
Abstract
Background:
Few studies have evaluated the clinical and radiological outcomes of medial open-wedge high tibial osteotomy (MOWHTO) in patients who had previously undergone arthroscopic meniscectomy.
Purpose:
To verify whether previous arthroscopic meniscectomy affects the clinical and radiological outcomes of MOWHTO.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 183 consecutive knees that underwent MOWHTO and had a minimum 5 years of follow-up were retrospectively reviewed. We compared the preoperative and postoperative clinical and radiological data of 32 knees with a history of meniscectomy (previous meniscectomy group) to 151 control knees without a history of meniscectomy. Cartilage status was also compared at first- and second-look arthroscopic surgery according to the International Cartilage Repair Society grading system. Failure was defined as conversion to total knee arthroplasty or revision MOWHTO. On subgroup analysis, the previous meniscectomy group was divided into 2 subgroups based on the time from meniscectomy to MOWHTO (<3 vs ≥3 years).
Results:
The mean age at the time of surgery was 55.9 years (range, 38-70 years), and the mean follow-up period was 86.2 months (range, 60-164 months). The mean time between meniscectomy and MOWHTO was 48.9 months (range, 5-156 months), and all meniscectomy procedures were performed on the medial side. Preoperative patient characteristics were similar between the study groups. Clinical and radiological outcomes were not significantly different between the groups at the latest follow-up, and no significant between-group differences were observed regarding postoperative cartilage status on arthroscopic examination. One knee in the control group underwent conversion to total knee arthroplasty at 7 years postoperatively for arthritic progression. Subgroup analysis of the previous meniscectomy group indicated no significant differences in clinical outcomes based on the time from meniscectomy to MOWHTO.
Conclusion:
Based on the results, a history of meniscectomy did not adversely affect the midterm to long-term outcomes of MOWHTO. Furthermore, the time between previous meniscectomy and MOWHTO was not associated with the clinical outcomes of MOWHTO.
Medial open-wedge high tibial osteotomy (MOWHTO) is a well-established treatment option for patients with knee osteoarthritis (OA) of the medial compartment with varus malalignment.9,23,24,27,31,40 Although satisfactory results have been reported in most patients undergoing MOWHTO, dissatisfactory results unexpectedly occur in a few patients.5,14 Various factors have been reported to be associated with inferior outcomes after MOWHTO, including advanced age, greater body mass index, lower preoperative range of motion, and high-grade OA.5,21,28-30
A history of arthroscopic meniscectomy has been rarely reported in patients with OA knees undergoing MOWHTO. Although arthroscopic meniscectomy is considered minimally invasive surgery on a native knee to reduce mechanical symptoms resulting from a torn meniscus, previous meniscectomy, especially in a varus knee, may accelerate the progression of arthritis because of increased loading on the affected knee. 32 Moreover, prior meniscectomy is thought to increase surgical difficulties and postoperative complications, such as surgical site infections or stiffness.10,36 Despite such concerns, whether a history of arthroscopic meniscectomy affects the results of MOWHTO has been rarely reported.
In this regard, the current study aimed to verify whether previous arthroscopic meniscectomy affects the clinical and radiological outcomes of MOWHTO. We compared the midterm to long-term outcomes of MOWHTO in patients who had undergone arthroscopic meniscectomy and those who had not. It was hypothesized that previous arthroscopic meniscectomy would not affect the clinical and radiological outcomes of MOWHTO because MOWHTO would be effective in reducing medial contact pressure by shifting the weightbearing axis to the lateral compartment, regardless of the condition of the medial meniscus.
