, the loss of posterior slope may lead to recurvatum and hyperextension of the knee, which has been reported in several studies.18,21,24 However, there are currently no data on the incidence or degree of growth arrest after fixation of TT fractures. Proximal tibial (hemi)epiphysiodesis using screws, stapes, or plates that bridge the proximal tibial physis is applied widely for correction of coronal plane deformity or limb-length correction. 13 However, quantifying changes in sagittal alignment (PTSA) after TT fracture ORIF may inform the potential efficacy of anterior tibial epiphysiodesis that temporarily halts growth at the tibial apophysis, leading to a reduction in PTSA. Furthermore, bone age at the time of TT fracture is likely to influence rate of change in PTSA in accordance with peak growth velocity and physeal closure.16,30 Notably, the rate of change in tibial slope after TT fracture has not been quantified.
The aim of this study was to quantify the rate of change in PTSA as a result of physeal growth arrest after operatively treated displaced TT fractures in skeletally immature patients and to determine how this rate is affected by skeletal age. We hypothesized that there would be a progressive loss of posterior tibial slope after injury and that rate of change in PTSA would be highest during peak growth velocity.
Methods
Participants
We performed a retrospective analysis of pediatric patients who sustained TT fractures treated with ORIF at a Level 1 pediatric trauma center. After the study protocol received institutional review board approval, we reviewed all relevant radiographic images and measured PTSA at specific time points. Radiographic follow-up was not standardized, but measurements were generally taken at time of injury and at approximately 3 months, 6 months, and 1-year postoperatively. Longer-term follow-up timepoints were included when available.
Displaced TT fracture (Ogden type 2B or greater) was an indication for operative fixation. Patients undergoing all fixation methods (screw, K-wire, and suture anchor) were included. Patients were excluded from the study if they were >18 years old at the time of injury, underwent nonoperative treatment, had a fracture pattern precluded accurate measurement of PTSA, had less than 6 months of postoperative radiographic follow-up, or were skeletally mature at the time of index assessment. Each knee was assessed separately for patients who had bilateral TT fractures. Nondisplaced fractures that were managed nonoperatively were not included in the analysis. Lateral knee radiographs from the index assessment and subsequent follow-up timepoints were included for PTSA measurement.
PTSA Measurement, Bone Age Determination, and Fracture Classification
Bone age at the time of injury was determined using radiographic standards in the Pyle and Hoerr Atlas. 26 PTSA was measured between the long axis of the tibia, defined by a line bisecting 2 perfect circles drawn in the proximal tibia at roughly 5 cm and 15 cm distal to the articular surface abutting the anterior and posterior tibial cortex, and a best parallel line to tibial articular surface (Figure 1).15,19 In 3 knees in which inadequate tibial length was visible to determine the long axis, the fibula long axis was used instead. The measurement method was consistent for all radiographs for a particular patient. Negative slope value indicated posterior tibial slope, whereas a positive value indicated relatively anterior slope (Figure 1).
