
Abstract
Background:
The optimal limb position during stress ultrasound (SUS) evaluation of elbow valgus laxity has not been standardized.
Purpose:
To compare 2 elbow positions (at 90° and 30° of flexion) and report which position method better represents the increased valgus laxity characteristics of baseball players.
Study Design:
Controlled laboratory study.
Methods:
Eighteen college baseball players with no history of elbow pain or elbow disorders who belonged to a college baseball club between April and November 2021 participated in this study. The medial elbow joint space (MEJS) was recorded by ultrasonography at rest and under valgus stress, and the difference in MEJS between the conditions was considered the valgus laxity. For all participants, the MEJS was recorded at 90° and 30° of elbow flexion. In the 90° of flexion position, the participant was positioned in the supine position with abduction and external rotation of the shoulder, and 2.5 kgf of valgus stress was applied proximally to the wrist. In the 30° of flexion position, the participant was positioned in the sitting position with abduction and external rotation of the shoulder, and 3.0 kgf of valgus stress was applied to the ulnar head. Valgus laxity on the throwing and nonthrowing sides was compared between the 2 elbow positions using paired t tests or Wilcoxon signed-rank tests after checking the normality.
Results:
There was a significant difference in valgus laxity on the throwing side between the 90° and 30° of flexion positions (1.9 vs 1.1 mm, respectively; P = .002), whereas no significant difference between positions was seen on the nonthrowing side (P = .06).
Conclusion:
SUS with the elbow flexed at 90° more clearly detected valgus laxity in the study participants than the 30° of flexion position.
Clinical Relevance:
The quantitative evaluation of valgus laxity is important for baseball players to assess the risk of ulnar collateral ligament injury.
In the baseball throwing motion, a large valgus stress is loaded on the throwing elbow joint from the late cocking phase to the acceleration phase. 7 This valgus stress is repeatedly loaded on the elbow with each throw, resulting in valgus laxity.5,6,8,9,11,13,20 Excessive increase in valgus laxity is a reported risk factor for ulnar collateral ligament (UCL) injury among baseball players. 22 Hence, quantitative evaluation of valgus laxity is important.
Stress radiography has been commonly used to evaluate valgus laxity; however, the use of stress ultrasound (SUS) is being increasingly reported.2,4,10,11,18,20,22,23 Nevertheless, the limb position for SUS has not been standardized. Ciccotti et al 4 evaluated valgus laxity in baseball players in the sitting position with 30° of elbow flexion and 90° of forearm supination and reported that valgus laxity was greater on the throwing side. Several reports also applied the same limb position method for SUS.2,18 On the other hand, Sasaki et al 20 evaluated valgus laxity among baseball players in the supine position, 90° of elbow flexion, and forearm neutral rotation; they reported that valgus laxity was greater on the throwing side. This limb position method for SUS was applied in similar studies.10,11,22,24 However, it is unclear which limb position method more clearly detects valgus laxity in baseball players.
The purpose of this study was to determine the method that can detect valgus laxity in baseball players (90° or 30° of elbow flexion) and to directly compare the 2 positions to report which elbow position method better represents the increased valgus laxity characteristics of baseball players. We hypothesized that the 90° of flexion method, with an elbow joint flexion angle similar to that of the throwing motion, is superior to the 30° of flexion method.
Methods
Study Population
Eighteen asymptomatic college baseball players (4 pitchers and 14 fielders) who belonged to a college baseball club between April and November 2021 were included in this study. All participants were young men with no history of elbow pain or elbow surgery. The overall age of the participants was 18 to 20 years (mean ± SD, 18.8 ± 0.5 years), and they had 9 to 12 years (mean ± SD, 10.6 ± 0.9 years) of baseball experience. Seventeen were right-handed throwers and 1 was a left-handed thrower. All participants provided written informed consent. This study was conducted in accordance with the Declaration of Helsinki, and the study protocol was approved by the ethics committee of our institution.