Methods
Patients
The study protocol was approved by our institutional review board, which waived the requirement for informed consent from patients owing to the retrospective nature of the study. Between February 2008 and August 2017, a total of 222 knees underwent MOWHTO for medial compartment OA of the knee at our institution. Inclusion criteria for this study were patients with symptomatic medial compartment OA (Kellgren-Lawrence [K-L] grades 1-4) with varus malalignment necessitating correction (>5°) and a minimum 5-year follow-up. Exclusion criteria were as follows: (1) secondary OA, such as hemophilic arthropathy, rheumatoid arthritis, osteonecrosis, and posttraumatic OA and (2) cases without second-look arthroscopic surgery after MOWHTO. Ultimately, 183 knees were included in the study (Figure 1). To investigate whether previous arthroscopic meniscectomy affects the outcomes of MOWHTO, we divided the cohort and compared 32 knees (17.5%) that had undergone arthroscopic meniscectomy before MOWHTO (previous meniscectomy group) and 151 knees that underwent MOWHTO without a history of meniscectomy (control group).

Flow diagram showing enrollment process. MOWHTO, medial open-wedge high tibial osteotomy; OA, osteoarthritis.
Surgical Procedure and Postoperative Management
All operative procedures were performed by a single senior surgeon (K.-I.K.) using the same technique.17,18 No cartilage restoration or meniscal repair was conducted with MOWHTO. After arthroscopic examination and debridement, osteotomy was performed with a superomedial incision of the tibia. Through preoperative planning, the osteotomy gap was set, such that the weightbearing line passed through or slightly below the Fujisawa point according to the arthroscopic cartilage status, 9 and a medial locking compression plate (TomoFix; Synthes) was placed after biplanar osteotomy.11,13,25,35,39 On the day of surgery, the patients were encouraged to perform isometric quadriceps and active ankle exercises. Range of motion exercises in the sitting position and partial weightbearing ambulation with crutches were permitted from the day after surgery. Patients were allowed full weightbearing ambulation at 6 weeks postoperatively. Plate removal and second-look arthroscopic surgery were performed at 2 years after surgery if patients consented.
Evaluations
All included patients underwent preoperative radiological and clinical evaluations. Postoperatively, patients underwent annual follow-up evaluations. For the radiological evaluation, standing anteroposterior and lateral radiographs of the knee as well as lower extremity arthrograms were assessed preoperatively and at 6 weeks, 3 months, 6 months, and 1 year postoperatively. Thereafter, follow-up was conducted annually until the latest follow-up. The radiological evaluation assessed the K-L grade, 22 hip-knee-ankle angle (negative values indicated varus alignment), 6 medial proximal tibial angle, 4 and correction angle.
The clinical evaluation included the American Knee Society score, 12 the Western Ontario and McMaster Universities Osteoarthritis Index, 3 and the Knee injury and Osteoarthritis Outcome Score (KOOS) 34 preoperatively and at the latest follow-up. Failure was defined as conversion to total knee arthroplasty (TKA) or revision MOWHTO. Radiological and clinical data were compared between the 2 groups.
For the arthroscopic evaluation, the cartilage status of the medial femoral condyle and medial tibial plateau were compared using 2-stage arthroscopic surgery that was performed at the time of MOWHTO and at plate removal. The International Cartilage Repair Society (ICRS) grading system was used to assess cartilage status. 26 The second-look arthroscopic findings were compared with the first-look arthroscopic findings, and the change in cartilage status was defined as “progressed” if there was progressive change in cartilage of the medial femoral condyle or medial tibial plateau or “not progressed” if there was no progression.16,19
Subgroup Analysis of Previous Meniscectomy Group
In the 32 knees in the previous meniscectomy group, the tear location and extent of meniscectomy were assessed. In addition, subgroup analysis was performed to determine whether the time between meniscectomy and MOWHTO was associated with midterm to long-term outcomes after MOWHTO, with a criterion of 3 years. 15 The knees were divided into 2 subgroups based on the time from meniscectomy to MOWHTO: <3 years (n = 12) or ≥3 years (n = 20). Additional subgroup analysis was performed of clinical outcomes based on the extent of meniscectomy: partial (n = 25) or subtotal (n = 7).