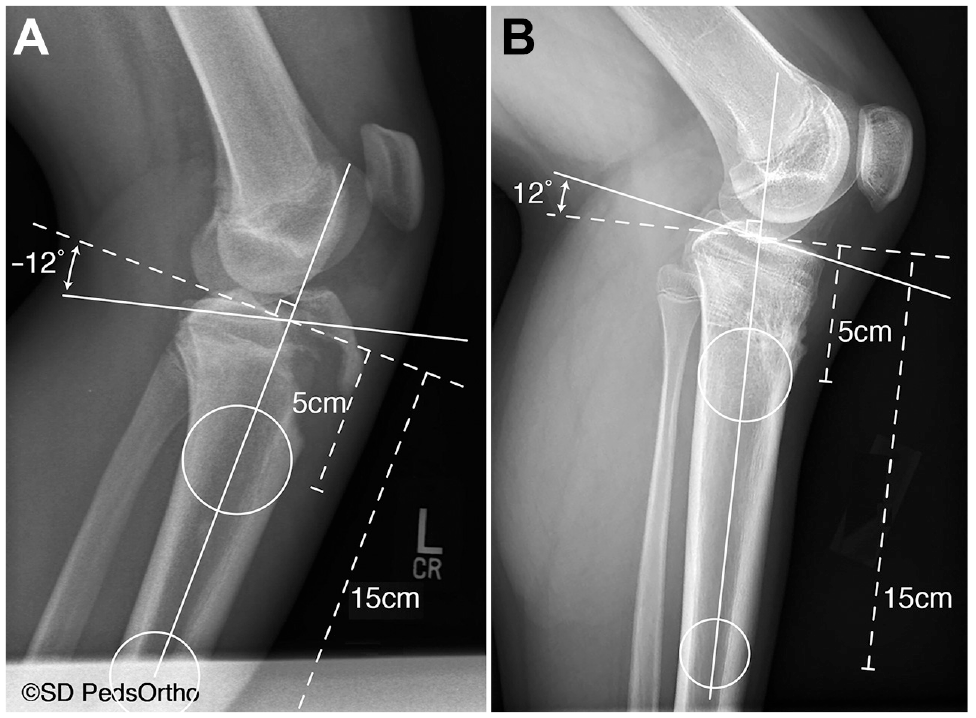
Lateral radiographs depicting the circle method for determining PTSA in 2 patients, with examples of (A) a relatively posterior tibial slope denoted by an angle of -12° and (B) a relatively anterior slope denoted by an angle of 12°. PTSA, posterior tibial slope angle.
Tibial slope measurements were performed by a single researcher, and bone age determination was performed by a separate researcher, both of whom were blinded to each other's respective calculations. A random sample of measurements that were repeated by the original researcher and a separate researcher to calculate intra- and interrater reliability demonstrated an acceptable level of agreement (intraclass correlation coefficient >0.75). 17 Fractures were classified using the Ogden (modified Watson-Jones) classification. 23 Demographic data were also collected via chart review.
Statistical Analysis
Descriptive statistics (mean and standard deviation) or mean (range) were used to characterize baseline demographics (chronological age, bone age, sex, height, weight, body mass index [BMI]), follow-up length, and overall change in PTSA for the entire group. PTSA measurements were plotted and univariate linear regression analyses were used to determine the rate of change of slope angle (ΔPTSA; degrees per month) from index to final follow-up. Linear regressions were generated for individual patients to determine each patient's ΔPTSA across their follow-up timepoints, as well as for entire cohort and sex-based aggregate data. The Pearson correlation coefficient (r) was used to compare PTSA with months postfixation for the whole cohort. A generalized estimating equation (GEE) analysis was also performed to determine a total cohort slope.
Individual patient PTSA trends were then stratified based on radiographically determined bone age and averaged to obtain mean ΔPTSA values for each bone age as well as bone age groupings (10-12, 13-14, and 15-16 years). Analysis of covariance (ANCOVA) was used to determine the interaction of patient sex, fixation method, and Ogden classification in the whole cohort model. Significance for all statistical analyses was set at P < .05. Statistical analysis was performed using SPSS Version 27.0.1 (IBM).
Results
A total of 28 patients who underwent operative treatment for TT fracture between 2013 and 2022 were screened, and 22 (79%) patients (23 knees) met inclusion criteria. Five (17.9%) patients were excluded for having less than 6 months of postoperative radiographic follow-up, and 1 (3.6%) was excluded for a fracture pattern that extended significantly into the tibial plateau that precluded measurement of index PTSA. Of the 3 patients with bilateral TT fracture, 2 had 1 knee treated nonoperatively, and the nonoperative knee was not included in the analysis. Mean follow-up for operatively treated knees was 17 months (range, 6-52 months). Mean chronological age was 14 years (range, 10-16 years), and mean bone age was 14 years (range, 10-16 years) at the time of injury. The majority of patients were male (86%) and underwent ORIF with screw fixation (82%) (Table 1). The majority of TT fractures in our cohort were displaced with fracture extension through the epiphysis (73.9%; Ogden 3B) while the remainder were Ogden 2B (26.1%), which is a displaced fracture between proximal apophysis and epiphysis.
