
Abstract
Background:
Single-bundle anterior cruciate ligament reconstruction (SB-ACLR) with concomitant anterolateral ligament reconstruction (ALLR) has been associated with better clinical results when compared with isolated SB-ACLR. However, it is not known whether the improved outcomes are the result of the influence of concomitant ALLR on ACL graft healing.
Purpose/Hypothesis:
The purpose of this study was to determine whether concomitant ALLR is associated with improved graft ligamentization after SB-ACLR. It was hypothesized that ALLR would not affect graft healing.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A 1 to 1 matching study was conducted on a consecutive series of 732 patients who underwent ACLR using a hamstring tendon autograft between 2007 and 2019. Patients were excluded if they had skeletal immaturity, inflammatory joint disease, multiple ligament reconstruction (other than ALLR), or a graft rupture. Patients with concomitant SB-ACLR and ALLR (SB-ACLR/ALLR) and isolated SB-ACLR were matched 1 to 1 based on age, sex, examination under anesthesia (EUA) grade 3 pivot shift, EUA grade 3 anterior drawer test, presence of graft impingement, sagittal graft angle, skeletal maturity, lack of generalized ligamentous laxity, and multiple ligamentous injury. A total of 40 matched pairs underwent postoperative magnetic resonance imaging (MRI) within the second year after surgery to assess graft ligamentization, which was measured by the signal-to-noise quotient (SNQ) of the ACL graft.
Results:
The mean follow-up period was 41 months, with a 2-year follow-up rate of 80% in the SB-ACLR/ALLR group and 98% in the isolated SB-ACLR group. The mean duration between the index operation and MRI was 16.4 ± 3.4 months. No significant difference was observed in the SNQ of the ACL graft between the SB-ACLR/ALLR and SB-ACLR groups (6.9 ± 4.6 vs 5.2 ± 4.8, respectively; P = .066).
Conclusion:
Study findings indicated that a concomitant ALLR at the time of hamstring tendon autograft ACLR did not affect graft healing as assessed by the SNQ of the ACL graft.
Keywords
During anterior cruciate ligament (ACL) reconstruction (ACLR), a tendon graft is used to reconstruct the torn ACL. The tendon graft undergoes a series of biological events after its implantation— including revascularization, graft necrosis, proliferation, and remodeling. 1 The healing process after ACLR can be lengthy and may take up to 2 years to complete. 15 During this period, the mechanical strength of the graft is reduced. 16
Residual laxity is not uncommon after ACLR.7,11,18 In the meta-analysis by Grassi et al, 11 abnormal anteroposterior or rotatory laxity was present in at least 10% of patients who received ACLR. The prevalence of residual laxity is approximately 12% to 17% and 23% to 32% in double-bundle ACLR and single-bundle ACLR (SB-ACLR), respectively. 18 During the early healing phase of the ACL graft, there is an increase in the magnetic resonance imaging (MRI) signal intensity of the graft. This increase in MRI signal intensity is associated with a decrease in the mechanical strength of the graft. 28 In 2022, Chiba et al 7 showed that the increased signal intensity of the ACL graft in early postoperative MRI was associated with a higher incidence of residual ACLR laxity at a 1-year follow-up. It is possible that residual laxity in ACLR resulted from stretching of the graft during the remodeling process.