Assessment
For all participants, the medial elbow joint space (MEJS), defined as the distance between the medial distal end of the humeral trochlea and the proximal end of the ulnar sublime tubercle, was measured on rest days when they had no athletic training. We used an ultrasound system with an 11-MHz linear array transducer (SONIMAGE MX1; Konica Minolta Japan Inc) and a standard transducer gel to capture images at 90° and 30° of elbow flexion, with the elbow at rest and under valgus stress (Figure 1). Valgus laxity was then calculated as the difference between MEJS values under valgus stress and at rest.

Measurement positions of a study participant: (A) 90° of flexion position with the elbow at rest, (B) 90° of flexion position with the elbow under valgus stress, (C) 30° of flexion position with the elbow at rest, and (D) 30° of flexion position with the elbow under valgus stress.
The elbow limb positions were based on previous studies.4,22 In the 90° of flexion position, the participant was positioned supine on the examination table, with 90° of shoulder abduction, 90° of elbow flexion, and neutral forearm rotation. At rest, the forearm was placed on the examination table to avoid valgus stress of the weight of the forearm. If the shoulder joint external rotation was below 90°, a towel was placed under the forearm. Under valgus stress, the position of the participant was adjusted as shown in Figure 1B. Additionally, a handheld dynamometer (μTas F-2; ANIMA Co, Ltd) adjusted to 2.5 kgf of valgus stress was attached to the proximal wrist joint. In the 30° of flexion position, the participant was positioned in the sitting position, with 90° of shoulder abduction, 30° of elbow flexion, and 90° of forearm supination. A processed acrylic plate was used to maintain the 30° of flexion position of the elbow. Under valgus stress, the same handheld dynamometer adjusted to 3.0 kgf of valgus stress was attached to the ulnar head. An assistant supported the upper arm of the participant with a wooden block to ensure that the valgus stress was properly loaded on the elbow (Figure 2). Forearm rotation and amount of valgus stress in the 2 limb positions were based on previous studies.4,22

Photograph showing the 30° of flexion position under valgus stress. An assistant supported the participant’s upper arm to ensure that valgus stress was properly loaded on the elbow.
The fiber direction of the UCL was identified, and a probe was placed parallel to it. Ultrasonographic images of the medial epicondyle, UCL, medial surface of the humeral trochlea, and coronoid process of the ulna depicted in the same field of view were used for MEJS measurements (Figure 3). ImageJ Version 1.53t (National Institutes of Health) was used as the image analysis software.
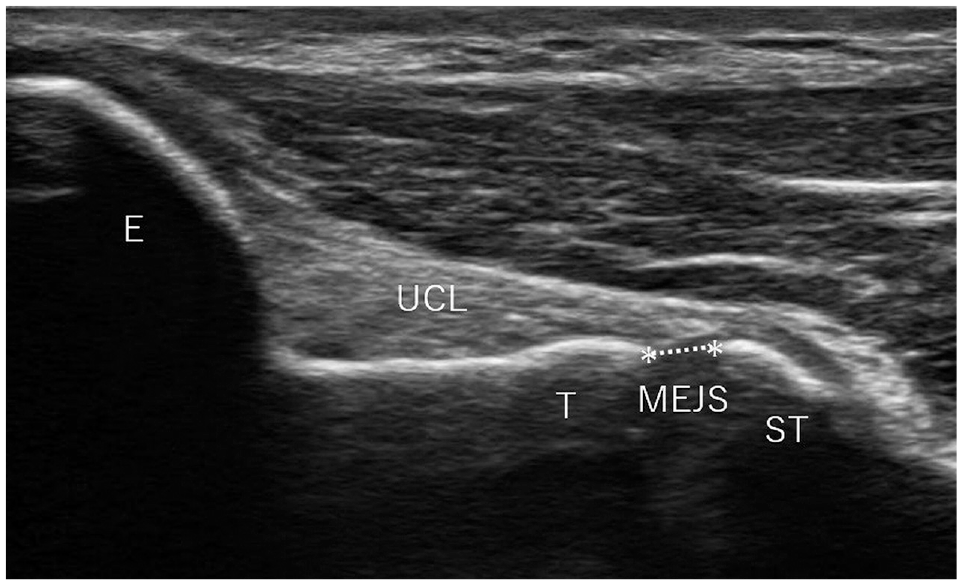
Long-axis image demonstrating the measurement of medial elbow joint space (MEJS; represented by asterisks). E, medial humeral epicondyle; ST, proximal end of the ulnar sublime tubercle; T, medial distal end of the humeral trochlea; UCL, ulnar collateral ligament.
