
Abstract
Background:
Arthroscopic rotator cuff repair (RCR) is a common orthopaedic procedure, but it has a high rate of retears that can negatively affect the functional outcomes. Bone marrow stimulation (BMS) has been suggested as an additional treatment to improve the outcomes of RCR.
Purpose:
To compare the effectiveness of the BMS procedure during RCR with conventional RCR.
Study Design:
Systematic review; Level of evidence, 2.
Methods:
A systematic literature search was conducted in MEDLINE/PubMed, Embase, Cochrane Library, and Scopus, on March 1, 2023, for studies comparing postoperative retear rates and functional outcomes between patients who underwent primary arthroscopic RCR with and without the BMS procedure. Only level 1 and 2 randomized controlled trials with a minimum 12-month follow-up were included. The primary outcomes were retear rates and functional outcomes as measured by the Constant; American Shoulder and Elbow Surgeons (ASES); and University of California, Los Angeles (UCLA) scores and by postoperative range of motion. Subgroup analyses were performed based on repair technique (single-row repair vs double-row or suture-bridge repair). The standardized mean difference (SMD) and odds ratio (OR) were utilized to synthesize continuous and dichotomous outcomes, respectively. Homogeneity was evaluated using the chi-square test and I2 statistic.
Results:
The literature search yielded 661 articles, of which 6 studies (522 patients; 261 with BMS, 261 without BMS) met the eligibility criteria. The combined analysis showed no significant decrease in retear rates with the utilization of the BMS procedure during RCR (OR, 0.60; 95% CI, 0.35 to 1.03; P = .07; I2 = 24%). There was no significant intergroup difference in functional outcomes (Constant score: SMD, 0.13; 95% CI, –0.04 to 0.31; P = .13; I2 = 0%; ASES score: SMD, 0.04; 95% CI, –0.20 to 0.28; P = .73; I2 = 0%; UCLA score: SMD, –0.13; 95% CI, –0.50 to 0.23; P = .47; I2 = 0%). Subgroup analyses revealed no significant differences in postoperative retear risk or total Constant score according to the repair technique.
Conclusion:
Based on the available evidence, this systematic review did not find a significant benefit of the BMS procedure at the footprint during arthroscopic RCR compared with conventional RCR in terms of retear rates and functional outcomes at short-term follow-up.
Rotator cuff tears are a prevalent cause of shoulder pain and impaired shoulder function. 45 Arthroscopic rotator cuff repair (RCR) has proven effective in restoring the anatomy of the original rotator cuff tendon insertion, improving shoulder strength and function, and reducing pain in cases where conservative treatments have failed.12,26 Despite advancements in repair techniques and instruments, there remains a significant risk of retear, particularly in large to massive tears, with reported retear rates ranging from 20% to 94%.4,6,11,15,20,40,46 This high incidence of retear is primarily attributed to biological aspects related to the disorganized formation of scar tissue and continuous progression of tendon degeneration. 5
As structurally intact repaired tendons may produce better results, improving tendon-to-bone healing and reducing retear rates after repair are important goals.38,40 Therefore, many efforts have been made to optimize the biologic environment, achieve biological integration of the tendon, and improve the rate and quality of healing of the rotator cuff tendon using platelet-rich plasma or stem cells.14,17,30,44 Bone marrow stimulation (BMS) is one biologic approach to improve healing rates by creating multiple channels between bone marrow and the tendon footprint and recruiting the biologic elements, including bone marrow–derived mesenchymal stem cells (MSCs) and growth factors, to the repair site of the rotator cuff tendon.3,21
With increasing interest in BMS for rotator cuff tears, many clinical studies have been conducted to evaluate the efficacy of BMS in RCR. However, there are inconsistencies regarding the effectiveness of the BMS on structural integrity, retear rates, and clinical outcomes.18,19,22,29,33,42 Two previous systematic reviews have focused on this topic.1,25 However, clinical evidence of BMS in RCR remains unclear, and the reliability of the conclusions is questionable due to the limited numbers of studies included. Furthermore, several high-quality randomized controlled trials (RCTs) have been published in recent years.23,36,37,43 These additional studies can provide a better understanding of the effects of BMS in RCR.
The purpose of this study was to identify, summarize, and synthesize the currently available clinical results on BMS in primary arthroscopic RCR. Our hypothesis was that the application of BMS at the footprint during RCR would significantly improve retear rates or functional outcomes compared with conventional RCR without BMS.