The anterolateral ligament (ALL) is an important secondary restraint against rotational instability of the knee. 27 Reconstruction of the deficient ALL in the form of lateral extra-articular tenodesis (LET) was performed in the mid-20th century as one of the treatment options for patients with ACL injury. 3 However, the results of LET were not consistent, and this operation was gradually replaced by ACLR in the late 20th century.9,12 Despite this, some centers in France and Italy continued to perform LET procedures, usually as a concomitant procedure at the time of ACLR.19,23
There has been increasing interest in the role of the ALL after the 2013 study by Claes et al 8 on the anatomy of the structure. A 2022 meta-analysis of randomized controlled trials showed that SB-ACLR with concomitant ALL reconstruction (SB-ACLR/ALLR) led to better clinical outcomes than SB-ACLR without concomitant ALLR, as evidenced by a lower incidence of graft rupture, a higher chance of returning to premorbid sport, and less residual ACL laxity. 21
Despite the relatively abundant publications on the clinical outcomes of concomitant ACLR and ALLR,2,4,10,13,14,23,24,25,30 limited data are available in the literature on the use of postoperative MRI to investigate the influence of concomitant ALLR on the healing of the ACL graft.5,26 We are aware of only 2 MRI studies that have compared the MRI signal intensity—as measured by the signal-to-noise quotient (SNQ) of the ACL graft between patients who underwent ACLR with versus without concomitant ALLR in the form of LET.5,26 However, conflicting conclusions were reported by these 2 studies: Cavaignac et al 5 reported a positive effect of concomitant LET on the maturation of the ACL graft, while Rojas et al 26 reported the opposite finding.
This study aimed to determine whether concomitant ALLR is associated with improved graft healing after SB-ACLR. The extent of graft maturation was assessed by comparing the SNQ on postoperative MRI of patients who underwent SB-ACLR/ALLR versus isolated SB-ACLR. It was hypothesized that ALLR would not affect graft healing after SB-ACLR.
Methods
The local human research ethics committee approved the study protocol. The need for informed consent from the participants was waived by the ethics committee. A retrospective study comparing the short-term outcomes of patients receiving SB-ACLR/ALLR and SB-ACLR was performed by reviewing the prospectively collected data in our institution's ACLR registry. The review was conducted between July 2007 and January 2019. One of the 2 fellowship-trained sports medicine surgeons (including W.P.Y.) performed all operations. Concomitant ALLR was indicated for young, active male patients who were scheduled for primary ACLR, and it was performed at our institution from 2014 onward.
The patients in the SB-ACLR/ALLR group of the present study had been recruited for enrollment in a separate randomized controlled trial comparing SB-ACLR/ALLR and double-bundle ACLR. The inclusion and exclusion criteria for this study are shown in Table 1.
Study Inclusion and Exclusion Criteria a

ACL, anterior cruciate ligament; ALLR, anterolateral ligament reconstruction; MRI, magnetic resonance imaging; SB-ACLR, single-bundle anterior cruciate ligament reconstruction.
Surgical Techniques
SB-ACLR
SB-ACLRs were performed endoscopically using a 4-stranded ipsilateral hamstring tendon autograft. All the patients underwent the same ACLR technique in the SB-ACLR. Femoral tunnel drilling was performed using anteromedial portal drilling. The graft was fixed on the femur with a cortical button and on the tibia using a bioabsorbable interference screw under maximal manual tension with the knee at 30° of flexion. Endobutton CL and Bio-RCI (Smith & Nephew) were used in 28 cases, while Rigidloop adjustable and MILARGO Advance BR (DePuy Synthes) were used in 12 cases.
SB-ACLR/ALLR
ALLR was performed by an open technique. A lateral longitudinal incision was made over the distal thigh. The iliotibial band was split longitudinally to expose the lateral collateral ligament and the lateral femoral epicondyle. The ALLR femoral footprint was identified as a proximal and posterior point to the lateral femoral epicondyle. A stab wound was then made over the Gerdy tubercle. The ALLR tibial footprint was identified at the prominence of the Gerdy tubercle. The ALLR graft was passed to the tibial wound, deep to the iliotibial band but superficial to the lateral collateral ligament. The graft was fixed at 30° of flexion and neutral rotation with 2 suture anchors. Caution was taken to avoid overtensioning of the ALLR graft during fixation.