Statistical Analysis
Statistical analysis was performed using SPSS software (Version 23; IBM), and continuous data were expressed as means with standard deviations. All dependent variables were examined for the normality of distribution and equality of variance using the Kolmogorov-Smirnov test and were analyzed using nonparametric tests if they showed a nonnormal distribution. The Student t test was used to compare continuous outcomes between the groups. Categorical data between groups were evaluated using the chi-square test or Fisher exact test. Statistical significance was set at P < .05.
To improve the reliability of the grading system, 2 independent board-certified orthopaedic surgeons (D.K. and J.-H.K.) measured all radiological and arthroscopic variables. The measurements were repeated 2 weeks later, and intraobserver and interobserver reliabilities were determined. The intraclass correlation coefficients ranged from 0.87 to 0.95 for intraobserver reliability and from 0.89 to 0.97 for interobserver reliability, indicating excellent agreement between the measurements.
Results
The mean age of the study patients at the time of surgery was 55.9 years (range, 38-70 years), and the mean follow-up period was 86.2 months (range, 60-164 months). All 32 knees in the previous meniscectomy group underwent medial meniscectomy (Table 1). The mean time between previous meniscectomy and MOWHTO was 48.9 months (range, 5-156 months).
Characteristics of Previous Meniscectomy Group (n = 32) a

MOWHTO, medial open-wedge high tibial osteotomy.
Radiological Outcomes
Most preoperative demographic data were not significantly different between the 2 groups. Moreover, the radiological outcomes at the latest follow-up were not significantly different between the groups (Table 2).
Patient Characteristics and Radiological Outcomes of Previous Meniscectomy and Control Groups a

Data are presented as No. of knees or mean ± SD. K-L, Kellgren-Lawrence.
Negative values indicate varus alignment.
Clinical Outcomes
Preoperatively, most clinical outcomes, with the exception of the KOOS Symptoms subscore, were similar between the previous meniscectomy and control groups. None of the postoperative clinical outcomes were significantly different between the groups (Table 3).
Clinical Outcomes of Previous Meniscectomy and Control Groups a

Data are presented as mean ± SD. Boldface value indicates a statistically significant difference between groups (P < .05). KOOS, Knee injury and Osteoarthritis Outcome Score; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Arthroscopic Outcomes
There were no significant differences in preoperative ICRS grades of the medial compartment between the 2 groups. Moreover, postoperative ICRS grades of the medial compartment, as well as the change in the ICRS grade from first- to second-look arthroscopic surgery, were not significantly different between the 2 groups (Table 4).
Arthroscopic Outcomes of Previous Meniscectomy and Control Groups a

Data are presented as No. of knees or n (%). ICRS, International Cartilage Repair Society.
Subgroup Analysis
On subgroup analysis of the previous meniscectomy group, most of the preoperative and all of the postoperative clinical outcomes were not significantly different between the subgroups (Table 5). Furthermore, there was no significant difference in preoperative and postoperative clinical outcomes based on the extent of meniscectomy.