Methods
This study utilized the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 31 The tasks involved in the study, such as study screening and selection, quality assessment, data extraction, and result pooling, were carried out independently by 2 authors (K.-H.S. and S.-B.H.). To maintain consistency and resolve any discrepancies, a third author (J.-U.K.) reviewed the data independently and reached a consensus.
Search Strategy
The following databases were searched on March 1, 2023, to obtain all relevant articles addressing the effect of BMS in patients receiving primary arthroscopic RCR: MEDLINE/Pubmed, Cochrane Library, Embase, and Scopus. The following keywords, Medical Subject Headings (MeSH) terms and their combinations were searched in the [Title/Abstract] field of the search engines: “rotator cuff” OR “supraspinatus” OR “infraspinatus” OR “subscapularis” OR “teres minor” OR “rotator cuff” [MeSH term] OR “rotator cuff injuries” [MeSH term] OR “rotator cuff arthropathy” [MeSH term] AND “microfracture” OR “nanofracture” OR “drilling” OR “channeling” OR “crimson duvet” OR “bone marrow stimulation” OR “arthroplasty, subchondral” [MeSH term]. No other restrictions were applied, including language restrictions. To find the relevant articles that were omitted during the database search, eligible references in the selected articles were examined. During the first stage of screening, duplicated publications were removed, and 2 independent authors (K.H.S. and S.B.H.) screened all the titles and abstracts. The full text of the articles was reviewed in the second stage of the screening process to select articles that met the inclusion and exclusion criteria. The inclusion and exclusion criteria for this review were as follows:
Participants: The review included patients who underwent primary arthroscopic RCR for full-thickness rotator cuff tear.
Interventions: The intervention group (BMS group) received arthroscopic RCR with BMS, including microfracture, drilling, channeling, crimson duvet formation, and so forth.
Comparisons: The control group received arthroscopic RCR alone.
Outcomes: The review focused on 2 main outcomes. The first outcome of interest was the retear rate of the rotator cuff, which was evaluated using magnetic resonance imaging (MRI) or sonography. The second outcome was functional outcomes, which included the Constant score, the American Shoulder and Elbow Surgeons (ASES) score, the University of California, Los Angeles (UCLA) score, and postoperative range of motion (ROM).
Follow-up: Only studies with a minimum clinical follow-up of 12 months were included in the review.
Study design: The review considered RCTs to be eligible study designs for inclusion.
Data Extraction and Outcomes of Interest
The following data were extracted: (1) study characteristics, such as the first author's name, the publication year, and country; (2) patient demographics, including the number of patients, sex, and age; (3) surgical procedures including repair method and BMS protocol; (4) rehabilitation programs; (5) follow-up period; and (6) outcomes of interest.
Quality Assessment
The Cochrane risk of bias tool was utilized to assess the methodological quality of the included RCTs.16,39 Each RCT was evaluated based on the following items: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other biases. The risk of bias for each item was rated as high, low, or unclear. Visual plots depicting risk of bias were generated using robvis. 28
Statistical Analysis
Inter-reviewer reliability was assessed using the kappa statistic (κ) for study screening and selection, quality evaluation, data extraction, and result pooling. The standardized mean difference (SMD) was used to calculate the intergroup difference in mean outcomes divided by the standard deviation of the difference in the outcome for continuous outcomes and is presented with 95% CI. Dichotomous outcomes were analyzed using the odds ratio (OR) with 95% CI. Meta-analyses were conducted to combine the effects and calculate associated 95% CIs. A test of homogeneity based on the chi-square test was performed, and I2 statistics were determined. When I2 was <50%, the fixed-effects model (Mantel-Haenszel method) was used due to low heterogeneity, while I2≥50% was considered significant heterogeneity. A “leave-one-out” sensitivity analysis was conducted by removing 1 study at a time to identify the source of heterogeneity. If heterogeneity was present after excluding each study, the random-effects model (DerSimonian-Laird method) was used. 7 Subgroup analyses were performed for available outcomes based on repair techniques, including single-row repair and double-row or suture bridge repair. Publication bias was examined using the Egger regression symmetry test. 8 All statistical analyses were performed using RStudio Version 1.0.143 (RStudio), with a significance level of P < .05.