There were 2 subgroups in the SB-ACLR/ALLR cohort. In the first subgroup (n = 14), the ALLR graft was a 1–cm wide 2-stranded graft harvested from the central one-third of the iliotibial band. A Swivelock suture anchor (Arthrex Inc) was used to secure the ALLR graft. The technique of ACLR—including femoral tunnel drilling and the ACL graft preparation and fixation in the first group—was the same as that of the SB-ACLR. The implants used for the ACLR were Rigidloop adjustable and MILARGO Advance BR (DePuy Synthes). In the second subgroup (n = 26), the ALLR graft was constructed using the remaining length of the semitendinosus tendon as a 1-stranded graft. The suture anchor used to fix the ALLR graft was a double-loaded BioComposite corkscrew suture anchor (Arthrex Inc). The graft used for the ACLR component of the second subgroup was the same as that of SB-ACLR—a 4-stranded ipsilateral hamstring tendon autograft. The outside-in technique was used to prepare the femoral tunnel of the ACLR in the second group. The ACL graft was fixed within the femoral tunnel with a bioabsorbable interference screw (MILARGO Advance BR; DePuy Synthes) and at the tibial tunnel with a cortical button (Rigidloop adjustable XL; DePuy Synthes).
Rehabilitation and Follow-up
Regardless of whether concomitant ALLR was performed, the rehabilitation protocol for primary ACLR was the same. All the patients were advised not to return to pivoting sports until 9 months after surgery. The patients were observed every 3 months in the first year and then annually in a designated ACLR clinic. Postoperative reassessment MRI was arranged for all patients. The typical schedule for postoperative MRI in the author's institute is 12 to 36 months after ACLR.
Magnetic Resonance Imaging
All MRIs were performed with a 1.5-T scanner. The patient was instructed to lie supine on the examination table with the involved knee in an extended position. T1-weighted, T2-weighted, and fat–saturated proton density images were taken. The images were captured in the coronal, sagittal, and axial planes. A T2-weighted sagittal image with a slice thickness of 3 mm and a matrix size of 512 × 512 was used to measure the SNQ. All MRIs were performed without contrast.
The ACL graft was assessed for potential impingement in the T2-weighted sagittal MRI slice that best showed the whole graft. The definitions of graft impingement were as follows: Blumensaat line posterior to the anterior margin of the tibial tunnel, graft compression, and graft hyperintensity. The sagittal graft angle was measured (Figure 1) in the T2-weighted sagittal cut that best showed the whole graft. Two circles were drawn in the proximal tibia, each touching the anterior and posterior tibial cortex. The longitudinal axis of the proximal tibia was identified by connecting the centers of these 2 circles. The angle formed by the perpendicular to the proximal tibial axis and the longitudinal axis of the ACLR graft was determined to the the sagittal graft angle.

Sagittal graft angle on postoperative MRI. The T2-weighted sagittal cut that best showed the whole graft was selected for measurement. The longitudinal axis of the proximal tibia was identified. Two circles were drawn in the proximal tibia, each touching the anterior and posterior tibial cortex. The longitudinal axis of the proximal tibia was identified by connecting the centers of these 2 circles. The angle formed by the perpendicular to the proximal tibial axis and the longitudinal axis of the ACLR graft was determined to the the sagittal graft angle. ACLR, anterior cruciate ligament reconstruction; MRI, magnetic resonance imaging.
Primary Outcome Measure: SNQ of the Graft
The SNQ of the whole graft was measured according to the methodology described by Chan and Yau. 6 The eUnity DICOM workstation and viewer (Mach7 Technologies Canada Inc) was used to perform the measurement. The T2-weighted sagittal slice that best showed the whole length of the ACL graft was used for SNQ measurement. The intra-articular portion of the graft was outlined, and the mean signal intensity per unit area of the whole graft was measured. Normalization of data was performed using the quadriceps tendon signal and the background signal (2 cm anterior to the patellar tendon) according to the following formula (Figure 2):

Two independent observers (W.P.Y. and W.L.) performed the SNQ measurements. Inter- and intraobserver reliability of the measurements data on intraobserver repeatability were obtained by repeating the measurement 1 week after the first measurement, and reliability was calculated using the intraclass correlation coefficient (ICC). The ICC values were interpreted as excellent (0.75-1), good (0.6-0.74), fair (0.4-0.59), or poor (<0.4).

SNQ Measurement on postoperative MRI. A is the signal of the graft, B is the signal of the quadriceps tendon, and C is the signal of the background. MRI, magnetic resonance imaging; SNQ, signal-to-noise quotient.