Demographic and Baseline Characteristics for Patients With Operatively Managed TT Fractures (N = 22) a
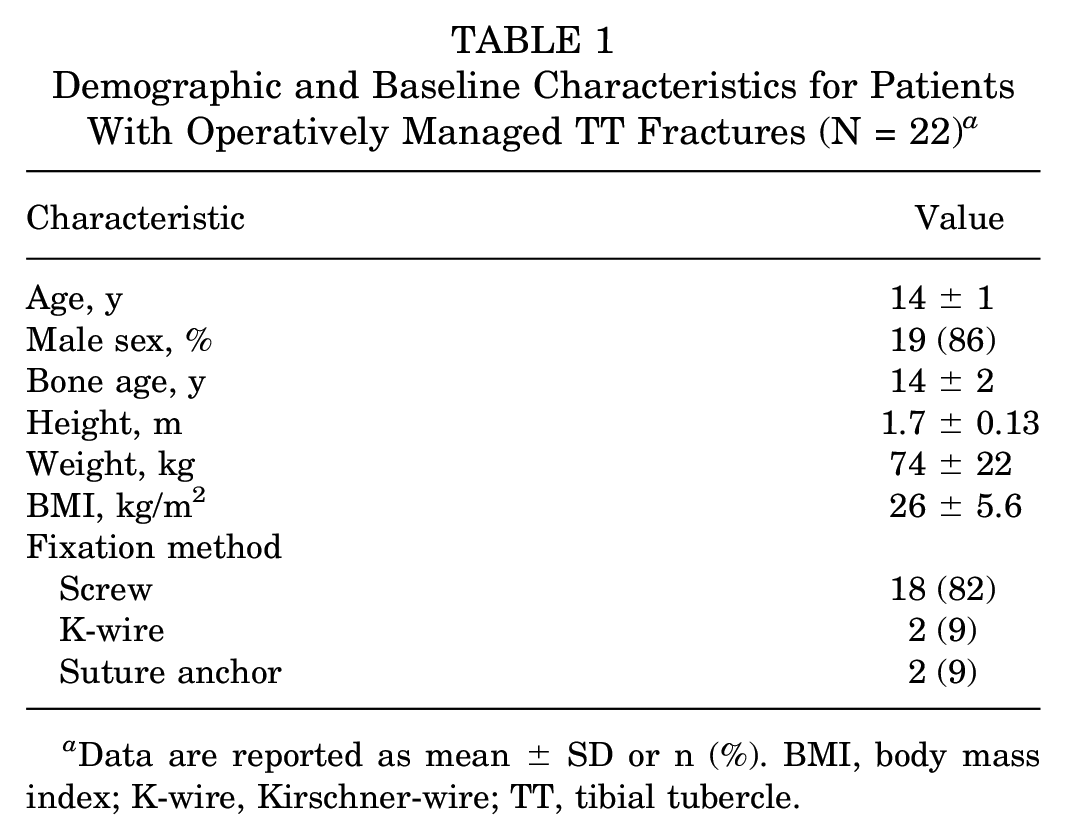
Data are reported as mean ± SD or n (%). BMI, body mass index; K-wire, Kirschner-wire; TT, tibial tubercle.
Overall, patients had a mean PTSA of -12°± 2.4° at the time of injury. The ΔPTSA for each patient after fracture fixation ranged from -0.27° to 0.97° per month, with an overall mean ΔPTSA of 0.30°± 0.31° per month across all patients. There were 2 patients with a negative ΔPTSA (slope became more posterior): -0.27° per month for a patient of bone age 12, and -0.08° per month for a patient of bone age 13. For the entire cohort, PTSA was correlated significantly with months postfixation (r = 0.71; P < .001). Linear regression revealed a significant relationship between months postfixation and PTSA, demonstrating a ΔPTSA of 0.31° per month (95% CI, 0.24°-0.38°; P < .001) (Figure 2).