Results
Search Results
Figure 1 summarizes the study identification and selection process. Initially, 661 articles were identified through the literature search. After removing 281 duplicates and screening the remaining 380 articles based on their titles and abstracts, 40 full-text articles were assessed for eligibility. Of these, 34 articles were excluded for not meeting the inclusion criteria. Ultimately, 6 articles (522 cases; 261 with BMS, 261 without BMS) were included in the meta-analysis.23,29,33,36,37,43 The reliability values for tasks such as study screening, selection, quality evaluation, data extraction, and result pooling ranged from 0.93 to 1.00, indicating an excellent level of agreement.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram of study inclusion.
Study Characteristics
The baseline characteristics of included studies are described in Table 1. A total of 522 patients were included in this meta-analysis. The mean age of patients ranged from 57.8 to 63.9 years, and the follow-up period ranged from 12 to 29 months. Five studies23,29,33,37,43 enrolled patients with full-thickness rotator cuff tears while 1 study, by Ruiz et al, 36 included patients with supraspinatus tears <3 cm. Two studies29,33 used a single-row repair technique, and 3 studies23,36,37 used a double-row or transosseous equivalent repair technique. One study, by Toro et al, 43 determined the repair technique according to the size of the tear. In the case of tears <1 cm, the single-row technique was used, while the double-row technique was preferred for tears >1 cm. 43 The BMS technique and postoperative rehabilitation program are summarized in Table 2.
Characteristics of the Included Studies a
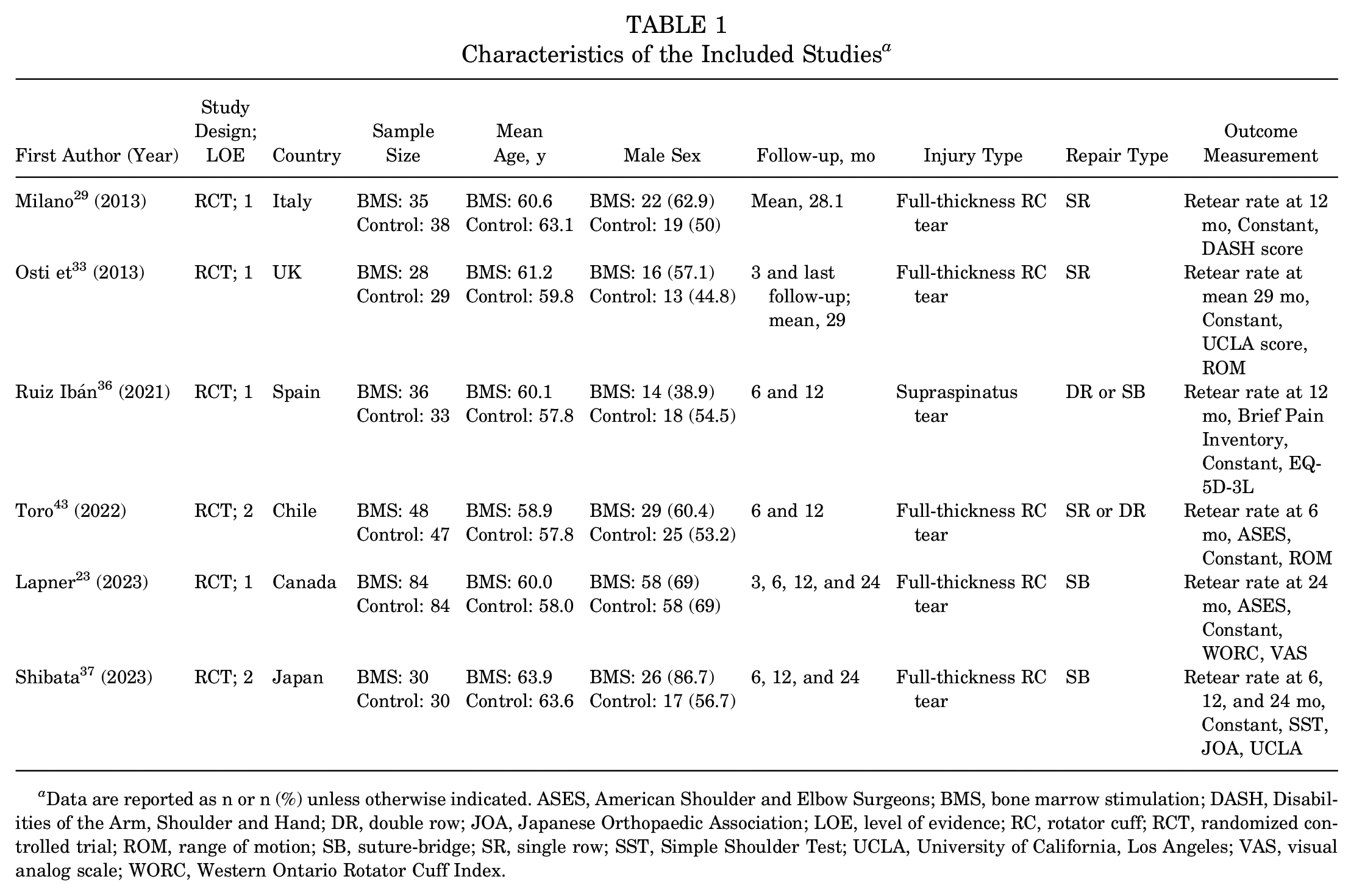
Data are reported as n or n (%) unless otherwise indicated. ASES, American Shoulder and Elbow Surgeons; BMS, bone marrow stimulation; DASH, Disabilities of the Arm, Shoulder and Hand; DR, double row; JOA, Japanese Orthopaedic Association; LOE, level of evidence; RC, rotator cuff; RCT, randomized controlled trial; ROM, range of motion; SB, suture-bridge; SR, single row; SST, Simple Shoulder Test; UCLA, University of California, Los Angeles; VAS, visual analog scale; WORC, Western Ontario Rotator Cuff Index.
