
Abstract
Keywords
Introduction
Total knee arthroplasty (TKA) relieves pain and improves the functional status and quality of life (QOL) of patients with end-stage knee osteoarthritis (OA). 1 Treatment efficacy after TKA is often assessed using patient-reported outcome measures (PROM). The Knee injury and Osteoarthritis Outcome Score (KOOS) is a reliable PROM often used in clinical practice for determining treatment efficacy in active young, middle-aged, and post-TKA patients. 2 In addition to monitoring the effects of surgical, pharmacological, and other interventions, the KOOS can be used to monitor the course of various diseases. The KOOS is particularly useful for patients with higher expectations of physical function compared to those requiring only activities of daily living (ADL) after TKA. 3 These benefits of KOOS help healthcare providers in clinical practice.
Interpreting treatment effects using minimal clinically important difference (MCID) in KOOS parameters rather than statistically significant differences supports patient-oriented medicine. The MCID is the amount of change in the rating scale at which the treatment is effective. If the change due to the treatment exceeds the MCID, a meaningful change has occurred. 4 MCID can be calculated using anchor methods or distribution-based methods. KOOS MCID calculated using distribution-based methods are lower and less valid than minimal detectable change (MDC) 80, MDC 90, and MDC 95. 5 On the other hand, KOOS MCID determined using the anchor method in patients with TKA can discriminate between improved and nonimproved patients for each KOOS subscale, and the area under the curve (AUC) of receiver operating characteristic (ROC) is high. 6
Long-term KOOS MCIDs, 1 or 2 years after TKA, have been determined,5,6 but the short-term postoperative KOOS MCIDs, 3 or 6 months after TKA, have not been established. Establishing short-term postoperative KOOS MCIDs will support early decision-making about treatment strategies. Additionally, the ability to assess a patient's degree of short-term recovery is useful for making clinical decisions about continuing treatment.
The purpose of this study was to determine short-term postoperative KOOS MCIDs with high predictive ability by subscale using the anchor method. The purpose was also to determine the MCID achievement rate by KOOS subscales.
Materials and methods
Ethics
This study followed the principles of the Declaration of Helsinki. The study was approved by the Ethics Review Board at the authors’ institutions before beginning the study. All measurements were noninvasive and necessary to assess the functional status of the subjects. Additionally, all subjects provided written informed consent before participating in the study.
Study design
In this 6-month follow-up prospective cohort study, MCIDs for KOOS subscales 3 and 6 months after TKA were determined using the anchor method.
Setting
The study was conducted in the rehabilitation department of a hospital in Japan. Patients were recruited by the staff of the physical therapy department. Recruitment, follow-up, and data collection were conducted between June 2021 and March 2023.
Participants
Patients with knee OA who underwent unilateral TKA and were able to walk independently before and after TKA with or without assistive devices were included in the study. The exclusion criteria were rheumatoid arthritis, systemic lupus erythematosus, dementia, psychiatric disorders, neurological problems (e.g., paralysis and stroke), post-TKA complications (e.g., deep vein thrombosis, fracture), and revision TKA. Patients with these conditions were excluded as the conditions can affect the evaluation of KOOS.
All subjects underwent a clinical pathway rehabilitation program after TKA. The rehabilitation program was initiated 1 day after TKA and consisted of a range of motion exercises, gait training, and progressive lower extremity resistance exercises, including hip abductor, hip extensor, knee extensor, and ankle exercises.
