
Abstract
Purpose
Few studies have assessed the link between tibial tubercle (TT) morphology and anterior cruciate ligament (ACL) injury, and most focus only on the TT–trochlear groove (TT–TG) distance. This study aimed to examine the relationship between ACL injury, TT morphology, and posterior tibial slope (PTS) by comprehensively evaluating TT-related radiological parameters.
Methods
Radiological images of 100 patients who underwent isolated ACL reconstruction for non-contact injury between 2016 and 2022 and 100 demographically matched controls with no relevant abnormalities on knee MRI were retrospectively analyzed. Thirteen radiological parameters were measured and compared, including PTS; TT torsion (TTT); TT-rotational angle (TT-RA); plateau axis–tuberosity axis (PA-TA); TT-TG; TT–PCL distance and ratio; TT lateralization (TTL) distance and ratio; TT height (TTH); and TT angle (TTA). Associations between these parameters and ACL injury, as well as interparameter correlations, were evaluated using t-tests, logistic regression, ROC analysis, and Pearson correlation.
Results
Mean TTT, TT-RA and PA-TA values were significantly lower in the ACL injury group (5.68° vs 8.34°, p < .001; 7.96° vs 12.09°, p < .001; 8.41° vs 11.58°, p < .001). Conversely, TT-TG, PTS and TTH were higher (10.69 mm vs 8.17 mm, p < .001; 12.84° vs 10.61°, p < .001; 11.69 mm vs 10.02 mm, p < .001). Logistic regression showed TTT (OR = −0.849), TT-RA (OR = −0.822), TT-TG (OR = 1.298), PTS (OR = 1.177), and TTH (OR = 1.327) independently associated with ACL injury.
Conclusion
In isolated ACL injury patients, TT torsion was lower and TT prominence higher. TT morphology assessment may help personalize ACL reconstruction, identify high-risk individuals, and support future clinical and biomechanical research on ACL injury susceptibility.
Introduction
The development of anterior cruciate ligament (ACL) injury is extensively studied, with numerous risk factors identified, particularly those associated with anatomical variations.1–3 Regarding anatomical factors, coronal, and sagittal malalignment of the knee, including varus and valgus deformities and a steep posterior tibial slope (PTS), have been recognized as anatomical risk factors that increase the risk of ACL injury.4–8 Compared to coronal and sagittal malalignments, studies investigating the impact of axial malalignment on ACL injury have increased in recent years, and tibiofemoral rotation has been recognized as an important factor associated with the risk of ACL injury.9,10
Biomechanical and clinical studies have demonstrated that increased internal rotation of the tibia relative to the femur elevates the strain on the ACL by enhancing anterior tibial translation during axial loading, thereby contributing to the development of ACL injury.10–13 Previous studies have reported an association between an increased tibial tubercle–trochlear groove (TT–TG) distance and ACL injury.14,15 It has been proposed that a greater TT–TG distance may lead to increased internal rotation of the tibia in the axial plane, thereby elevating the rotational load on the ACL and contributing to a higher risk of injury. 15 Numerous studies have examined the relationship between the tibial tubercle (TT) position, lateralization, rotation, torsion, and patellofemoral instability.16–18 Literature data linking TT morphology to the risk of ACL injury remains limited. Moreover, the limited existing evidence is confined to the association between an increased TT–TG distance, a quantitative indicator of TT lateralization, and ACL injury. 15 However, although the TT–TG distance provides indirect information about axial malalignment, it may not fully represent true TT malposition owing to its susceptibility to factors such as age, patient size, femur–tibia flexion angle, and tibiofemoral rotation. 14 To minimize the influence of tibiofemoral rotation, the tibial tubercle rotational angle (TT-RA) and plateau axis–tuberosity axis (PA-TA) angles have been defined based solely on tibial anatomical landmarks to represent torsion of the TT,19,20 whereas the tibial tubercle–posterior cruciate ligament (TT-PCL) and tibial tuberosity lateralization (TTL) distances and ratios have been introduced to quantitatively assess its lateralization.21,22
To the best of our knowledge, no study has specifically investigated the association between isolated malpositioning of the TT (i.e., its lateralization, rotation, and torsion relative to the proximal tibia, independent of the femur) and ACL injury. The primary aim of this study was to radiologically evaluate the morphology of the TT in patients who underwent ACL injury. The secondary aim was to investigate the relationship between TT rotational, torsional, and lateralization parameters and other radiological parameters such as PTS and TT–TG distance, both of which have been associated with ACL injury in previous studies. The hypothesis of this study was that radiological parameters indicating TT malposition may differ between patients who underwent ACL rupture and controls. Radiological parameters related to the TT may enhance the predictive value of PTS for ACL injury. Furthermore, we propose that these measurements may be independently associated with ACL injury, apart from established parameters such as PTS and TT–TG distance.