Technique of Bone Marrow Stimulation and Postoperative Rehabilitation a

NR, not reported; postop, postoperatively; ROM, range of motion.
Quality Assessment
The results of the assessment for the risk of bias in the included studies are summarized in Figure 2. Of the 6 studies included, 1 study 43 did not clearly report the random sequence generation, and 2 studies33,43 did not clearly report the allocation concealment. Therefore, these 2 studies were rated as having an unclear risk of bias. All RCTs, except 1 study, 37 reported the blinding of outcome assessments and were rated as having a low risk of bias. Three studies29,33,43 were found to have an unclear risk of reporting bias without a prereported protocol.
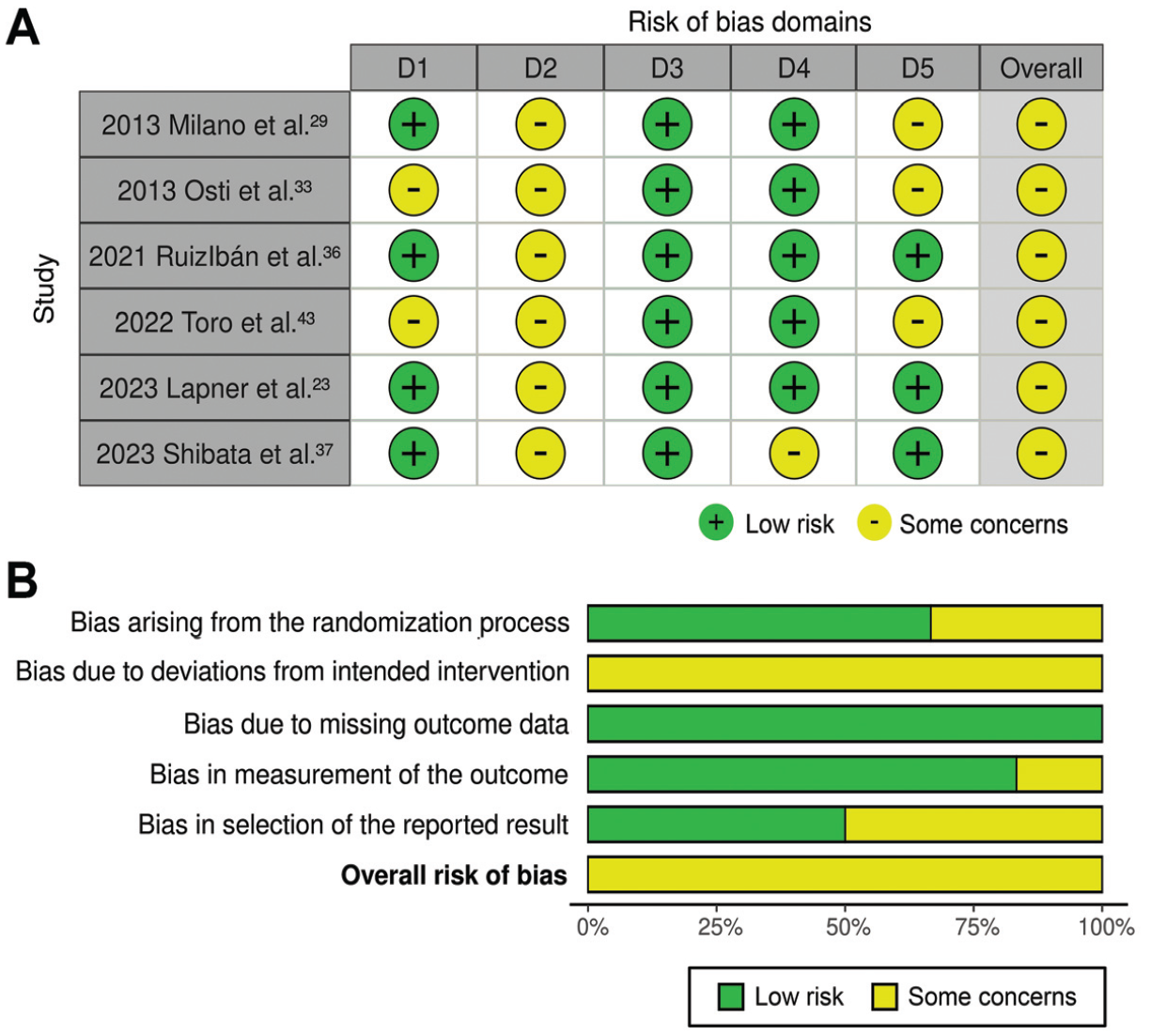
