
Abstract
Background:
Despite the overall prevalence and success of total knee arthroplasty (TKA), a significant portion of patients are dissatisfied with their outcomes.
Purpose:
To assess the responsiveness and determine the minimally important difference (MID) of 2 patient-reported outcome measures (PROMs)—the Knee injury and Osteoarthritis Outcome Score–Joint Replacement (KOOS-JR) and the Patient-Reported Outcomes Measurement Information System Global–10 (PROMIS 10)—in patients after TKA.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
Included were patients who underwent TKA from August 2015 through August 2019 and completed baseline and postoperative KOOS-JR and PROMIS 10 surveys. The PROMIS 10 consists of 2 domains: physical health and mental health. Estimates for the reliable change index (RCI) and MID, using anchor-based and distribution-based methods, were calculated for each PROM. Regression modeling was used to determine whether patient and clinical factors predicted MID thresholds or MID achievement.
Results:
A total of 1315 patients were included. Distribution-based MIDs, calculated using various methods from baseline scores, ranged from 19.3 to 31 for the KOOS-JR, and the RCI was 4.38. Of these patients, 293 (22.3%) demonstrated small or moderate improvement, and this cohort was included in the calculation of anchor-based MIDs. The anchor-based MIDs were 16.9 and 24.3 at 3-month and 1-year follow-up, respectively, and 66% of patients achieved the MID at 12 months. Higher preoperative PROM score, male sex, non-White race, and current smoker status were predictive of failing to achieve the anchor-based MID for KOOS-JR at 1 year postoperatively (P < .05). Higher preoperative PROM score and any 90-day adverse event predicted lower thresholds of important change in anchor-based MIDs. Higher baseline PROM scores, younger age, male sex, non-White ethnicity, higher American Society of Anesthesiologists classification, preoperative narcotics use, not smoking, and longer hospital stay were all associated with lower odds of achieving the MID on the KOOS-JR or either of the PROMIS 10 subscales.
Conclusion:
The study results demonstrated relevant values for interpretation of the KOOS-JR and PROMIS 10. While patient demographics did not accurately predict which patients would achieve the MID, some potential factors predicting successful patient-reported outcomes after TKA were identified.
Keywords
Total knee arthroplasty (TKA) is one of the most common orthopaedic surgeries, and it is a successful17,36 and cost-effective35,76 treatment for late-stage knee osteoarthritis. In 2008, over 650,000 TKAs were performed in the United States alone, 8 and that number continues to rise. 72 TKAs are highly successful in the long term, as the 25-year survival rate of TKAs is estimated to be approximately 81% to 83%. 18 However, focusing entirely on revision rates underestimates poor outcomes, 57 particularly in the short term, as issues related to pain,5,21 stiffness, 21 dissatisfaction,4,65,75 and reduced quality of life 7 do not always result in revision surgery. The overutilization of TKA could be a reason for high failure rates, as operating on patients who lack appropriateness for surgery has been associated with poor outcomes.16,37,60-63 With the prevalence of TKA continuing to rise, it is critical to better define appropriateness criteria, strengthen shared decision-making tools, and identify patients most likely to benefit from surgery.16,37,60-63
Patient-reported outcome measure (PROM) scores have become an important tool for patient-centered health care, as they allow investigators to capture patients’ perspectives toward health-related constructs. 14 PROMs can be used to measure the perceived change in health status experienced by patients after a treatment and are useful for comparing different therapies or providing evidence of health care quality.11,47,48 Significant work is required to develop PROMs and confirm they are of sufficient quality for clinical use. Development and testing should include assessment of many psychometric properties, including reliability, internal structure, validity, and responsiveness. 52 Many PROMs used in patients undergoing TKA have not demonstrated sufficient quality. A 2017 review by Gagnier et al 24 found that 4 of 32 PROMs used in this population had positive evidence of measurement properties in ≥50% of the relevant categories. Two relatively new questionnaires designed for use in patients undergoing TKA are the Knee injury and Osteoarthritis Outcome Score–Joint Replacement (KOOS-JR), a modified short-form KOOS specific to TKA, and the Patient-Reported Outcomes Measurement Information System (PROMIS) Global–10 (10), a 10-item general quality of life measure with 2 domains, physical health (PH) and mental health (MH). Establishing the measurement properties is important to improve the clinical utility of these PROMs in patients undergoing TKA.
One important measurement property is responsiveness, which reflects the ability of an instrument to detect changes across time or in response to an intervention, even if those changes are small.26,27 A related concept or property is interpretability. Interpretability is the degree to which one can assign qualitative meaning to a quantitative score on a measure. Interpretability is often reported as the minimally important difference (MID), minimal clinically important difference (MCID), or minimally important change.13,38 These metrics are estimated through either distribution-based (ie, statistically based on the distribution of outcome scores) or anchor-based (ie, directly asking patients if they have changed by a small but important amount) methods. Anchor-based methods can vary by subgroup; thus, understanding whether demographic or patient characteristics are associated with reported MIDs can lead to better interpretation.1,59,73 Similarly, the reliable change index (RCI) can be used to interpret whether true change has occurred within patients. 27 The RCI represents the magnitude of change required for 2 scores to be considered statistically significantly different given the measurement error of the instrument, much like a minimal detectable change (MDC) score. To date, the RCI has never been estimated for the KOOS-JR or the PROMIS 10.