Methods
This study was a retrospective, cross-sectional investigation. The study protocol received approval from the institutional ethics committee. The medical records of patients who underwent ACL reconstruction for isolated complete ACL rupture due to non-contact injury at our clinic between January 2016 and January 2022 were reviewed, and 100 patients with available preoperative magnetic resonance imaging (MRI) and lateral knee radiographs were included.
A control group of 100 patients with similar age and sex distribution, a history of minor trauma, no specific knee pathology suspected on physical examination, no detectable pathology on MRI, and in whom ACL rupture was excluded, was selected.
Radiological images of all patients were retrospectively evaluated. Data were obtained from the hospital’s electronic medical records system. The exclusion criteria were: age <18 years, suboptimal MRI or lateral radiograph quality, history of patellofemoral instability, patellar tendon or ligament injury, major trauma, prior lower extremity fractures or surgeries, and lower limb malalignment (e.g., varus/valgus deformities, limb length discrepancy).
The schematic illustrations of the measurement techniques for radiological parameters are shown in Figure 1. The tibial tubercle torsion (TTT), TT-RA, PA-TA, tibial tuberosity–trochlear groove (TT-TG) distance, TT-PCL distance and ratio, and TTL distance were measured on axial MRI images. PTS, TT height (TTH), and TT angle (TTA) were measured on true lateral radiographs. TT–PCL and TTL ratios were obtained by dividing each distance by the tibial width. Schematic illustration of radiologic parameters measured on axial MRI. TTT: tibial tubercle torsion; TT-RA: tibial tuberosity – rotation angle; PA-TA: plateau axis -tuberosity axis; TT-TG: tibial tubercle -trochlear groove; TT-PCL: tibial tubercle - posterior cruciate ligament; TTL: tibial tuberosity lateralization.
Measurement of torsional parameters associated with TT
The TTT
As defined by Chassaing et al., this angle is measured between the line connecting the posterior femoral condyles and the line passing through the medial and lateral edges of the patellar tendon at its most proximal insertion into the TT (Figure 2).
23
Measurement of torsional parameters associated with TT on axial magnetic resonance imaging scans. (a) The torsion of TT, defined as TTT, relative to the posterior condylar line of the femur. (c) The torsion of the TT, defined as TT-RA, relative to the dorsal condylar line of the tibial plateau. (b) The torsion of the TT, defined as PA-TA, relative to the plateau axis (PA) line passing through the geometric center (GC) of the tibial plateau. (d) Proximal tibial torsion (PTT), defined as the torsion of the dorsal line of the tibia at the axial MRI slice where the tibial tubercle is most clearly visualized, relative to the dorsal line of the tibial plateau.
The TT-RA
As described by Kim et al., the angle was measured between the dorsal condylar line of the tibia—on the section where the posterior cruciate ligament (PCL) is clearly visible—and the line drawn through the medial and lateral edges of the patellar tendon at its most proximal insertion on the TT (Figure 2). 19
The PA-TA
Following the method described by Polat et al., the PA–TA angle was measured between the plateau axis (PA), defined as a line perpendicular to the posterior condylar axis through the tibial geometric center, and the tuberosity axis (TA), which is the bisector of the angle between lines tangent to the medial and lateral cortices of the TT (Figure 2). 20
Measurement of radiological parameters related to TT lateralization
The TT-TG
The distance between the perpendicular line drawn from the deepest point of the trochlear groove and the perpendicular line drawn from the TT to the posterior condylar line of the femur was measured as described by Schoettle et al. (Figure 3).
24
Measurement technique of radiological parameters related to TT lateralization on MRI (a) The TT-TG distance is defined as the distance between the perpendicular lines drawn from the trochlear groove (a) and TT prominence (b) to the femoral posterior condyles. (b) Measurement of TT-PCL and TTL distances and ratios (a) A perpendicular line was drawn from the medial border of the PCL to the dorsal condylar line of the tibia. (b) Perpendicular line drawn from the TT prominence to the dorsal line of the tibia. (c) The lateral border of the tibia; (d) The medial border of the tibia; (a-b). The TT-PCL distance; (b–d). The TTL distance; (c-d). The tibial width; (a-b/c-d). The TT-PCL ratio; (b–d/c-d). The TTL ratio.
The TT-PCL
Using the methods described by Seitlinger et al. and Tensho et al., the mediolateral distance between the tip of the tibial tubercle and the medial border of the PCL was measured (Figure 3). 21
The TTL
According to the method described by Tensho et al., TTL was measured as the mediolateral distance between the tip of the tibial tubercle and the medial edge of the tibial condyle (Figure 3). 22
Radiological parameters measured on the lateral radiograph
The PTS
In previous studies, the PTS was defined as the angle between the tangent to the medial tibial plateau and the anatomical axis of the tibia on true lateral radiographs.25,26 The anatomical axis was determined by a line perpendicular to the midpoint of the anterior and posterior cortices measured at 5 and 15 cm distal to the joint line (Figure 4). Radiological parameters measured on the lateral radiograph. (a) The measurement of PTS, defined as the angle between the tangent of the medial plateau line and the anatomical axis of the tibia (vertical dashed line). The anatomical axis of the tibia was determined by connecting the midpoints (centers of the blue circles) of the anterior and posterior cortices of the tibia located 5 and 15 cm distal to the knee joint. (b) The measurement of TTH (red line), defined as the perpendicular distance from the reference line (dashed line) to the most prominent anterior part of the TT. (c) TTA (red angle), defined as the angle between the endpoints of the reference line (dashed line) and the most prominent anterior part of the TT.
