
Abstract
Purpose:
To examine the results of medial open-wedge high tibial osteotomy (MOWHTO) combined with all-inside repair focusing on medial meniscus posterior root tears (MMPRT) by second-look arthroscopy and determine the clinical relevance of the findings.
Methods:
From June 2015 to June 2017, 27 consecutive patients underwent MOWHTO and meniscal treatment for MMPRT using all-inside repair. All were available for second-look arthroscopy evaluation at the time of plate removal. Cartilage regeneration in the medial condyles and healing status of the MMPRT were assessed at the time of second-look arthroscopy. Clinical outcomes were evaluated by the Hospital for Special Surgery (HSS) scores and the Lysholm score scale. The potential factors affecting the healing of MMPRT, including age, body mass index (BMI), weight-bearing line rate (WBLR) and femorotibial angle (FTA) were discussed.
Results:
There were 11 (41%) cases with complete healing (group A) and 16 (59%) cases with lax healing (group B). A complete cartilage coverage of chondral lesions was observed at second-look arthroscopy. Improvements of HSS in both groups were 41.25 ± 6.18 and 38.82 ± 5.43, while improvements in Lysholm score seen in both groups were 30.40 ± 4.84 and 32.65 ± 4.11. There was no significant difference in the postoperative clinical results between the two groups. In group A, the age (months), BMI, WBLR, and FTA are 54.61 ± 2.53, 23.58 ± 2.39, 66.10 ± 2.86% and 169.00 ± 2.62°, respectively, while in group B, they are 55.16 ± 4.92, 29.58 ± 3.91, 57.51 ± 5.49% and 175.21 ± 2.87°, respectively. A significant difference has been identified between two groups except for age.
Conclusion:
As seen in this retrospective study, a higher healing rate of MMPRT using all-inside repair and regeneration of degenerated articular cartilage in the medial condyles after MOWHTO can be expected. Healing of the MMPRT was not related to a better clinical outcome. Moreover, it can be inferred that BMI, WBLR and FTA may affect the healing status of MMPRT.
Keywords
Introduction
Medial meniscus posterior root tears (MMPRT), which are defined as radial tears within 9–10 mm from the posterior root attachment of the medial meniscus, 1 lead to extrusion of the meniscus during weight-bearing as well as loss of the load-sharing ability of meniscus, which results in osteoarthritis. 2 There are several therapies to manage MMPRT, 1 mainly including non-operative treatment and surgical treatment. Non-operative treatment of MMPRT is associated with poor clinical outcome, worsening arthritis and a relatively high rate of arthroplasty at a 5-year follow-up study, 3 especially for MMPRT patients with large meniscus extrusion. 4 The latter involves partial meniscectomy 5 or meniscal repair by a variety of techniques, such as suture anchors 1 and pullout sutures 6 in order to restore hoop tension. MMPRTs are noticed while performing valgus-producing open-wedge high tibial osteotomy (HTO) frequently. As Hwang et al. 7 put it, the mechanical axis angle may contribute to the development of MMPRT. In the varus knee, medial open-wedge high tibial osteotomy (MOWHTO), which is used to produce valgus realignment of the proximal tibial articular surface, could off-load the medial compartment in cases of varus tibiofemoral deformity. By such means, a high rate of healing of MMPRT without attempted repair was obtained. 8 On a different note, Lee et al. 9 showed that MMPRT had a lower rate of healing potency without suture in the context of HTO. This suggests that the repair of MMPRT in the varus knee is still a subject of controversy. It is assumed that, with all-inside repair, higher healing rates of MMPRT would emerge together with MOWHTO and regeneration of degenerated articular cartilage in the medial compartment can be expected. The objective of this study is to determine the structural integrity of MMPRT after MOWHTO combines with the all-inside repair and the cartilage coverage of chondral lesions in the medial condyles by a second look of arthroscopy and to evaluate the clinical relevance of these findings.