Clinical Outcomes of Previous Meniscectomy Group With Respect to Time to MOWHTO a
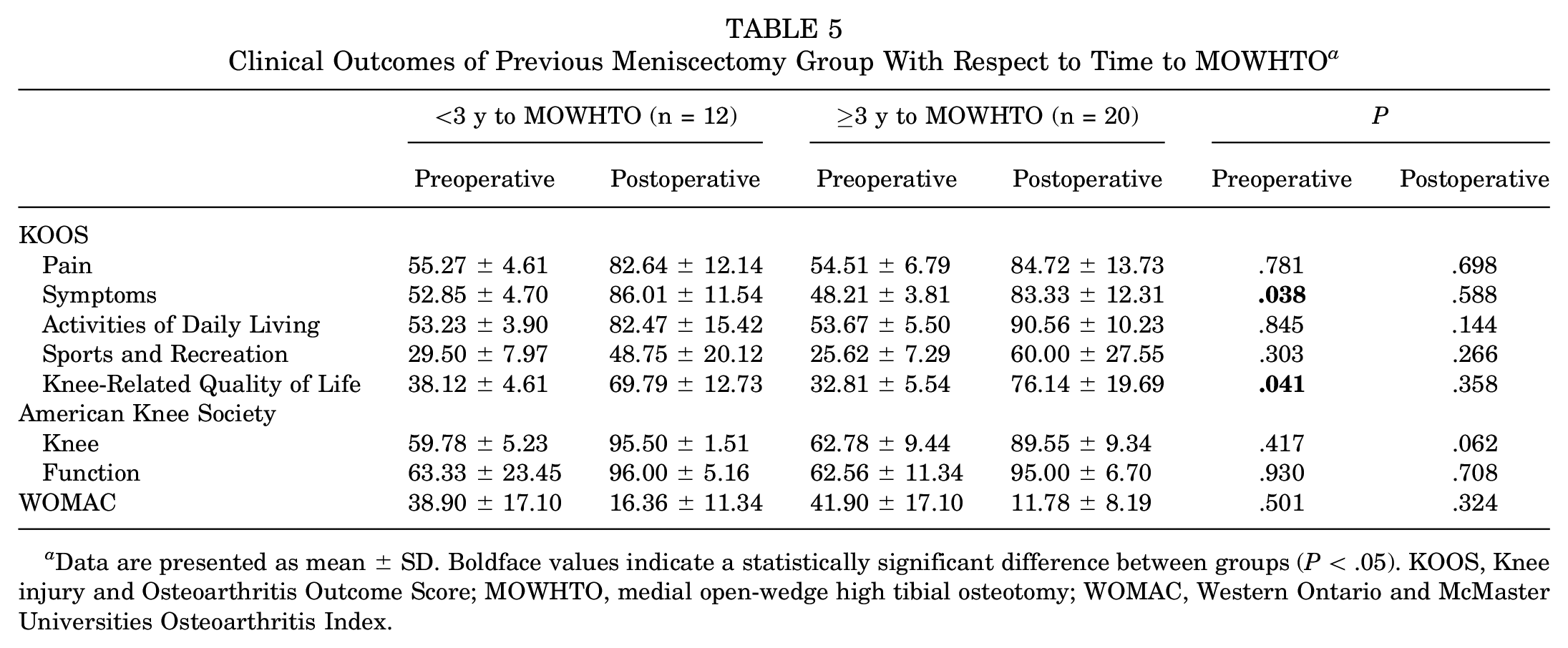
Data are presented as mean ± SD. Boldface values indicate a statistically significant difference between groups (P < .05). KOOS, Knee injury and Osteoarthritis Outcome Score; MOWHTO, medial open-wedge high tibial osteotomy; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Failure was found in only 1 knee in the control group. The patient underwent conversion to TKA at 7 years postoperatively for arthritic progression.
Discussion
The main finding of this study was that radiological and clinical outcomes were not significantly different at midterm to long-term follow-up, regardless of whether the patients had previously undergone arthroscopic meniscectomy. Subgroup analysis indicated that the time between meniscectomy and MOWHTO (<3 vs ≥3 years) did not affect clinical outcomes.
The findings of this study indicated that among 183 consecutive knees, 17.5% underwent arthroscopic meniscectomy before MOWHTO, which is consistent with previous studies.15,38 Spahn et al 38 reported that 7.4% of 94 patients undergoing MOWHTO had undergone previous arthroscopic meniscectomy. Khoshbin et al 15 reported that 20% of patients underwent arthroscopic meniscectomy within 3 years before MOWHTO. As the meniscus in a knee with OA would be easily torn and be symptomatic, a history of arthroscopic meniscectomy has been occasionally observed in patients undergoing MOWHTO.