(A) Risk of bias per domain and overall in the included studies. Domains: D1, bias arising from the randomization process; D2, bias due to deviations from the intended intervention; D3, bias due to missing outcome data; D4, bias in measurement of the outcome; D5, bias in selection of the reported result. (B) Summary of the risk of bias per domain and overall.
Retear
The results of meta-analyses on the retear rates are presented in Figure 3 and Supplemental Table S1 (available online). Five studies evaluated the tear integrity using MRI at various postoperative time points, including 6 months,37,43 12 months,29,36,47 and 24 months, 37 as well as the final follow-up. 33 Lapner et al 23 used sonography to assess the retear rate at 24 months postoperatively.
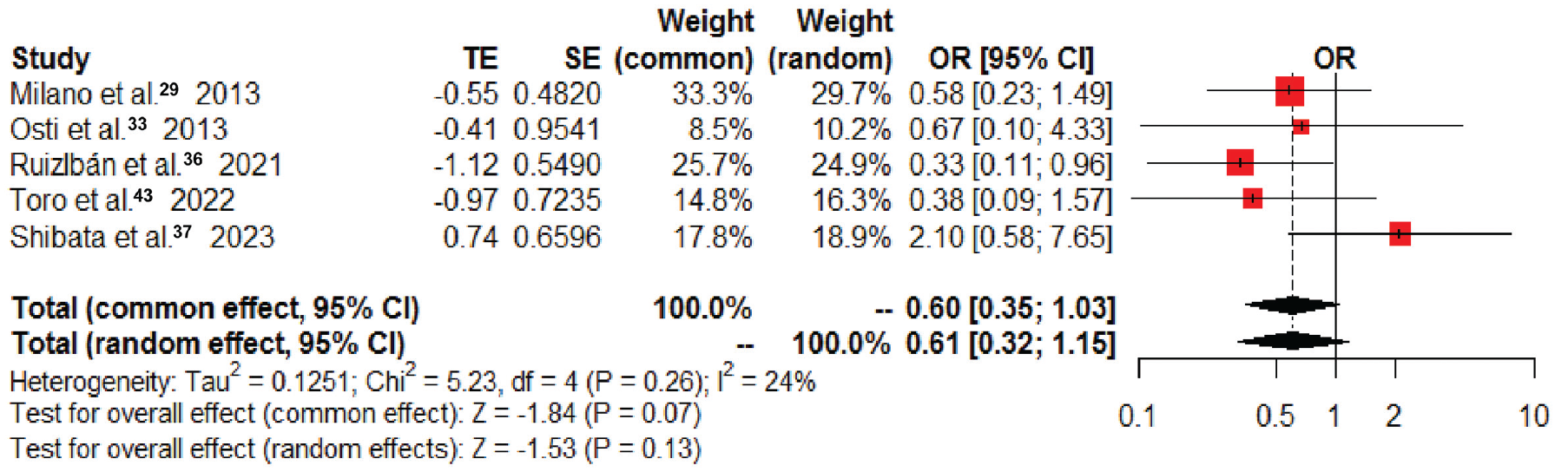
Forest plot of postoperative overall retear rates. OR, odds ratio; TE, treatment effect.