Statistical Analysis
Descriptive statistics were reported. The Student t test was used to compare the primary outcome measure (ie, SNQ) between the SB-ACLR/ALLR and SB-ACLR groups. Comparison of the study results with data from previously published studies was performed with the 1-sample Kolmogorov-Smirnov test. Statistical significance was set at P < .05. The data was analyzed using SPSS software (Version 28; IBM).
An a priori sample size calculation was performed using the data obtained from the study of Rojas et al 26 as reference values. The SNQ of the ACL graft of isolated SB-ACLR and SB-ACLR with concomitant Lemaire extra-articular tenodesis, as reported by Rojas et al, was 4.62 ± 4.29 and 7.59 ± 4.68, respectively. The sample size was determined to search for a 2.97 SNQ difference between SB-ACLR and SB-ACLR/ALLR; 0.05 and 0.8 were used for type 1 and type 2 errors, respectively. With an enrollment ratio of 1, the minimal number of samples required for each group was 33.
Results
A total of 732 ACLRs—including 685 primary ACLRs and 47 revision ACLRs—were performed at our institution between July 2007 and January 2019. Of the 685 primary ACLRs, 101 SB-ACLR/ALLRs and 584 SB-ACLRs were performed. After applying the inclusion and exclusion criteria, there were 40 SB-ACLR/ALLRs and 183 SB-ACLRs. All recruited patients underwent postoperative MRI in the second year after the index operation at a mean interval of 16.4 months postoperatively. No patient in the SB-ACLR/ALLR group was found to have graft impingement on the reassessment MRI. The mean sagittal graft angle of the SB-ACLR/ALLR group was 56.9°. A total of 40 matched pairs (40 SB-ACLR/ALLR and 40 SB-ACLR) were identified and included in the study (Figure 3). The mean follow-up length for the overall cohort was 41 months, with a 2-year follow-up rate of 80% in the SB-ACLR/ALLR group and 98% in the isolated SB-ACLR group.