TTH and TTA
As described by Rosenthal et al., TTH was measured as the perpendicular distance from the most prominent point of the tibial tubercle to a reference line drawn 10 cm distal to the anterior tibial cortex. The TTA was defined as the angle between the line endpoints and the most prominent anterior point (Figure 4). 27
Statistical analysis
The sample size was calculated using G*Power software (version 3.1.9.4, Heinrich Heine University, Düsseldorf) by entering the mean and standard deviation values. By accepting an effect size of 0.5, an alpha level of 5%, and a power of at least 80%, it was determined that a minimum of 99 patients was required in each group.
All parameter measurements were conducted in two separate sessions by two observers who were blinded to each other and the diagnoses. Data were analyzed using SPSS software (IBM- Version 27.0; Armonk, NY, USA). Descriptive statistics and frequency analyses were used to analyze the data.
The intra- and inter-class correlations between the measurements made by the same observer in separate sessions and those made by the two observers were assessed using the intra-group correlation coefficient (ICC). In this context, ICC values below 0.5 indicate poor reliability, values between 0.5 and 0.74 indicate moderate reliability, values between 0.75 and 0.9 indicate good reliability, and values above 0.90 indicate excellent reliability.
The mean values and confidence intervals of the 10 measurements were entered into a computer. Normality assessment of the numerical data was performed using the Shapiro-Wilk test. Independent sample t-tests and Mann-Whitney U tests were used to compare independent variables, where p < 0.05 were considered significant. Correlation analyses were performed using Pearson’s and Spearman’s rho tests. Receiver operating characteristic (ROC) analysis was performed to determine pathological