Patients and methods
Patients
From June 2015 to June 2017, a total of 27 patients (15 female and 12 male with an average age of 55.43 ± 6.71 years, ranging from 47 to 68) underwent MOWHTO in a combination with suturing of MMPRT, using all-inside repair procedure at our institution. All enrolled in this retrospective study met the following inclusion criteria: medial knee pain, osteoarthritis grades 2–4 of the medial compartment on radiological assessment according to Kellgren and Lawrence, malalignment with more than 4° of varus angulation between the tibial and femoral mechanical axis measured on a hip-to-ankle standing anterior–posterior radiograph, and MMPRT, grade 3 or 4 of articular cartilage defects in the medial compartment as confirmed during arthroscopy according to the recommendations from International Cartilage Research Society. Complex root tears were considered irreparable and root tears with definitive medial meniscus degeneration were excluded because the severe degeneration of the meniscus was not thought to be strong enough to withstand the tension created by the sutures. Second-look arthroscopy was then performed during metal removal for fixation. The average follow-up period was 18 months (ranging from months 11 to 24 months). Healing status was categorized into four types, namely complete healing, lax healing, scar tissue healing and failed healing described according to Seo et al. 10 . Complete healing is defined as meniscal continuity with no cleft, no lifting on probing and normal meniscal tension at the repair site. Lax healing is reflected by an apparent increase in meniscus lifting and mobility on probing with good meniscal continuity. Scar tissue healing means a meniscus that can be easily raised on probing and shows no true meniscal continuity except for some connecting scar tissue fibres between the tibial attachment site and the posterior horn of the medial meniscus. Failed healing refers to no continuity and no evidence of meniscal healing at the repair site. Three senior doctors witnessed the healing status for classification and all patients enrolled in this study gave their informed consent. In addition, the study protocol was approved by the competent research ethics board.
Surgical technique
Prior to every valgus HTO, arthroscopy of the knee was conducted. The patient was in a supine position on the operating table and the leg placed in an inflated tourniquet (300 mm Hg). Standard anterolateral and anteromedial arthroscopic portals were created. The femoral condyle, tibial plateau and posterior medial meniscus root attachments were evaluated, in the case that a meniscus tear was identified, as the root tear type was defined by Laprade et al. 11 Then, the MMPRT was sutured through the FasT-Fix device (Smith & Nephew Endoscopy, Andover, Massachusetts, USA) by a method of crossing horizontal mattress tightly, which were lateral and medial to the tear. A chondral resurfacing (CR) procedure, such as microfracture or abrasion, was not applied in the process. However, a debridement of the cartilage lesion was performed in order to obtain a stable edge of healthy cartilage around the cuts of some patients.
Subsequent to intra-articular procedures, a MOWHTO in a biplanar fashion was performed. 12 The mechanical axis was positioned at a point 50–75% lateral on the transverse mediolateral diameter of the tibial plateau, aiming at a slight overcorrection of varus malalignment 13 (Figure 1). The TomoFix instrumentation system (Synthes, Oberdorf, Switzerland) was used for fixation in all cases (Figure 2). The surface of the medial collateral ligament was released distally by periosteal elevator, while the upper border of the pes anserinus marked the starting point of the osteotomy. Two K-wires adjacent to the tibiofibular joint were placed to mark the saw cut. The lateral 10 mm of the tibial head was left intact as a hinge for the osteotomy. Another separate ascending cut of the biplanar osteotomy was made 1.5 cm behind the tibial tuberosity in the frontal plane at an angle of 100–110° to the first osteotomy plane. In the whole operation, several chisels were used to gradually open the osteotomy, and a laminar spreader used for the final opening. The TomoFix plate was inserted into a subcutaneous tunnel on the medial side of the tibia and fixed in a place with eight locking screws. No bone graft or bone substitute was placed into the osteotomy site.