Previous studies estimating the MID of the KOOS-JR have provided a wide range of MID values, from 6 to 14 points depending on the method used.10,39,47,69 Two studies assessing responsiveness of the PROMIS 10 did not report MID values,55,70 and 1 study that did report the MCID of the PROMIS 10 PH domain showed approximately 2.5 points regardless of method; however, the PROMIS 10 MH domain did not change during follow-up, so the MID could not be assessed. 39 Further evidence supporting MID thresholds and understanding whether these thresholds vary when calculated through various methods within a cohort, or for different subgroups, is required.
The purpose of this study was to assess the responsiveness and interpretability of the KOOS-JR and PROMIS 10 in patients after undergoing TKA. Our specific objectives were to (1) establish the MIDs and RCI for KOOS-JR, PROMIS 10 PH, and PROMIS 10 MH among patients who underwent TKA; (2) compare MID estimates determined through various methods for robustness and triangulation; (3) assess the influence of baseline patient characteristics and clinical factors on these estimates; and (4) determine preoperative threshold values for KOOS-JR that might predict patients at risk of not achieving the MID.
Methods
Participants
This retrospective cohort study involved searching our institutional joint replacement database for patients who underwent primary, unilateral TKA between August 2015 and August 2019. As this study involved retrospective analysis of deidentified registry data, ethics approval was waived by our institutional review board before this review. Patients were excluded from our analysis if they were missing preoperative KOOS-JR data, underwent bilateral TKA, or underwent revision surgery during the study period.
Data Collection
Data used in this analysis were obtained from our institutional database and the Michigan Arthroplasty Registry Collaborative Quality Initiative, a statewide joint registry in which these patients were included. Patients participating in the registry provided demographic information preoperatively and completed PROMs at each clinical visit. Surgical information and outcome data were recorded for each participant. We pulled data related to demographics, surgical information, surgical outcomes, and PROMs. Baseline demographics and patient characteristics included age, sex, body mass index (BMI), laterality, race, the American Society of Anesthesiologists (ASA) classification, preoperative smoking status, history of diabetes mellitus, preoperative opioid use, length of stay, discharge disposition, and 90-day postoperative events. The ASA classification is a subjective assessment that categorizes a patient into 1 of 6 groups based on his or her preoperative, physiological status to predict operative risk,15,51 which we used as a proxy for overall health. Ninety-day event data included prosthetic joint infection, periprosthetic fracture, dislocation, deep vein thrombosis/pulmonary embolism, return to emergency department, readmission, return to operating room, and death.
Outcome Measures
Patients completed the KOOS-JR and PROMIS 10 at baseline and each postoperative visit. In addition, a satisfaction questionnaire was completed at each postoperative visit. We categorized follow-up visits into early (2-16 weeks) and late (6-18 months) postoperative time points, and patients with PROMs for ≥1 visit within each follow-up category were included. The PROMIS 10 was not completed in early follow-up, so only data from the late postoperative time point were included.
The KOOS-JR score is a disease-specific questionnaire that was developed from the original full version of the KOOS survey and contains 7 items that ask patients to rate symptoms experienced over the past week on a 5-point ordinal scale (none, mild, moderate, severe, or extreme). 45 Items are categorized into 3 subscales: stiffness, pain, and functional limitations. Total scores range from 0 (total knee disability) to 100 points (perfect knee health). Previous studies have demonstrated reliability, validity, and responsiveness of the KOOS-JR in patients undergoing TKA.39,46
The PROMIS 10 was developed from the original full version of the PROMIS survey and provides a generic, rather than disease-specific, assessment of a patient's overall PH and MH. It contains 9 items scored on a 5-point ordinal scale and 1 pain scale scored on an 11-point numeric rating scale. The score can be categorized into two 4-item domains, MH and PH. 29 Subscores are standardized to the general population using a T-score conversion, where 50 points represents the average score of the US population and higher scores reflect better health. 67
The satisfaction survey included the following 3 questions: (1) How much did your surgery improve the quality of your life? (2) How satisfied are you with the results of your surgery? and (3) If you could go back in time and decide to have surgery again, would you? Patients responded on a 7-point Likert scale to indicate their agreement with each question; responses ranged from no improvement (0 points) to more improvement than I thought possible (6 points).
Statistical Analysis
We did not perform a formal sample-size calculation for this retrospective study, as all patients with available data were included and there is no accepted method for performing sample-size calculation for establishing minimal differences. We reported baseline characteristics using means and standard deviations for continuous variables and proportions for categorical variables. To determine whether demographic characteristics were associated with loss to follow-up, we compared demographic characteristics of patients who completed late postoperative forms with those who did not using the independent t test for continuous data and the chi-square test or Fisher exact test for categorical data.