thresholds, differentiate patients based on measurements, and establish cutoff values. The results are presented as the area under the curve (AUC), cutoff points, sensitivity, and specificity. Logistic regression analysis was used to investigate whether the parameters were associated with an ACL injury independently of other parameters.
The power of the study was reassessed after statistical analysis (post hoc). Post-hoc power calculations were performed using G*Power software, with an alpha error of 0.05 for two-tailed significance testing.
Results
ICC results of both groups a .

aICC values for intra-rater (observer 1 and observer 2) and inter-rater reliability are presented for both groups. Higher ICC values indicate better measurement reliability.
Demographic characteristics of the patients a .

aFindings are presented as n (mean), ±SD, median (min-max), n (%).
T-test, Pearson chi-square test.
Comparison of the mean values of radiological parameters related to TT (Tibial tubercle) a .

Boldface p values indicate a statistically significant difference between groups (p < .05).
aData are reported as mean ± SD (min-max).
Correlation of the mean values of radiological parameters related to TT (tibial tubercle) a .
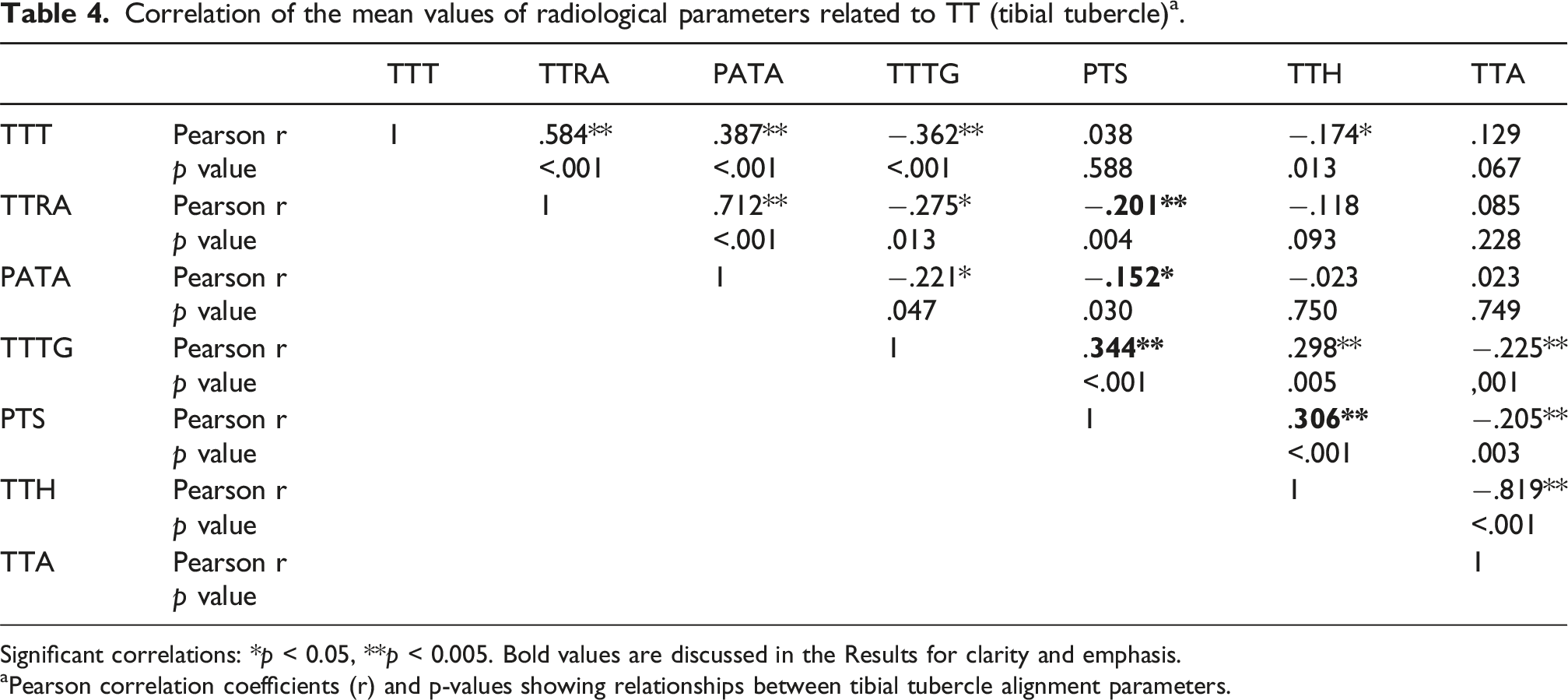
Significant correlations: *p < 0.05, **p < 0.005. Bold values are discussed in the Results for clarity and emphasis.
aPearson correlation coefficients (r) and p-values showing relationships between tibial tubercle alignment parameters.
Results of the logistic regression analysis a .

aBoldface p values indicate statistical significance (p < .05).
Receiver operating characteristic (ROC) analysis of TT-TG, PTS, TTH, and tibial tubercle torsional measurements.
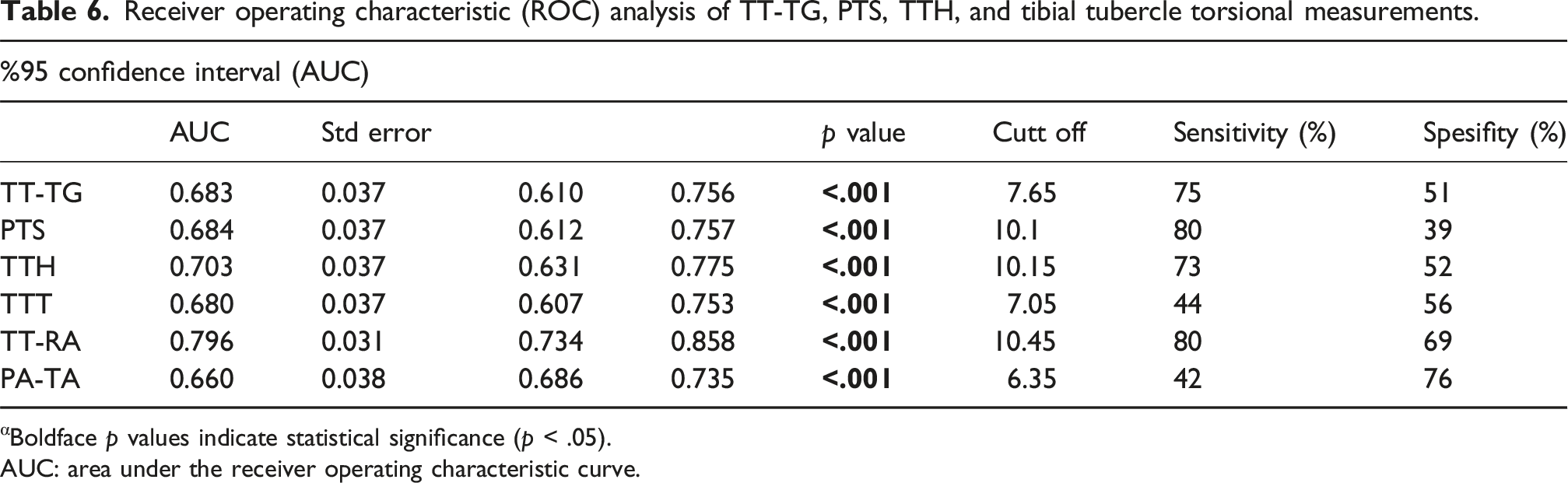
αBoldface p values indicate statistical significance (p < .05).
AUC: area under the receiver operating characteristic curve.

