
Abstract
Background:
Although bone marrow stimulation (BMS) is believed to promote rotator cuff healing, there is no comparison of clinical outcomes and structural integrity between different BMS techniques in patients undergoing arthroscopic rotator cuff repair (ARCR).
Purpose/Hypothesis:
The purpose of this study was to compare the clinical outcomes and structural integrity between BMS inside the rotator cuff footprint area (“greenhouse” technique) and BMS outside the rotator cuff footprint area (“crimson duvet” technique). It was hypothesized that the new “greenhouse” technique would provide better clinical outcomes and structural integrity at short-term follow-up.
Study Design:
Randomized controlled trial; Level of evidence, 1.
Methods:
This study included 60 patients who underwent ARCR using the “greenhouse” technique or “crimson duvet” technique (n = 30 per group). Functional outcomes at 24 months postoperatively were assessed including the ASES (American Shoulder and Elbow Surgeons) score, CMS (Constant-Murley score), UCLA (University of California, Los Angeles) score, SST (Simple Shoulder Test), VAS (visual analog scale) for pain, and range of motion consisting of forward elevation, external rotation, and internal rotation. The minimal clinically important difference, patient acceptable symptom state, substantial clinical benefit, and maximum outcome improvement were also compared between the 2 groups. Structural integrity was evaluated by magnetic resonance imaging at 2 years postoperatively and compared between the 2 groups.
Results:
All functional outcomes improved significantly compared with preoperatively in both groups at the last follow-up (all P < .001). However, there were no significant differences between the 2 groups postoperatively. Overall, 52 patients (86.7%) achieved the minimal clinically important difference, 44 patients (73.3%) achieved the patient acceptable symptom state, 45 patients (75.0%) achieved the substantial clinical benefit, and 31 patients (51.7%) achieved the maximum outcome improvement, without significant differences between the 2 groups. The retear rate after ARCR in the “greenhouse” group was 6.7% and 10.0% in the “crimson duvet” group, which was not significantly different.
Conclusion:
In ARCR, both the “greenhouse” and “crimson duvet” techniques exhibited significant functional improvement in patients with rotator cuff tears. The new “greenhouse” technique provided comparable clinical outcomes and structural integrity compared with the traditional “crimson duvet” technique at short-term follow-up.
Registration:
NCT04686968 (ClinicalTrials.gov)
A rotator cuff tear (RCT) is one of the most common shoulder diseases. Many patients with RCTs are symptomatic and experience pain, limitations in range of motion (ROM), and deficiency in activities of daily living. Nowadays, arthroscopic rotator cuff repair (ARCR) is considered a first-line treatment option when patients suffer from an acute full-thickness RCT. 34 Although the clinical outcomes of ARCR are satisfactory in most instances,3,27 there are still reports of retear rates ranging from 9% to 12% because of poor tendon healing after surgery.10,11,14,20,29,37,42 Improving the healing rate of ARCR has become the key goal of treatment.
Bone marrow stimulation (BMS) was first introduced by Snyder and Burns 36 in 2009. The authors employed several bone vents on the lateral side of the footprint area after single-row ARCR, that is, bone marrow extravasation, called the “crimson duvet,” which contained stem cells and a variety of growth factors derived from bone marrow around the footprint. It was believed that this would enhance tendon healing after an RCT. 36 A subsequent study revealed a high level of patient satisfaction, with 91% reporting positive results and 92% of the rotator cuff structure intact. 8 However, there is still controversy about the effect of BMS. The “crimson duvet” technique is performed lateral to the repaired tendon, as it was proposed that the uncovered bony bed might not maintain the efficiency of growth factors for a long time. 43 Therefore, it is critical to concentrate the tendon healing–promoting factors created by BMS inside the footprint area. In 2022, a new “greenhouse” technique was proposed to combine the modified Mason-Allen method without knotting and BMS for ARCR. Compared with the “crimson duvet” technique, the “greenhouse” technique is performed across the full area of the footprint before rotator cuff repair. After the threads are tensioned and fixed by an anchor, the rotator cuff tendon fully covers the bony bed, which prevents the extravasation of relevant substances far from the tendon healing location. 23 Theoretically, the new BMS technique provides a better biological environment than the traditional “crimson duvet” technique. However, there is neither a report on its clinical outcomes nor any comparison between this new technique and the traditional “crimson duvet” technique.