The pooled results demonstrated no significant difference in the postoperative retear rates in favor of BMS (OR, 0.60; 95% CI, 0.35-1.03; P = .07; I2 = 24%) (Figure 3). Sensitivity analyses demonstrated that the study by Lapner et al 23 strongly affected the pooled results of overall retear risk, and thus this study was excluded from the meta-analysis. After its exclusion, heterogeneity was resolved, and the significance of the results did not change (Supplemental Figures S1 and S2). Furthermore, at 6, 12, and >24months postoperatively, no significant differences in retear rates were found between 2 groups (Supplemental Table S1).
Clinical Outcomes
The clinical outcomes are summarized in Supplemental Table S1. All included studies23,29,33,36,37,43 evaluated the total postoperative Constant score, and the pooled results demonstrated that there were no significant intergroup differences overall (SMD, 0.13; 95% CI, –0.04 to 0.31; P = .13; I2 = 0%) (Figure 4A) or at the 3-, 6-, 12-, and >24-month follow-ups (Supplemental Table S1). Two studies23,43 assessed the postoperative ASES score, and the pooled results indicated that BMS during arthroscopic RCR did not improve overall (SMD, 0.04; 95% CI, –0.20 to 0.28; P = .73; I2 = 0%) (Figure 4B) or at 6 and 12 months postoperatively (Supplemental Table S1). Two studies33,37 evaluated the postoperative UCLA score, and the pooled results demonstrated no intergroup difference (SMD, –0.13; 95% CI, –0.50 to 0.23; P = .47; I2 = 0%) (Figure 4C and Supplemental Table S1). Two studies33,43 reported postoperative ROM in forward flexion and external rotation, with pooled results demonstrating no intergroup difference (Supplemental Table S1).
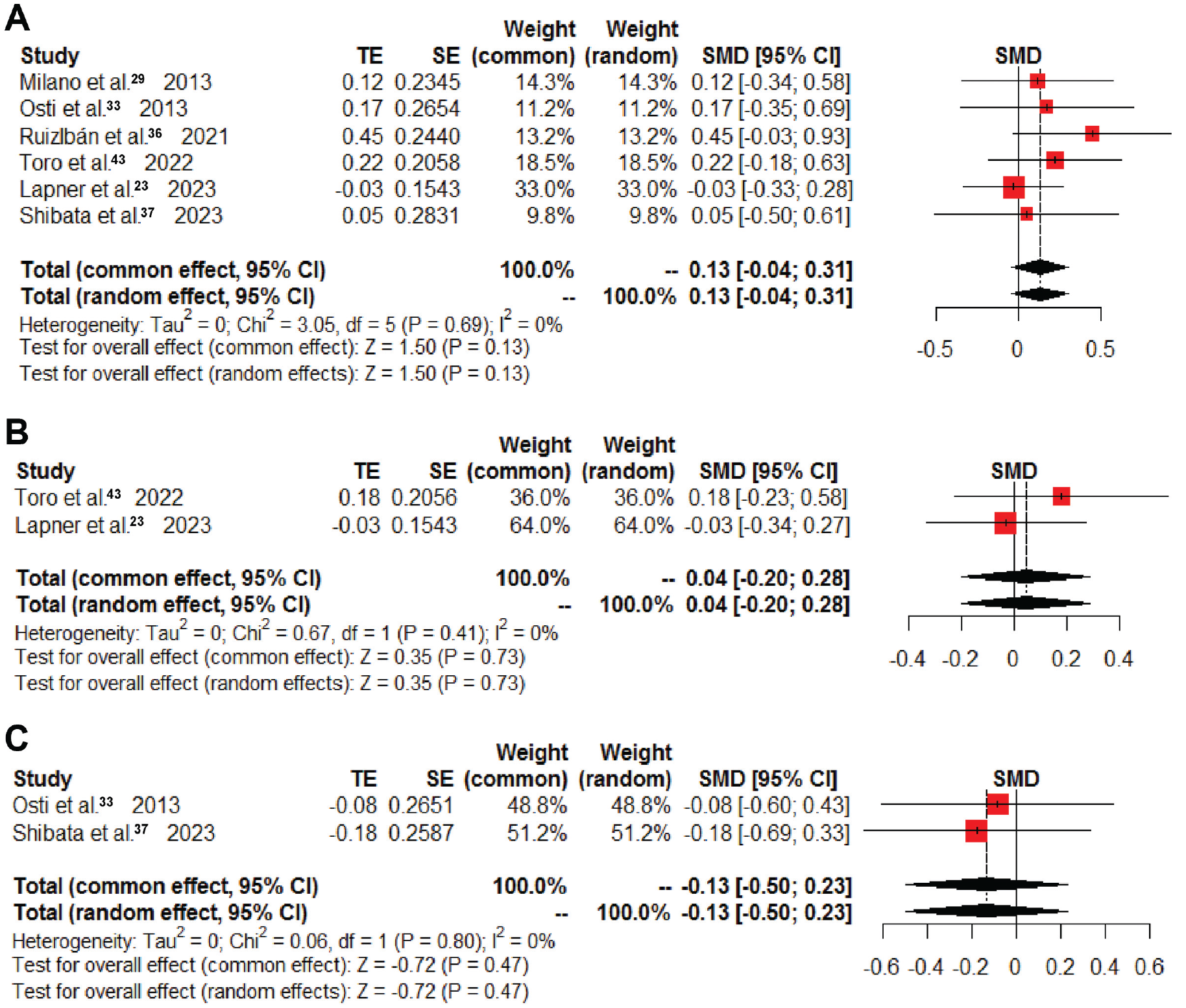
Forest plot of overall postoperative (A) Constant score, (B) American Shoulder and Elbow Surgeons score, and (C) University of California, Los Angeles, score. SMD, standardized mean difference; TE, treatment effect.
Subgroup Analysis
The details of the sensitivity and subgroup analyses are summarized in Supplemental Table S2. The statistical results were stable and supported our conclusion favorably. Subgroup analyses indicated there were no significant differences according to repair technique in terms of retear risk and postoperative Constant score.
Discussion
The most important findings of our study indicate that the utilization of the BMS procedure in arthroscopic RCR does not provide a significant improvement in retear rates (OR, 0.60; 95% CI, 0.35 to 1.03; P = .07; I2 = 24%) or functional outcomes, encompassing total Constant scores (SMD, 0.13; 95% CI, –0.04 to 0.31; P = .13; I2 = 0%), ASES scores (SMD, 0.04; 95% CI, –0.20 to 0.28; P = .73; I2 = 0%), and UCLA scores (SMD, –0.13; 95% CI, –0.50 to 0.23; P = .47; I2 = 0%), when compared with conventional RCR.