First, we estimated the MDC score, or the smallest change in outcome score that exceeds the instrument's measurement error, using the RCI. The RCI was calculated using the formula described previously by Ferguson et al 20 and Jacobson and Truax. 34 We calculated the reliability of the KOOS-JR in our sample using the Cronbach alpha and used this value to calculate the standard error of difference (SED) between KOOS-JR scores. We determined the mean change in score required to obtain an RCI of >1.96, which reflects real change beyond measurement error. 34
Second, we determined the ability of each PROM to detect clinically important change. We used several methods to assess the robustness of the MID estimates and better triangulate thresholds.33,53 The distribution-based MID, which assumes a normal response distribution, was calculated using several approaches. We used the standard deviation of baseline scores to estimate the MID. We divided the standard deviation by 2 and 3 to establish 0.5 SD and 0.33 SD estimates. 54 Then, we used receiver operating characteristic (ROC) curves to quantify the area under the ROC curve (AUC) for each PROM. The sensitivity and specificity were used to calculate a range of possible MIDs for each PROM.12,23 Next, we calculated the anchor-based MIDs using the first question of the global satisfaction survey, which asked for the patient-reported improvement in quality of life, as our external criterion.56,78 Patients who reported “a little improvement” and “moderate improvement” at early or late postoperative visits were selected. Patients who demonstrated greater improvement were excluded to estimate small, important change. We calculated the mean change score on each PROM for these patients, then presented this value as the MID. We determined the proportion of patients whose change scores exceeded the MIDs and determined the magnitude of change each patient experienced in MID units (ie, we divided each patient's change score by the MID).
Next, we investigated whether the MID threshold differed for certain subgroups of patients. We used linear regression analysis to determine whether demographic and surgical characteristics, including age, BMI, sex, race, preoperative smoking status, preoperative opioid use, baseline PROM score, history of diabetes mellitus, ASA classification, length of stay, and any 90-day adverse event, were associated with the magnitude of change scores for patients included in the anchor-based analysis (ie, those who indicated a little or moderate change on the satisfaction scale). We checked all assumptions and presented the effect estimate, associated 95% CI, and P value for each predictor.
Then, we used logistic regression analysis to determine whether demographic and surgical characteristics were associated with achieving the MID in the entire cohort. We included the demographic and surgical characteristics described above, checked all assumptions, and provided effect estimates, 95% CIs, and P values for each predictor.
Previous studies have shown that preoperative outcome scores are associated with failure to achieve the MID after treatment.19,42,74,80 Thus, we performed ROC curve analysis and calculated the Youden index to estimate a threshold score on preoperative PROMs that might predict which patients are unlikely to experience the MID after undergoing TKA. 79 We evaluated this threshold using the AUC, where a value >0.7 was considered acceptably predictive. All statistical analyses were performed using either Excel (Microsoft) and Stata/MP (Version 14.2; Stata). Statistical significance was set at P < .05 for all analyses.
Results
Of the 1507 patients who underwent primary unilateral TKA, 1315 (87.3%) were included in this analysis. Demographic characteristics for our sample, which had a mean age of 67 years and was 58% female, are presented in Table 1. Availability of outcome data is reported in the Strengthening the Reporting of Observational studies in Epidemiology flow diagram (Figure 1).
Demographic Characteristics of Patients Undergoing TKA a

Data are reported as mean ± SD or n (%). ASA, American Society of Anesthesiologists; BMI, body mass index; MID, minimal important difference; TKA = total knee arthroplasty.
These patients demonstrated small or moderate improvement and were used to calculate the anchor-based MID.

Strengthening the Reporting of Observational studies in Epidemiology flowchart for patients in the study cohort. KOOS-JR, Knee injury and Osteoarthritis Outcome Score–Joint Replacement; Postop, postoperative; PROM, patient-reported outcome measure; PROMIS, Patient-Reported Outcomes Measurement Information System; TKA, total knee arthroplasty.
The early and late follow-up visits occurred at a mean of 3 months and 1 year postoperatively, and KOOS-JR scores were available for 1148 (87%) patients at the early follow-up, 765 (58%) at the late follow-up, and 683 (52%) at both time points. The proportion of patients missing preoperative KOOS-JR surveys differed by surgeon, and those excluded had higher baseline PROMIS 10 PH scores compared with those who were included (P < .05). Missing late postoperative KOOS-JR forms was associated with ethnicity, surgeon, smoking status, and preoperative opioid use (P≤ .01 for all) (Appendix Table A1).
Mean PROM scores at baseline and each follow-up appointment, along with change scores between baseline and 1 year, are presented in Table 2. The 90-day adverse event rate was 12.5%; overall, however, patients were satisfied, as 87% indicated they would undergo the surgery again. A summary of 90-day outcomes is available in Appendix Table A2.
Baseline and Postoperative Scores for the KOOS-JR and PROMIS 10 a

Data are reported as mean ± SD. Dashes indicate scores were not measured for that period. KOOS-JR, Knee injury and Osteoarthritis Outcome Score–Joint Replacement; MH, mental health; PH, physical health; PROM, patient-reported outcome measure; PROMIS 10, Patient-Reported Outcomes Measurement Information System Global 10.
Difference between baseline and late postoperative scores using patients with available outcomes at both time points.
P value for change in scores from baseline to late postoperative. All differences were statistically significant (P < .05).
KOOS-JR
The RCI for the KOOS-JR was 2.93 (95% CI, 2.80-3.07) at the early follow-up and 4.38 (95% CI 4.19-4.58) at the late follow-up. The distribution-based MIDs were 4.53 and 6.80 points when calculated using 0.33 SD and 0.5 SD of baseline scores, respectively. The ROC curve–based estimates ranged from 16.5 to 31.0 points at the 3-month and 1-year follow-up, respectively; however, only the 3-month follow-up estimate showed sufficient predictive reliability (range, 16.5-19.7 points, AUC = 0.72). Of 1315 patients, 284 demonstrated small or moderate change at 3 months, while 144 demonstrated small, important change at 1 year. The anchor-based MIDs were 16.9 and 24.3 points at the 3-month and 1-year visits, respectively.