Therefore, this study aimed to compare the clinical outcomes and structural integrity of the “greenhouse” technique and traditional “crimson duvet” technique in patients with full-thickness RCTs at short-term follow-up. It was hypothesized that the new “greenhouse” technique would provide better clinical outcomes and structural integrity compared with the traditional “crimson duvet” technique at short-term follow-up.
Methods
Study Design
This was a prospective randomized controlled study. Institutional review board approval was obtained (No. K202066000). The protocol was registered at ClinicalTrials.gov (NCT04686968). All participants were enrolled in this study between July 2021 and March 2022, and follow-up visits were completed by April 2024. This trial was conducted under CONSORT (Consolidated Standards of Reporting Trials) guidance. All patients were recruited from one hospital, and all patients provided informed consent. The current trial was a double-blinded study, with both participants and evaluators unaware of the group assignments.
Inclusion Criteria
Inclusion criteria were as follows: (1) patients aged 18-65 years; (2) failure of nonoperative treatment for at least 3 months; (3) physical examination, magnetic resonance imaging (MRI), and arthroscopic findings confirming a reparable full-thickness RCT that involved only the supraspinatus tendon or the supraspinatus and infraspinatus tendons; (4) ARCR as the initial surgical procedure; (5) ability to attend rehabilitation sessions and follow-up visits; and (6) ability to undergo MRI at 2 years postoperatively.
Exclusion Criteria
Exclusion criteria were as follows: (1) patients aged <18 years or >65 years; (2) partial, massive, or irreparable RCTs; (3) isolated subscapularis tendon tears; (4) stage ≥3 fatty infiltration according to the Goutallier classification, stage 3 tendon retraction according to the Patte classification, or shoulder osteoarthritis; (5) significant shoulder comorbidities (eg, rotator cuff arthropathy, Bankart lesion, SLAP [superior labral anterior to posterior] lesion, etc); (6) previous surgery on the affected shoulder; (7) significant medical comorbidities such as diabetes, immune diseases, or infections; and (8) unwillingness to participate in the study.
Sample Size Analysis
The study group was the “greenhouse” group, while the control group was the “crimson duvet” group. The primary parameter was the American Shoulder and Elbow Surgeons (ASES) score. According to the results of a pre-experiment, the difference between the 2 groups was 9, the standard deviation was 9.8, and the 2-sided alpha was 0.05. The power (1 –β) was 0.9, and the sample size ratio of the study group to the control group was 1:1. The sample size was calculated to be 26 cases in each group at least.
Randomization
A computer-generated simple randomization process was used to assign the participants to either the “greenhouse” or “crimson duvet” group. The surgeon was informed of the group assignment in the operating room by a circulating nurse, who was not involved in the study. Participants and evaluators were unaware of the randomization.
Surgical Procedure
One group of surgeons performed all the procedures. The patient was placed in the beach-chair position. Acromioplasty and tenotomy or tenodesis of the long head of the biceps tendon were performed as necessary. The full-thickness RCT was confirmed after bursectomy. After footprint preparation, a different procedure was performed using the “greenhouse” or “crimson duvet” technique.
“Greenhouse” Technique (Study Group)
A polyester suture thread was passed through the rotator cuff tendon in a modified Mason-Allen fashion without knotting after tendon debridement. If the anterior-to-posterior diameter of the tendon tear was >2 cm, then an additional suture thread was used in the same way. Next, the threads were retrieved and loaded into the anchor (Co.Rejoin). BMS was then performed with a 2 mm–diameter awl, creating 6 to 8 holes on the bony bed. After bone marrow extravasated from the holes, the anchor-loaded threads were inserted at the distal part of the greater tuberosity by tightening the threads 23 (Figure 1).