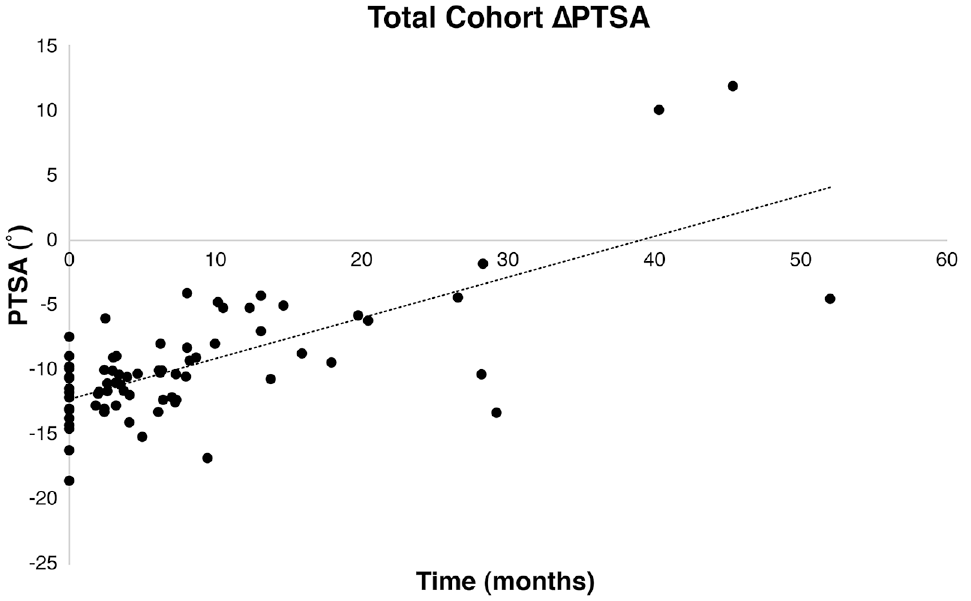
Scatterplot depicting aggregate PTSA data for the entire cohort at time of injury and at follow-up repeat radiographs. Pearson's r2 was 0.50 (P < .001), with linear regression demonstrating a ΔPTSA of 0.31° per month (95% CI, 0.24°-0.38°; P < .001). CI, confidence interval; PTSA, posterior tibial slope angle; ΔPTSA, change in PTSA.
A GEE analysis resulted in similar slope of 0.313° (95% CI, 0.12° to 0.50°; P < .001). When stratified by bone age, we obtained the following ΔPTSA values: 0.41°± 0.12° per month at 10 years, -0.10°± 0.24° per month at 12 years, 0.40°± 0.42° per month at 13 years, 0.58°± 0.44° per month at 14 years, 0.18°± 0.12° per month at 15 years, and 0.31°± 0.14° per month at 16 years; there were no data for bone age 11 years. When separated into 3 bone age groups, the highest ΔPTSA was observed among the 13 to 14 bone age group (0.49°± 0.41° per month) (Figure 3). The average overall absolute change in PTSA from surgery to final follow-up was 4.1° (range -3.4° to 21°).

Graph depicting the mean ΔPTSA for patients by bone age grouping. The greatest mean ΔPTSA was observed in the 13 to 14 bone age group (0.49°± 0.41° per month). Error bars depict standard deviations. PTSA, posterior tibial slope angle; ΔPTSA, change in PTSA.