Variable
The KOOS consists of 42 questions regarding five subscales: Symptoms, Pain, ADL, Sport/Recreation, and QOL. 7 The primary endpoints were the KOOS MCIDs at 3 and 6 months after TKA. The KOOS questionnaire includes 7 questions for symptoms, 9 for pain, 17 for ADL, 5 for sport/recreation, and 4 for QOL. Each subscale has five response options, with 0% being the worst condition and 100% being the best condition. KOOS has been highly validated and reliable as a PROM after TKA.2,8
Statistical analysis
The MCID was calculated using the anchor method. Anchor questions were asked using global rating of change (GRC) scales,9,10 with the degree of improvement in each subscale (Symptoms, Pain, ADL, Sport/Recreation, and QOL) rated as “a great deal better,” “somewhat better,” “equal,” “somewhat worse,” or “a great deal worse.” For each subscale at 3 months after TKA and 6 months after TKA, those who selected “a great deal better,” and “somewhat better” were included in the improvement group, and those who selected “equal,” “somewhat worse,” and “a great deal worse” were included in the nonimprovement group. ROC curves were then created by the change in scores on each subscale of the KOOS preoperatively and at 3 and 6 months postoperatively (e.g., KOOS subscale scores at 3 months postoperatively–KOOS subscale scores preoperatively) and the improvement and nonimprovement groups binarized by the GRC scales. The MCIDs were calculated using the Youden index. 11 In addition, the percentage of TKA patients who achieved MCID by subscale was also calculated. All statistical analyses were performed using IBM SPSS statistics version 29 (IBM Corp., Armonk, NY, USA).