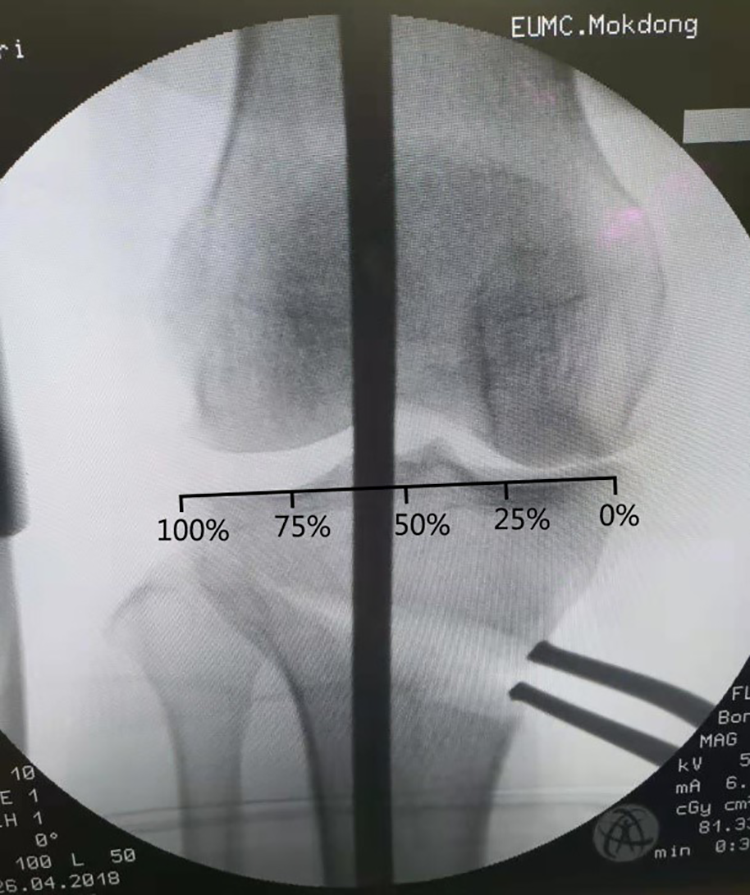
The weight-bearing line was defined as a line drawn from the centre of the femoral head to the centre of the superior articular surface of the talus. The WBLR was defined as the tibial insertion of the weight-bearing line/tibial width, with the medial tibial edge at 0% and the lateral tibial edge at 100%. WBLR: weight-bearing line rate.
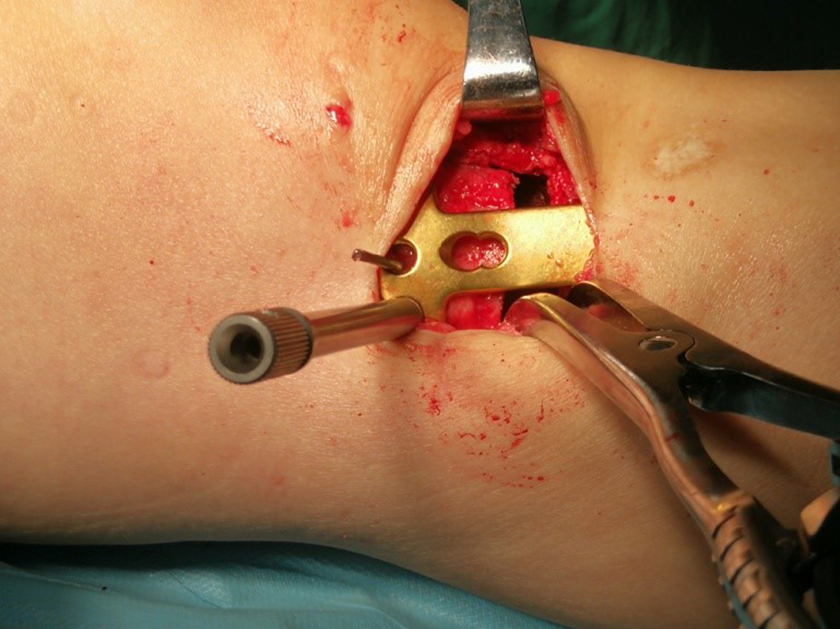
Intraoperative photos of osteotomy procedure. The TomoFix instrumentation system was used for fixation in all cases.