Receiver operating characteristic (ROC) curve of radiological parameters (a) ROC curve of torsional parameters of TT; TTT (blue curve line) (AUC: 0.680), TT-RA (red curve line) (AUC: 0.796), and PA-TA (green curve line) (AUC: 0.660) (b) ROC curves for TT-TG (blue curve line) (AUC: 0.683), PTS (red curve line) (AUC: 0.684), and TTH (green curve line) (AUC: 0.703).
Discussion
Key findings
The most important finding of this study was that the parameters reflecting TT torsion (TTT, TT-RA, and PA-TA) were significantly lower in the ACL injury group than in the control group, whereas the TT-TG distance, which represents the TT position, and TTH, which reflects TT prominence, were significantly greater. These results suggest that patients undergoing ACL injury may exhibit abnormal TT torsion and increased TT prominence.
Biomechanical interpretation
Chassaing et al. suggested that all three positional abnormalities associated with TT (TT torsion, TT TG distance, and TT rotation) are related to patellar instability and may originate from a common underlying factor, such as tibial torsion. 23 If these parameters are associated with tibial torsion, we hypothesize that increased internal tibial torsion, which plays a role in the mechanism of ACL injury, may be related to these three positional abnormalities of the TT.
Tibial torsion is a complex parameter that plays a critical role in lower extremity biomechanics and can vary across different segments. Jakob et al., in a cadaveric study, reported that the greatest torsional changes occur in the proximal quarter of the tibia, highlighting the significance of morphological variations at the level of the TT. 28 In a recent imaging-based study, Wang et al. evaluated femoral and tibial torsion parameters using MRI and reported that all parameters, except for proximal tibial torsion (PTT), were significantly higher in cases with ACL injury. It has been suggested that femoral torsion may serve as the primary factor contributing to the torsional loading of the knee. 10 In contrast, Winkler et al. 29 analyzed tibial torsion segmentally and reported that the deformation primarily occurs in the distal tibia and is not directly related to the position of the tibial tubercle. These findings contradict the proximal-focused torsion hypothesis proposed by Jakob et al. PTT is commonly defined as the angle between the line connecting the borders of the posterior tibial plateau at the level of the PCL and the posterior cortex at the level of the TT and is frequently used as a reference in segmental torsion analyses. However, a common limitation of the studies by Wang and Winkler is that the torsional behavior of the TT itself (i.e., TT torsion) was not assessed. While PTT is based on the posterior anatomy of the tibia, TT torsion reflects the rotational orientation of the patellar tendon insertion and represents an anterior tibial morphology-specific parameter (Figure 2).
A proposed mechanism linking tibial tubercle torsion to ACL injury