Sample size
The sample size was calculated using MedCalc statistical software version 20.110 (MedCalc Software bvba, Ostend, Belgium). Before plotting the ROC curve, the following values were set: statistical significance (p < 0.05), statistical power (0.8), and the ROC value to be included in the null hypothesis (0.5). The AUC can distinguish between nonpredictive (AUC < 0.5), less predictive (0.5 < AUC < 0.7), moderately predictive (0.7 < AUC < 0.9), highly predictive (0.9 < AUC < 1), and perfect predictive (AUC = 1). 12 An AUC of 0.7 was used as the criterion for superior statistical discrimination in a previous study. 13 For the group ratio, a value of 1 was tentatively used because no previous studies reported reliable data; the validity of the value was subsequently examined. A sample size of 62 participants, including 31 per group, was determined based on these parameters. A sample size of 62 participants, including 31 in each improvement and nonimprovement group, was determined based on these parameters.
Results
Cohort characteristics
At 3 months, 65 of the 68 patients who met the eligibility criteria were followed up. At 6 months after the start of observation, 62 were followed up and 3 were lost to follow-up (Figure 1). Baseline patient characteristics and KOOS data before and after TKA are shown in Tables 1 and 2, respectively.
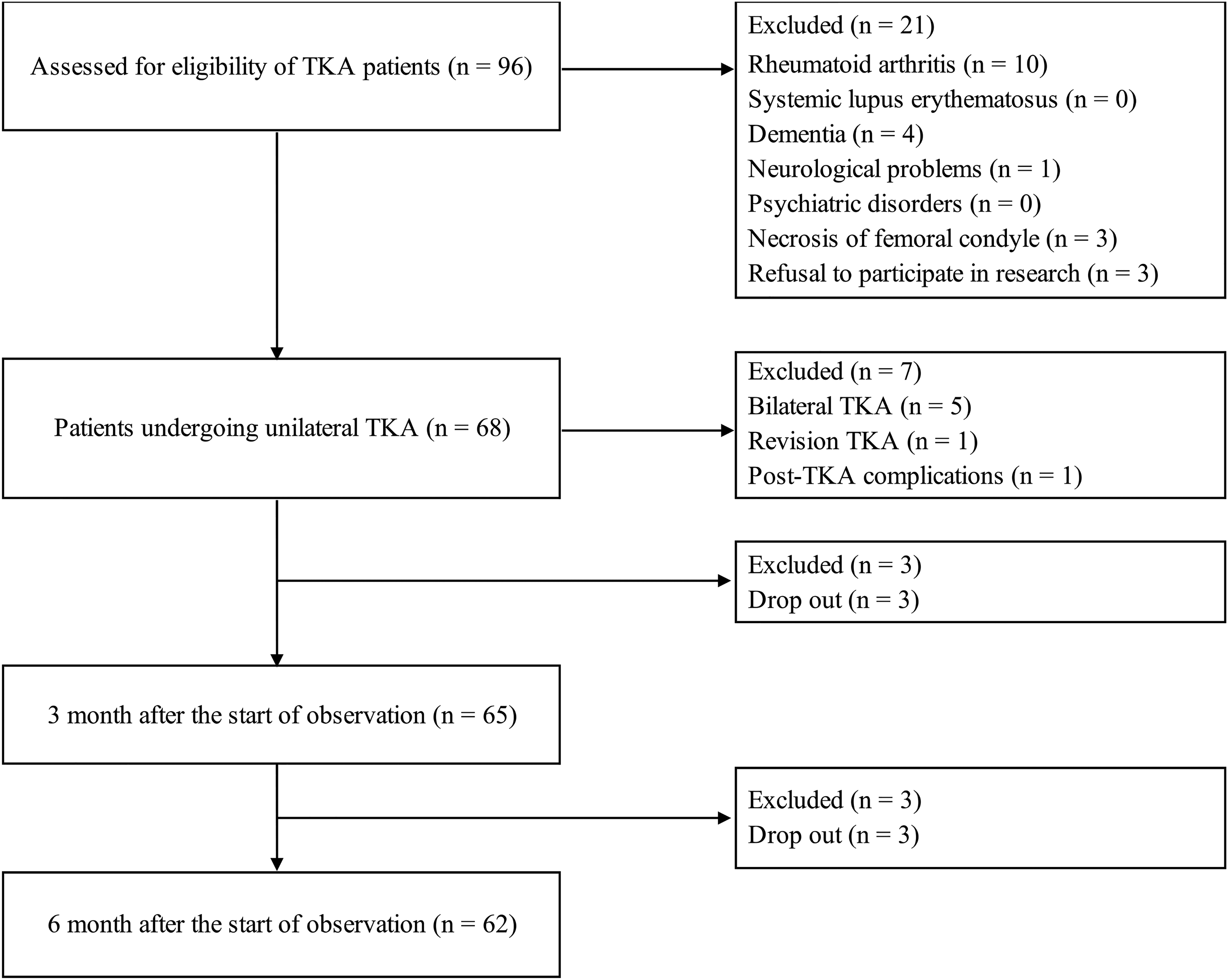
The flow diagram. TKA: total knee arthroplasty.
Patient characteristics at baseline.
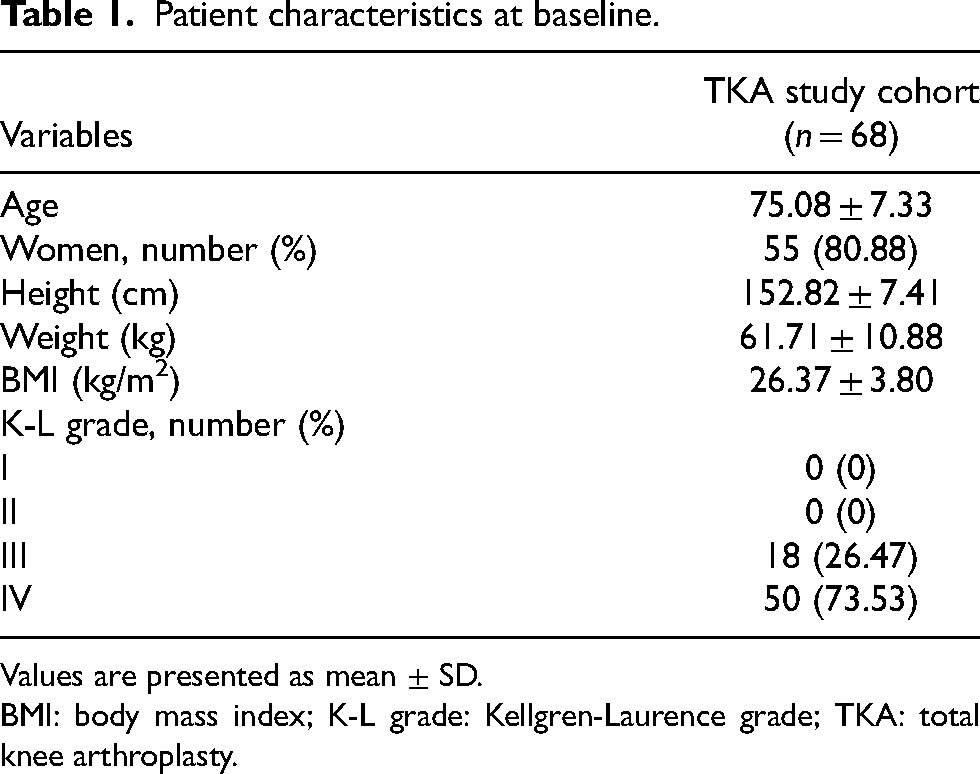
Values are presented as mean ± SD.