“Greenhouse” technique for a rotator cuff tear in a right shoulder. (A) Tendon debridement before bone marrow stimulation (BMS). (B) BMS on the footprint area using a 2 mm–diameter awl. (C) The tendon was pulled back to the original site, and the holes from BMS were fully covered.
“Crimson Duvet” Technique (Control Group)
The torn tendon was repaired by 1 to 2 double-loaded polyether ether ketone anchors (Co.Rejoin) depending on the tear size in a single-row procedure. The anchor was placed 5 to 7 mm lateral to articular cartilage to minimize tension and leave part of the footprint uncovered. After tendon repair, BMS was performed with a 2 mm–diameter awl, creating 6 to 8 holes lateral to the repaired tendon edge until bone marrow extravasated from the holes 36 (Figure 2).

“Crimson duvet” technique for a rotator cuff tear in a right shoulder. (A) Tendon debridement before suturing. (B) After anchor insertion, the sutures were tied in a modified Mason-Allen fashion. (C) Bone marrow stimulation was performed with a 2 mm–diameter awl on the lateral side of the footprint area.
Rehabilitation
Both groups received the same rehabilitation protocol. The patient was protected by wearing a sling for 6 weeks. Pendulum exercises were allowed after surgery, followed by passive range of shoulder motion and active-assisted motion at 6 weeks postoperatively under strict supervision. Also, patients were instructed to avoid excessive abduction (>90°) for 6 weeks postoperatively. Weightbearing, strengthening exercises, and activities of daily living were encouraged at 3 months after surgery.
Outcome Measures
All participants’ shoulder function was evaluated preoperatively and at 24 months postoperatively. The primary parameter of this study was the ASES score.25,31 The minimal clinically important difference (MCID) for the ASES score was considered to be 15.2 points. 24 The substantial clinical benefit (SCB) was considered to be 17.5 points, 7 the patient acceptable symptom state (PASS) was considered to be 86.7 points, 12 and the maximum outcome improvement (MOI) was considered to be 69.5%. 4 The secondary parameters included the normalized Constant-Murley score (CMS),5,6 the Simple Shoulder Test (SST), 22 and the University of California, Los Angeles (UCLA) score.2,9 The visual analog scale (VAS) was used to assess the level of pain. ROM including forward elevation (FE), external rotation (ER) at 90° of abduction, and internal rotation (IR) was also measured at 24 months postoperatively. A goniometer was used to measure FE and ER, and IR was evaluated by referring to the vertebral level reached by the thumb. To simplify statistical analysis, the vertebral levels were translated into numbers from 19 for the thigh to 1 for T1. 15
At the last follow-up, patients were surveyed about their willingness to undergo surgery if the same situation occurred in the contralateral shoulder (yes or no). All findings and measurements of this study were recorded by an independent shoulder surgeon, who was unaware of the randomization.
All participants underwent MRI at 24 months after surgery to evaluate the repaired rotator cuff structure. The Sugaya classification was used to assess structural integrity 37 ; types IV and V were identified as retears. An independent senior radiologist, who was unaware of this study, performed the MRI evaluation.
Statistical Analysis
Statistical analyses were performed with SPSS software (Version 24.0; IBM). Categorical variables were described as frequencies with percentages, and continuous variables were described as means and standard deviations. The Shapiro-Wilk test was used to assess the distribution of continuous variables. The Student t test was performed to compare continuous data between the study and control groups, and the chi-square test was used to analyze categorical variables. The MCID, SCB, PASS, and MOI for the ASES score after ARCR in previously published studies were used.4,7,12,13,18,24,38 The level of statistical significance was set at P < .05.
Results
Patient Characteristics
From July 2021 to March 2022, there were 85 patients with RCTs assessed for eligibility, 64 patients met the selection criteria, and 4 were lost to follow-up (2 in each group). Thus, a total of 60 patients (93.8%) were finally enrolled in this study, with 30 patients in each group (Figure 3).