The techniques used in arthroscopic RCR have evolved from single-row to double-row to transosseous equivalent suture-bridging techniques to maintain the biomechanics and improve tendon healing rates. However, the failure rates of RCR still remain high, with reported retear rates over 20%.4,11,15,20,40,46 As a result, interest in novel biologic approaches has increased to achieve biologic tendon integration and improve healing.
The BMS procedure is an adjuvant technique proposed for arthroscopic RCR, which introduces biologic factors for tendon healing such as bone marrow–derived MSCs, and growth factors.13,27 Previous basic research has shown that the BMS procedure has positive effects on bone–tendon junction healing and improves ultimate force to failure.3,21 Additionally, various retrospective cohort studies have reported that applying the BMS procedure to the footprint during arthroscopic RCR has significant beneficial effects, including decreased retear rates and marginally improved functional outcomes.18,19,34,42,47
Two previous systematic reviews have examined this topic and reported the potential of the BMS procedure to enhance tendon-to-bone healing and reduce retear rates.1,25 However, these reviews have certain limitations that affect the reliability of their conclusions. One systematic review 25 included overlapping cohorts with different follow-up periods and incorporated a study that involved patch augmentation, compromising the reliability of the findings.18,19,47 Additionally, another systematic review 1 included only 4 studies, combining RCTs and retrospective cohort studies, with a small sample size. Moreover, both of the retrospective studies included in the review were found to have a risk of time-varying confounding and did not mention the use of an unbiased outcome assessor.1,19,42
As the interest in the BMS procedure continues to grow, several recent high-quality RCTs have been published.23,36,37,43 However, these studies have yielded inconsistent results regarding the effectiveness of the BMS procedure in terms of structural integrity, retear rates, and clinical outcomes. Therefore, the objective of this review is to provide a comprehensive summary and synthesis of the current evidence on the effectiveness of the BMS procedure during arthroscopic RCR. Specifically, this review aims to address 2 key questions: (1) “Does it improve the retear rates or tendon integrity?” and (2) “Does it improve functional outcomes?”