Postoperative rehabilitation
On the first day after the operation, all patients were instructed to exercise isometric quadriceps, ankle pump and straight-leg raises as much as possible. The range of motion exercises was gradually initiated to increase the knee flexion angle by 15–30 per week to achieve deep flexion within 8 weeks. Non-weight-bearing with the use of crutches and a knee brace locked in extension was required for 4 weeks postoperatively. Then patients were allowed to start the partial weight-bearing exercise. Full weight bearing was allowed 6 weeks after surgery. More importantly, all patients were instructed to wear a knee brace for 6 weeks postoperatively.
Statistical analysis
The comparison of preoperative results and final recovery for all patients were determined using paired tests. Variables compared between the two groups included age, Body Mass Index (BMI), improvement in the Hospital for Special Surgery (HSS) and the Lysholm scores, weight-bearing line rate (WBLR) and femorotibial angle (FTA) on the basis of independent sampling test. In the analysis process, the average data of these measurements were used. This study used SPSS (version 24, SPSS Inc, Chicago, Illinois, USA) software package to carry out the statistical analysis and all reported p values are two-tailed and the statistical significance level was set at a p value below 0.05.
Results
All patients were confirmed to have MMPRT at the HTO procedure. The average FTA and WBLR of all patients were improved to an average of 173.29 ± 3.01°, 60.57 ± 6.16° postoperatively compared with 182 ± 2.5%, 30.1 ± 13.2% preoperatively, indicating that the knee alignment had moved towards the lateral compartment of the knee. After 6 weeks of surgery, all patients had a smooth transition to the full weight-bearing. At the second-look arthroscopy, 11 (41%) patients showed complete healing (group A) and 16 (59%) lax healing (group B). There was no case with scar tissue healing or failed healing. As presented in Table 1, significant differences were observed between group A and group B in terms of BMI, WBLR and FTA. No obvious differences were identified in terms of age and the last follow-up.
Background factors of the patients (mean ± SD).

Group A: the complete healing group; group B: the lax healing group; BMI: body mass index; WBLR: weight-bearing line rate; FTA: femorotibial angle; F/U period: the last follow-up period.
a Compared group A with group B.
b Measurement results at the last follow-up.
In terms of clinical assessment, the medial pain in the knee joints has been relieved in all cases postoperatively. Table 2 shows the comparison between preoperative symptoms and postoperative results in each group. In all cases, HSS and lysholm score (LKS) increased significantly at the final follow-up (p < 0.001). But no significant differences were captured between group A and group B in terms of the improvement in HSS and LKS at the final follow-up.
Comparisons of the clinical results preoperative and postoperative statuses of the patients.

IHSS, ILKS: improvement in HSS and LKS compared between preoperation and postoperation; ILKS: I-Lysholm score; HSS: Hospital for Special Surgery; LKS: lysholm score.
All patients showed complete cartilage coverage in the medial condyles at the time of second-look arthroscopy (Figures 3 and 4).