Three orthopaedic surgeons who use ultrasound in their daily practice (R.M., T.O., and Y.H.) participated in the acquisition of the images, and MEJS measurements were performed by a single orthopaedic surgeon with 10 years of experience (R.M.). We evaluated the intraobserver and interobserver reliability of the MEJS and valgus laxity measurements by using the intraclass correlation coefficient (ICC) on a different set of study participants. Intraobserver reliability data were obtained twice by a single orthopaedic surgeon (R.M.) from 10 elbows with a 1-month interval between measurements. Interobserver reliability data were obtained independently by 2 orthopaedic surgeons (R.M. and S.T.) from 10 elbows each. ICC values were interpreted according to the criteria of Landis and Koch 15 : 0.00 to 0.20, slight; 0.21 to 0.40, fair; 0.41 to 0.60, moderate; 0.61 to 0.80, substantial; and 0.81 to 1.00, almost perfect.
Statistical Analysis
All data were analyzed using SPSS Statistics Version 27 (IBM Corp). First, the normality of each variable was checked using the Shapiro-Wilk test. If the P values of the 2 variables to be compared were >.05, they were considered to follow a normal distribution and a paired t test was performed. If either variable had a P value <.05, the Wilcoxon signed-rank test was performed. The paired t test or Wilcoxon signed-rank test was performed for comparisons of the measurements between the throwing side and nonthrowing side in both the 30° and 90° of flexion positions. Significant differences were set at a level of 5%. The effect size (ES) was calculated using the Cohen d.
Results
The intraobserver reliability (ICC[1,1]) of the MEJS and valgus laxity measurements ranged from 0.75 to 0.94, and the interobserver reliability (ICC[2,1]) ranged from 0.73 to 0.89, indicating substantial to almost perfect agreement for all measurements (Table 1).
Intraobserver and Interobserver Reliability of MEJS and Valgus Laxity a
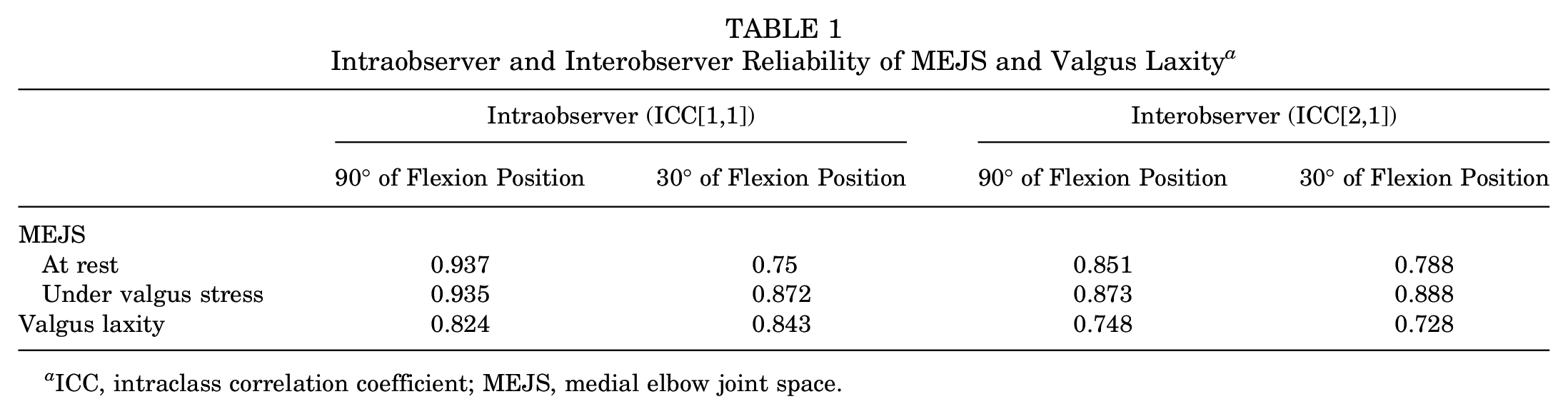
ICC, intraclass correlation coefficient; MEJS, medial elbow joint space.