K-wire fixation with interval removal was used infrequently in our study cohort (n = 2) and was used in the small/comminuted fracture patterns that were not amenable to screw fixation. One patient (chronological age, 10 years; bone age, 10 years) receiving K-wire fixation had a ΔPTSA of 0.50 per month (95% CI, 0.40 to 0.60; P < .001), eventually requiring a slope correcting osteotomy at 48.6 months after the initial injury film date. The second patient (chronological age, 14 years; bone age, 15 years) had a ΔPTSA of 0.45 per month (95% CI, -6.6 to 7.5; P = .56). Suture anchor fixation was also infrequent in our study (n = 2) and performed in the setting of TT fractures with a concomitant partial patellar tendon rupture.
There were a small number of female patients included in this cohort (n = 3) with bone ages of 10, 12, and 13 years, respectively, and all underwent ORIF with screw fixation. Among the male knees (n = 20), there was a significant relationship between months after surgery and PTSA (0.31° per month; 95% CI, 0.24° to 0.39°; P < .001). There was a similar relationship observed among the female knees (0.34° per month; 95% CI, 0.020° to 0.65°; P = .040).
An ANCOVA model was generated to determine whether the linear regression of PTSA and months from fixation was influenced by sex, Ogden classification, fixation method, and variable interaction effects. The model revealed no significant interaction between the above factors and the regression between PTSA and months from fixation.
Discussion
To our knowledge, this is the first study that utilized TT fractures as a model to quantify change in PTSA. In our cohort, we found a significant decrease in PTSA after ORIF of a displaced TT fracture in skeletally immature patients. Furthermore, we found that the greatest rate of change in tibial slope angle occurred at bone age 14 years, corresponding with peak growth velocity for men. 16 Our findings depict the natural progression of change in PTSA after ORIF of displaced TT fracture and serve as a model to understand change in PTSA after anterior epiphysiodesis.
Excessive posterior tibial slope is a known risk factor for ACL injury, graft failure, and ACL revision in both pediatric and adult patients.9,10 The proposed mechanism is greater PTSA leading to increased anterior tibial translation and strain on the ACL, which increases its risk of injury. 2 Given that most of the knees assessed in this study experienced a relatively anterior change in slope (21 of 23; 91.3%), it is possible that TT fracture may decrease risk of future ACL injury.
Our data may inform the utility of an anterior tibial epiphysiodesis during ACLR or revision (essentially simulating TT ORIF) in select skeletally immature patients. A recent study demonstrated an 11-fold risk of ACL graft failure among patients with PTSA ≥12° (-12° by the convention used in this study). 25 One review theorized using anterior correcting wedge osteotomy (ACWO) in patients with PTSA ≥12° and instability after ACLR, even considering primary ACWO during ACLR for patients with extreme pathologic slope. 3 For skeletally immature patients, screw anterior tibial epiphysiodesis with fixation may be considered at the time of ACLR as a minimally invasive intervention for patients who are expected to have further steepening of PTSA either on the basis of their bone age or demonstrated progression using previous ipsilateral radiographs. A similar technique was described in a small case series (n = 8) implementing hemiepiphysiodesis at the time of ACLR to correct genu valgum as a risk factor for graft failure. They reported successful procedural implementation and correction of malalignment, although with similar rates of graft failure compared with control. 22 The data from our study may help to predict rate and overall change in tibial slope as well as the optimal timing (ie, bone age) for an anterior epiphysiodesis at time of ACL surgery.
While arrest of the anterior tibial physis may have a beneficial effect on reducing the risk of ACL injury and graft failure, excessive anterior tibial slope may result. This was exemplified by 1 of the patients in our study who sustained a displaced TT fracture and who eventually received a slope correcting osteotomy for clinical recurvatum (Figure 4). This corroborates previous studies that have demonstrated genu recurvatum as a potential sequela of fixation of a displaced TT fracture.18,21,24 Our study further confirms this possibility of recurvatum after displaced TT fractures and may help predict the rate at which this may occur depending on bone age. 28 Furthermore, it has been shown that anterior tibial slope can cause increased strain on the PCL and may increase risk of PCL injury.1,5 Thus, optimal timing of an anterior epiphysiodesis is essential to prevent overcorrection of tibial slope and the subsequent risk of recurvatum and PCL injury.