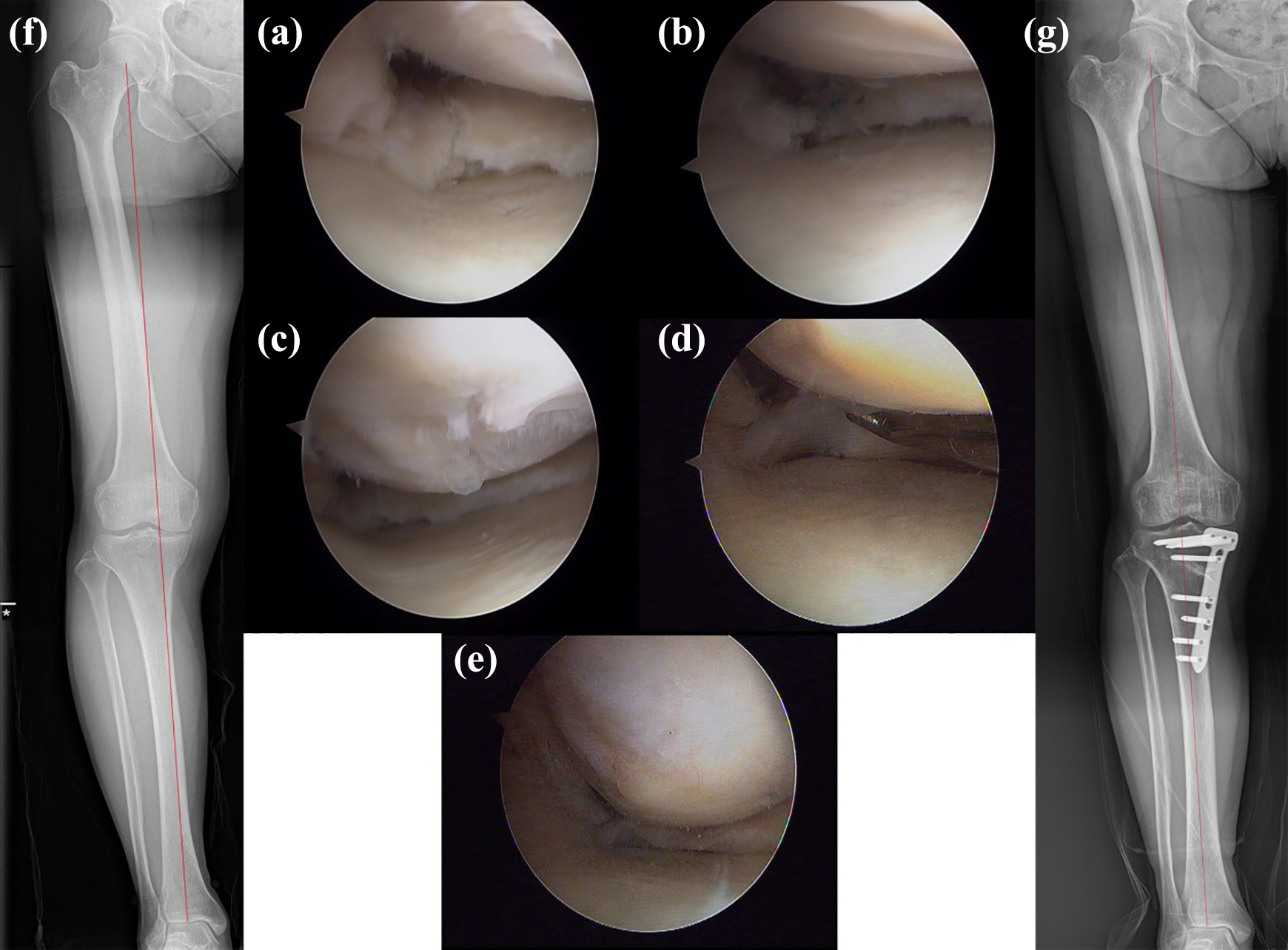
A case of a 53-year-old woman suffering from medial knee pain. (a) Arthroscopic view of posterior root tear of the medial meniscus. (b) Suture the MMPRT using the FasT-Fix device. (c) Grade 3 of articular cartilage defects in the medial compartment. (d) Second-look arthroscopic findings of lax healing of MMPRT. (e) Second-look arthroscopic findings of complete cartilage coverage in the medial condyle. (f) Anteroposterior standing radiogram of the knee prior to surgery. (g) Anteroposterior standing radiogram of the knee at the last follow-up. MMPRT: medial meniscus posterior root tears.