Figure 4 shows the MEJS results for each elbow position. At rest, MEJS was 3.9 ± 0.9 mm on the throwing side and 3.8 ± 1.0 mm on the nonthrowing side in the 90° of flexion position. In the 30° of flexion position, it was 4.5 ± 0.8 mm on the throwing side and 4.7 ± 0.7 mm on the nonthrowing side. There was no significant difference between the 2 sides for both limb positions in the resting condition (90° of flexion position: P = .62; 30° of flexion position: P = .56). Under valgus stress, MEJS was 5.8 ± 1.2 mm on the throwing side and 5.1 ± 1.5 mm on the nonthrowing side in the 90° of flexion position and 5.6 ± 0.7 mm on the throwing side and 5.4 ± 0.7 mm on the nonthrowing side in the 30° of flexion position. In the 90° of flexion position, the MEJS was significantly larger on the throwing side than on the nonthrowing side (P = .019; ES = 0.61); whereas in the 30° of flexion position, there was no significant difference between the throwing and nonthrowing sides (P = .28).
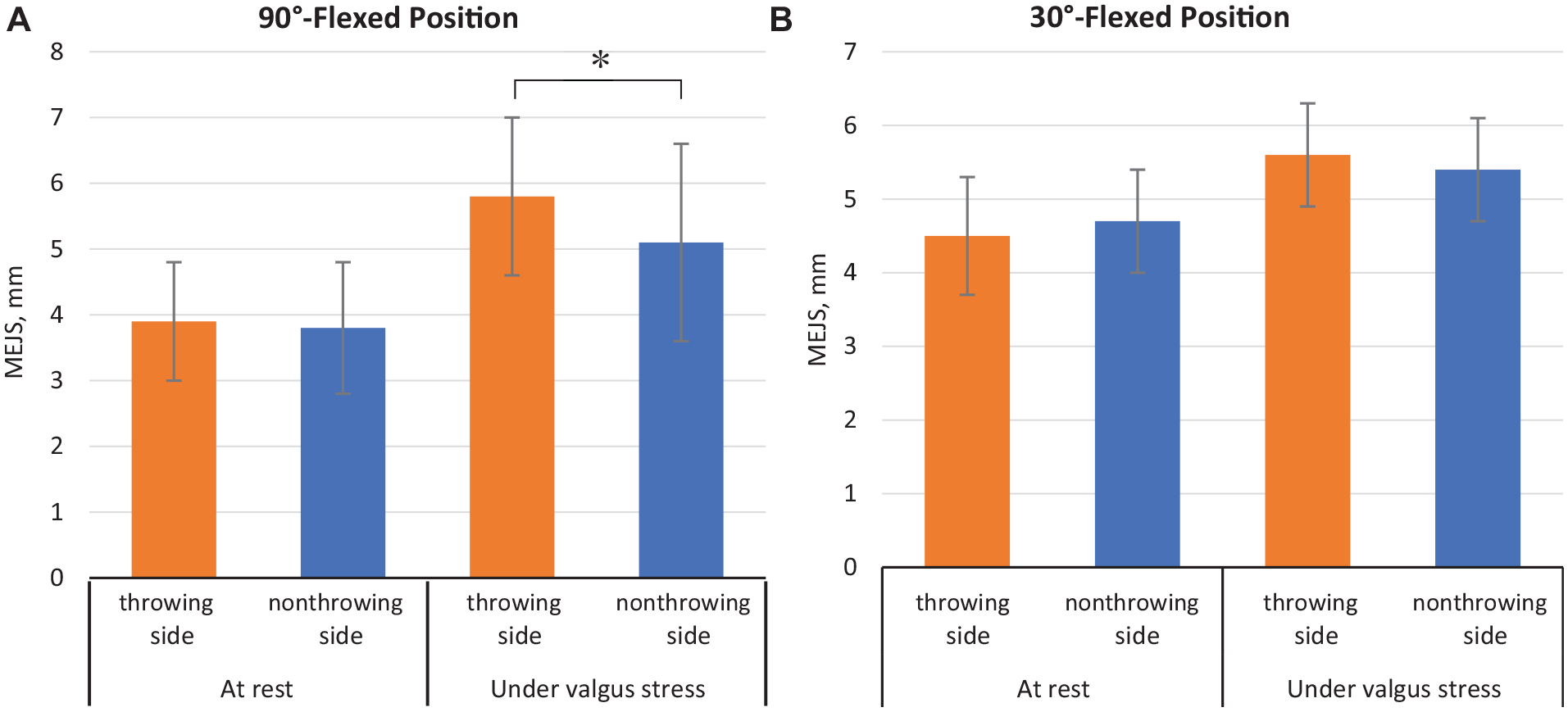
Bar graph illustrating the MEJS for the (A) 90° of flexion position and (B) 30° of flexion position. Error bars indicate standard deviation. *Statistically significant difference between throwing and nonthrowing sides (P < .05). MEJS, medial elbow joint space.