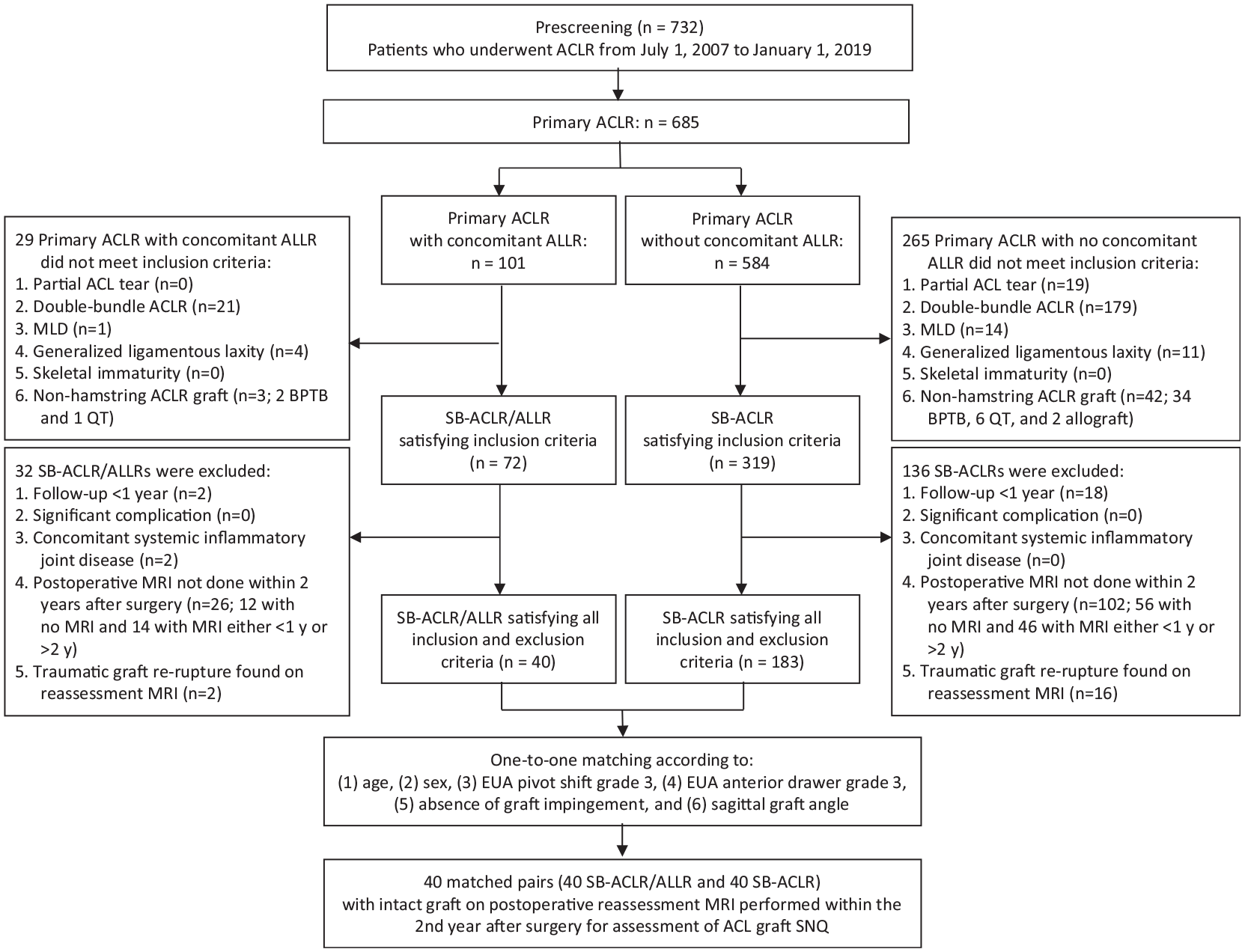
Flowchart of the enrollment procedure for the patients. ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; ALLR, anterolateral ligament reconstruction; BPTB, bone–patellar tendon–bone; EUA, examination under anesthesia; MLD, multiple ligament deficiency with concomitant ligament reconstruction, other than ALLR; MRI, magnetic resonance imaging; QT, quadriceps tendon; SB-ACLR, single-bundle anterior cruciate ligament reconstruction; SNQ, signal-to-noise quotient.
The characteristics of the matched-pair groups are reported in Table 2. The length of follow-up for the SB-ACLR/ALLR group was significantly shorter than that of the SB-ACLR group (38.2 ± 22 vs 61.1 ± 45.1 months, respectively; P = .003). There was no difference between the groups in terms of the interval between injury and surgery (P = .051) or between surgery and reassessment MRI (P = .172) (Table 2).
Patient and Surgical Data of the Matched-Pair Groups a
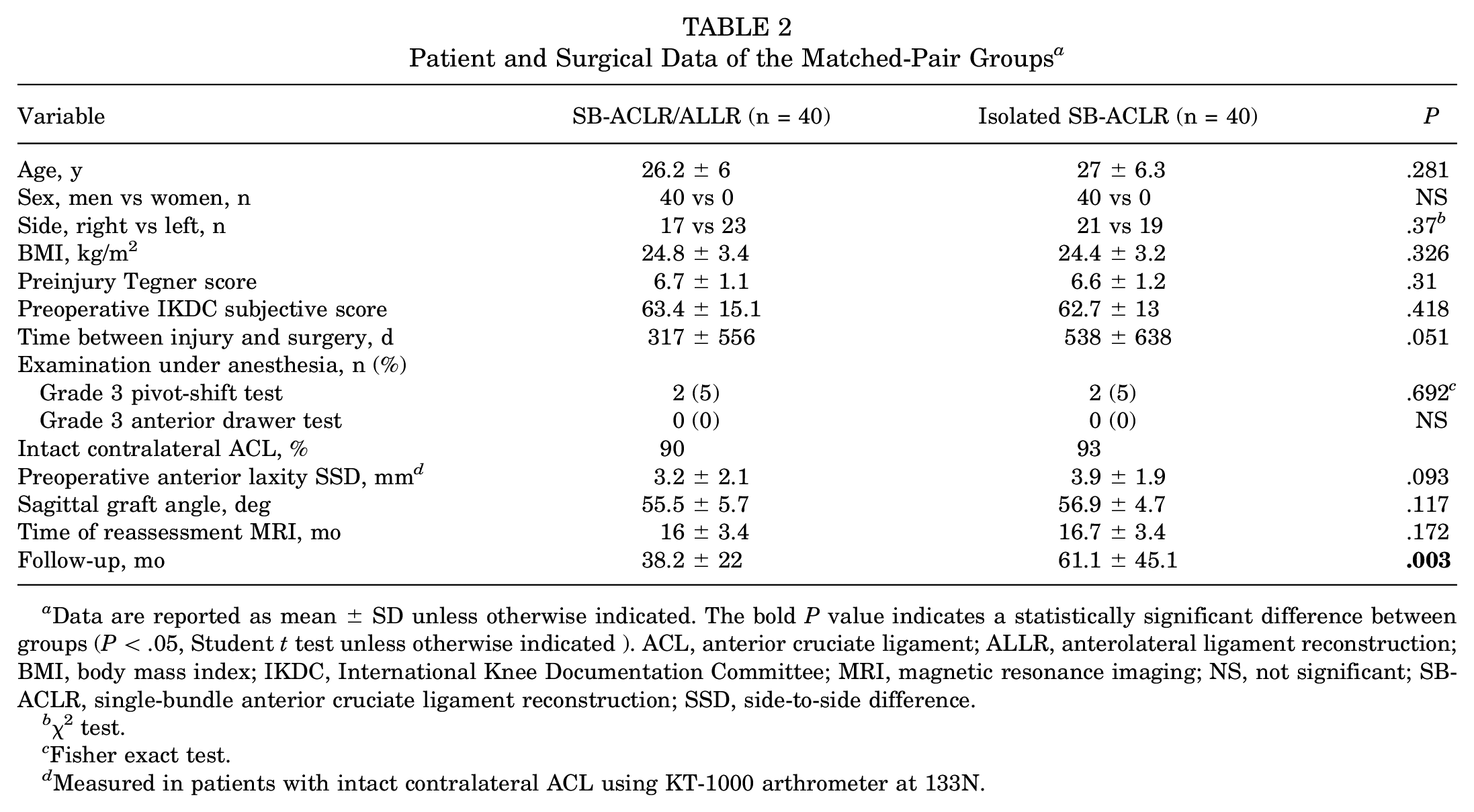
Data are reported as mean ± SD unless otherwise indicated. The bold P value indicates a statistically significant difference between groups (P < .05, Student t test unless otherwise indicated ). ACL, anterior cruciate ligament; ALLR, anterolateral ligament reconstruction; BMI, body mass index; IKDC, International Knee Documentation Committee; MRI, magnetic resonance imaging; NS, not significant; SB-ACLR, single-bundle anterior cruciate ligament reconstruction; SSD, side-to-side difference.