PROMIS GH-10 PH
The distribution-based MIDs for the PROMIS 10 PH were 2.03 and 3.04 points using the 0.33-SD and 0.5-SD estimates from baseline scores, respectively, while the ROC curve method showed the MID range was 8.8 to 11.0 points. A total of 93 patients who completed the PROMIS 10 PH at 12 months improved by a small or moderate amount, and the anchor-based estimate from this cohort was 6.59 points.
PROMIS GH-10 MH
The distribution-based MIDs for the PROMIS 10 MH were 2.86 and 4.29 points at the 3- and 12-month follow-ups, respectively, while the ROC-curve based MID estimate was 3.4 points. A total of 98 patients improved by a small or moderate amount at 12 months and completed the PROMIS 10 MH, and the MID estimate was 1.64 points (Table 3).
MID Estimates, Proportion of Patients Achieving Those Thresholds, and Mean Number of MID Units They Improved by for Each PROM a
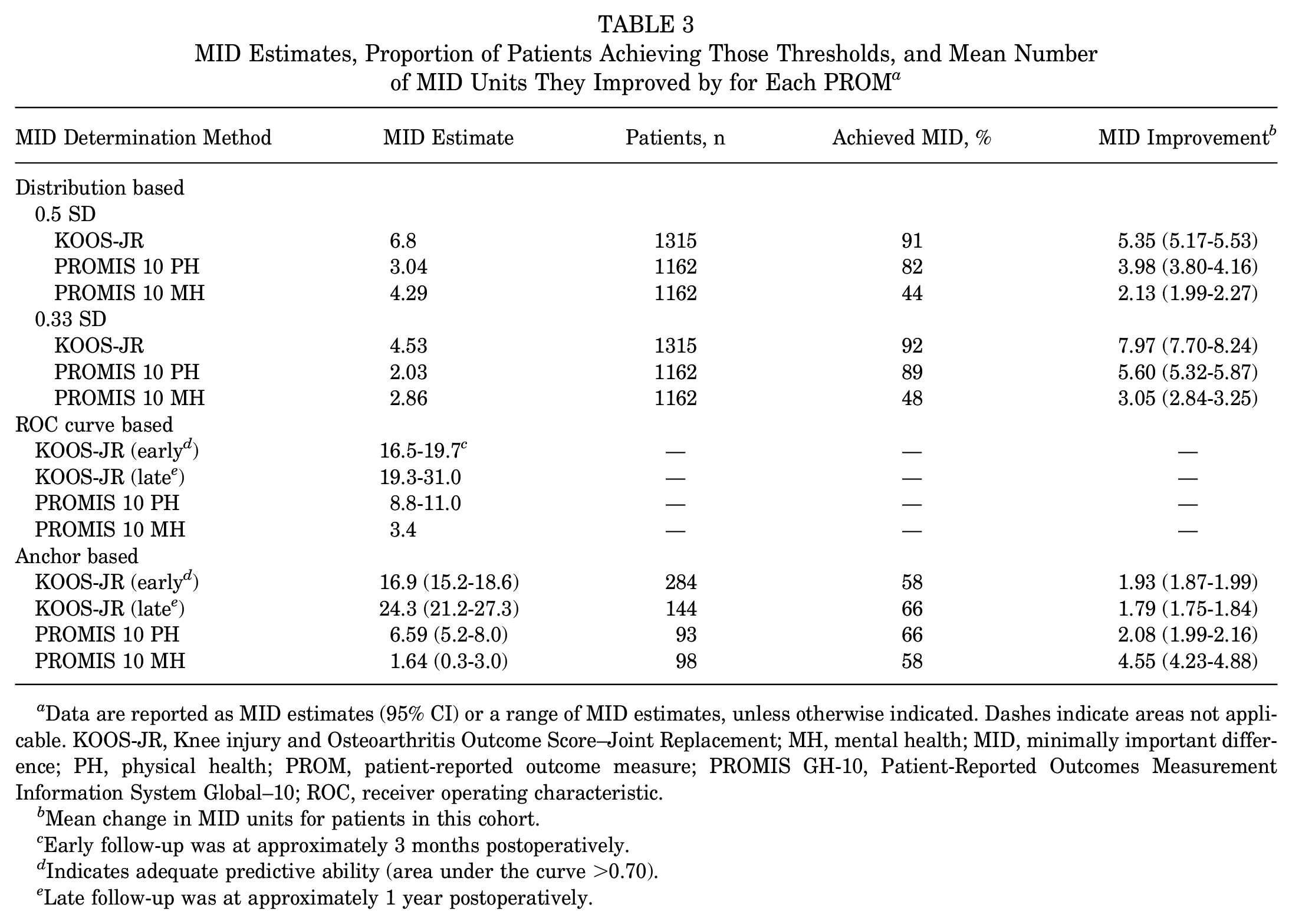
Data are reported as MID estimates (95% CI) or a range of MID estimates, unless otherwise indicated. Dashes indicate areas not applicable. KOOS-JR, Knee injury and Osteoarthritis Outcome Score–Joint Replacement; MH, mental health; MID, minimally important difference; PH, physical health; PROM, patient-reported outcome measure; PROMIS GH-10, Patient-Reported Outcomes Measurement Information System Global–10; ROC, receiver operating characteristic.