However, the findings of this study do not support our initial hypothesis that the BMS procedure during arthroscopic RCR leads to a lower retear rate and better functional outcomes when compared with conventional arthroscopic RCR. The study conducted by Lapner et al 23 stands out as the largest multicenter RCT on this subject. However, it was excluded from the meta-analyses of retear risk through sensitivity analyses. Despite not reaching statistical significance, Lapner et al reported that the BMS group exhibited a lower healing rate and no difference in clinical outcomes. Importantly, the exclusion of this study did not significantly affect the overall meta-analysis results. The lack of a significant beneficial effect observed with the intraoperative BMS procedure may be attributed to several factors. First, the BMS procedure might compromise the bony integrity and surface area at the rotator cuff footprint, which is crucial for structural healing of the repaired tendon and functional outcomes.38,40 When creating large-diameter and multiple bone channels during the BMS procedure, there is a risk of damaging fibrocartilage, subchondral bone, and the critical contact areas between the tendon and bone that are important for optimal tendon healing.2,9,24,32,41 This may limit the demonstrated benefits of BMS in promoting rotator cuff tendon healing, despite the recruitment of MSCs and growth factors. Second, conventional procedures such as footprint decortication and acromioplasty may influence the results. Acromioplasty can release stem cells and growth factors from the cancellous bone of the acromion, while footprint decortication can introduce MSCs at the tendon insertion site, similar to the BMS procedure.10,32,35 These confounding factors might influence the beneficial effects of BMS procedure during arthroscopic RCR in terms of optimizing the biologic environment of the rotator cuff tendon with regard to the recruitment of growth factors and MSCs.
Nevertheless, some studies have reported positive findings. Milano et al 29 observed a higher healing rate in the BMS group when specifically analyzing large tears as a subgroup. Shibata et al 37 found that retears in the BMS group exclusively occurred at the musculotendinous junction, with no retears at the tendon insertion site where MSCs are exposed through BMS. Similarly, Ruiz Ibán et al 36 reported comparable retear rates at the musculotendinous junction, but significantly higher tendon-to-bone healing rates, resulting in an overall reduction in retear rates by <50%. Furthermore, Osti et al 33 reported less pain, improved UCLA and Constant scores, and enhanced ROM in the BMS group at the 3-month postoperative mark, attributed to the rapid healing process at the tendon-bone interface. Although the pooled results of this review did not reach statistical significance, there was a trend suggesting a decreased retear risk in the BMS group. It is worth noting that the small sample size of participants included in this review may have limited the statistical power of the analysis, which warrants caution when interpreting the results of this study.
Limitations
There are several limitations to this review. First, the number of participants enrolled was relatively low, and RCTs of levels of evidence 1 and 2 were included. Second, the studies were highly heterogeneous in terms of tear size, repair techniques of the rotator cuff, techniques of footprint preparation and BMS, rehabilitation protocol, and assessment methods of outcomes. In particular, for accurately assessing subtle improvements in tendon integrity, detailed grade results based on the Sugaya classification are important. However, in this review, only the retear risk corresponding to Sugaya grades 4 and 5 was examined in all included studies. 40 Although subgroup analyses based on the repair technique of the rotator cuff demonstrated the robustness of the results, the findings should be interpreted with caution. Third, the included studies did not clearly document and analyze the potential risk factors or confounders that may have an impact on postoperative outcomes, such as adjuvant acromioplasty, footprint decortication, smoking, body mass index, and diabetes. Fourth, due to the lack of long-term data, the analyses were confined to short-term outcomes, and a definite conclusion cannot be drawn. Future studies with larger sample sizes, long-term follow-up, and adequate control of potential confounding factors are required to establish a definite conclusion about the necessity of the BMS procedure in arthroscopic RCR.
Conclusion
Based on the available evidence from this systematic review, it cannot be concluded that BMS procedures at the footprint during arthroscopic RCR provide significant benefits in terms of retear rates and functional outcomes compared with conventional RCR during the short-term follow-up. These findings suggest that the routine use of the BMS procedure in arthroscopic RCR may not be necessary and that its application should be considered on a case-specific basis.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671231224482 – Supplemental material for Effect of Bone Marrow Stimulation on Arthroscopic Rotator Cuff Repair: A Systematic Review and Meta-analysis
Supplemental material, sj-pdf-1-ojs-10.1177_23259671231224482 for Effect of Bone Marrow Stimulation on Arthroscopic Rotator Cuff Repair: A Systematic Review and Meta-analysis by Kyun-Ho Shin, Jin-Uk Kim, Il-Tae Jang and Seung-Beom Han in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted June 29, 2023; accepted August 16, 2023.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.