Generally, previous surgery of the affected knee is associated with surgical difficulties and postoperative complications. 33 Although arthroscopic meniscectomy is considered minimally invasive surgery, postoperative complications, such as infections, hemarthrosis, or stiffness, can occur after surgery.10,36 Moreover, although medial meniscectomy reduces mechanical symptoms resulting from a torn meniscus, previous meniscectomy, especially in a varus knee, may accelerate arthritic progression because of increased loading on the meniscectomized knee. 32 In this regard, the current study showed that the preoperative K-L grade in the previous meniscectomy group was higher than that in the control group, although it was not statistically significant (P = .051). However, there is a lack of information regarding the influence of previous medial meniscectomy on the outcomes of MOWHTO. Khoshbin et al 15 reported that a history of meniscectomy within 3 years increased the risk of conversion to TKA after MOWHTO. It was shown that patients who undergo arthroscopic meniscectomy are more likely to have an increased risk of arthritic progression because of the degree of meniscal loss, especially in varus knees.2,7 In contrast, Spahn et al 38 reported that prior arthroscopic meniscectomy did not influence outcomes after MOWHTO at a mean follow-up of 45.9 months. As controversy remains whether previous arthroscopic meniscectomy affects clinical and radiological outcomes after MOWHTO, the current study focused on this issue and demonstrated that patients with or without a history of arthroscopic meniscectomy before MOWHTO had similar radiological and clinical outcomes as well as similar failure rates at midterm to long-term follow-up.
On subgroup analysis of the previous meniscectomy group in the current study, preoperative KOOS Symptoms and Knee-Related Quality of Life subscores were significantly worse in the subgroup with a time to MOWHTO of ≥3 years versus <3, although none of the clinical outcomes were significantly different. These findings indicate that a recent history of arthroscopic meniscectomy of the ipsilateral knee did not have a significant influence on outcomes after MOWHTO. This could be explained by the significant effectiveness of MOWHTO in reducing medial contact pressure by shifting the weightbearing axis to the lateral compartment, regardless of the condition of the medial meniscus,1,8 thus improving the mechanical symptoms of OA in a varus knee. 23 As we hypothesized, previous arthroscopic meniscectomy did not affect the midterm to long-term clinical outcomes of MOWHTO. Moreover, the time from previous medial meniscectomy to MOWHTO did not influence the outcomes of MOWHTO.
Limitations
Our study has some limitations. First, it has a retrospective design. However, all the procedures in this study were performed by a single senior surgeon and were followed by consistent rehabilitation protocols. Moreover, to minimize the risk of bias, 2 independent investigators performed radiological and arthroscopic evaluations. Second, a predominance of female sex was observed in our patients. It may be difficult to generalize the results of this study to the entire population. This predominance occurred because Asian women have a higher rate of high tibial osteotomy than women in Western populations.20,37 Further research would be interesting for a comparison with Western or male-predominant cohorts. Third, there was a substantial difference in the number of knees between the 2 groups; however, this seemed inevitable, considering the incidence of arthroscopic meniscectomy before MOWHTO.15,38 Fourth, although we retrospectively reviewed all consecutive knees that underwent MOWHTO, there was no patient with a history of lateral meniscectomy; this could be explained by the fact that patients who undergo MOWHTO have a degenerative abnormality of the medial compartment of the knee joint. This limitation should be noted before extrapolating our results to patients with a history of lateral meniscectomy. Lastly, although we tried to contact all of the patients who underwent MOWHTO, 27 patients (12.2%) were not included in the current study because of a loss to follow-up. Failure might have occurred in these 27 patients, who were not able to be contacted by telephone.
Conclusion
Based on the study results, a history of meniscectomy did not adversely affect the midterm to long-term outcomes of MOWHTO. Furthermore, the time between previous meniscectomy and MOWHTO was not associated with the clinical outcomes of MOWHTO.
Footnotes
Final revision submitted May 31, 2023; accepted June 19, 2023.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Kyung Hee University Hospital at Gangdong (No. KHNMC 2022-09-052).