A case of a 55-year-old man suffering from medial knee pain. (a) Arthroscopic view of posterior root tear of the medial meniscus. (b) Suture the MMPRT using the FasT-Fix device. (c) Grade 4 of articular cartilage defects in the medial compartment. (d) Second-look arthroscopic findings of complete healing of MMPRT. (e) Second-look arthroscopic findings of complete cartilage coverage in the medial condyle. (f) Anteroposterior standing radiogram of the knee prior to surgery. (g) Anteroposterior standing radiogram of the knee at the last follow-up. MMPRT: medial meniscus posterior root tears.
Discussion
The major findings of this study are promising results can be achieved through MMPRT repair using all-inside technique and subjective scores, combined with HTO in medial osteoarthritis and varus malalignment follow-up for medial 18 months. With regard to prognostic factors, the BMI and the alignment after surgery should be considered.
Recently, MMPRT has aroused people’s interest. 14,15 The posterior horn of the medial meniscus endures most of the stress applied to the medial compartment. 14 Meanwhile, this region has very limited mobility because of its strong attachment to the tibia at the meniscal root. Hence, the medial meniscus posterior horn is particularly vulnerable to injury, especially microinjury. Due to the loss of hoop tension in knees, the MMPRT increase the tibiofemoral contact pressure significantly, which can lead to degeneration and degenerative osteoarthritis. 16
The risk for MMPRT was severe varus deformity to the lower extremity. Hwang et al. 7 identified the risk factors for MMPRT, demonstrating that the most potent risks associated with MMPRT are sex, BMI and mechanical axis angle. In his study, multiple logistic regression analysis showed that females had 5.9 times of MMPRT increase, a varus mechanical axis angle with a 3.3 times increase and a BMI of more than 30 kg/m2 with a 4.9 times increase. MMPRT is definitely connected to extrusion of the meniscus, 1 and eventually associated with further varus misaligned knee. This sets up a vicious circle leading to the degeneration of the medial compartment and the progression of medial compartment osteoarthritis. 17 Thus, HTO may be a viable option for selecting patients with MMPRTs, especially in the varus knee cases.
A few studies referred to the healing of MMPRT after HTO. Nha et al. 8 retrospectively reported on 20 patients who have been through concurrent HTO and debridement of the MMPRT without attempted repair. Ten patients (50%) showed complete healing, 6 (30%) incomplete healing and 4 (20%) no healing at an average 28 months follow-up period. Progression of chondral lesions was not observed at second-look arthroscopy while Kellgren–Lawrence (K–L) grade did not improve at all. The median Lysholm score and the median HSS improved from 58 to 88.5 and from 62.4 to 87.2, respectively, at the last follow-up. Recently, Lee et al. 9 initiated a similar study but in his study, MMPRT had a lower rate of healing potency in terms of HTO without the suturing of MMPRT. None meniscus had completely healed, together with 5 lax healings, 6 scar tissue healings and 13 failed healings. Even so, as presented by Nha et al., 8 cartilage regeneration in different degrees of chondral lesions was observed in some patients. A similar result was observed for the Lysholm score and the HSS score, which improved from 34.7 preoperatively to 77.1 and from 36.5 to 82.4, respectively at the last follow-up. Jung et al. 18 noted the repair of MMPRT with pull-out suture technique in the cases of medial tibiofemoral joint osteoarthritis performing HTO in 2009; however, the follow-up results have not been provided so far. Our findings confirmed previous researches, indicating the healing of MMPRT after HTO. More importantly, the findings in this research make such study goes further. So far it can be seen that a combination of meniscal repair and HTO may provide better results than HTO alone. However, selection differences may affect the results, as mentioned above that severe degeneration of the meniscus was excluded in our study.