Mean change in MID units for patients in this cohort.
Early follow-up was at approximately 3 months postoperatively.
Indicates adequate predictive ability (area under the curve >0.70).
Late follow-up was at approximately 1 year postoperatively.
The RCI for the KOOS-JR indicated that 64% and 83% of patients were found to have undergone statistically significant change at early and late follow-up visits, respectively. Based on our estimated MIDs, 58% and 66% of patients achieved the KOOS-JR anchor-based MID at early and late follow-up, respectively. On average, patients who achieved the MID improved by 1.93 and 1.79 MID units at the early and late visits, respectively. The Cronbach alpha for the KOOS-JR was .85, and the SED was 7.45 points. For the PROMIS 10 PH and PROMIS 10 MH, we found 66% and 58% of patients achieved the anchor-based MIDs, respectively.
Our linear regression model showed that higher baseline PROM scores on the KOOS-JR and PROMIS 10 MH predicted lower anchor-based MID thresholds within patients reporting a little to moderate improvement (P < .05), while experiencing an adverse event within 90 days of surgery was also associated with smaller change scores on the KOOS-JR at the late follow-up (P = .04) (Table 4).
Results of Multivariable Regression for Predicting the Anchor-Based MID Threshold Using Demographic and Surgical Characteristics a
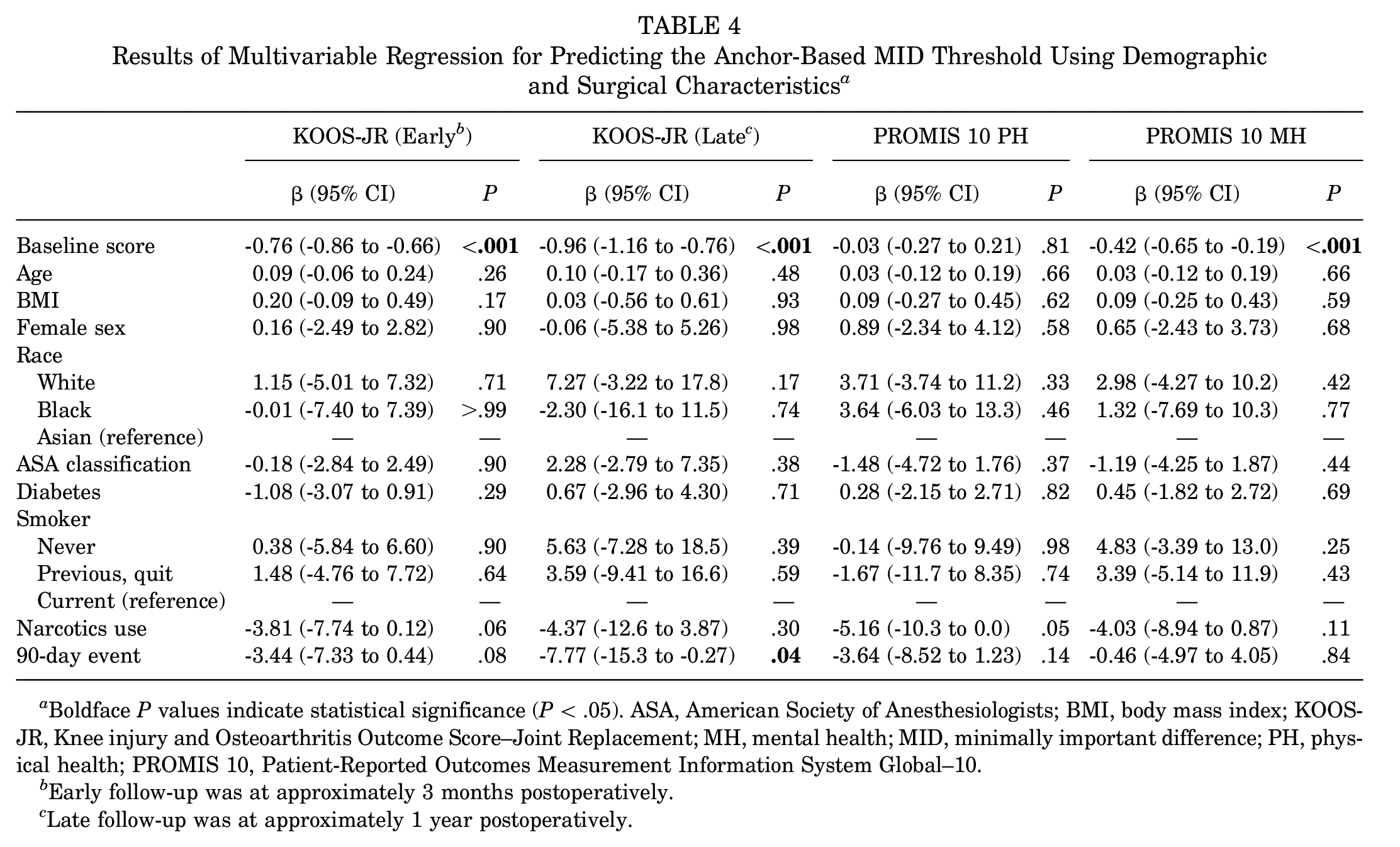
Boldface P values indicate statistical significance (P < .05). ASA, American Society of Anesthesiologists; BMI, body mass index; KOOS-JR, Knee injury and Osteoarthritis Outcome Score–Joint Replacement; MH, mental health; MID, minimally important difference; PH, physical health; PROMIS 10, Patient-Reported Outcomes Measurement Information System Global–10.