Valgus laxity was 1.9 ± 0.7 mm on the throwing side and 1.3 ± 0.8 mm on the nonthrowing side in the 90° of flexion position and 1.1 ± 0.7 mm on the throwing side and 0.8 ± 0.6 mm on the nonthrowing side in the 30° of flexion position. In the 90° of flexion position, the difference was significantly larger on the throwing side than on the nonthrowing side (P = .022; ES = 0.60), whereas in the 30° of flexion position, there was no difference between the throwing and nonthrowing sides (P = .13).
Valgus laxity was significantly larger in the 90° of flexion position than in the 30° of flexion position on the throwing side (P = .002; ES = 0.87). Ultrasound images of a representative case are shown in Figure 5. In contrast, there was no significant difference in the valgus laxity between the 30° and 90° of flexion positions on the nonthrowing side (P = .06).
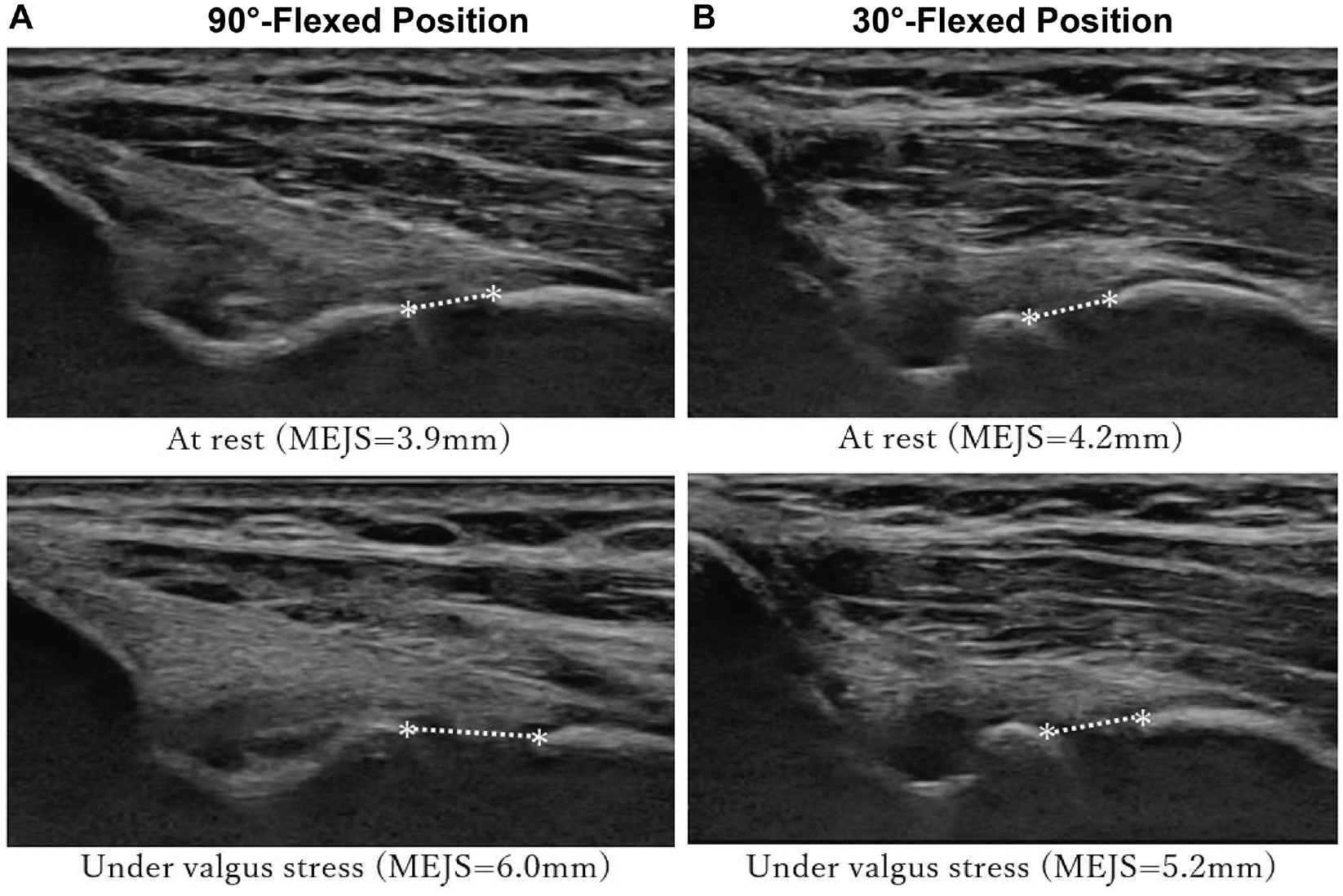
Ultrasound images from a 19-year-old pitcher showing the medial elbow joint space (MEJS; represented by asterisks) on the throwing side for the (A) 90° of flexion and (B) 30° of flexion positions. Valgus laxity was greater at the 90° of flexion position than at the 30° of flexion position (2.1 vs 1.0 mm).
Discussion
The major findings from our study were that the elbow valgus laxity on the throwing side was significantly larger (by 0.8 mm) in the 90° of flexion position than in the 30° of flexion position (1.9 vs 1.1 mm; P = .002; ES = 0.87), whereas there was no significant difference on the nonthrowing side. Therefore, the valgus laxity of the throwing elbow joint was more clearly detected with a static force in the 90° of flexion position than in the 30° of flexion position among baseball players. This indicates that the 90° of flexion position is the more optimal limb position for SUS evaluation of valgus laxity.
The evaluation of valgus instability at the elbow joint in stress radiography indicated that instability occurs when the medial joint opening exceeds 1 mm. 14 Generally, joint laxity is less severe than joint instability. Considering these factors, a difference of 0.8 mm is a clinically significant value for valgus laxity despite the difference between SUS and stress radiography. Furthermore, the difference between MEJS on the throwing and nonthrowing sides could be detected in the 90° of flexion position but not in the 30° of flexion position. These results lend further support that the 90° of flexion position is the more optimal limb position for the SUS evaluation of valgus laxity.