Flowchart of this study according to CONSORT (Consolidated Standards of Reporting Trials) guidelines.
There were 25 male (41.7%) and 35 female (58.3%) patients. The mean age was 50.8 years (range, 31-64 years). Overall, 41 RCTs (68.3%) had dominant-side involvement. The mean body mass index was 24.4 kg/m2 (range, 18.1-29.7 kg/m2). The mean time from injury to surgery was 10.0 months (range, 3-84 months). Among the 60 patients included in the study, 29, 19, and 12 patients had small, medium, and large tear sizes, respectively. There were 21 patients with Goutallier stage 0 fatty infiltration of the supraspinatus, 28 with stage 1, and 11 with stage 2. Among all participants, 26 patients (43.3%) underwent acromioplasty. Additionally, 22 patients (36.7%) underwent tenotomy/tenodesis of the long head of the biceps tendon. No significant differences were found in patient characteristics at baseline between the 2 groups (Table 1). There were also no significant differences in clinical outcomes, pain, or ROM at baseline (Table 2).
Patient Characteristics a
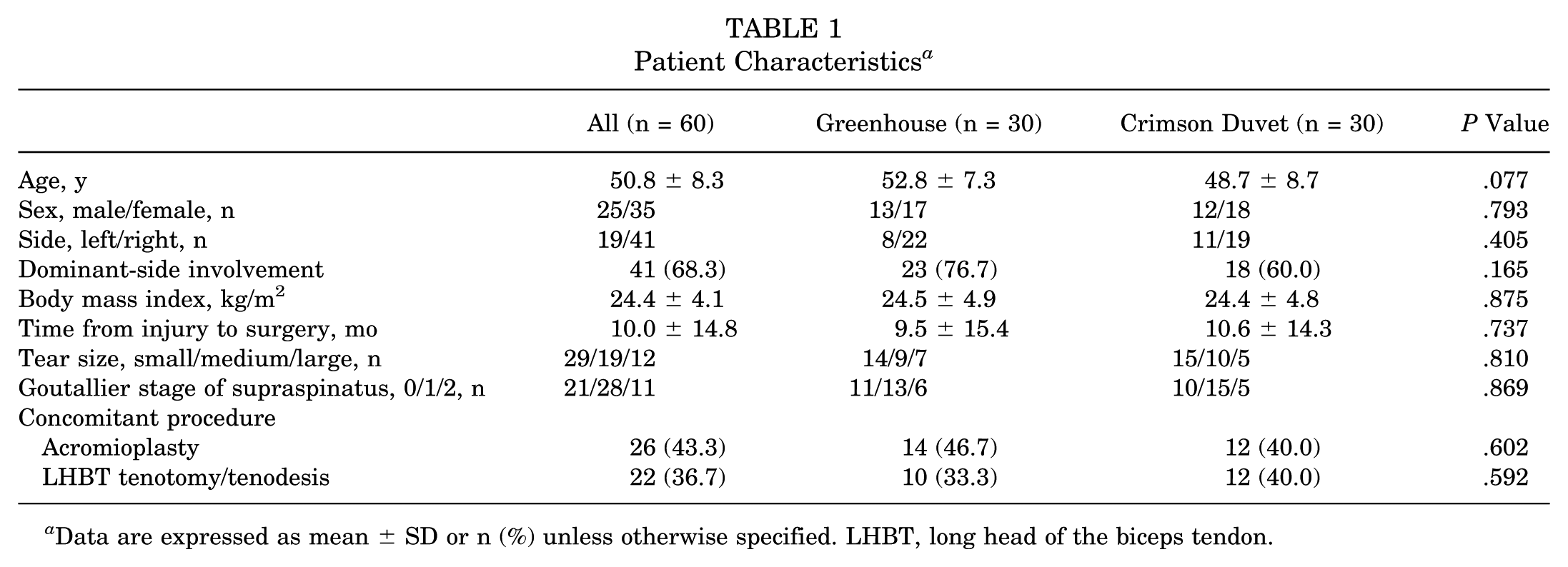
Data are expressed as mean ± SD or n (%) unless otherwise specified. LHBT, long head of the biceps tendon.