Early follow-up was at approximately 3 months postoperatively.
Late follow-up was at approximately 1 year postoperatively.
Table 5 contains the results of our logistic regression model identifying predictors associated with achieving the anchor-based MID within our cohort. Higher baseline PROM scores were associated with lower odds of achieving the MID for all PROMs and time points (P < .05). Older age was associated with higher odds of achieving the KOOS-JR at early follow-up (odds ratio [OR], 1.03; 95% CI, 1.03-1.06; P = .01), while female sex was associated with higher odds of achieving the MID for the early and late KOOS-JR and the PROMIS 10 MH (P < .05). Higher ASA class was associated with lower odds of achieving the MID for PROMIS 10 PH (OR, 0.50; 95% CI, 0.32-0.78; P < .001). Preoperative opioid use (OR, 0.55, 95% CI, 0.35-0.87; P = .01) and longer hospital stay (OR, 0.80; 95% CI, 0.68-0.93; P < .001) were associated with lower odds of achieving the KOOS-JR MID at early follow-up, and patients who had an adverse event in the first 90 days were less likely to achieve the MID for PROMIS 10 MH (OR, 0.49; 95% CI, 0.25-0.95; P = .04). Additionally, non-White ethnicity was associated with lower odds of achieving the MID for KOOS-JR at both early and late follow-up and for PROMIS 10 PH (P < .05). Last, current smokers were more likely to achieve the MID for KOOS-JR at late follow-up (OR, 4.53; 95% CI, 1.16-17.64; P = .03).
Results of Multivariable Regression Analysis to Determine Predictors of Achieving Anchor-Based MIDs for Each PROM and Time Point a

Boldface P values indicate statistical significance (P < .05). ASA, American Society of Anesthesiologists; BMI, body mass index; KOOS-JR, Knee injury and Osteoarthritis Outcome Score–Joint Replacement; MH, mental health; MID, minimally important difference; PH, physical health; PROM, patient-reported outcome measure; PROMIS 10, Patient-Reported Outcomes Measurement Information System Global–10.
Early follow-up was at approximately 3 months postoperatively.
Late follow-up was at approximately 1 year postoperatively.
When the Youden index was used, the threshold values for KOOS-JR at early and late follow-up were 46 and 49, respectively. For PROMIS 10 MH and PROMIS 10 PH, they were 50 and 39, respectively. These threshold values define the maximum preoperative scores after which the likelihood of a patient's experiencing an MID began to diminish. However, none of these calculations were acceptably predictive, with all AUC values <0.7 and corresponding sensitivity and specificity values ranging only from 26% to 50% (Table 6).
Threshold Values Calculated Using the Youden Index and Their Predictive Capabilities a

AUC, area under the receiver operating characteristic curve; KOOS-JR, Knee injury and Osteoarthritis Outcome Score–Joint Replacement; MH, mental health; PH, physical health; PROMIS 10, Patient-Reported Outcomes Measurement Information System Global–10.
Early follow-up was at approximately 3 months postoperatively.
Late follow-up was at approximately 1 year postoperatively.
Discussion
Defining successful outcomes after TKA is challenging, as health is multifactorial and what constitutes success may differ between stakeholders. The purpose of our study was to estimate what change in health status constitutes important change for 2 questionnaires, the KOOS-JR and PROMIS 10, after TKA. We found a wide range of scores for the MID, from 4.5 to 31 points on the KOOS-JR, and from 2.0 to 11.0 points on the PROMIS 10, depending on the time point and method used. Providing a range of MIDs is recommended, but still only specific to a sample with similar characteristics to our study. Previous studies have shown considerable variation related to the method of estimation, the population included, and follow-up frequency and duration, 3 though the variance in our study was greater. Our distribution-based estimates derived from the variance of baseline scores are lower than our anchor-based estimates, similar to a previous study of KOOS-JR responsiveness after TKA. 47 Accepting the distribution-based MID on its own when the anchor-based MID is much higher may be inappropriate, as it disregards patients’ perspective of importance. 25 Ultimately, it is important to remember that MIDs are designed to provide some threshold for clinicians to assess whether true, important change has occurred. However, other thresholds, such as Patient Acceptable Symptom State or substantial clinical benefit, may be better suited for determining whether a change in treatment is required. 66 As such, we agree with previous suggestions that utilizing the lower end of the estimate may be appropriate when there are few consequences to consider. 33 However, a more conservative approach utilizing a higher threshold is necessary when evaluating treatment effects or determining sample size for studies that utilize a threshold of important change.
One factor that may contribute to variance in anchor-based calculations is the lack of a gold standard in terms of the external criterion used to assess global improvement. Poor anchoring questions lead to poor estimates of MIDs, and the use of different change measures affects the ability to interpret or apply results across different populations. In our study, minimally important change was defined as a “little” or “moderate” improvement in quality of life from the time of surgery. Including patients who improved by a moderate amount could overestimate the amount of score change required to reach the minimally important threshold however, we felt it was better to include these patients than limit the estimate to those who changed by a little, which patients may or may not equate to important change.