BMI: body mass index; K-L grade: Kellgren-Laurence grade; TKA: total knee arthroplasty.
KOOS subscale data at pre-TKA, 3 months after TKA, and 6 months after TKA.
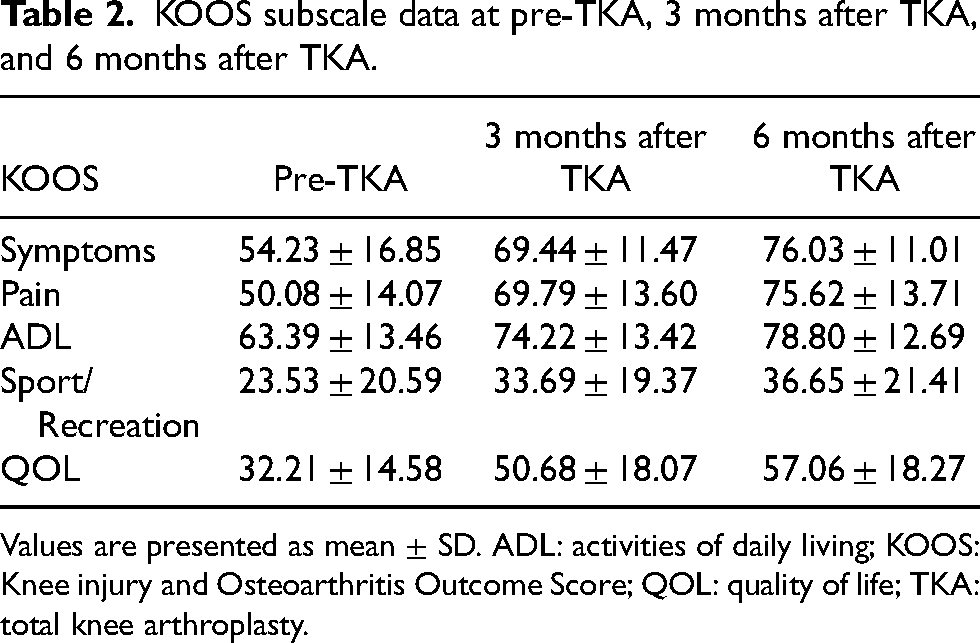
Values are presented as mean ± SD. ADL: activities of daily living; KOOS: Knee injury and Osteoarthritis Outcome Score; QOL: quality of life; TKA: total knee arthroplasty.
Minimally clinically important difference
The KOOS MCIDs at 3 months after TKA were 6 for symptoms, 10 for pain, 6 for ADL, 8 for sport/recreation, and 10 for QOL (Table 3). The KOOS MCIDs at 6 months after TKA were 9 for symptoms, 13 for pain, 10 for ADL, 9 for sport/recreation, and 16 for QOL (Table 4). The AUCs were 0.8–0.9 for both the 3 and 6 months postoperative KOOS MCIDs (Tables 3 and 4). Three months after TKA, 56.92%–78.46% of patients achieved MCIDs, and at 6 months after TKA, 64.51%–80.64% of patients achieved MCIDs (Tables 3 and 4).
MCID of the KOOS at 3 months after TKA.