Increased internal tibial torsion has been shown to alter the direction and magnitude of tibiofemoral contact forces under axial loading conditions, thereby increasing anterior tibial translation and, consequently, elevating the mechanical loading on the ACL.13,30
In studies assessing the rotational position of the TT, its isolated torsional behavior has often been overlooked, with measurements primarily based on femoral references.23,31,32 TT-RA and PA-TA are parameters defined in a limited number of studies that evaluated TT using only tibial references, independent of femoral influence.19,20 In our study, in addition to TTT, TT-RA, and PA-TA were evaluated, demonstrating a significant association between increased isolated internal torsion of the TT and ACL injury. Lower values of these parameters suggest increased internal rotation of the TT relative to the proximal tibia independent of tibiofemoral rotation, indicating that isolated TT malrotation may increase the mechanical load on the ACL and contribute to the risk of rupture. Indeed, our findings suggest that increased internal torsion of the TT may generate rotational stress at the level of the patellar tendon insertion on the tibia, potentially altering the transmission of quadriceps forces across the knee joint and leading to increased internal tibial rotation. 12
From a biomechanical perspective, a TT torsional profile predisposed to internal rotation may cause the patellar tendon insertion on the tibia to be positioned in a relatively internally rotated orientation even at rest. During dynamic activities—particularly at low knee flexion angles (0–30°)—axial tibiofemoral compressive loading acting on this pre-existing internally rotated patellar tendon configuration may generate an additional internal rotational moment on the tibia (Figure 6). Schematic illustration (superior view) demonstrating the potential biomechanical effects of TT torsional alignment on ACL loading under axial tibiofemoral compressive loading at low knee flexion angles (0–30°). (a) Neutral TT torsional configuration. The patellar tendon insertion is aligned without excessive internal rotation, allowing balanced transmission of quadriceps forces and physiologic tibiofemoral kinematics under axial loading. (b) Internally rotated TT torsional configuration. Increased internal torsion of the TT may position the patellar tendon insertion in a relatively internally rotated orientation. Under axial loading, this configuration may increase internal rotational stress acting on the tibia, potentially elevating mechanical loading on the ACL.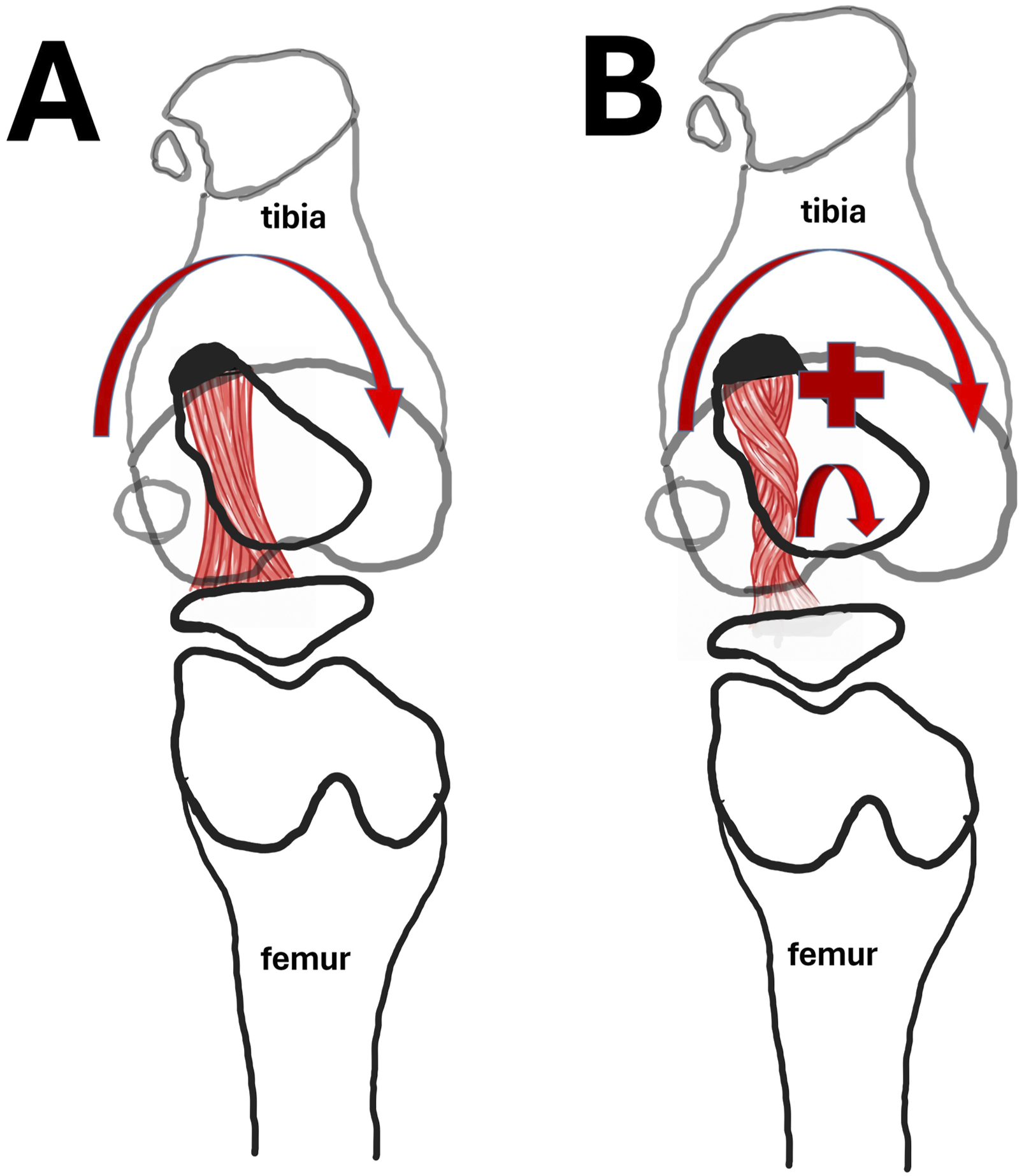
In this mechanism, internal malrotation of the tibial tubercle may shift the patellar tendon force vector toward internal rotational and anteriorly directed components, thereby further increasing internal tibial rotation and ACL loading.
To the best of our knowledge, no previous study has specifically investigated the association between rotational malposition of the TT, defined solely by tibial references, and ACL injury. In this context, our study provides pioneering findings by evaluating femur-independent TT torsion using the TT-RA and PA-TA angles and demonstrating their association with ACL injury.