Radiographs from a single study patient (male; chronological age, 10 years; bone age, 10 years) from the time of TT fracture to after ORIF with K-wires and interval removal, demonstrating progressively more anterior (ie, more positive) tibial slope over the follow-up interval. K-wire, Kirschner-wire; ORIF, open reduction internal fixation; TT, tibial tubercle.
In addition, the risk of sustaining a TT fracture in the first place may be increased in patients with more posterior slope before injury. 27 Sheppard et al 27 found that patients with TT fracture had a PTSA of -10.20°± 4.25° (mean ± SD; negative by our convention), which is similar to the index PTSA in our cohort (-12°± 2.4°) and more posterior than the baseline population.
An important consideration in this study is whether the fracture, fixation construct, or both contribute to physeal arrest. While the true causation could not be determined by this study, we analyzed whether the fracture pattern or method of fixation had any influence on the PTSA regression. Fractures involving more of the proximal tibial epiphysis, as indicated by the Ogden classification, could potentially cause a greater degree of growth arrest. 14 However, Ogden classification in our cohort did not significantly influence the overall PTSA trend. Furthermore, fixation method did not have a significant influence on the PTSA trend in our study. However, the relatively small number of fractures fixed with K-wires and suture anchors limits our ability to determine whether these fixation methods may have had a different effect on growth arrest compared with screw fixation. Given that these fixation methods differ in terms of construct stability and interposition in the physis compared with a screw, it is plausible that construct type could have differing influence on ΔPTSA. This could be the subject of future study; however, screw fixation would be the most likely construct used in the setting of anterior epiphysiodesis for increased slope and is the construct from which the vast majority of our data was generated.
Limitations
Our study has several important limitations. Being a retrospective case series, this study may be subject to selection bias and confounding variables. Addition of a control group would have strengthened the validity of our findings; however, there is inherent difficulty in finding healthy knee patients who have serial radiographic follow-up in a similar interval to our cohort, and are also bone-age- and sex-matched to our study cohort. The majority of patients in this study were male, and therefore, our data might not be generalizable to female patients, although the 3 female patients in our study did show overall similar loss of posterior slope after injury. Our study had relatively low sample size and is thus underpowered to determine statistically significant differences between groups, especially regarding method of fracture fixation. Furthermore, there was likely some degree of error in measuring PTSA and determining bone age, as there was some inconsistency in radiographic quality and type (ie, imperfect lateral views, tibia/fibula vs knee radiographs). However, we were able to confirm intra- and inter-rater reliability. There was a wide range of radiographic follow-up in this study; it is possible that complete overall changes in PTSA were not captured for younger patients with follow-up that did not reach skeletal maturity. Finally, there were 2 patients (8.7%) who observed a slight increase of posterior slope rather than loss of posterior slope, which was observed in the majority of patients. This may have been the result of 1 or more of the above factors, including variation of growth plate disruption, intrinsic growth variations, variability in measurement, and inconsistent radiographic follow-up. Further prospective studies using larger sample sizes, more consistent radiographic technique, and consistent, long-term follow-up are therefore warranted. Nevertheless, our data offer important insight into changes in tibial slope after TT fracture and should prompt further research on this topic, especially as it relates to reducing the risk of ACL injury or graft failure in skeletally immature patients.
Conclusion
Our data demonstrated that PTSA becomes progressively more anterior after injury and subsequent surgical fixation. Furthermore, the greatest rate of change in PTSA corresponded with peak growth velocity (bone age 14 years in men), which was consistent with our hypothesis. This concept may serve as a model in clinical practice and future studies to detail modulation of excessive PTSA in the pediatric ACL-deficient knee.
Footnotes
Final revision submitted July 10, 2023; accepted August 16, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.M.Z. has received education payments from ImpactOrtho and SportsTek Medical. A.T.P. has received education payments from ImpactOrtho and SportsTek Medical and consulting fees from OrthoPediatrics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from University of California at San Diego (ref No. 192008).