χ2 test.
Fisher exact test.
Measured in patients with intact contralateral ACL using KT-1000 arthrometer at 133N.
Primary Outcome Measure
The SNQ of the ACL graft of the SB-ACLR/ALLR group was 6.9 ± 4.6 and that of the SB-ACLR group was 5.2 ± 4.8. The observed difference did not reach statistical significance (P = .066; Student t test). The interobserver reliability in the SNQ measurement was good (ICC, 0.667), and the intraobserver reliability was excellent (ICC, 0.825).
Discussion
In the present retrospective 1 to 1 matching study, no significant difference was found in the SNQ of the ACL graft between SB-ACLR/ALLR and SB-ACLR (P = .066). Two years after surgery, postoperative MRI was used to assess the SNQ of the ACL graft, and the results showed similarity between the 2 groups. We compared the results of the present study to those of the 2 other studies5,26 that evaluated the SNQ of the ACL graft between patients who underwent ACLR with and without concomitant ALLR. The SNQ of the ACL graft in the SB-ACLR/ALLR group (6.9 ± 4.6) was significantly smaller than that of the participants in the Rojas et al 26 study (7.59 ± 4.68; P = .048) but significantly larger than that of the participants in the Cavaignac et al 5 study (0.5 ± 2.1; P < .001). Unlike the Rojas et al 26 study, which identified a negative impact of concomitant ALLR on ACL graft maturation, and the Cavaignac et al 5 study, which reported a positive influence, we did not find any association between concomitant ALLR and the degree of ligamentization of the ACL graft within the second year after the index surgery.