Through experimental in vitro studies, Chassaing et al. developed a TT osteotomy technique that provided isolated 30° internal torsion of the TT without medializing it while preserving its original rotational alignment in cadaveric models with induced patellar instability. They confirmed that internal torsion of the TT improved patellar stability. 33 Loddo et al. described the Anterior Tibial Tubercle Internal Torsion Osteotomy (ATTITO) technique in a case series of 29 patients with a history of patellar dislocation and increased TTT angle. 34 Our results showed that TT-RA and TT torsion were significantly lower in patients with ACL injury. Whether this reduction is related to the PTS, TT-TG, or other biomechanical factors should be clarified in future studies. As in the study by Chassaing et al., the effect of increased TT internal torsion on ACL loading should be investigated using experimental models. 33 Additionally, based on the case series by Loddo et al., it remains to be determined whether ATTITO increases the long-term risk of ACL injury. 34
An increased medial PTS has been demonstrated to be associated with ACL injury in numerous studies.26,35–37 In our study, PTS was measured from the medial tibial plateau. This approach was based on the belief, as indicated by O’Malley and Vyas, that medial PTS may have a more pronounced effect on anteroposterior translation of the tibia due to its proximity to the tibial attachment site of the anteromedial bundle.36,37 Visuri et al. conducted the first comprehensive measurement of the TT on lateral knee radiographs of patients with Osgood-Schlatter disease (OSD). 38 Green et al. suggested that growth stimulation of the TT in OSD may predispose to increased PTS. 25 Yaka et al. demonstrated an association between increased PTS and both ACL injury and OSD in the pediatric population. 39 However, these findings do not extend to the general adult population. Considering the external tibial torsion mechanism in OSD 40 and our findings indicating a relationship between ACL injury and internal tibial torsion of the TT, the rare coexistence of ACL injury and OSD, despite both being associated with increased PTS, raises the possibility that these two conditions may exert compensatory biomechanical effects. Rosenthal et al. defined TTH and TTA parameters to assess TT prominence and reported their correlation with increased PTS, which is associated with ACL injuries in the general population. 27 However, this study did not directly investigate the relationship between TTH or TTA and ACL injury. In our study, patients who underwent ACL injury demonstrated significantly higher TTH values and significantly lower TTA angles, with TTH identified as the most predictive parameter in the regression analysis. Additionally, the PTS was found to correlate positively with TTH and negatively with TTA. These findings are consistent with those reported by Rosenthal et al. 27
A proposed mechanism linking tibial tubercle prominence to ACL injury
An increased anterior prominence of the tibial tubercle may alter the line of action of the patellar tendon, thereby increasing the anteriorly directed component of quadriceps force transmission across the tibiofemoral joint. In the presence of an increased PTS, this configuration may facilitate anterior tibial translation under axial loading conditions, potentially contributing to increased mechanical loading on the ACL.
Although the present study was not designed to establish a causal relationship, the observed associations among TTH, TTA, and PTS suggest that tibial tubercle prominence may represent one of the radiological morphological features that should be considered in the context of ACL injury. Furthermore, a pronounced anterior prominence of the tibial tubercle may, over time—particularly during periods of growth and repetitive loading—increase the anteriorly and superiorly directed tensile forces transmitted to the tibia via the patellar tendon. This process may influence the sagittal morphology of the proximal tibia and potentially contribute to an increase in PTS (Figure 7). However, validation of this hypothesis requires longitudinal biomechanical and clinical studies that also account for developmental processes. Schematic illustration showing different knee morphologies with respect to tibial tubercle prominence and PTS. (a) Knee morphology with physiological tibial tubercle prominence and normal posterior tibial slope. (b) Knee morphology characterized by increased anterior prominence of the tibial tubercle and increased posterior tibial slope, representing a knee configuration at increased risk for ACL injury.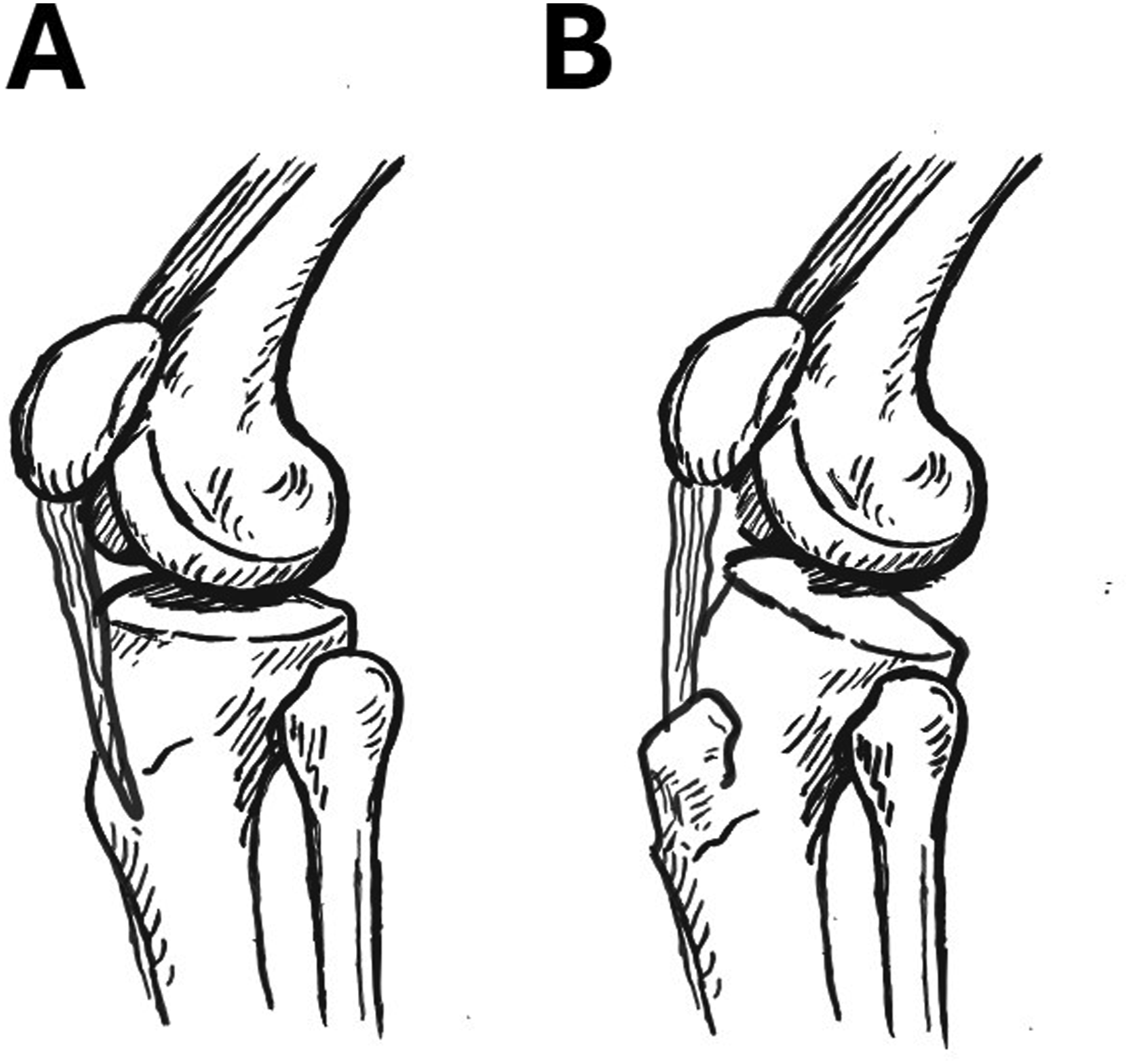