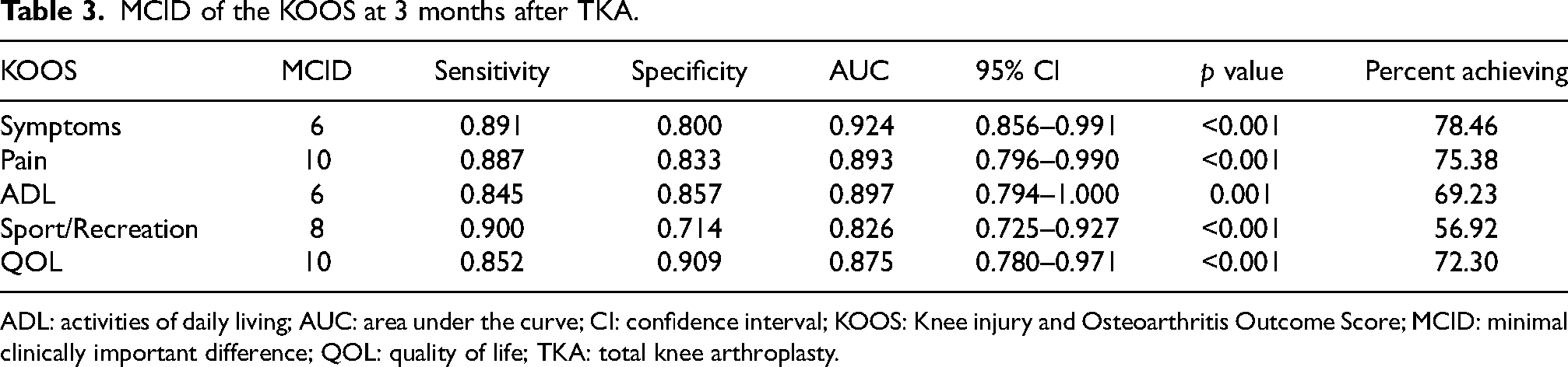
ADL: activities of daily living; AUC: area under the curve; CI: confidence interval; KOOS: Knee injury and Osteoarthritis Outcome Score; MCID: minimal clinically important difference; QOL: quality of life; TKA: total knee arthroplasty.
MCID of the KOOS at 6 months after TKA.
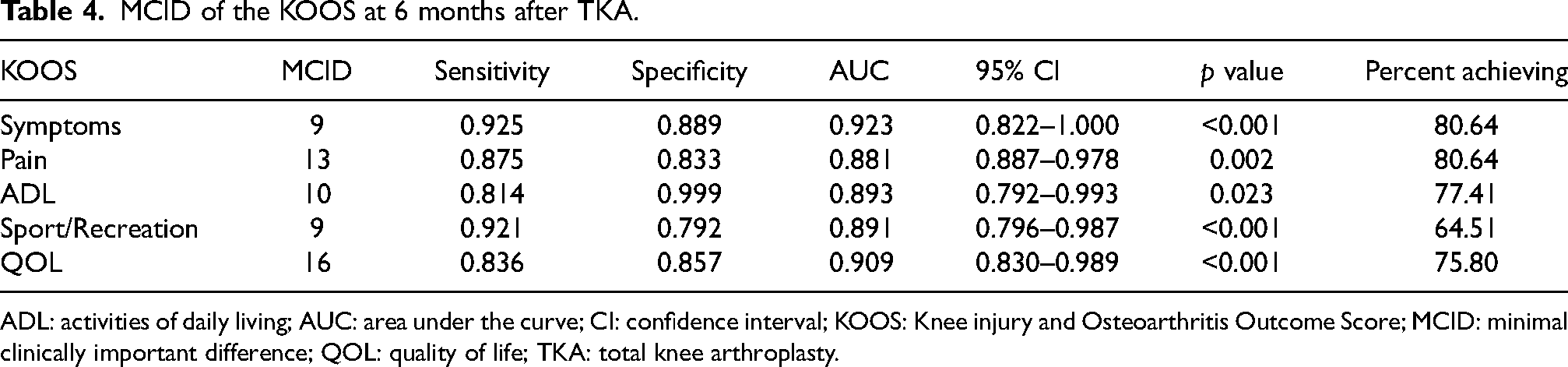
ADL: activities of daily living; AUC: area under the curve; CI: confidence interval; KOOS: Knee injury and Osteoarthritis Outcome Score; MCID: minimal clinically important difference; QOL: quality of life; TKA: total knee arthroplasty.