The different outcomes among the studies conducted by Rojas et al, 26 Cavaignac et al, 5 and us may be due to differences in the study designs (Table 3). Despite all 3 studies being retrospective cohort studies, our study was the only study that matched the study groups according to the known risk factors for increased SNQ of the ACL graft. There was also a difference in the choice of the ACL graft among the 3 studies. Rojas et al 26 used a 6-stranded graft (3 strands of the semitendinosus tendon and 3 strands of the gracilis tendon), while both Cavaignac et al 5 and our study used a 4-stranded graft. However, Cavaignac et al 5 used a graft composed of 4 strands of semitendinosus tendon. Our quadrupled graft consisted of 2 strands of the semitendinosus tendon and 2 strands of the gracilis tendon. The graft used in ALLR also differed among the 3 studies. Rojas et al 26 performed LET and used the central slip of the fascia lata as their graft. Although Cavaignac et al 5 described their technique as LET, they used a 2-stranded gracilis tendon graft as the graft for the ALL surgery. We used either a 2-stranded iliotibial band graft (n = 14) or a 1-stranded semitendinosus tendon graft (n = 26) as our graft for the ALLR. There was a difference in the SNQ measurement technique. Both Rojas et al 26 and Cavaignac et al 5 measured the graft signal at 3 sampled sites of the ACL graft (proximal, middle, and distal) and took the mean of these measurements as the SNQ of the graft. We measured the signal of the whole graft, which potentially minimizes sampling error.
Comparison of Studies Reporting the SNQ of the ACLR Graft in SB-ACLR/ALLR a

Data are reported as mean ± SD. ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; ALL, anterolateral ligament; ALLR, anterolateral ligament reconstruction; G, gracilis; ITB, iliotibial band; MRI, magnetic resonance imaging; SB-ACLR, single-bundle anterior cruciate ligament reconstruction; SB-ACLR/ALLR, single-bundle anterior cruciate ligament reconstruction with concomitant anterolateral ligament reconstruction; SB-ACLR/LET, single-bundle anterior cruciate ligament reconstruction with concomitant lateral extra-articular tenodesis; SNQ, signal-to-noise quotient; ST, semitendinosus.
One of the most commonly utilized noninvasive methods of examining the maturity of the ACLR graft is the SNQ,17,20,22,26,29 and it is considered suitable for comparing data within the same cohort. 29 However, no study has confirmed that the SNQ is a reliable research tool for comparing results among different studies. Hence, the discussion arising from the comparison of the SNQ of the ACL graft in SB-ACLR/ALLR between the present study and the reported data in the literature5,26 needs to be interpreted with caution.
The degree of ligamentization in the primary ACLR graft can be influenced by various factors, such as the duration since index surgery, 20 the presence of graft impingement, 29 the activity level of the patient, 17 the orientation of the implanted graft, 22 and concomitant ALLR.5,26 The differences in the reported SNQs of the ACL graft in SB-ACLR/ALLR among the present study and those of Rojas et al 26 and Cavaignac et al 5 suggest that concomitant ALLR might not be the most important factor affecting the SNQ of the ACL graft. Other confounders17,20,22,29 may be more important in determining the degree of ligamentization and healing of the graft after SB-ACLR. These include time from surgery,20,29 graft size, 22 graft bending angle, 22 and the activity level of the patient. 17 In the absence of graft impingement, the time from the index operation is the most important confounder that affects the degree of healing of the ACL graft and the SNQ measured in the reassessment MRI.20,29 Using contrast-enhanced MRI, Muramatsu et al 20 showed that the SNQ peaked at 4 to 6 months after the operation and gradually decreased from 12 to 48 months. Yau and Chan 29 found that ligamentization of the ACL graft was completed within 36 months after surgery. Oshima et al 22 reported that a large ACL graft and an acute graft bending angle were associated with a higher SNQ assessed at 1 year after surgery. Li et al 17 reported that patients with a higher Tegner activity scale were likely to have a higher SNQ when a reassessment MRI was performed at a mean of 31 months after ACLR.