Clinical implications
The observed correlation between the PTS and torsional parameters of the TT supports the notion that beyond TT overgrowth, the torsional morphology of the TT is also quantitatively related to the sagittal morphology of the proximal tibia. This positions our study among the few studies that highlight the connection between TT morphology and ACL injury, thus contributing to the literature. Comprehensive evaluation of anatomical and morphological risk factors related to TT is essential for identifying individuals at high risk of ACL injury on MRI and radiographs. This may guide the development of preventive strategies and personalized surgical approaches, including osteotomies targeting TT torsion and overgrowth correction, when necessary.
In addition to the assessment of primary ACL injury risk, evaluation of tibial tubercle–related torsional and morphological parameters in future studies involving patients with ACL graft failure or re-rupture may allow a more comprehensive understanding of clinical decision-making in this patient population. In particular, in cases with unexplained clinical outcomes or those requiring revision ACL reconstruction despite standard surgical and rehabilitation approaches, tibial tubercle–related torsional mechanisms may represent potential contributing factors and warrant further investigation.
Limitations
Although the power analysis was adequate, the extensive and stringent exclusion criteria substantially reduced the number of eligible participants, thereby resulting in a smaller sample size. Consequently, studies with larger cohorts are warranted. Although the groups were matched for age and sex, the lack of assessment of potential confounding variables—such as body mass index, physical activity levels, quadriceps muscle weakness, and hamstring tightness—represents a significant limitation of the study. This limitation is related to the retrospective design of the study and the lack of standardized documentation of these parameters in the patient records. Consequently, the retrospective nature of the study underscores the need for prospective data collection and further investigation of factors associated with ACL injury.
The lateral and medial tibial plateau slopes differ, and some studies have suggested that the lateral tibial plateau slope may be a more sensitive risk factor for ACL injury.41,42 The assessment of only the medial tibial plateau slope in our study represents a limitation, as evaluating both slopes concurrently could have provided a more comprehensive risk assessment.
Conclusion
This study demonstrated that, in patients with isolated ACL injury, TT torsion was significantly lower, whereas TT prominence was significantly greater compared with the control group.
The assessment of TT morphology may offer valuable insights for individualizing ACL reconstruction surgery, identifying high-risk populations, and developing preventive strategies. Our findings provide a foundation for future simulation and biomechanical studies of knees with varying TT morphologies and may open new avenues for investigating the role of TT morphology in ACL injury susceptibility and graft failure.
Footnotes
Acknowledgements
Ethical considerations
This study was approved by the Ethics Committee of Necmettin Erbakan University (Approval No: 2025/5581]).
Consent to participate
Informed consent was obtained from all patients that their radiological images would be used for scientific purposes in accordance with the decision of the university ethics committee.
Author contributions
(According to ICMJE), The original idea of the study was conceived by H.Y. The methodology was validated by O.B. and M.F.K. Data were collected by M.F.K, H.Y., M.D., F.B., FT and curated by O.B. and F.T. The initial draft of the manuscript was written by M.F.K All authors made substantial contributions to the design and planning of the study, participated in data collection, and were actively involved in the critical revision, editing, and final approval of the manuscript. Each author has assumed full responsibility for the accuracy and integrity of the content.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.