There are 2 important points regarding this result from a biomechanics perspective. First, the UCL is the primary static stabilizer for valgus stress of the elbow joint.12,17 Previous research on cadavers indicated that the maximum valgus instability occurs in 90° flexion position when the UCL is dissected. 3 This indicates that the maximum contribution of the UCL as a static stabilizer to valgus stress is in the 90° of flexion position. Morrey and An 16 also reported that in the 90° of flexion position, the contribution of the UCL as a static stabilizer to valgus stress is greater than that of the bone and joints. Second, the maximum valgus stress on the elbow joint in the throwing motion occurs immediately before the maximum external rotation of the shoulder joint and around 90° of elbow flexion. 8 At this instant, the elbow joint is loaded with a large varus torque comparable to the breaking strength of the UCL.1,8,25 With each pitch, the elbow joint is repeatedly loaded with this stress, resulting in valgus laxity over time.5,6,8,9,11,13,20 These 2 statements support the hypothesis that the valgus laxity in baseball players is best detected in the 90° of flexion position.
Regarding the difficulty of the procedure in different limb positions, in actual clinical practice, we consider that a reproducible and simple technique such as the 90° of flexion position is visually clear and is considered highly reproducible. In contrast, we consider that the 30° of flexion position is not visually clear and requires time, effort, and measurement with an angle meter to ensure reproducibility. In terms of simplicity, the 90° of flexion position does not require any special equipment. However, in the 30° of flexion position, equipment is needed to properly load valgus stress while maintaining the flexion angle. In this study, a simply processed acrylic plate was used to maintain the 30° of flexion position, but multiple assistants were required to maintain the limb position, such as upper arm support when loading valgus stress. Some studies have indicated using dedicated devices; however, they are expensive and not practical in clinical or sports fields.2,4,6,10,21,23 We consider that the same can be stated for limb positions other than 30°, such as 45° and 60°. Therefore, the evaluation method using the 90° of flexion position is easier to use clinically than the evaluation method using the 30° of flexion position.
In this study, the difference between the 2 limb positions is the forearm rotation in addition to the elbow flexion angle. In the 90° of flexion position, the forearm was in neutral rotation, and in the 30° of flexion position, the forearm was in supination. Safran et al 19 investigated the effect of forearm rotation on elbow valgus laxity at 30°, 50°, and 70° of elbow flexion in a cadaveric study. Results showed that when the UCL was intact, valgus laxity was greater in the neutral forearm position compared with forearm pronation or supination at all elbow flexion angles. In this study, forearm rotation in the 30° of flexion position was defined as supination on the basis of previous studies, but it is unclear whether the forearm rotation affected the magnitude of valgus laxity.
Strengths and Limitations
The strengths of this study include the uniformity of the technique, the precision of high-resolution ultrasonography, and the methods being conducted by experienced orthopaedic surgeons. It is possible that previous studies conducted with the 30° of flexion elbow position adopted in this study have not adequately assessed the valgus laxity characteristics of baseball players.
There are several limitations of this study. First, the study is limited to college baseball players. It is not known whether the same results could be obtained for other age or sex groups. Second, the number of participants in this study is small. Third, subgroup analyses by age and years of baseball experience could not be performed because of the small individual differences in these parameters in the participants. Fourth, it did not consider the differences in valgus laxity by forearm rotation within the same elbow flexion angle. Fifth, the 30° of flexion position was not measured under conditions where gravity was applied to the forearm, and this approach may have resulted in differences from the measurements in the 90° of flexion position. Sixth, ultrasound effectiveness depends on the observer. Although intraobserver and interobserver reliability was high in this study, results can differ depending on the observer’s experience with SUS. Seventh, this study did not investigate the association between valgus laxity and injuries, such as UCL injuries.
Conclusion
In the current study, the 90° of flexion position of the elbow more clearly detected valgus laxity than the 30° of flexion position, indicating that the 90° of flexion position is more optimal for SUS evaluation of elbow valgus laxity in baseball players.
Footnotes
Acknowledgements
Final revision submitted May 21, 2023; accepted July 31, 2023.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Tsukuba (reference No. 1517-3).