Clinical Outcomes a

Data are expressed as mean ± SD (95% CI). ASES, American Shoulder and Elbow Surgeons; CMS, Constant-Murley score; ER, external rotation; FE, forward elevation; IR, internal rotation; ROM, range of motion; SST, Simple Shoulder Test; UCLA, University of California, Los Angeles; VAS, visual analog scale.
Statistically significant (P < .05).
Clinical Outcomes
Overall, all parameters showed significant improvements at the last follow-up compared with preoperatively. The ASES score improved from 48.1 ± 10.1 to 89.1 ± 14.0 in the study group (P < .001) and from 53.5 ± 20.7 to 85.2 ± 10.8 in the control group (P < .001). The CMS value improved from 53.4 ± 21.8 to 90.0 ± 12.2 in the study group (P < .001) and from 57.8 ± 24.1 to 86.1 ± 13.9 in the control group (P < .001). The UCLA score improved from 15.9 ± 5.4 to 31.6 ± 4.8 in the study group (P < .001) and from 17.7 ± 5.2 to 30.9 ± 5.4 in the control group (P < .001). The SST score improved significantly from 4.7 ± 2.9 to 10.2 ± 2.1 in the study group (P < .001) and from 5.4 ± 2.7 to 9.8 ± 1.8 in the control group (P < .001). However, there were no significant differences in any scores between the study and control groups postoperatively (P = .567 for ASES, P = .297 for CMS, P = .605 for UCLA, and P = .490 for SST). When comparing the net improvement of functional outcomes, there were also no significant differences in any scores between the 2 groups (P = .273 for ASES, P = .531 for CMS, P = .276 for UCLA, and P = .341 for SST) (Table 3).
Net Improvement in Clinical Outcomes a
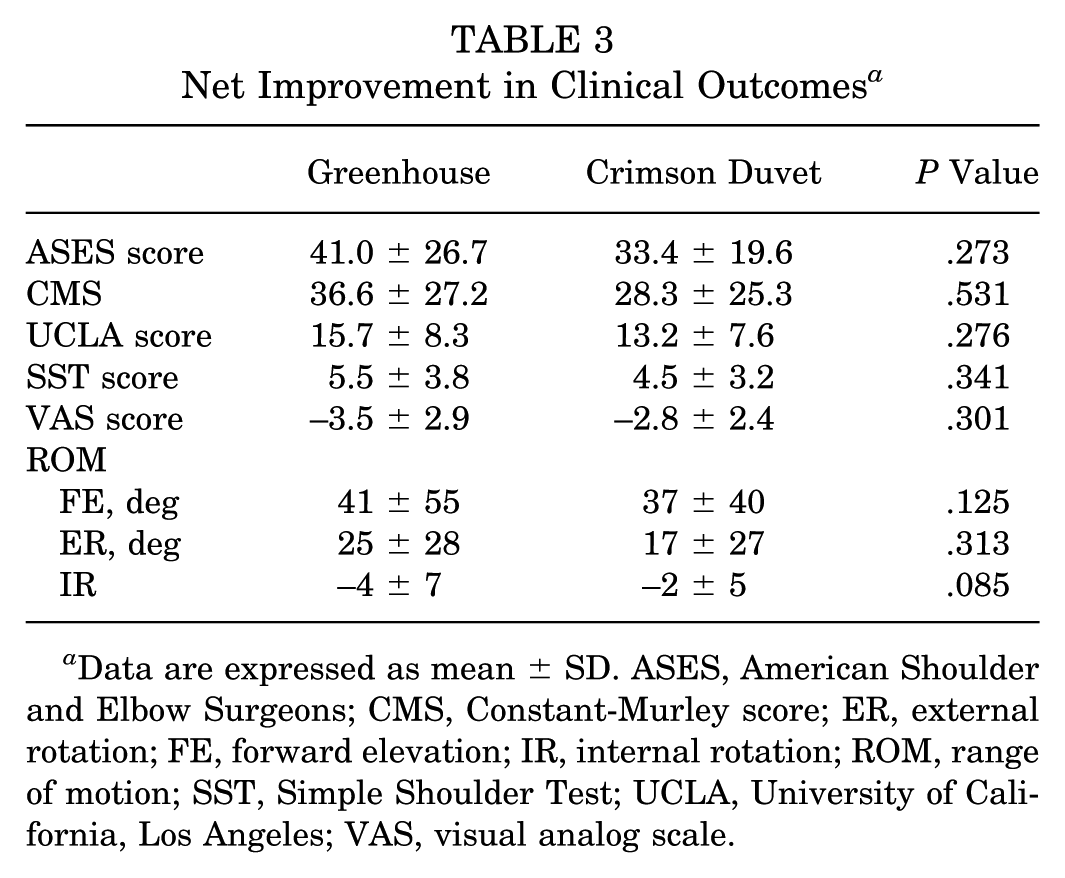
Data are expressed as mean ± SD. ASES, American Shoulder and Elbow Surgeons; CMS, Constant-Murley score; ER, external rotation; FE, forward elevation; IR, internal rotation; ROM, range of motion; SST, Simple Shoulder Test; UCLA, University of California, Los Angeles; VAS, visual analog scale.
Additionally, 52 patients (86.7%) exceeded the MCID, with 27 patients (90.0%) in the study group and 25 patients (83.3%) in the control group. A total of 44 patients (73.3%) achieved the PASS, with 23 patients (76.7%) in the study group and 21 patients (70.0%) in the control group. A total of 45 patients (75.0%) achieved the SCB, with 23 patients (76.7%) in the study group and 22 patients (73.3%) in the control group. There were 31 patients (51.7%) who achieved the MOI, with 17 patients (56.7%) in the study group and 14 patients (46.7%) in the control group. Although all achievement rates in the study group were higher than those in the control group, these differences were not statistically significant (Table 4).
Achievement of MCID, PASS, SCB, and MOI a

Data are expressed as n (%). MCID, minimal clinically important difference; MOI, maximum outcome improvement; PASS, patient acceptable symptom state; SCB, substantial clinical benefit.
Pain
The mean VAS score improved from 4.6 ± 2.1 preoperatively to 1.1 ± 1.9 at the last follow-up in the study group (P < .001) and from 4.2 ± 2.2 to 1.4 ± 1.9 in the control group (P < .001). However, no significant difference was found between the 2 groups postoperatively (P = .646). Also, there was no significant difference in the net improvement of the VAS score between the 2 groups (P = .301) (Tables 2 and 3).
Range of Motion
ROM improved significantly from baseline to the last follow-up in both groups. FE improved from 122°± 51° to 163°± 17° in the study group and from 126°± 40° to 163°± 10° in the control group (both P < .001). ER at 90° of abduction improved from 28°± 24° to 54°± 12° in the study group (P = .001) and from 40°± 24° to 55°± 12° in the control group (P = .001). IR improved from 15 ± 4 preoperatively to 10 ± 4 postoperatively in the study group and from 13 ± 5 preoperatively to 10 ± 4 postoperatively in the control group (both P < .001). No significant differences were found in ROM between the 2 groups at the last follow-up (P = .855 for FE, P = .233 for ER, and P = .913 for IR). Also, no significant difference was found in the net improvement of ROM between the 2 groups (P = .125 for FE, P = .313 for ER, and P = .085 for IR) (Tables 2 and 3).
Tendon Integrity
MRI was performed in all participants at the last follow-up. The retear rate was 8.3% overall, consisting of 2 patients in the study group (6.7%) and 3 in the control group (10.0%), without statistical significance (P = .640). No significant difference was found in the Sugaya classification distribution between the 2 groups (P = .961) (Table 5).