The influence of concomitant ALL surgery—including both LET and ALLR—on SB-ACLR may be 2-fold. On the one hand, concomitant ALL surgery improves the rotational stability of SB-ACLR 21 and possibly results in faster maturation of the ACL graft. 5 On the other hand, the addition of concomitant ALL surgery may lead to a shielding effect on the ACLR and negatively affect graft maturation. 26
The sample size analysis was performed using data from Rojas et al. 26 However, the anterolateral procedure performed in their study was the Lemaire procedure, not ALLR. Only 2 available studies in the literature have investigated the influence of an anterolateral procedure on the healing of ACL graft by measuring the SNQ using postoperative MRI.5, 26 However, LET was the anterolateral technique used in both of the studies. Therefore, the sample size estimation was performed using the data from the study by Rojas et al. 26
Limitations
The main limitation of this study is its retrospective cohort design, in which bias is commonly present. Prospective data collection helped to reduce transfer and recall bias. The attempt to perform an exact 1 to 1 matching in nearly all the matching criteria helped to minimize selection bias. The observer’s blinding during the SNQ measurement helped decrease assessment bias. Even though these precautions were observed, bias could not be completely eliminated in this retrospective study.
In the present study, MRI was only performed at a single time point. As sequential postoperative MRI at regular intervals was not performed, it was impossible to monitor ACL graft maturation progress in both the SB-ACLR and SB-ACLR/ALLR groups. It is also unclear whether the 1.5-T MRI scanner used in this study was as accurate in measuring the SNQ as a 3.0-T scanner. Compared with SB-ACLR, the surgeons in this study began performing SB-ACLR/ALLR only from 2014 onward. Even though graft impingement was excluded and the orientation of the ACL graft was similar between the 2 groups by matching the sagittal graft angle, there was still a possibility that the surgeons gained experience in performing ACLR since SB-ACLR/ALLR was performed later in the study period.
Although the present study showed no difference in the SNQ of the ACL graft between SB-ACLR/ALLR and SB-ACLR, the P value (P = .066) was only marginally higher than .05. The data from this study are, therefore, “fragile.” If the number of patients is further increased, statistical significance could be attained and the outcome could differ. Even if the present sample size meets the power analysis criterion, the sample size issue remains a limitation of this study, and readers should be informed about this. Data on intraobserver repeatability was obtained by repeating the measurement 1 week after the initial measurement. This time frame can be considered extremely short, and the observer's memory may have biased the results.
This study aimed to determine the association between concomitant ALLR and the SNQ of the ACL graft using postoperative MRI to evaluate graft maturation. Only patients with an intact graft on the postoperative MRI were included; therefore, the incidence of graft rupture was not assessed. Graft ruptures were more common in patients with a high SNQ, as assessed on postoperative MRI. 29 Excluding patients with graft ruptures resulted in the exclusion of those with poor graft maturation and higher SNQ, leading to bias in comparing ACL graft healing between SB-ACLR and SB-ACLR/ALLR. Graft rupture is known to occur more frequently in SB-ACLR than in SB-ACLR/ALLR. 21 The SNQ of the ACL graft in the SB-ACLR group may have been higher than the value reported in this study if postoperative MRI was done at the same time point for all patients before any graft ruptures.
Conclusion
The addition of an ALLR at the time of hamstring tendon autograft ACLR did not affect the SNQ of the ACL graft. Moreover, ALLR did not appear to affect graft healing as measured by the SNQ.
Footnotes
Final revision submitted July 29, 2023; accepted August 10, 2023.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from The University of Hong Kong (ref No. UW 23-124).