Though the best repair methods with respect to MMPRT remain controversial, both pull-out 19 and all-inside techniques 20 have shown to provide functional and clinical benefits. Since its introduction introduced by Y.M. Kim in 2006, repairing MMPRT with the pull-out method has been well-accepted by the industry. 17 In addition, as one of the most commonly and commercially available all-inside meniscal repair devices, FasT-Fix is comparable to the classic vertical mattress repair technique. 21 In the FasT-Fix system, a side-to-side repair can be carried out by tightening the cleft. There has been no study assessing the clinical and radiographic results after repair of a radial tear in the posterior horn of the medial meniscus in the context of HTO. However, clinical results were satisfactory after meniscal repair of a radial tear in the MMPRT by using the FasT-Fix system. 20 In current studies, it was shown that the repair with FasT-Fix was an effective procedure combined with HTO with the premise of good quality of MMPRT.
With respect to the cartilage regeneration, more and more scholars tend to advocate the degenerated cartilage of the medial compartment could be regenerated by HTO. 22,23,24 However, there have been debates on the role of the CR procedure. Jung et al. 25 found cartilage regeneration in 95% of cases after opening-wedge HTO without cartilage regeneration strategies, when the mechanical tibiofemoral angle ranged from 0 to 6. Kim et al. 23 suggested that the open-wedge HTO should be highly successful in terms of cartilage regeneration without cartilage addressing procedures, especially for lower BMI patients. In Schuster et al.’s study, combined with CR procedure and HTO, a complete cartilage coverage was found in 40.9% cases while incomplete or no coverage was 59.1%. 26 Good to excellent cartilage regeneration was found in 84.8% on the femoral condyler. Afterwards, Jung et al. 24 again discovered that there was no significant difference in the formation of fibrocartilage with or without subchondral drilling, considering that subchondral drilling is not necessarily required after MOWHTO. Consistent with the results published in some literature works, our results of HTO demonstrate that better results can also be obtained without cartilage addressing procedures at the last follow-up.
A number of factors potentially affecting the healing of MMPRT and subjective scoring have been discussed, including age, sex, BMI, postoperative mechanical axis and so on. In the study, the BMI and the alignment after surgery are associated with the results, while age did not play a role in the overall results. This is partially in line with the findings of Hwang et al., 7 who found a lower BMI and proper mechanical axis to be closely related to a good outcome.
The postoperative functional scores showed no correlation with the healing degree of MMPRT by now. Seo et al. 10 showed improvements in mean Lysholm scores from 56.1 to 83.0 and an average HSS from 64.1 to 87.4 at 13 months follow-up while complete healing was not observed in all patients. MMPRT fixation did not prevent the progression of arthrosis. Chung et al. 17 noted the Lysholm score improved significantly although the joint space width and the K–L grade worsened greatly after MMPRT more than 5 years postoperation. A systematic review by Feucht et al. 27 concluded the significant improvement of functional outcome scores in all 172 patients at a 3-year follow-up after transtibial MMPRT repair, although complete healing of the repaired root was observed in only about 60% of patients. The reason for all patients’ clinical improvement despite incomplete or failed healing on second-look arthroscopy remains unclear.
There are several limitations of this study, which should be considered. First, this was a retrospective study without a controlled group. Neither does the control group has suturing of MMPRT alone without HTO nor is treated with HTO alone without suturing for evaluation as to what extent healing could be achieved. Second, the cohort was small and arthroscopic evaluation between 1 and 2 years was kind of short. A large scale, long-term follow-up is needed for a more reliable and accurate conclusion.
Conclusions
A higher healing rate of MMPRT using all-inside repair and regeneration of degenerated articular cartilage in the medial condyles after MOWHTO can be expected. Healing of the MMPRT is not related to a better clinical outcome. Low BMI and proper alignment adjustment may be one of the predictive factors for the healing status of MMPRT. With the appropriate subject patient selection and proper surgical technique, a more satisfactory outcome can be achieved.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.