Tendon Integrity a

Data are expressed as n (%).
Complications
A total of 8 patients (13.3%) had complications during the study period. There were 2 patients who had persistent pain and 1 patient who had shoulder stiffness (FE <90°) in the study group (10.0%), with 3 and 2 patients, respectively, in the control group (16.7%). However, none of patients accepted further surgical interventions. No other complications were found. All patients were asked about their willingness to undergo surgery if the contralateral shoulder had the same condition; 52 patients (86.7%) answered “yes.” Because of the limited number of cases, we did not perform further risk factor analysis.
Discussion
The main finding of this study is that the “greenhouse” technique achieved functional improvement after ARCR in patients with RCTs, with a low retear rate. Compared with the traditional BMS technique, this new BMS technique provided comparable clinical outcomes and structural integrity at short-term follow-up.
Although ARCR has shown excellent functional results for treating patients with RCTs, retears of the tendon still cannot be avoided, leading to the progressive deterioration of shoulder function.19,30,39 Snyder and Burns, 36 in 2009, proposed a biological method of treating patients with RCTs. By drilling holes on the surface of the footprint after single-row repair of the rotator cuff, growth factors, fibroblasts, and mesenchymal stem cells are released and flow from the bone marrow cavity to the repaired tendon site and form red blood clots. Snyder and Burns 36 named it the “crimson duvet,” which was believed to promote tendon healing in patients with RCTs. In 2021, the same research group reported a low retear rate of 8%, with 91% satisfactory results in 91 cases of ARCR with BMS at >2 years’ follow-up. 8 As of now, most surgeons agree that BMS can reduce the retear rate after ARCR.8,21,32,33,43 Milano et al 26 found a healing rate of 65.7% in patients who underwent ARCR combined with BMS compared with 52.6% after ARCR alone, as determined by MRI. Kida et al 16 observed that BMS could improve the strength of fixation by adhering the tendon-bone interface. Jo et al 15 also reaffirmed the role of BMS in patients with RCTs by reporting a significantly lower retear rate in the BMS group after ARCR compared with those without BMS (22.2% vs 45.2%, respectively; P < .023). Recently, a meta-analysis including 9 studies with a total of 827 patients showed a significant difference in the retear rate between ARCR combined with BMS and ARCR alone (17.5% vs 28.9%, respectively; P < .0001). Further, the CMS value was significantly higher in the ARCR combined with BMS group (P = .02), but there were no differences in ASES, UCLA, and VAS scores between the 2 groups, while the differences in all scores did not achieve the MCID. 41 In the present study, 86.7% of patients reported being satisfied with their clinical results. In the “greenhouse” group, 90.0% achieved the MCID, 76.7% achieved the PASS, 76.7% achieved the SCB, and 56.7% achieved the MOI, with a retear rate of 6.7% and a complication rate of 10.0%. Therefore, it was proven that the new BMS technique is an effective way to provide satisfactory clinical outcomes and tendon integrity at short-term follow-up after ARCR. However, the retear rate in our series, whether using the “greenhouse” or “crimson duvet” technique, was lower than in previous studies. The main possible reason may be that all patients that we enrolled had reparable superoposterior RCTs with good tendon quality and that those with massive and irreparable RCTs with poor tendon quality and severe tendon retraction were all excluded.
Although BMS was proven as an effective approach in the present study, the technique to perform BMS is still debated.1,17,28,35 Kim et al 17 reported that BMS could not promote tendon healing if the footprint coverage was <50% for large to massive RCTs. Yoon et al 43 indicated that an uncovered footprint might not sustain bone marrow droplets, which would instantly disappear. Theoretically, bone marrow–derived mesenchymal stem cells and growth factors may not have an effect in tendon repair if they do not reach the footprint area or vanish quickly during surgery. Because of this disadvantage, the new “greenhouse” technique was invented to perform BMS right in the footprint area and pull the repaired tendon to fully cover the BMS site using the knotless modified Mason-Allen method, which prevents the extravasation of relevant substances from bone marrow far from the tendon healing location. 23 However, one interesting finding in the present study is that all parameters, including clinical scores, ROM, pain, and the retear rate, with the “greenhouse” technique only showed comparable results compared with the traditional “crimson duvet” technique, regardless of its theoretical advantages, which suggests that a different BMS technique may play a similar role in ARCR at short-term follow-up.