Discussion
The purpose of this study was to determine short-term postoperative KOOS MCIDs and its accuracy using the anchor method. This study determined KOOS MCIDs at 3 and 6 months after TKA. The AUCs were in the 0.8–0.9 range at both 3 and 6 months after TKA. At 3 months after TKA, 56.92%–78.46% of patients achieved the MCIDs, and 6 months after TKA, 64.51%–80.64% of patients achieved the MCIDs.
To the best of our knowledge, this is the first study to reveal short-term postoperative KOOS MCIDs. Previous studies focused on long-term KOOS MCIDs 1–2 years after TKA.5,6 In addition, MCIDs for each subscales were not calculated separately in previous studies focused MCID for relatively short-term KOOS, such as 3–6 months after TKA. 14 Consequently, the strength of this study is the novel short-term postoperative KOOS MCIDs and the MCIDs for each KOOS subscale in patients undergoing TKA. Using the MCIDs from this study, the effectiveness of various interventions and treatments for TKA can be determined. Additionally, the ability to clarify the effects of treatment earlier is beneficial to both clinicians and patients and significantly contributes to clinical practice.
The KOOS MCIDs determined in this study show high predictive accuracy, with AUCs ranging from 0.8 to 0.9 both 3 and 6 months after TKA. Although MCIDs generally have higher specificity than sensitivity, 15 the superiority of sensitivity and specificity in this study differed depending on the time of assessment and the subscales. In particular, the specificity of the sport/recreation was much lower than the specificity of the other subscales. The questions for the sport/recreation involve higher levels of activity, such as running and jumping, and are more valid in younger patients with knee injuries, which may contribute to the lower accuracy of this subscale relative to the other subscales. 16 Therefore, caution should be exercised in interpreting the MCID in elderly patients undergoing TKA.
For all subscales, the MCID at 6 months after TKA was higher than that at 3 months, and the achievement rate was also higher. In previous reports, more than 90% of patients scheduled for primary TKA rated improvement in symptoms, pain, ADL, and QOL as very important in their decision to undergo TKA. 2 In this study, the MCID achievement rate for symptoms, pain, ADL, and QOL at 6 months after TKA was found to increase from 75.80% to 80.64%, which may provide useful information for clinicians to demonstrate the recovery process to the patients. The MCID achievement rate for sports/recreation was 64.51% at 6 months after TKA, suggesting that patients who wish to return to sports and recreation may require additional interventions to the usual rehabilitation after TKA.
This study has several limitations. First, the timing of knee OA onset and the length of time leading up to TKA were not considered in the study. The results may not be the same for different times of end-stage knee OA diagnoses and TKA. Second, the study size was not sufficient for generalization. Although the study size was sufficient to validate the moderate predictive values, the results may not represent the entire population of patients who undergo TKA. Future studies with larger sample sizes are needed to increase the generalizability of this study. Third, this study did not adequately adjust for potential confounding factors that may affect pain and function, such as psychosocial factors. For example, anxiety, depression, or pain catastrophizing may significantly impact the KOOS results. Fourth, evaluating the use of drugs that may affect pain and ADL was not included in this study.
To conclude, KOOS MCIDs at 3 and 6 months postoperatively in patients who underwent unilateral TKA for knee OA were identified, and its accuracy was high. The results may be useful in determining the effectiveness of various interventions and treatments for patients undergoing TKA.
Footnotes
Acknowledgments
The authors thank the staff of the Graduate School of Humanities and Social Sciences at Hiroshima University for their helpful advice.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Medical Rehabilitation and Research Foundation.