Comparison of MID values and overall patient satisfaction in our cohort further supports the idea that our anchor-based MID overestimated the amount of change required to reach a threshold of importance. We found that just 66% of patients in this cohort achieved the anchor-based MID of 24.3 points, yet 87% of patients indicated they were satisfied with their TKA and would undergo the surgery again if given the opportunity. Previous research has shown more similar results between important improvement and satisfaction after TKA compared with our findings. 41 While change in health status and satisfaction are distinct constructs, both are multifaceted, and overlap likely exists between them. Qualitative interviews with patients could help elicit similarities and differences between these constructs.6,26 Lyman et al 47 reported anchor-based MIDs for the KOOS-JR of 14 to 20 points, slightly lower than what we found. Within their cohort, 81% to 91% of patients achieved the MID by 2 years postoperative, which more closely aligns with traditional success rates post-TKA. 57 Interestingly, 83% of our sample achieved the RCI for the KOOS-JR at 1-year follow-up, which more closely matched our assessment of global patient satisfaction.
We estimated that the MID for the PROMIS GH-10 PH was 2 to 11 points using distribution-based methods and 5 to 8 points using anchor-based methods. MIDs for the PROMIS GH-10 PH were previously reported in patients undergoing TKA in a study by Khalil et al, 39 and they found the MID was much lower, ranging from 2.3 to 2.5 points. The authors determined the anchor-based MID using the KOOS-JR to be their external criterion, though the KOOS-JR is not designed to measure the importance of change experienced by patients. This unproven anchor along with our decision to include patients who experienced moderate change could both contribute to the differences between their estimates and ours. Our distribution-based MIDs calculated from baseline variance closely approximated their MIDs, though comparison with our anchor-based thresholds suggests their values may underestimate what patients consider important change within our sample. Further research related to significant discrepancies between distribution- and anchor-based MIDs between and within studies needs to be undertaken before MIDs are used to compare treatments and guide clinical decision making.
One potential way to improve the clinical application of PROMs is to define cutoff scores that predict which patients may or may not benefit from treatment. While we presented cutoff scores for each questionnaire and time point in our study, our threshold values are clinically useless, as the AUC value falls well below the acceptable threshold of 0.7. Thus, using these values to identify surgical candidates likely to achieve good outcomes after TKA would be potentially harmful. Khalil et al 39 also performed ROC analyses to determine baseline PROM scores that may discriminate between achieving and failing to achieve the MID. For PROMIS 10 PH, their calculated threshold value of 38 was similar to our estimate of 39, and although they demonstrated higher sensitivity (59%) and specificity (70%), 39 this cut point would require further validation to be useful. While patients with higher baseline scores may be less likely to achieve large change scores postoperative, this does not necessarily mean they are poor surgical candidates. These patients likely opt for surgery because their osteoarthritis is symptomatic enough to prevent acceptable function. These patients may accept smaller changes as important, which would suggest important change is not necessarily linear (ie, a 5-point change in PROM score may not have the same meaning in those with severe limitations compared to those with mild limitations if they are both considering surgery). Many studies across a wide variety of musculoskeletal disorders have shown that baseline PROM scores are related to differences in MIDs9,19,40,42,74,80; thus, it is important to assess the impact of patient characteristics on reported MIDs. In our linear regression model, the only other variable that significantly affected anchor-based MID estimates was suffering an adverse event within 90 days, which predicted a reported MID approximately 8 points lower on the KOOS-JR at 1 year. This shows that early adverse events can affect the long-term trajectory of PROMs and potentially influence the magnitude of change those patients later consider to be important, a new finding in this area.
Additionally, we used logistic regression analysis to predict which patients had a higher probability of achieving the MID postoperatively. Higher preoperative PROM scores were associated with smaller change in outcome scores and failing to achieve the MID for all PROMs, which is consistent with prior research. 28 While this could be due to differences in the degree of change or proportion of change considered important, these patients may warrant particular attention when it comes to presurgical counseling and setting of realistic patient expectations. Applying this to the general population, patients with high functional scores seeking knee replacement surgery should understand that while TKA generally leads to improvement in pain and function, they may not see the magnitude of change that patients with greater functional limitations realize. It is possible that small increases in functional scores could be important to these patients, which may explain why they are seeking surgery despite having better preoperative function than others in the TKA population.
Several factors were associated with lower odds of achieving the KOOS-JR MID by 3 months postoperatively, including younger age, male gender, non-White ethnicity, preoperative narcotics, and longer hospital stays. Preoperative narcotic use has been associated with poor pain control requiring greater narcotic use postoperative,68,77 early TKA revision, 2 and longer postoperative hospital stay. 43 Longer hospital stays may be required for patients with risk factors or complications, which could also affect improvement over the first 3 months postoperative. Male sex, non-White ethnicity, and being a nonsmoker were associated with not achieving MIDs for various PROMs at 1 year postoperative. Our finding that smokers are more likely to achieve the MID for the KOOS-JR at 1 year postoperative contradicts our clinical hypotheses and previous findings in the literature, as the negative impact of smoking on health status and its association with poor outcomes after TKA is well-documented.44,50,71 This may be a spurious result due to the small number of current smokers in our study, as this relationship was only found for 1 questionnaire, at 1 time point, with significant uncertainty around the estimate (95% CI, 1.16-17.64). Interestingly, smoking may also be a proxy for lower socioeconomic status, 31 representing a lack of resources and access to health care. We also found that non-White ethnicity was associated with lower odds of achieving the MID on the PROMIS 10 PH and KOOS-JR at any time point. Previous studies have shown that race and ethnicity are associated with higher risk of emergency department visits, readmission, and aseptic revision after TKA for Black patients compared with White patients. 30 Issues of health disparity are multifaceted; and individual, health care, and societal factors may all contribute to worse outcomes in Black patients. 32 Early adverse events were associated with worse PROMIS 10 MH scores at 1 year postoperatively, which demonstrates that physical setbacks early in rehabilitation can have lasting mental effects in patients. Further work exploring and calculating MIDs within subgroups of patients that may differ could improve the delivery and interpretation of treatments for all patients.