We considered the possible explanations as follows: (1) The 2 different BMS techniques, although both release growth factors from bone marrow, would affect the rotator cuff on different sides initially. With the “greenhouse” technique, the torn rotator cuff was repaired and fully covered the footprint, which led the released growth factors to mostly accumulate underneath the repaired tendon. Thus, it would first promote tendon healing on the articular side. On the contrary, with the “crimson duvet” technique, the torn rotator cuff was repaired medially with a single row first, and then BMS was performed to release growth factors lateral to the tendon, which would initially affect tendon healing on the bursal side. The side on which the healing process occurred initially in the rotator cuff demonstrated no difference in the present study. (2) The “greenhouse” technique was performed with the knotless modified Mason-Allen method. Without an anchor in the middle of the footprint, the released growth factors would flow to the glenohumeral joint later. It would thus weaken the long-term effect of BMS as a “greenhouse.” Unfortunately, we still do not know the exact timing of BMS's effect. Li and Zhang 21 reported in a systematic review that BMS can promote rotator cuff healing and decrease the retear rate at a very early time after tendon repair but might lose its effect at 1 year postoperatively. Osti et al 28 also reported a significant improvement in clinical results at 3-month follow-up in the ARCR with BMS group compared with the ARCR alone group; yet, these differences were not significant at a minimum of 2 years’ follow-up. Those previous works, combined with the present study, suggest that further investigation is still needed on how to maintain BMS's effect. (3) Although the “greenhouse” technique showed better clinical outcomes and a lower retear rate than the “crimson duvet” technique, these findings might significantly differ at midterm or long-term follow-up.
Limitations
There are some limitations in the present study. First, this study did not enroll a group that only underwent ARCR without BMS as a sham group. However, previous studies have already proven the efficacy of BMS in ARCR; the “crimson duvet” technique was invented in 2009 and has been proven to be an effective approach for promoting healing by previous studies. 36 Our recent study also found that the “greenhouse” technique could significantly reduce the retear rate after ARCR. 40 To compare the different BMS techniques, we set the “crimson duvet” technique as the control group. Second, we excluded massive RCTs and irreparable RCTs with poor tendon quality (Goutallier stage 3-5) in the present study. Because of higher retear rates and unexpected clinical outcomes, we believe that shoulder arthroplasty, tendon transfer, or superior capsular reconstruction/patches might be a better choice than ARCR. Third, there is still no universally accepted technique for BMS. We used a 2 mm–diameter awl to create holes 1 cm deep and 5 mm apart until bone marrow extravasated from the holes for both the “greenhouse” and “crimson duvet” techniques according to personal preference. Although we did not know the best way to perform BMS in ARCR, the satisfactory outcomes in the present study demonstrated its efficacy. Fourth, the number of patients in this study was limited, and the follow-up time was short. Further studies should be performed with more patients and a long-term follow-up. Finally, we did not investigate patients aged >65 years because we doubt that aging may affect clinical outcomes. We think that by excluding elderly patients with RCTs, we can avoid selection bias as possibly as we can.
Conclusion
In the ARCR procedure, both the “greenhouse” and “crimson duvet” techniques exhibited significant functional improvement in patients with RCTs. The new “greenhouse” technique provided comparable clinical outcomes and structural integrity compared with the traditional “crimson duvet” technique at short-term follow-up.
Footnotes
Final revision submitted August 14, 2025; accepted September 18, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Beijing Jishuitan Hospital, Capital Medical University (No. K202066000).