Strengths and Limitations
This study has several strengths. We utilized multiple methods to estimate a range of MIDs for the KOOS-JR and PROMIS 10 MIDs, which improves the likelihood of capturing meaningful improvement. Collection of the global satisfaction questionnaire within our institutional registry led to a large sample for anchor-based estimates, which few joint registries are capable of. We believe the large, well-characterized representative sample improves the validity and generalizability of our MID estimates.
Our study also has limitations. This retrospective study was limited by the availability of the collected data; while 87% of patients completed early postoperative surveys, only 58% completed surveys at 1 year, increasing the potential for attrition bias and potentially affecting generalizability. We were able to compare the demographic characteristics of patients with data to those without to increase transparency and identify potential subgroups that may be underrepresented in the complete data set. Additionally, patients were only followed for 1 year postoperatively in this registry. While this may limit our findings, previous studies have shown the majority of improvement does occur within the first year after TKA.22,58,64 Last, this study was limited to our single institution with a patient population that was predominantly White, obese, and with a higher proportion of patients classified as ASA III (severe systemic disease) compared with previous studies.47,49 While it is critical to define what constitutes important change in complex patients, the estimates and results of this study may not be applicable to all patient populations.
Conclusion
The results of this study demonstrate relevant values for interpretation of the KOOS-JR and PROMIS 10, including the RCI and a range of MID values 3 and 12 months post-TKA, along with some considerations for interpretation of these thresholds. While we were unable to accurately predict achievement of the MID using patient demographics, some potential factors predicting successful patient-reported outcomes post-TKA were identified in this study.
Footnotes
Appendix
Event Data at 90 Days and Postoperative Satisfaction for the Study Cohort (N = 1315)
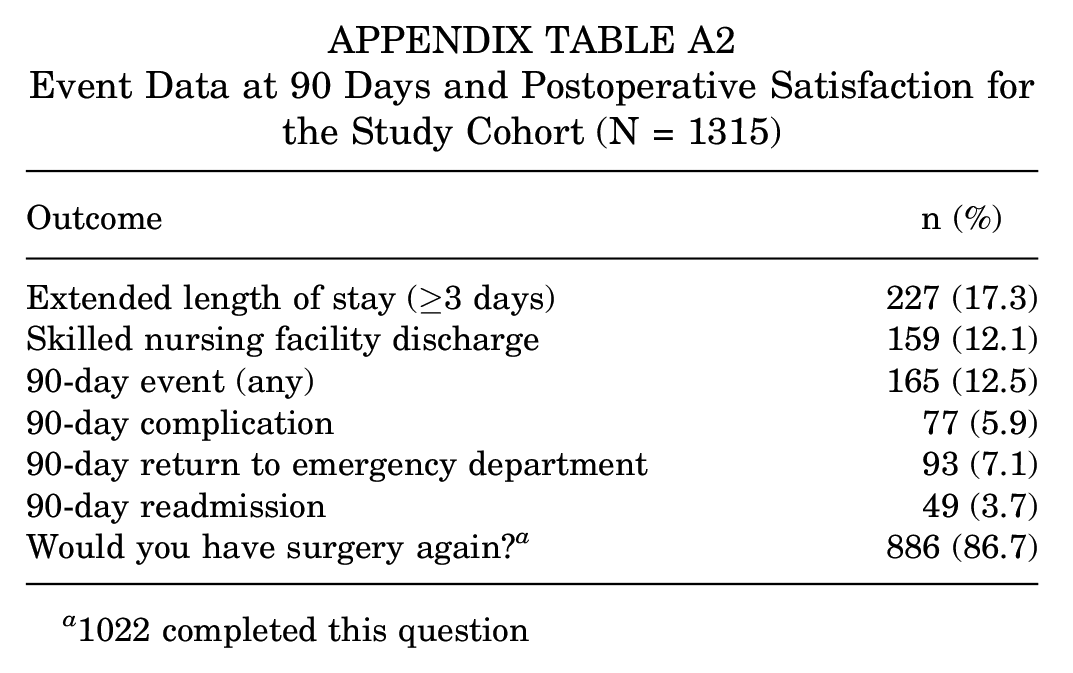
| Outcome | n (%) |
|---|---|
| Extended length of stay (≥3 days) | 227 (17.3) |
| Skilled nursing facility discharge | 159 (12.1) |
| 90-day event (any) | 165 (12.5) |
| 90-day complication | 77 (5.9) |
| 90-day return to emergency department | 93 (7.1) |
| 90-day readmission | 49 (3.7) |
| Would you have surgery again? a | 886 (86.7) |
1022 completed this question
Final revision submitted May 10, 2023; accepted June 29, 2023.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by University of Michigan (reference No. HUM00172773).